Cardiac Anatomy
25
Cardiac Anatomy
-
Upload
northtec -
Category
Health & Medicine
-
view
1.612 -
download
2
description
cardiac
Transcript of Cardiac Anatomy

Cardiac Anatomy

Cardiac Circulation
The heart has its own blood supply that comes off the root of the aorta just after it leaves the heart (Sinus of Valsalva.)
The heart’s circulation occurs during the diastolic (relaxation) phase of the ventricles.

There are two principal systems (right and left coronary systems) that run over the external surface of the heart muscle and give the heart nutrients and oxygen.
Simplistically, the right coronary artery (RCA) usually supplies the inferior or underside of the heart. It also supplies most of the fuel for the electrical centers of the heart (SA and AV nodes).

The left coronary artery (LCA) starts with left main stem (LMS.) Its less than an inch in length.
It divides into the left anterior descending (LAD) branch down the front of the heart and the circumflex branch around the left side of the heart.
The LCA supplies the bulk of the muscle of the LV and ventricular septum.

From this simple understanding of the structure of the heart you can work out quite a lot of clinically important information.
For example, if there is a blockage of the RCA then the changes on the ECG will be seen on the inferior surface of the heart.
Because the RCA supplies the SA and AV nodes then clearly you can get problems with the formation and passage of electrical information in the heart.

There may be less damage to the left ventricle if your RCA is blocked as it supplies less of the total muscle.
On the other hand, if you have a blockage within the left side of the coronary circulatory system there tends to be greater damage to the left ventricle, particularly if the important LAD is involved.

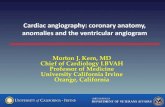
Conduction system of the heart. By permission from Cunningham JG, Textbook of Veterinary Physiology, Saunders, 2002

ECG Leads The leads act as "microphones or viewing posts"
that detect the electrical activity as it approaches.
V1-6 are the precordial (chest or horizontal) leads that are essentially all at roughly the same level on a horizontal plane that is…
right and left---------anterior/posterior. They are relatively poor at giving useful
information in the vertical plane (inferior/superior).

Leads aVR, aVL, and aVF are limb or verticle leads attached to the right arm, left arm, and left leg respectively.
The earth lead (ground) is attached to the right leg.
They detect "sound" in essentially the same way as the precordial leads but this time are best at differentiating right/left and inferior/superior signals.

Six Limb Leads
Leads aVR, aVL, and aVF are 'augmented limb leads'. They are derived from the same three electrodes as leads I, II, and III.
However, they view the heart from different angles (or vectors)
The positive electrode is always the "exploring electrode."


Bipolar Limb Leads

Unipolar or Augmented Leads

Horizontal or Chest leads (also unipolar)

12 lead ECG

Atrial Fibrillation Your heart rate is usually a lot faster than
normal.
Your heart beat is irregular. This is called an abnormal heart rhythm or an 'arrhythmia'.
The force of each heart beat can vary in intensity.

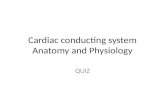
What happens is that the normal controlling 'timer' in the heart is over-ridden by many random electrical impulses that 'fire off' from the heart muscle in the atria.
The atria then 'fibrillate'. This means that the atria only partially contract - but very rapidly (can be up to 400 times per minute).
The ventricular response to the atrial rate can vary significantly

Multiple foci (areas) send out impulses which cause the atria to fibrillate.
Picture courtesy of the Heart Rhythm Society. www.hrsonline.org.

Atrial Fibrillation
Fine P-wave with variable rate

Types of Atrial Fibrillation
Paroxysmal A Fib. Episodes of A Fib that end spontaneously are called paroxysmal A Fib. The irregular heart rhythm may last for a few seconds, minutes, hours or longer before the heart resumes a normal rhythm on its own.
Persistent A Fib. With this condition, the irregular heart rhythm continues indefinitely unless it is treated.
Permanent A Fib. In this situation, normal rhythm cannot be restored.**The sooner its treated, the higher the chance that it can be corrected!

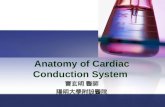
Atrial Flutter
Zaw Tooth P-waves

Causes of A-Fib High blood pressure
Coronary artery disease
Heart failure—a condition in which the heart’s main pumping chambers (the ventricles) don’t work well, and this can lead to problems with the atria
Valvular heart disease—damage to a valve can cause the atria to enlarge and lead to Afib
Lung diseases-some people with chronic lung diseases have changes in the structure of the atria that leads to Afib
Thyroid problems
Others

Symptoms caused by A-Fib Palpitations—skipped or extra heartbeats Shortness of breath Fatigue and tiredness Chest discomfort or pain Dizziness Syncope Fluid retention Anxiety and Apprehension

Risks associated with A-Fib:
Related to decrease in Cardiac Output
*Stroke *Heart Failure
(30% of C.O. is provided by the Atrial)
Related to “Electrical Remodeling”*Damage to heart muscle
(alteration in diastolic phase of the atria)

Treatment options for A-Fib:
Anticoagulation Therapy Drugs to control rate and irregularity of
heart (i.e. Digoxin) Cardioversion Pacemaker Ablation