CARCINOMA VULVA. Mons pubis Labia majora Labia minora Clitoris Vestibule Perineum Bartholin gland...
33
CARCINOMA VULVA
-
Upload
william-oneal -
Category
Documents
-
view
265 -
download
3
Transcript of CARCINOMA VULVA. Mons pubis Labia majora Labia minora Clitoris Vestibule Perineum Bartholin gland...

CARCINOMA VULVA

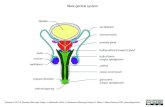
•Mons pubis •Labia majora•Labia minora•Clitoris •Vestibule•Perineum•Bartholin gland•Vestibular
gland
Vulva - AnatomyVulva - Anatomy

Incidence Incidence
• 4-5% of the genital tract malignancies
• Post-menopausal women
• Highest between 60-70 years

ETIOLOGY ETIOLOGY
Still unknown, but certain Still unknown, but certain associatedassociated
etiological factors:etiological factors:
• Human Papilloma virus Human Papilloma virus ( 16,18,31)( 16,18,31)
• Herpes Simplex Type II virusHerpes Simplex Type II virus
• Carcinoma cervix (20-50%)Carcinoma cervix (20-50%)
• Immune suppressionImmune suppression

ETIOLOGYETIOLOGY
• Lower socioeconomic classLower socioeconomic class• Poor hygienePoor hygiene• SmokingSmoking• Chronic granulomatous venereal Chronic granulomatous venereal
lesionslesions• Diabetes MellitusDiabetes Mellitus• Hypertension & arteriosclerosisHypertension & arteriosclerosis• ObesityObesity
Contd.

Lichen sclerosis
pre-cancerous


•Asymptomatic 20%
•Pruritus vulvae 71%
•Vulvar mass 58%
•Ulceration 28%
•Bleeding 26%
•Vulvar pain 23%
•Urinary tract symptoms 14%
•Discharge 13%
CLINICAL FEATURES

SITESITE
• Labia Majora Labia Majora 75%75%
• ClitorisClitoris
• Labia MinoraLabia Minora
• Posterior FourchettePosterior Fourchette
Less common

Advanced squamous cell carcinoma

SITESITE

ROUTES OF SPREADROUTES OF SPREAD
LocalLocal • Vagina Vagina • PerineumPerineum• Anal canalAnal canal• Urethra Urethra • BoneBone
LymphaticLymphatic
•Superficial Superficial
inguinalinguinal
•Deep inguinalDeep inguinal
•Pelvic nodesPelvic nodes

Lymphatic drainage

PATHOLOGYPATHOLOGY
Squamous cellSquamous cell 90%90%MelanomaMelanoma 5-10%5-10%Basal cell Basal cell carcinomacarcinoma
2%2%
AdenocarcinomaAdenocarcinoma 1%1%

FIGO staging (1995)
Stage I Tumour confined to the vulva or perineum , 2 cm or < in greater dimension. No nodal metastasis
Stage Ia
Less than 1mm stromal invasion
Stage Ib
>1 mm stromal invasion
Stage II Tumour confined to the vulva or perineum or both more than 2 cm in greatest dimension. No nodal metastasis

Stage III Extends beyond the vulva, vagina, lower urethra or anus; or unilateral regional lymph node metastasis
Stage IVa
Involves the mucosa of rectum or bladder; upper urethra; or pelvic bone; and / or bilateral regional lymph node metastasis
Stage IVb
Any distant metastasis, including pelvic lymph node
FIGO staging (1995)

DIAGNOSISDIAGNOSIS
•HistoryHistory
•ExaminationExamination
•BiopsyBiopsy

Histological ClassificationHistological Classification
Squamous carcinoma in situ (VIN III) Squamous carcinoma in situ (VIN III) • Paget's disease Paget's disease • InvasiveInvasive
– Squamous cell carcinoma Squamous cell carcinoma – Basal cell Basal cell – Malignant melanoma Malignant melanoma – Adenocarcinoma (Bartholin's gland or Skene's Adenocarcinoma (Bartholin's gland or Skene's
gland)gland)

VIN Invasive VIN
Pathology

Basal and Squamous cell ca
Squamous cell carcinoma
Pathology

Histopathology

Histopathology
Paget’s disease

MANAGEMENTMANAGEMENT
MAINSTAY OF TREATMENT IS MAINSTAY OF TREATMENT IS SURGERYSURGERY
• HEMIVULVECTOMYHEMIVULVECTOMY
• RADICAL VULVECTOMY WITH RADICAL VULVECTOMY WITH LYMPHADENECTOMYLYMPHADENECTOMY EN BLOC DISSECTION BY BUTTERFLY EN BLOC DISSECTION BY BUTTERFLY
INCISIONINCISION SEPARATE VULVAR & INGUINAL INCISIONS SEPARATE VULVAR & INGUINAL INCISIONS
(TRIPLE INCISION)(TRIPLE INCISION)


PREOPERATIVE PREOPERATIVE EVALUATIONEVALUATION
• Blood CPBlood CP• Blood glucose random Blood glucose random • Urine REUrine RE• X-ray chest, ECGX-ray chest, ECG• Pap’s smearPap’s smear• Pelvic ultrasoundPelvic ultrasound
IN ADVANCED CASESIN ADVANCED CASES• Colposcopy, Cystoscopy, ProctoscopyColposcopy, Cystoscopy, Proctoscopy CT Scan, MRICT Scan, MRI

COMPLICATIONS OF COMPLICATIONS OF SURGERYSURGERY
IMMEDIATEIMMEDIATE
• HaemorrhageHaemorrhage
• Wound induration Wound induration
• Partial wound dehiscencePartial wound dehiscence
• Infection Infection

LATE COMPLICATIONSLATE COMPLICATIONS
•Lymphoedema
•Osteitis pubis
•Sexual dysfunction
•Femoral inguinal hernia
•DVTDVT
•ParaesthesiaParaesthesia

ADJUVANT ADJUVANT RADIOTHERAPHYRADIOTHERAPHY
•Pre operativePre operative
•Post operativePost operative

CHEMORADIOTHERAPCHEMORADIOTHERAPHYHY
Has a role in clitoris & Has a role in clitoris & sphincter preserving surgery in sphincter preserving surgery in advanced casesadvanced cases

Follow UpFollow UpPost SurgicalPost Surgical• Every 4 months Every 4 months 1 Year 1 Year • Every 6 monthsEvery 6 months 2 – 5 Years2 – 5 Years• Annually Annually + 5 Years+ 5 Years
Post Radiation Post Radiation • First visit First visit 1 Month1 Month• Every 2 monthsEvery 2 months 1 Year1 Year• Every 6 monthsEvery 6 months 2 – 3 Years 2 – 3 Years • Annually Annually + 3 Years+ 3 Years

SURVIVAL RESULTSSURVIVAL RESULTSDepend on the extent of the Depend on the extent of the disease at the time of diagnosis disease at the time of diagnosis and treatment undertakenand treatment undertaken
Five year survival rate.Five year survival rate.
1.1. Stage I & II Stage I & II 90%90%
2.2. All stagesAll stages 75%75%
3.3. Negative lymph nodes Negative lymph nodes 96%96%
4.4. Positive lymph nodes Positive lymph nodes 66%66%