Canine Sports Medicine and Rehabilitation ...c.ymcdn.com/sites/ D… · recruitment PAIN MANAGEMENT...
42
7/22/13 1 CANINE SPORTS MEDICINE AND REHABILITATION: WHAT YOUR CLIENTS EXPECT Janet B. Van Dyke, DVM, Diplomate, American College of Veterinary Sports Medicine and Rehabilitation Canine Rehabilitation Institute CVMA Annual Conference September 20 , 2013 MUSCULOSKELETAL DYSFUNTION: A Lameness Presents and the Radiographs Are Negative, Now What? What is Veterinary Sports Medicine? It is not the same as Veterinary Orthopedics Canine Sports Medicine includes: Anatomy and Biomechanics Exercise Physiology Conditioning and Retraining Orthopedics Internal Medicine Pulmonology
Transcript of Canine Sports Medicine and Rehabilitation ...c.ymcdn.com/sites/ D… · recruitment PAIN MANAGEMENT...

7/22/13
1
CANINE SPORTS MEDICINE AND
REHABILITATION: WHAT YOUR CLIENTS EXPECT
Janet B. Van Dyke, DVM, Diplomate, American College of Veterinary Sports Medicine and Rehabilitation
Canine Rehabilitation Institute
CVMA Annual Conference
September 20 , 2013
MUSCULOSKELETAL DYSFUNTION:
n A Lameness Presents and the Radiographs Are Negative, Now What?
What is Veterinary Sports Medicine?
� It is not the same as Veterinary Orthopedics
� Canine Sports Medicine includes: � Anatomy and Biomechanics � Exercise Physiology � Conditioning and Retraining � Orthopedics � Internal Medicine � Pulmonology
7/22/13
2
CANINE SPORTS MEDICINE IS:
� Cardiology
� Neurology
� Gerontology
� Nutrition
� Rehabilitation
� Complementary/Alternative Medicine
AMERICAN COLLEGE OF VETERINARY SPORTS MEDICINE
AND REHABILITATION
AMERICAN COLLEGE OF VETERINARY SPORTS MEDICINE
AND REHABILITATION � Developed 2002-2010
� Approved by AVMA and ABVS 2010
� Residencies, Training Programs, Examination
� Currently 85 Diplomates from 5 countries
� 7 Active Residencies � 3 Equine � 4 Canine
� www.VSMR.org

7/22/13
3
Why Add Sports Medicine to Your Practice?
� Opportunity to practice state-of-the-art rehabilitation medicine
� Work with highly educated clients who have significant financial and time investment in their dogs
� Healthy dogs are fun to work with
� Measurable success: Return to sport or work
CANINE SPORTS Non Breed Specific:
� Agility
� Obedience � Tracking
� Skijoring/Skatejoring
� Flyball � Disc Dog
� Dock Diving � Canine Puissance
Breed Specific: � Lure Coursing
� Herding � Field Trials/Hunt Tests
� Earth Dog Tests
� Coon Dog Tests � Schutzhund
� Mushing � Carting
ORGANIZED CANINE SPORTS
7/22/13
4
Agility
FLYBALL

7/22/13
5
Schutzhund
DOCK DIVING

7/22/13
6
PUISSANCE
DISC DOG
SKIJORING/SKATEJORING

7/22/13
7
PULLING/CARTING
WORKING DOGS � Search and rescue
(SAR)
� Bomb detection
� Police
� USDA Beagle Brigade
� Guide Dogs
� Assistance Dogs
� Mold detection
� Geese Police
Why Learn About These Sports?
� You injure your foot playing Soccer with your kids.
� You visit a physician who asks, “What is Soccer?” � Your comfort level with having him
treat you? � Your willingness to follow his plan of
care?

7/22/13
8
What is Veterinary Rehabilitation?
� Definition:
� The treatment of physical injury or illness in an animal to decrease pain and restore function
What is Veterinary Rehabilitation? � It is NOT all about the
Underwater Treadmill…Or
the LASER…

7/22/13
9
EDUCATION " Physical Therapists � 4-5 year post graduate program � All graduate with a clinical doctorate degree " DPT
� Advanced Certification in clinical specialties " Orthopaedics, Neurology, Cardiopulmonary,
Sports Medicine " Animal Rehabilitation Special Interest Group
A ‘New’ Diagnostic Algorithm
� Kent Allen: “In the absence of a diagnosis, Surgery is trauma, Medicine is poison, and Alternative Therapy is witchcraft.”
� The physical therapist’s approach to the patient � Emphasis upon soft tissues � Special tests allowing determination of
specific tendinopathies and soft tissue impairments
Objective Outcome Measures

7/22/13
10
REHABILITATION APPROACH
" Emphasis on a proper, thorough soft tissue diagnosis
" Emphasis on problem solving
" Emphasis on creating and meeting goals which are functional
REHABILITATION APPROACH
� Majority of therapeutics involve manual therapies and problem solving � Joint Mobilizations � Arthrokinematics VS Osteokinematics
� Therapeutic exercise � Concentric
VS Eccentric contractions � Modalities � Cryotherapy � Laser � E-Stim
� “I believe that in the near future, failing to refer a patient for physical therapy will amount to malpractice.”

7/22/13
11
� “I believe that in the near future, failing to refer a patient for physical therapy will amount to malpractice.” -1959
H. A. Apfelbach, MD
Director of Orthopedics Rush Presbyterian Medical Center Chicago, IL
ANIMAL REHABILITATION � WHAT IS DRIVING THIS NEW FIELD?
PUBLIC AWARENESS � Similar to Acupuncture in
the 1980’s � Client driven demand for
veterinary services
� Current Drivers for Canine Rehabilitation � Agility � 2012: >1 Million Entries � >1000 Sanctioned
Events in the US

7/22/13
12
WHY SHOULD YOU ADD REHABILITATION TO YOUR
PRACTICE? " Increased awareness
" Client demand � Pain management � Return to sports � Improved geriatric
therapy � Weight management
SPORT-SPECIFIC AND JOB-SPECIFIC INJURIES COMMONLY
TREATED WITH REHABILITATION � Shoulder Insertionopathies
� Medial Shoulder Instability
� Teres Major Strain
� CCL Injuries
� Iliopsoas Strain

7/22/13
13
REAHABILITATION OPTIONS FOR THE CCL PATIENT
� Treatment techniques address the following: � Pain � Inflammation
� Hypomobility � Hypermobility � Weakness � Altered muscle
recruitment
PAIN MANAGEMENT n Physical Therapists bring their skills to
the veterinary industry
n Determining specific soft tissue pathologies allows us to apply focused treatments to patients previously treated with “Rest and NSAID’s”
PAIN MANAGEMENT � Medical Management
� Physical Modalities
� Joint Mobilizations
� Stretches
7/22/13
14
REAHABILITATION OPTIONS FOR THE CCL PATIENT
� Treatment techniques address the following: � Pain � Inflammation
� Hypomobility � Hypermobility � Weakness � Altered muscle
recruitment
RANGE OF MOTION n OSTEOKINEMATICS
Osteo = bone
Kinematic = motion
DEFINITION:
Bony segments moving around a joint axis
RANGE OF MOTION n Two kinds of Osteokinematic ROM
- Active Range of Motion (AROM)
- Passive Range of Motion (PROM)
n Assessment of AROM and PROM are important components of the rehabilitation evaluation

7/22/13
15
ACTIVE RANGE OF MOTION n DEFINITION:
v Active motion performed by the patient
v Responsible for increasing strength
PASSIVE RANGE OF MOTION n DEFINITION: � The motion is performed
by the therapist � No muscular effort by the
patient
n Measured with a Goniometer � Specific bony landmarks
GONIOMETRY
Stable Arm
FULCRUM
Moving Arm
7/22/13
16
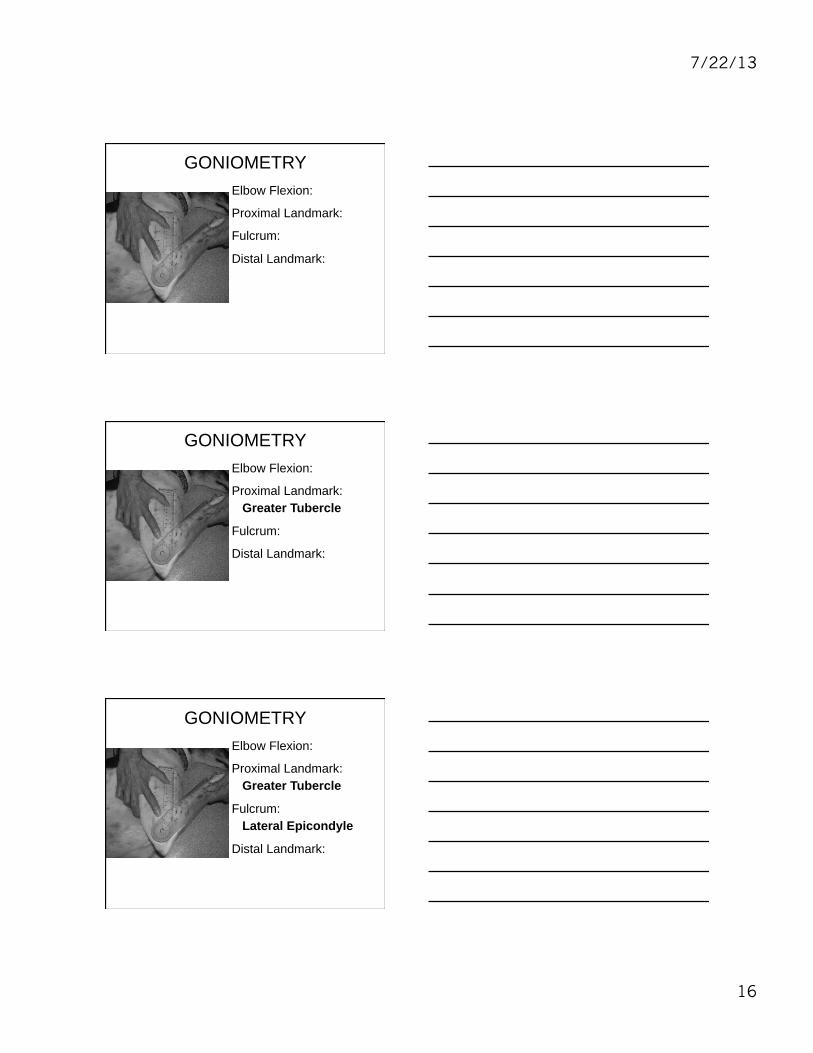
GONIOMETRY Elbow Flexion:
Proximal Landmark:
Fulcrum:
Distal Landmark:
GONIOMETRY Elbow Flexion:
Proximal Landmark: Greater Tubercle
Fulcrum:
Distal Landmark:
GONIOMETRY Elbow Flexion:
Proximal Landmark: Greater Tubercle
Fulcrum: Lateral Epicondyle
Distal Landmark:

7/22/13
17
GONIOMETRY Elbow Flexion:
Proximal Landmark: Greater Tubercle
Fulcrum: Lateral Epicondyle
Distal Landmark: Lateral Styloid Process
ACTIVE VS. PASSIVE ROM What Does It Tell Us?
Clinical Example: AROM: Shoulder Extension
1. Painful
2. AROM Limited
PROM: Shoulder Extension 1. No Pain
2. PROM Normal
ACTIVE VS. PASSIVE ROM What Does It Tell Us?
Clinical Example: AROM: Shoulder Extension
1. Painful
2. AROM Limited
PROM: Shoulder Extension 1. No Pain
2. PROM Normal DDx: Biceps or Supraspinatus Tendinopathy

7/22/13
18
QUESTIONS?
LIMITED PROM? � WHAT CAN LIMIT ROM? o Muscle/Tendon – decreased flexibility
o Intra-articular lesion (meniscus, bone)
o Joint Capsule shortening
o Pain
o Swelling
How do we determine which of these structures is limiting PROM?
n Answer: END FEEL
n Definition:
The sensation or feeling (in your hands) when the joint is at the end of its available PROM
7/22/13
19
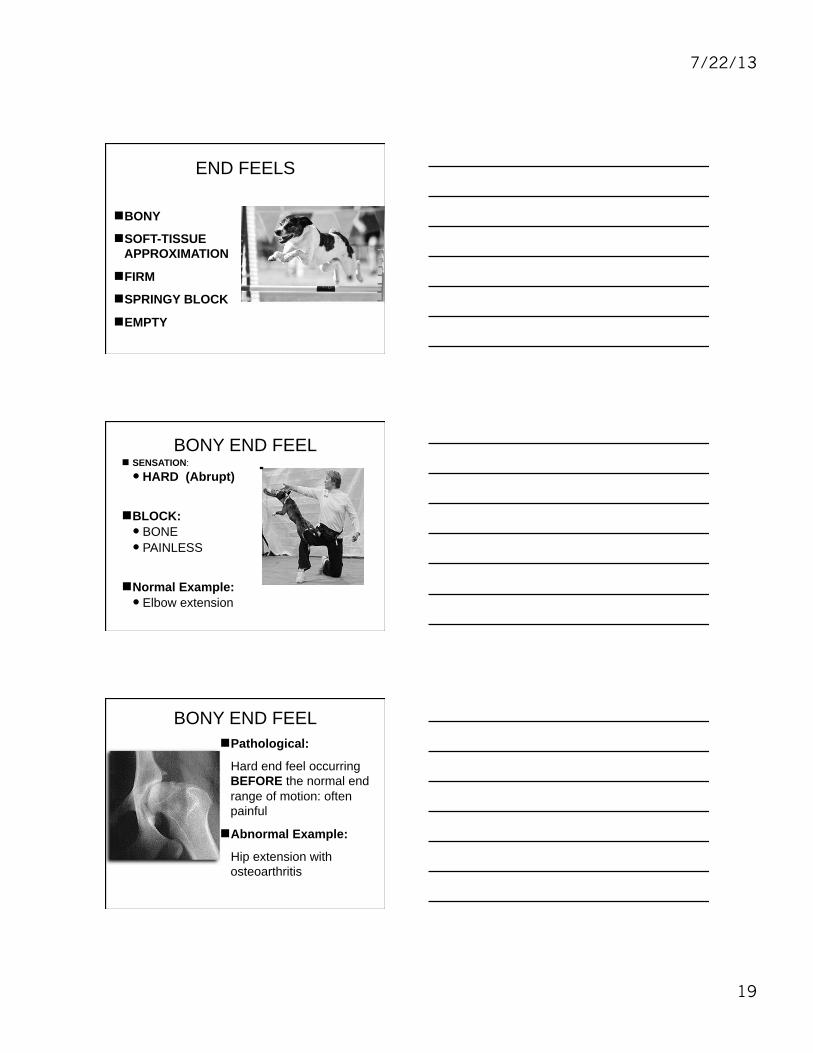
END FEELS
n BONY
n SOFT-TISSUE APPROXIMATION
n FIRM
n SPRINGY BLOCK
n EMPTY
BONY END FEEL n SENSATION: � HARD (Abrupt)
n BLOCK: � BONE � PAINLESS
n Normal Example: � Elbow extension
BONY END FEEL n Pathological:
Hard end feel occurring BEFORE the normal end range of motion: often painful
n Abnormal Example:
Hip extension with osteoarthritis

7/22/13
20
END FEELS n WHY DO WE CARE ABOUT
THEM? q Assists to identify the structure or the
tissue limiting PROM
q Allows focused treatment
ROM AND END FEELS n ROM
1. Active or Passive 2. Which motion? Flexion/Extension 3. Amount of motion
(Goniometer) 4. End Feel 5. Flexibility of 2 joint muscles
WHAT IS NEXT? n Assess: � Arthrokinematics � Accessory Joint Motions � Ligamentous Stability � Muscle Strength

7/22/13
21
ARTHROKINEMATICS n DEFINITION:
� Movement that occurs between two joint surfaces
n Glide
n Roll
PATHOLOGY DUE TO POOR ARTHROKINEMATICS
n PURE GLIDE WITHOUT ROLL RESULTS IN IMPINGEMENT OF SOFT TISSUE OR CARTILAGE.
n Example: Drawer without stifle ‘roll’ results in Meniscal entrapment
PATHOLOGOY DUE TO POOR ARTHROKINEMATICS
n PURE ROLL WITHOUT GLIDE RESULTS IN JOINT DISLOCATION
7/22/13
22
ARTHROKINEMATICS n Passive
n Involuntary
n “Accessory Joint Motion”
n Normal arthrokinematics are required for normal osteokinematics
QUESTIONS?
REAHABILITATION OPTIONS FOR THE CCL PATIENT
� Treatment techniques address the following: � Pain � Inflammation
� Hypomobility � Hypermobility � Weakness � Altered muscle
recruitment

7/22/13
23
REHABILITATION SKILLS � Manual
Techniques
� Therapeutic Exercise
� Physical Modalities
REGULAR REASSESSMENT IS VITAL
� Determine Appropriate Blend of Manual Work, Modalities and Therapeutic Exercise
� Justify Each Element of the Treatment Plan � Based upon Patient Response to Prior
Treatment � Based upon Today’s Findings
� As Pain and Mobility Issues are Resolved, Therapeutic Exercise is the Focus
STIFLE SPECIFICS � Biology and Biomechanics are Key
Contributors to CCL Disease and Injury
� Biology is Addressed with Modalities and Manual Therapy � Decrease Pain � Promote Tissue Healing � Reduce Inflammation and Swelling
� Laser, Ice/Compression
� Grade I-II Joint Compressions

7/22/13
24
STIFLE SPECIFICS � Biomechanics � Instability
Addressed with Therapeutic Exercise � Strengthen
Dynamic Stabilizers of the Stifle and Core
� Proprioceptive Inputting to Prevent Reinjury
TREATMENT RATIONALE � Depends upon the type of surgery � Osteotomy requires activity modification
to ensure bone healing � Human research supports: � Early use of NMES to prevent muscle
atrophy and associated weakness � Hasagawa, et al, 2011
� Early use of eccentric muscle contractions increase muscle mass and function
� Gerber, et al., 2009
� Perturbation exercises to enhance coordinated muscle activity
� Risberg et al., 2007, Chimielewski et al., 2005
Therapeutic Modalities !
� A device or application that delivers a physical agent to the body for therapeutic purposes!
Transfer of ENERGY for therapeutic purposes"

7/22/13
25
TREATMENT RATIONALE � Canine research supports:
� Cold Compression Therapy: � Decreased signs of pain,
swelling, and lameness � Increased stifle joint range of
motion in dogs during the first 24 hours after TPLO � Drygas, et al. JAVMA, Vol 238, No. 10,
May 15, 2011 pg. 1284-1291
TREATMENT RATIONALE � LASER: � Wound healing: � Increase: fibroblast proliferation,
differentiation, collagen deposition, angiogenesis
� Decrease inflammation and edema: � Decrease: IL-1, PG. Improve WBC activity,
decrease vessel permeability � Decrease pain: � Increase B endorphins, decrease bradykinin,
block C fiber depolarization
Hawkins, DH 2006; Tuner J, 2007; Montesinos M, 1988; Wakabayashi H, 1993
TREATMENT RATIONALE � NMES:
� Canine CCL transection model � Decreased: � cartilage damage, radiographic OA,
crepitus, lameness
� Increased: � thigh circumference
Johnson JM, Vet Res 1997

7/22/13
26
Neuromuscular Electrical Stimulation
n NMES � “E-Stim” � Application of electrical
current to elicit a muscle contraction
� Reduce edema � Muscle re-education � Reversal of atrophy � Wound healing
Effects of Electrotherapy Ø CELLULAR LEVEL - Excitation of nerve cells
- Changes in cell membrane permeability
- Protein synthesis
- Stimulation of fibroblasts, osteoblasts
Electrotherapy
Wound healing
n Increased blood flow to the area
n Stimulates cell turnover

7/22/13
27
Electrotherapy for Pain Control/Relief
Gate Theory � Severity of pain
sensation: � Balance of excitatory (C and A-Delta) and inhibitory (A-Beta) inputs to the T (transmission) cells in the spinal cord
Electrotherapy for Pain Control/Relief n TENS � Short-lived effect n One hour ?
� Uses: n Immediately PO n During therapy to
allow pain-free movement
THERAPEUTIC EXERCISE � Proprioception
� Balance
� Muscle Strengthening
� Endurance
� Gait Retraining

7/22/13
28
THERAPEUTIC EXERCISE VARIABLES
� Frequency
� Intensity
� Duration
� Environment
� Impact
THERAPEUTIC EXERCISE EQUIPMENT
� PHYSIOBALLS
� THERABANDS
� ROCKER BOARDS
� CAVALETTI POLES
� TREADMILL
THERAPEUTIC EXERCISE PATIENT CONSIDERATIONS
� Motivation
� Footing
� Assistive Devices
� Leash/Harness Control
OWNER HANDLER CONSIDERATIONS
� Body Mechanics

7/22/13
29
PROPRIOCEPTION � Addressed daily to regain proper
balance and to prevent reinjury
� Cavaletti poles and Weave poles
�
ECCENTRIC EXERCISES � ACL patient needs increased hamstring
strength
� Eccentric hamstring contraction: � Requires lengthening of the muscle while
contracted � Hip flexion � Stifle extension � Tarsus flexion
� Controlled Stand-to-Sit Exercise or Paws On The Counter
� Backward Walking

7/22/13
30
PROGRESSION OF EXERCISES � Once proprioception circuits
and strength exercises completed:
� Sports-specific exercises added
� Endurance work progressed
� Cross-training program initiated
� Training calendar created for owner/handler
SUPRASPINATUS TENDINOPATHY � What is a “Tendinopathy”? � Overuse injury of the
tendon and surrounding tissues
� Requires lengthy treatment
� Historically poor results
SUPRASPINATUS TENDINOPATHY
� Unilateral forelimb lameness � Non-responsive to rest and
NSAID’s � Worse after exercise

7/22/13
31
SUPRASPINATUS TENDINOPATHY � Anatomy: � Origin: Supraspinous
fossa � Insertion: Anterior
Greater Tubercle � Action: Stabilizer of the
joint; gleno-humeral extension
� Injury: Eccentric contraction during rapid elongation
SUPRASPINATUS TENDINOPATHY
� Physical Exam findings: � Supraspinatus atrophy � Pain on shoulder flexion � Especially with pressure on the insertion point
SUPRASPINATUS TENDINOPATHY
� Forelimb muscle girth diminished � Gulick Girthometer
� Decreased ROM Shoulder Flexion � Goniometer
7/22/13
32
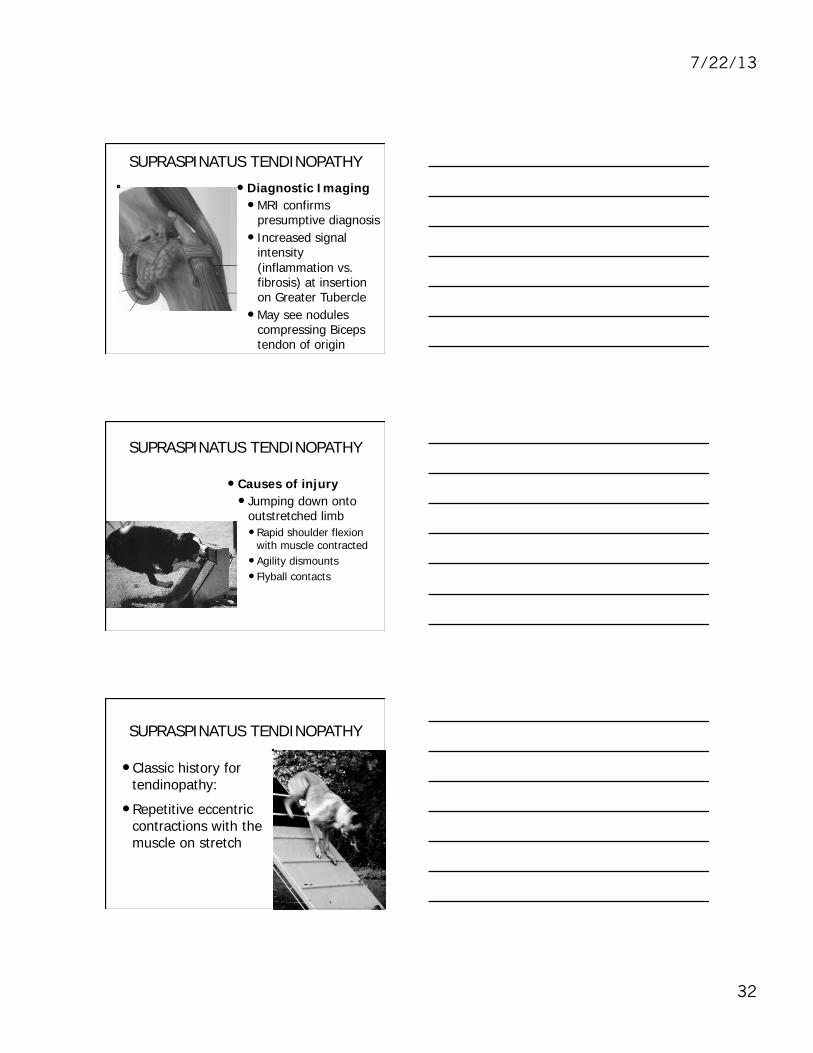
SUPRASPINATUS TENDINOPATHY
� Diagnostic Imaging � MRI confirms
presumptive diagnosis � Increased signal
intensity (inflammation vs. fibrosis) at insertion on Greater Tubercle
� May see nodules compressing Biceps tendon of origin
SUPRASPINATUS TENDINOPATHY
� Causes of injury � Jumping down onto
outstretched limb � Rapid shoulder flexion
with muscle contracted � Agility dismounts � Flyball contacts
SUPRASPINATUS TENDINOPATHY
� Classic history for tendinopathy:
� Repetitive eccentric contractions with the muscle on stretch

7/22/13
33
SUPRASPINATUS TENDINOPATHY � Principal lesion in chronic human rotator
cuff injury
� Research with animal models: � Overuse activity leads to decreased
elasticity � Reduced stress-to-failure � Proliferative nodule at insertion with no
signs of inflammation � Calcification in chronic cases
J Shoulder Elbow Surg 2000
SUPRASPINATUS TENDINOPATHY
� Surgical management � Historically: Tendon debridement and
release � Poor results reported � JAVMA 1990 and 2005 � Vet Record 1996 � JAAHA 2000
SUPRASPINATUS TENDINOPATHY
� Extracorporeal Shock Wave Therapy � U of Wisconsin, CVM � Good results
� Danova NA, Muir P: ESWT for supraspinatus calcifying tendinopathy in two dogs. Vet Rec 152:208-209, 2003

7/22/13
34
SUPRASPINATUS TENDINOPATHY � Physical Therapy
techniques in human Supraspinatus Tendinopathy: � Manual Therapy � Ultrasound � LASER � Therapeutic exercise
SUPRASPINATUS TENDINOPATHY
� Manual Therapy techniques � Joint Mobilizations � Massage � Create brief inflammatory response to
encourage a resolution of chronic signs � Cross Friction Massage � At tendon insertion � At tendon-muscle interface � With internal rotation of the humeral
head
SUPRASPINATUS TENDINOPATHY � Therapeutic Ultrasound � To warm tendon-muscle
interface � To reduce calcification in
tendon sheath
� Stretching after massage or Ultrasound � Shoulder flexion with
internal rotation of the humeral head

7/22/13
35
SUPRASPINATUS TENDINOPATHY
� LASER Therapy � Treatment of choice today � Stimulation of myocyte and fibroblast
mitochondria � Shown to speed healing of
microfractures in soft tissue
SUPRASPINATUS TENDINOPATHY
� Therapeutic Exercise � Upon relief of any proliferative nodules,
therapeutic exercise is prescribed � Strength Work � Resistance Work � Proprioception Work � Retraining Techniques
SUPRASPINATUS TENDINOPATHY � Therapeutic Exercise � Strength Work � Start with
Concentric Exercise � No resistance � Shoulder extension � Physioball � Cavaletti Poles

7/22/13
36
SUPRASPINATUS TENDINOPATHY
� Therapeutic Exercise--Strength Work � Progress to Concentric with Resistance � Therapy Bands � Water Walking
SUPRASPINATUS TENDINOPATHY
� Therapeutic Exercise--Strength Work
� Eccentric Exercise after Concentric � Shoulder Flexion with muscle contracted � Lie Down � Walk down stairs or ramp � Commando Crawl
SUPRASPINATUS TENDINOPATHY � Therapeutic Exercise � Proprioception Work

7/22/13
37
SUPRASPINATUS TENDINOPATHY � Retraining Techniques � Agility
� Warm up protocol � Cool down protocol � Alter contact techniques
� Flyball � Swimmers’ Turn
� Cross Train
ILIOPSOAS STRAINS ILIOPSOAS (FUSION OF THE PSOAS
MAJOR AND ILIACUS)
§ O: 1) Iliacus: Cranioventral Ilium
2) Psoas Major: Ventral bodies and transverse processes of all Lumbar vertebrae and last 3-4 thoracic vertebrae
§ I: Lesser Trochanter
§ A: Flexion and external rotation of the Hip
Flexion of the Lumbar spine
ILIOPSOAS STRAINS
� Unilateral hind limb lameness
� Diminished extension of rear limbs in jumping
� Decreased use of the rear limbs in weave poles

7/22/13
38
ILIOPSOAS STRAINS � Mild thigh girth atrophy � Pain on extension, internal
rotation, abduction of affected CF joint
� Pain on palpation of the region
� Breur, GJ et al: Traumatic injury of the Iliopsoas muscle in three dogs;JAVMA 210:163-164, 1997
ILIOPSOAS STRAINS � Injury tends to be close to
the myotendinous junction
� Chronic injury results in mineralization of the tendon of insertion
� Diagnostic ultrasound will detect the lesion
� MR or CT are also used

7/22/13
39
ILIOPSOAS STRAINS � Treatment for Acute: � Rest, muscle relaxants, ice, NSAIDs � Rehabilitation program for 6-9 weeks � Acupuncture for pain � Modalities: � Laser � Increase circulation � Decrease pain � Speed healing
� Therapeutic Ultrasound
ILIOPSOAS STRAINS � Manual Therapy � PROM without pain � No stretching in acute injury
� Therapeutic Exercise � Stabilization exercises with a gradual
increase in weight bearing � Progress to strength work and AROM � Cavaletti Poles � 2-leg standing (right or left) � Paws on Counter � Wobble Board
ILIOPSOAS STRAINS Treatment for Chronic Strains � Need to fire up the inflammatory process � No NSAIDs � Heat � Ultrasound � Laser � Massage
� Stretch after heat � Correct the mechanics of the lumbosacral spine
7/22/13
40
Therapeutic Exercise For Chronic Iliopsoas Strains
� More challenging than treating acute cases
� Require slower return to function
� Long term: High risk of re-injury � Advise warm-up
and stretch routines
ILIOPSOAS STRAINS
� Cross training is important to avoid boredom and reinjury � Endurance (Treadmill) � Jumping � Balance � Plyometrics
� Time off between ‘seasons’ is essential
WHAT WOULD IT TAKE TO ADD SPORTS MEDICINE/REHABILIATATION TO YOUR
PRACTICE? " Training your team
" Minimal equipment list
" Minimal space dedication
7/22/13
41
TRAINING THE REHAB TEAM
" Modules " Exams " Internships
IS VETERINARY REHABILITATION A VIABLE BUSINESS?
" Done correctly, YES!
" Business models that have worked the best: � Referral centers with surgery � Free standing rehab-only, referral-only
facilities � Specialty centers with emphasis on
Complementary Medicine and Pain Management
� General Practices that recognize the client-driven demand for Rehabilitation
CONCLUSION Know Your Patient’s Job And Expectations
� Great Diagnostics
� Anatomical Awareness
� Great Manual Skills
� Creative Problem Solving
� Awareness Of Current Techniques
� Excellent Pain Management
7/22/13
42
Canine Sports Medicine and Rehabilitation
Edited By: M. Christine Zink Janet B. Van Dyke
ISBN 978-‐0-‐8138-‐1216-‐8 E-Book ISBN 978-‐1-‐118-‐54151-‐7 April 2013 $99.99 / £62.99 / CAN$109.99
Order online at www.wiley.com
QUESTIONS? Questions?