BULLETIN PHARMACY -...
15
Psoriasis is a chronic inflammato- ry disease that affects primarily the skin and some of these patients may develop psoriatic arthritis. 1-3% of the general population worldwide were affected by psoriasis, with peak onset occurs between the ages of 16 to 22 years old and at 57 to 60 years old. The most common form of psori- asis is chronic plaque psoriasis, also known as psoriasis vulgaris. Its clini- cal features include raised, well- defined inflamed skin lesions (plaques) with silvery – white scale. Due to the increased loss of water through the affected epidermis, the lesions tend to be itchy. The lesions may also turn into painful fissures or cracks. Apart from physical discom- fort, patients may suffer from psycho- social issues because of the highly visible nature of the disease impact- ing on their daily activities, social in- teractions and ability to work. Pathophysiology of Psoriasis The exact cause of psoriasis is not fully understood yet, but current evidence showed that it involves an autoimmune process described below: Trigger factors (see page 3) induce clonal expansion of T cells in lymph node. When T cells being reactivated after entering dermis and epidermis, they release cytokines that cause hyper- propliferation of keratinocytes. Therefore, new skin cells differenti- ate and mature over 7 days in psoria- sis patients compared to 28 days for normal people. The abnormal turno- ver and buildup of skin cells cause the formation of psoriatic plaques. Decreased release of lipids at the skin surface lead to flaking, scaly presentation. Increased number and size of dermal blood vessels cause the redness be- neath psoriatic plaques. Figure 1 Pathophysiology of Psoria- sis PSORIASIS INSIDE THIS ISSUE: PSORIASIS 1-7 ADR Sept– Dis 2013 8 MADRAC UPDATE 9-11 FDA SAFETY UPDATE 12 ANNOUNCE- MENT 13 ACTIVITY OF PHARMACY DEPARTMENT 14 BULLETIN PHARMACY VOLUME 4/ 2013 EDITORIAL BOARD Advisor : Pn Siti Asmah Basi- min Editor : Tan Lay Chai Co-editor 1.Khoo Chee Shin 2.Tai Ann Nny 3.Nur Syahirah Bt Abd Raof HS FARMASI PHARMACY DEPARTMENT HOSPITAL SEGAMAT
Transcript of BULLETIN PHARMACY -...

Psoriasis is a chronic inflammato-
ry disease that affects primarily the
skin and some of these patients may
develop psoriatic arthritis. 1-3% of
the general population worldwide
were affected by psoriasis, with peak
onset occurs between the ages of 16
to 22 years old and at 57 to 60 years
old. The most common form of psori-
asis is chronic plaque psoriasis, also
known as psoriasis vulgaris. Its clini-
cal features include raised, well-
defined inflamed skin lesions
(plaques) with silvery – white scale.
Due to the increased loss of water
through the affected epidermis, the
lesions tend to be itchy. The lesions
may also turn into painful fissures or
cracks. Apart from physical discom-
fort, patients may suffer from psycho-
social issues because of the highly
visible nature of the disease impact-
ing on their daily activities, social in-
teractions and ability to work.
Pathophysiology of Psoriasis
The exact cause of psoriasis is not fully
understood yet, but current evidence
showed that it involves an autoimmune
process described below:
Trigger factors (see page 3) induce
clonal expansion of T cells in lymph
node.
When T cells being reactivated after
entering dermis and epidermis, they
release cytokines that cause hyper-
propliferation of keratinocytes.
Therefore, new skin cells differenti-
ate and mature over 7 days in psoria-
sis patients compared to 28 days for
normal people. The abnormal turno-
ver and buildup of skin cells cause
the formation of psoriatic plaques.
Decreased release of lipids at the
skin surface lead to flaking, scaly
presentation.
Increased number and size of dermal
blood vessels cause the redness be-
neath psoriatic plaques.
Figure 1 Pathophysiology of Psoria-
sis
PSORIASIS
I N S I D E T H I S
I S S U E :
PSORIASIS 1-7
ADR Sept–
Dis 2013
8
MADRAC
UPDATE
9-11
FDA SAFETY
UPDATE
12
ANNOUNCE-
MENT
13
ACTIVITY OF
PHARMACY
DEPARTMENT
14
BULLETIN PHARMACY V O L U M E 4 / 2 0 1 3
EDITORIAL
BOARD
Advisor : Pn Siti Asmah Basi-
min
Editor : Tan Lay Chai
Co-editor 1.Khoo Chee Shin
2.Tai Ann Nny
3.Nur Syahirah Bt
Abd Raof
HS
FARMASI
PHARMACY
DEPARTMENT
HOSPITAL
SEGAMAT

P A G E 2
Table 1: Classification of Psoriasis Type of
Psoriasis
Description
Psoriasis
vulgaris
Most common form (80-90% of patients)
Well-defined, inflamed plaques with silvery scale typically on
the lower back, knees and elbows
Flexural
psoriasis
Distinct reddened patches in body folds and flexures with min-
imal scaling because these areas tend to be moist
May occur alone or can be accompanied by plaques in other
body parts
Scalp psoriasis Present in about 50% of people with psoriasis
May present as discrete plaques or more profuse scale
extending beyond the hairline
Guttate
psoriasis
Acute form of psoriasis often triggered by upper respiratory
tract streptococcal infections
A sudden eruption of small inflamed lesions with a fine scale
usually develop over the trunk and limbs, and sometimes on
the face and scalp
May resolve spontaneously or require treatment
Nail psoriasis Can be associated with all types of psoriasis
Include yellow-brown discoloration, pitting, nail crumbling,
thickened nails
Fingernails are more commonly affected than toenails
Pustular
psoriasis
Localised: small, fluid-filled blisters (pustules) form on the
palms of the hands and soles of the feet, they do not rupture but
become a dark brown colour with scale as they reach the
surface and may be painful
Generalised: uncommon, but may be accompanied by fever and
tenderness, and requires immediate medical attention
Erythrodermic
psoriasis
Painful, generalised red rash develop over a large area of the
body and may be accompanied by a fever
Peeling and blistering of the skin can also occur
Rare but serious and needs urgent medical attention
May develop gradually from psoriasis vulgaris or acutely with
no previous skin lesions
Psoriatic arthritis Up to 50% of psoriasis patients may develop inflammatory
arthritis
Commonly affects joints in hands and lower spine
Symptoms include pain, swelling and stiffness
Similar to rheumatoid arthritis but rheumatoid factor antibody
is absent
Figure 2
Psoriasis vulgaris on
both knees
Figure 3
Flexural psoriasis at
armpit
Figure 4
Scalp psoriasis
Figure 5
Guttate psoriasis

P A G E 3
Risk and Trigger Factors
B U L L E T I N P H A R M A C Y
Figure 6
Nail changes in
psoriasis
Figure 7
Pustular psoriasis
on the palm of left
hand
Figure 8
Life-threatening
erythrodermic
psoriasis
Factors that may contribute to the
onset of psoriasis and trigger future
exacerbations:
Family history of psoriasis
Recent infection eg.
streptococcal infection
Trauma/injury to the skin
Personal history of skin
disorder
Sunburn
Seasonal changes in weather
Obesity
Smoking
Emotional stress
Excessive alcohol intake
Medicines
Medicines that have been reported
to trigger or exacerbate psoriasis:
Beta blockers
Lithium
Hydroxychloroquine
ACE inhibitors
Indomethacin
Terbinafine
Interferon alfa-2b
Amiodarone
Oral corticosteroids (on
cessation)
Citalopram, escitalopram
Psoriasis is associated with an increased risk of numerous co-morbidities particularly
metabolic syndrome and atherosclerosis-related diseases. Psoriasis patients have
significant risk of developing metabolic abnormalities such as abdominal obesity,
dyslipidaemia and diabetes mellitus. Atherosclerosis-related diseases that are associ-
ated with psoriasis includes ischemic heart disease and stroke. It is postulated that the
increased risk of cardiovascular disease is due to coronary artery calcification caused
by the chronic inflammatory process involved in psoriasis.
Psoriasis is also linked with elevated risk of developing autoimmune diseases such as
inflammatory bowel disease. Besides that, patients with severe psoriasis have higher
risk of depression and anxiety which could lead to suicide. Although psoriasis has
been associated with greater chance of skin cancer, it is uncertain that this is caused
by the disease itself or the phototherapy treatment.
Medical Co-morbidities
Figure 9 Koebner phenomenon
Psoriatic lesion appear at a site
of injury after localised trauma

V O L U M E 4 / 2 0 1 3 P A G E 4
Management of Psoriasis Psoriasis can be managed by lifestyle modifications
such as stress management, and pharmacological
treatments which include topical treatments,
phototherapy and systemic therapies. Although
psoriasis is not curable, available treatments help to
control symptoms and induce remission.
The choice of treatment depends on the severity of the
disease, the sites affected and the impact of the disease
on the quality of life. Table 2 shows the assessment of
severity of psoriasis based on the body surface area
(BSA), Psoriasis Area & Severity Index (PASI), and
Dermatology Life Quality Index (DLQI). Mild to
moderate with minimal impact on the quality of life
can be managed with topical treatments either
monotherapy or a combination of therapies which have
different mechanisms of action. As for psoriasis which
is severe, involves extensive areas or greatly reduces
patients’ quality of life, dermatologists may
recommend phototherapy or systemic agents.
Table 2 Severity of Psoriasis
Severity BSA PASI DLQI
Mild < 10% < 10 < 6
Moderate 10-29% 10-19 6-17
Severe ≥ 30% ≥ 20 ≥ 18
Coal tar is used to treat limited or scalp psoriasis due
to its anti-inflammatory and anti-pruritic properties.
Coal tar formulated in shampoo may be used twice
weekly up to once daily for scalp psoriasis. Coal tar
cream, lotion or gel can be applied once to three times
daily but it should be avoided on face, skin flexures
and genitals due to possible irritation. It is important to
prevent sunlight exposure for 24 hours after
application of coal tar because it causes
photosensitivity. Patients may less likely to adhere to
coal tar therapy due to its unpleasant smell. It also
stains the skin, hair or clothing.
Dithranol is useful, for treating thick plaque psoriasis
as it helps to reduce the rate of epidermal cell
proliferation. Dithranol 0.1-0.5% in ointment or paste
is suitable for overnight treatment, while 1-2% is used
for short contact treatment up to 1 hour. It should be
avoided on face, skin flexures and genitals because it
may cause local burning sensation and irritation. Like
coal tar, it also stains the skin, hair and clothing.
Topical Therapies
Topical treatments have minimal side effects
compared to systemic therapies but their efficacy
highly depends on the adherence to the treatments.
They are formulated as creams, ointments, lotions, gels
and shampoos. The choice of formulation depends on
the site of application. For an instance, gels or lotions
may be preferred for hairy areas. Topical treatments
available for psoriasis include emollients, keratolytics,
coal tar, dithranol, corticosteroids and calcipotriol.
Emollients such as aqueous cream and white soft
paraffin should be used regularly as a soap or applied
to the skin twice daily. Emollients hydrate and soften
the plaques to reduce itchiness, scaling and cracking of
the skin.
Salicylic acid, a keratolytic, helps to remove scale on
the skin or scalp. Therefore, it increases penetration of
other topical agents such as coal tar, dithranol and
corticosteroids when used in combination with these
agents. However, it can cause skin irritation and
redness.
Topical corticosteroids are used in the treatment of
psoriasis because they inhibit cytokine production,
thus reducing inflammation and the rate of epidermal
cell proliferation. They act quicker to clear the plaques
than coal tar and dithranol but remission period may be
shorter. Less potent agent such as hydrocortisone 0.5-
1% may be applied to face and flexures once to twice
daily up to 1 week. More potent agents such as
betamethasone valerate 0.01-0.1% and clobetasol
propionate 0.05% may be applied to other areas once
to twice daily for no more than 4 weeks. Occasionally,
topical corticosteroids may be used with occlusive
dressing under supervision of dermatologist to help
increase penetration into thick plaque. The risk of local
side effects such as skin thinning and allergic contact
dermatitis increases with prolonged use of topical
corticosteroids. Although systemic side effects are rare
with topical corticosteroids, it is recommended to
reduce the frequency of application or change to less
potent agent once the condition is controlled. Topical
corticosteroids are contraindicated for patients who
have untreated bacterial, fungal or viral skin lesions.
Figure 10 Fingertip unit (FTU)
rule for topical corticosteroids
and calcipotriol
1 FTU = 0.5g and should cover
an area equivalent to the size of
two hand palms of the patient

V O L U M E 4 / 2 0 1 3 P A G E 5
Management of Psoriasis Calcipotriol is a synthetic analogue of vitamin D used
to treat chronic stable plaque psoriasis and scalp
psoriasis. It reduces the rate of epidermal cell division
by binding to vitamin D receptors. It is available as
50mcg/g cream or ointment to be applied once daily up
to 100g weekly. It is also available as 50mcg/ml scalp
solution to be used twice daily up to 60ml weekly. It
may take up to 6 weeks of continuous use to get
desired improvement in symptoms. Avoid use on face
because local adverse effects of calcipotriol include
itching, burning, dryness and erythema. However, they
usually subside with continued use. Systemic adverse
effects such as hypercalcaemia may occur due to
application more than recommended dosage or
existing renal impairment. Patients should be advised
to avoid exposure to sunlight and sunlamps because
ultraviolet A (UVA) radiation can inactivate
calcipotriol. There is also a combination product
containing calcipotriol 50mcg/g and betamethasone
dipropionate 0.5mg/g ointment which is indicated for
resistant plaque psoriasis. It can be applied once daily
to maximum 30% of body surface up to 4 weeks with
maximum 100g per week. This combination has been
shown to be more effective than calcipotriol or
betamethasone alone.
Phototherapy
Phototherapy is indicated for moderate to severe
psoriasis which is not adequately controlled by topical
therapies. During treatment, patients are exposed to
controlled doses of artificial UV radiation which have
local immunosuppressive and anti-inflammatory
actions. Phototherapy is usually administered 2 to 3
times per week for a total of 20 to 25 sessions. About 6
weeks of phototherapy can induce remission that lasts
for 3 to 6 months. Local side effects include itching,
burning, erythema and hyperpigmentation. Long term
cumulative doses may increase the risk of skin cancer.
Systemic Agents
If phototherapy fails, or is contraindicated/unavailable,
a systemic agent is an alternative option for moderate
to severe psoriasis. All systemic agents have serious
side effects, therefore patients should be assessed for
their risk of side effects by baseline laboratory tests
before starting the treatment and are monitored
regularly during treatment. Besides conventional
systemic agents such as methotrexate, acitretin and
cyclosporine, newer biological agents are also
available. Dosage and monitoring of these systemic
agents are listed in Table 3.
Methotrexate is the most commonly prescribed
systemic agent for plaque psoriasis. It is a folate
antagonist that has antiproliferative and
immunosuppressive actions. It is administered either
orally or intramuscularly/subcutaneously once weekly. It
has slow onset of action, taking at least 3 months to
induce remission. Folate supplementation (5mg daily
except on the day of methotrexate dosing) is required to
reduce bone marrow suppression and gastrointestinal
side effects such as nausea and stomatitis. Slow dose
titration and regular blood tests are essential to prevent
hematological and liver toxicity. Methotrexate is
contraindicated in pre-existing blood dyscrasias, liver
disease, severe renal impairment and pregnancy.
Acitretin is an oral vitamin A analogue which has anti-
inflammatory effect and reduces the rate of epidermal
cell turnover. As it is not immunosuppressive, it may be
an alternative treatment for HIV patients with psoriasis
where phototherapy is not feasible. Acitretin is used as
single agent or in combination with topical therapies.
Side effects include hair loss, skin peeling, elevated
fasting blood glucose, hypercholesterolemia and elevated
liver function tests. Women of childbearing age should
avoid pregnancy for at least 1 month before, during and
for at least 3 years after treatment due to teratogenic
effect. Other contraindications include concurrent use
with methotrexate or tetracycline, breastfeeding and
severe liver or renal impairment.
Cyclosporine is an oral calcineurin inhibitor which has
immunosuppressive action. It can rapidly induce
remission in 6 to 12 weeks of treatment and is useful for
resistant plaque psoriasis which is not responding to
methotrexate. Side effects including hypertension, renal
toxicity, hypercholesterolemia, hyperuricemia,
periodontal diseases and malignancy concern usually
limit the duration of cyclosporine therapy to maximum
of 2 years. Cyclosporine is contraindicated in abnormal
renal function, uncontrolled hypertension, malignancies,
and concurrent use with other immunosuppressive
agents, phototherapy or coal tar therapy.
Figure 11
Cabinet for phototherapy
to treat psoriasis that
affects extensive areas

Drug Initial Dose Maintenance dose Monitoring
Methotrexate 2.5-5mg once
weekly
Increased by 2.5 to 5mg
every 2-4 weeks based
on clinical response or
toxicity
Maximum 25mg once
weekly
FBC, LFT, RP
2 weeks after starting
Monthly for the first 3
months, then every 2-3
months
Acitretin 25-30mg once daily
for 2-4 weeks
Adjust based on
response
Usually within 25-50mg
daily
Maximum 75mg daily
LFT, lipid profile
Every 4 weeks until
stable, then every 6-12
weeks
Cyclosporine 2.5mg/kg/day
divided into two
doses
Increased by 0.5mg/kg/
day if insufficient
response after 4 weeks
Additional dose
increases may be made
every 2 weeks if
necessary
Maximum 4mg/kg/day
BP, LFT, RP, lipid
profile
Monthly for the first 3
months, then every 2-3
months
Adalimumab 80mg followed by
40mg 1 week later
40mg every other week Baseline FBC, LFT,
RP, hepatitis test, TB
test
Etanercept 50mg twice weekly
(72-96 hours apart)
for first 3 months
50mg weekly
Infliximab 5mg/kg at 0, 2 and 6
weeks
5mg/kg every 8 weeks
Ustekinumab Patients weighing
≤100kg: 45mg
>100kg: 90mg
Given at week 0 and
4
Same dose given every 12
weeks
Table 3 Dosage and Monitoring of Systemic Agents P A G E 6

Biological agents are monoclonal antibodies that
block specific molecules involved in the
immunologic process of psoriasis such as tumor
necrosis factor alpha (TNF-α) and interleukins.
There are 4 biological agents available in
Malaysia for psoriasis: adalimumab, etanercept
and infliximab which are TNF-α inhibitors, and
ustekinumab which is an interleukin-12 and
interleukin-23 inhibitor. Adalimumab, etanercept
and ustekinumab are administered
subcutaneously while infliximab is administered
as intravenous infusion. Theoretically, they may
be less toxic to the liver, kidney and bone marrow
compared to conventional systemic agents and
need less monitoring. However, they are
expensive and their long term safety profile is not
well-established yet. Therefore, biologic therapy
is only indicated for patients with severe psoriasis
defined by BSA ≥30 or PASI ≥20 or DLQI ≥18
and have failed, intolerance or contraindication to
conventional systemic treatment and
phototherapy. Most patients respond within 4
weeks and show a significant improvement in
symptoms by 12 weeks.
These agents are contraindicated in the
following:
Active infection
Current and/or previous history of
tuberculosis
HIV infection
Hepatitis B/C
Current and/or previous history of
malignancy
Congestive cardiac failure
Demyelinating diseases
Intention to get pregnant
Pregnancy or breast-feeding
Patient who have had prior PUVA (>200
sessions) and UVB (>350 sessions)
1. Ministry of Health Malaysia. Clinical Practice Guideline: Management of psoriasis
vulgaris 2013.
2. Thompson M. Psoriasis. InPHARMation 2012; 13(1): 6-11. Pharmaceutical Society of
Australia.
3. Berth-Jones J. Psoriasis. In: Medical Progress. 2011. Available from: http://
www.mims.com/Malaysia/pub/topic/Medical%20Progress/2011-04/Psoriasis%20 4. Drugs for psoriasis. Australian Medicine Handbook. 2010.
5. Sullivan JR, Preda VA. Treatment for severe psoriasis. Aust Prescr. 2009; 32(1): 14-18.
References
P A G E 7
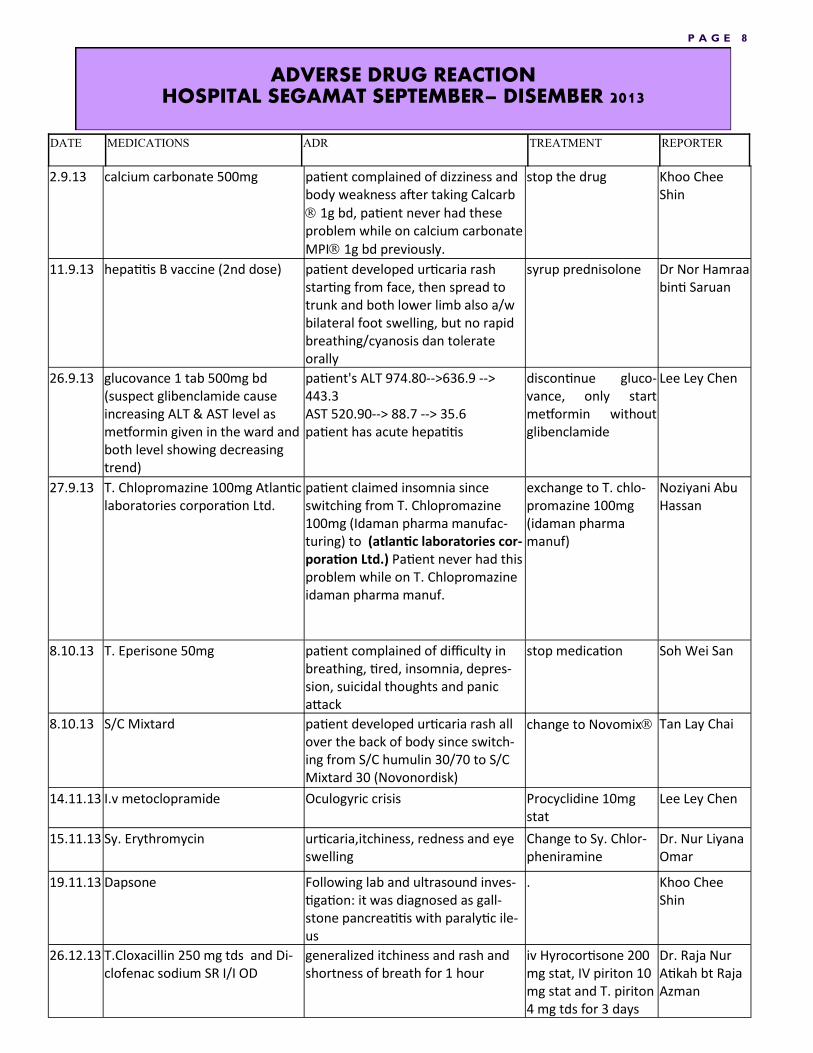
ADVERSE DRUG REACTION HOSPITAL SEGAMAT SEPTEMBER– DISEMBER 2013
DATE MEDICATIONS ADR TREATMENT REPORTER
2.9.13 calcium carbonate 500mg patient complained of dizziness and body weakness after taking Calcarb 1g bd, patient never had these problem while on calcium carbonate MPI 1g bd previously.
stop the drug Khoo Chee Shin
11.9.13 hepatitis B vaccine (2nd dose) patient developed urticaria rash starting from face, then spread to trunk and both lower limb also a/w bilateral foot swelling, but no rapid breathing/cyanosis dan tolerate orally
syrup prednisolone Dr Nor Hamraa binti Saruan
26.9.13 glucovance 1 tab 500mg bd (suspect glibenclamide cause increasing ALT & AST level as metformin given in the ward and both level showing decreasing trend)
patient's ALT 974.80-->636.9 --> 443.3 AST 520.90--> 88.7 --> 35.6 patient has acute hepatitis
discontinue gluco-vance, only start metformin without glibenclamide
Lee Ley Chen
27.9.13 T. Chlopromazine 100mg Atlantic laboratories corporation Ltd.
patient claimed insomnia since switching from T. Chlopromazine 100mg (Idaman pharma manufac-turing) to (atlantic laboratories cor-poration Ltd.) Patient never had this problem while on T. Chlopromazine idaman pharma manuf.
exchange to T. chlo-promazine 100mg (idaman pharma manuf)
Noziyani Abu Hassan
8.10.13 T. Eperisone 50mg patient complained of difficulty in breathing, tired, insomnia, depres-sion, suicidal thoughts and panic attack
stop medication Soh Wei San
8.10.13 S/C Mixtard patient developed urticaria rash all over the back of body since switch-ing from S/C humulin 30/70 to S/C Mixtard 30 (Novonordisk)
change to Novomix Tan Lay Chai
14.11.13 I.v metoclopramide Oculogyric crisis Procyclidine 10mg stat
Lee Ley Chen
15.11.13 Sy. Erythromycin urticaria,itchiness, redness and eye swelling
Change to Sy. Chlor-pheniramine
Dr. Nur Liyana Omar
19.11.13 Dapsone Following lab and ultrasound inves-tigation: it was diagnosed as gall-stone pancreatitis with paralytic ile-us
. Khoo Chee Shin
26.12.13 T.Cloxacillin 250 mg tds and Di-clofenac sodium SR I/I OD
generalized itchiness and rash and shortness of breath for 1 hour
iv Hyrocortisone 200 mg stat, IV piriton 10 mg stat and T. piriton 4 mg tds for 3 days
Dr. Raja Nur Atikah bt Raja Azman
P A G E 8

P A G E 9
V O L U M E 4 / 2 0 1 3
P A G E 1 0
V O L U M E 4 / 2 0 1 3
P A G E 1 1
V O L U M E 4 / 2 0 1 3

FDA Drug Safety Communication: FDA limits usage of
Nizoral (ketoconazole) oral tablets due to potentially fatal
liver injury and risk of drug interactions and adrenal
The U.S. Food and Drug Administration (FDA) is taking several actions related to Nizoral (ketoconazole) oral tablets, including limiting the drug’s use, warning that it can cause severe liver injuries and adrenal gland problems and advising that it can lead to harmful drug interac-tions with other medications. FDA has approved label changes and added a new Medication Guide to address these safety issues. As a result, Nizoral oral tablets should not be a first-line treatment for any fungal infection. Nizoral should be used for the treatment of certain fungal infections, known as endemic mycoses, only when alternative antifungal therapies are not available or tolerated.
The topical formulations of Nizoral have not been associated with liver damage, adrenal prob-
lems, or drug interactions. These formulations include creams, shampoos, foams, and gels ap-
plied to the skin, unlike the Nizoral tablets, which are taken by mouth.
Liver Injury (Hepatotoxicity)
Nizoral tablets can cause liver injury, which may potentially result in liver transplantation or death. FDA has revised the Boxed Warning, added a strong recommendation against its use (contraindication) in patients with liver disease, and included new recommendations for as-sessing and monitoring patients for liver toxicity.
Serious liver damage has occurred in patients receiving high doses of Nizoral for short periods of time as well as those receiving low doses for long periods. Some of these patients had no obvious risk factors for liver disease. The liver injury is sometimes reversible upon stopping the drug, but that is not always possible.
Adrenal Gland Problems (Adrenal Insufficiency)
Nizoral tablets may cause adrenal insufficiency by decreasing the body’s production of hor-mones called corticosteroids. Corticosteroids are produced by the adrenal glands, which are small glands located on top of each kidney. Corticosteroids affect the body’s balance of water and salts and minerals (electrolytes). Health care professionals should monitor adrenal func-tion in patients taking Nizoral tablets who have existing adrenal problems or in patients who are under prolonged periods of stress such as those who have had a recent major surgery or who are under intensive care in the hospital.
V O L U M E 4 / 2 0 1 3 P A G E 1 2

Drug Interactions Nizoral tablets may interact with other drugs a patient is taking and can result in serious and potentially life-threatening outcomes, such as heart rhythm problems. All medications that a patient is currently tak-
ing should be assessed for possible interactions with Nizoral tablets.
In summary, the drug label for Nizoral tablets has been updated to include the following information:
Limitation of the usage of Nizoral tablets by removing indications in which the risk outweighs the ben-efits. The use of ketoconazole tablets in Candida and dermatophyte infections is no longer indicated. Nizoral tablets should be used only when other antifungal drugs are not available or tolerated by the pa-tient.
Nizoral tablets are indicated only for the treatment of the following fungal infections: blastomycosis, coccidioidomycosis, histoplasmosis, chromomycosis, and paracoccidioidomycosis in patients in whom other treatments have failed or who are intolerant to other therapies.
Nizoral tablets are not indicated for the treatment of fungal infections of the skin or nails.
A new contraindication that Nizoral tablets should not be used in patients with acute or chronic liver disease.
For more information, please review: http://www.fda.gov/Drugs/DrugSafety/ucm362415.htm
Pegawai Farmasi U41 (FRP)
1) Mira Marina Binti Mahfodz
2) Wan Farhah Adiba Binti Wan Abd Ghafar
3) Tan Yew Jin
Pegawai Farmasi U41 (PRP)
1) Noorul Atiqah bt. Ibrahim
2) Chin Mei Ping
3) Norliana Bt Rosli 4) Ummu Zahidah Bt Abu Bakar
5) Syahrina Bt Syahlan
6) Noor Syafika Bt Mohd Ibrahim
7) Zulaikha Bt Ramlee
8) Mohd Azmer B Lias
9) Ahmad Fawwazuddin B. Rozaki 10) Nur Izzati Dhamirah Bt Mohd Yusof
11) Nur Syahirah Bt Abd Raof
Noorulhida Bt. Ishak
for her newnborn baby
P A G E 1 3 V O L U M E 4 / 2 0 1 3

.
ACTIVITIES OF PHARMACY
DEPARTMENT
One booth was opened on Diabetes day
( 18.2.2013)
by pharmacy department to educate patients
about diabetes and its management.
Pharmacists explain to the
participant about diabetes dis-
ease and its management.
Some quiz and gifts also
provided for
participant who can answer
questions correctly.
V O L U M E 4 / 2 0 1 3 P A G E 1 4

P A G E 1 5
V O L U M E 4 / 2 0 1 3