Bowel Adhesions: detecting the hidden evil...Adhesions: Facts not fiction • The most frequent...
29
BOWEL ADHESIONS: DETECTING THE HIDDEN EVIL Paul Tung, D.O. Michael Mousa, MD Roozbeh Houshyar, MD Chandana Lall, MD
Transcript of Bowel Adhesions: detecting the hidden evil...Adhesions: Facts not fiction • The most frequent...

BOWEL ADHESIONS: DETECTING THE HIDDEN EVIL
Paul Tung, D.O.
Michael Mousa, MD
Roozbeh Houshyar, MD
Chandana Lall, MD
Disclosure
Authors do not have any financial or other relevant disclosures.

Clustered bowel Segments
Coronal contrast enhanced CT image shows closely clustered small bowel loops in the right lower quadrant consistent with
high grade entero-enteric adhesions (green arrows) . No thickened overlying peritoneum to suggest abdominal cocoon.
Clustered or unusual crowded appearance of bowel
segments is typically seen with entero-enteric or
inter-loop adhesions, classically referred to as
“matted bowel”.
This finding has a high predictive value for bowel
adhesions.
This finding can also be seen with intra-abdominal
infections such as with abdominal tuberculosis.

Overview & Content Organization
– Review the etiologies, timeline and clinical significance of bowel adhesions
– Complications that can result secondarily
– Review spectrum of imaging findings related to bowel adhesions on multi-detector computed
tomography (MDCT) and MRI
– Emphasis on recognition of specific patterns and signs for bowel adhesions
– Assessment of severity as pertains to future risk of obstruction and possible bowel injury
during surgical procedures, due to underlying adhesions
• Role of the radiologist in identifying & reporting significant adhesions

Adhesions: Facts not fiction
• The most frequent cause of abdominal adhesions is abdominal surgery. Other etiologies include
trauma, peritoneal dialysis, infection such as tuberculosis
• Almost all patients who undergo abdominal surgery will develop adhesions of varying degree;
minimal to significant
• The risk is greater after lower abdomen and pelvic surgeries when compared to upper abdominal
surgeries eg: bowel & gynecologic procedures
• IMPORTANT POINT: Adhesions can become larger and tighter over time causing problems,
years after surgery

• Causes of abdominal adhesions include surgery and contact of tissues with foreign materials, such as
gauze, surgical gloves, and sutures as well as retained blood
– Gynecological surgeries, such as hysterectomy, are more prone to adhesion development
than most general abdominal surgeries
• A less common cause is inflammation such as ruptured appendicitis, inflammatory bowel disease,
abdominal TB and other infections, radiation treatment for cancer among others
• Rarely, abdominal adhesions form without apparent cause, ie de novo!
CAUSES OF BOWEL ADHESIONS

Types of bowel adhesions on cross-sectional imaging
Entero-Enteric
Adhesions between
adjacent bowel
loops
Entero-Visceral
Adhesions between
bowel and adjacent
organs
Entero-peritoneal
or Entero-Parietal
Adhesions between
bowel and parietal
peritoneum
Bowel Findings of Adhesions
1. Unchanged location of bowel segments on successive exams(inertia)
2. Loss of fat planes behind the rectus sheath and anterior peritoneum
3. Focal clustering or crowding of bowel loops
4. Kinking and angulation of bowel loops
5. Caliber change of bowel
6. Asymmetric thickness of the bowel wall
7. Fat notch sign
8. Localized stasis within bowel segments
9. “Star sign” of adhesions which may also signify underlying fistulization
10. Enteric-Organ adhesions

Mesenteric Findings
of underlying
adhesions
Focal increased
attenuation of
mesentery
Mesenteric Vascular
crowding Focal localized fluid

Peritoneal Changes associated with Adhesions
Focal or diffuse peritoneal thickening and enhancement
Peritoneal calcifications and Sclerosing Peritonitis
Loculated fluid in between loops of bowel
Peritoneal inclusion cyst

Entero-peritoneal adhesions with unchanged bowel location over time
Axial CT images were obtained almost 2 years apart : Note location of small bowel loops in the same
location, abutting the right anterior abdominal wall with obliteration of the right post-rectus fat plane (yellow
arrows). Normal left post rectus fat plane( green arrows)
CT: 3/2/14 CT: 11/7/15

Loss of fat planes posterior to the rectus sheath and anterior peritoneum
Normal bowel segments are nearly
always separated from the posterior
aspect of the rectus muscles by
mesenteric and omental fat. Following
intra-abdominal and pelvic surgeries,
the tissue disturbance at the level of
the visceral peritoneum results in
closely applied adherence of the small
bowel with resultant loss of the retro-
rectus fat planes.
50 year old female patient status post cholecystectomy, shows unchanged location of bowel loops along the anterior
peritoneum on studies over a period of 9 months with loss of posterior rectus sheath fat plane (yellow arrows).

Clustered bowel Segments
Coronal contrast enhanced CT image shows closely clustered small bowel loops in the right lower quadrant consistent with
high grade entero-enteric adhesions (green arrows) . No thickened overlying peritoneum to suggest abdominal cocoon.
Clustered or unusual crowded appearance of bowel
segments is typically seen with entero-enteric or
inter-loop adhesions, classically referred to as
“matted bowel”.
This finding has a high predictive value for bowel
adhesions.
This finding can also be seen with intra-abdominal
infections such as with abdominal tuberculosis.

Clustered bowel loops
60 year-old female patient status post hysterectomy. Contrast enhanced axial and sagittal CT images
show shows matted bowel loops clustered in the lower abdomen & pelvis (green arrows)

Kinking and Angulation of Bowel Loops
42 year old female status post hysterectomy, 3 years ago, presenting with chronic lower abdominal pain. Axial CT images
demonstrate acute angulation and kinking of multiple bowel loops (red arrows).
One of the most common signs of bowel
adhesions is acute angulation of bowel.
Normal small bowel being freely mobile
normally shows smooth curved loops
usually evenly distributed in the abdomen
and pelvis. With development of either
entero-enteric adhesions or entero-parietal
adhesions, loops become fixed at certain
points, leading to acutely angulated
segments with kinking and changes in
caliber as seen in these images
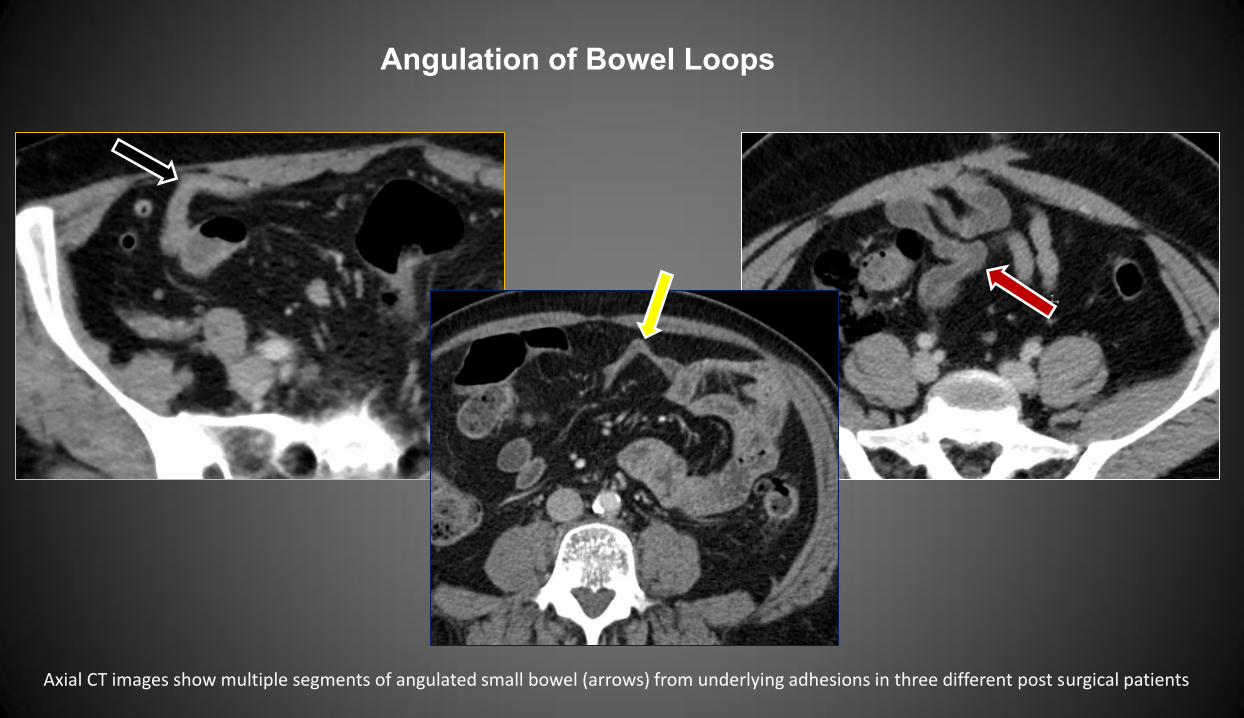
Angulation of Bowel Loops
Axial CT images show multiple segments of angulated small bowel (arrows) from underlying adhesions in three different post surgical patients

Caliber change of bowel and Localized stasis within bowel
Coronal CT image demonstrates focal caliber change of a small bowel loop in the mid abdomen (white
arrow) with fecalized material present proximal to the caliber change (red arrows).
Bowel adhesions may lead to caliber
change of the bowel with slow transit times
in focal segments of bowel. These
segments may demonstrate features of
stasis including fluid accumulation and
fecalized appearance of small bowel loops.
Finding of localized stasis may be an
indirect sign of unsuspected underlying
bowel adhesions.
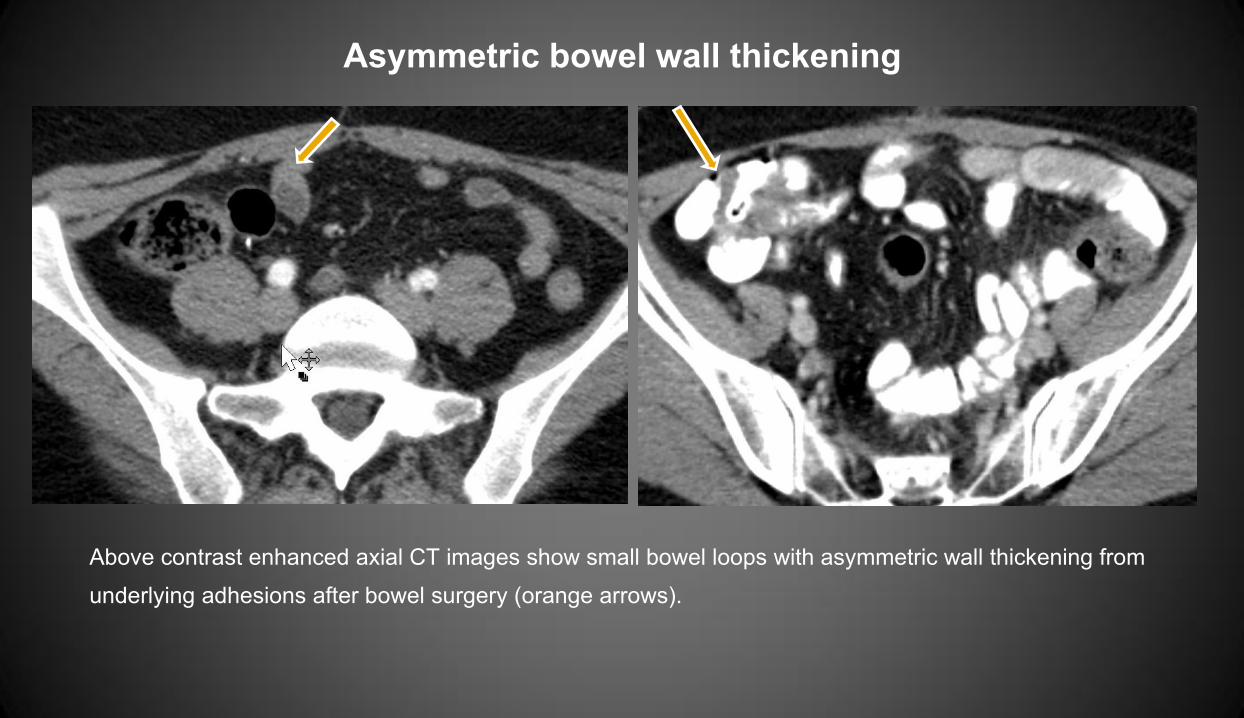
Asymmetric bowel wall thickening
Above contrast enhanced axial CT images show small bowel loops with asymmetric wall thickening from
underlying adhesions after bowel surgery (orange arrows).

Fat notch sign
44 year old female with past surgical history of hysterectomy presented with abdominal pain, nausea and vomiting. Axial CT
image demonstrates a fat indentation at level of adhesion, the “fat notch” sign ( arrow) along with associated dilated loops of
small bowel.
This sign reflects
insinuation of mesenteric
fat at an area of adhesions
with focal caliber change.
This has been described in
cases of small bowel
obstruction related to
adhesions and is a very
specific finding of adhesive
small bowel obstruction.
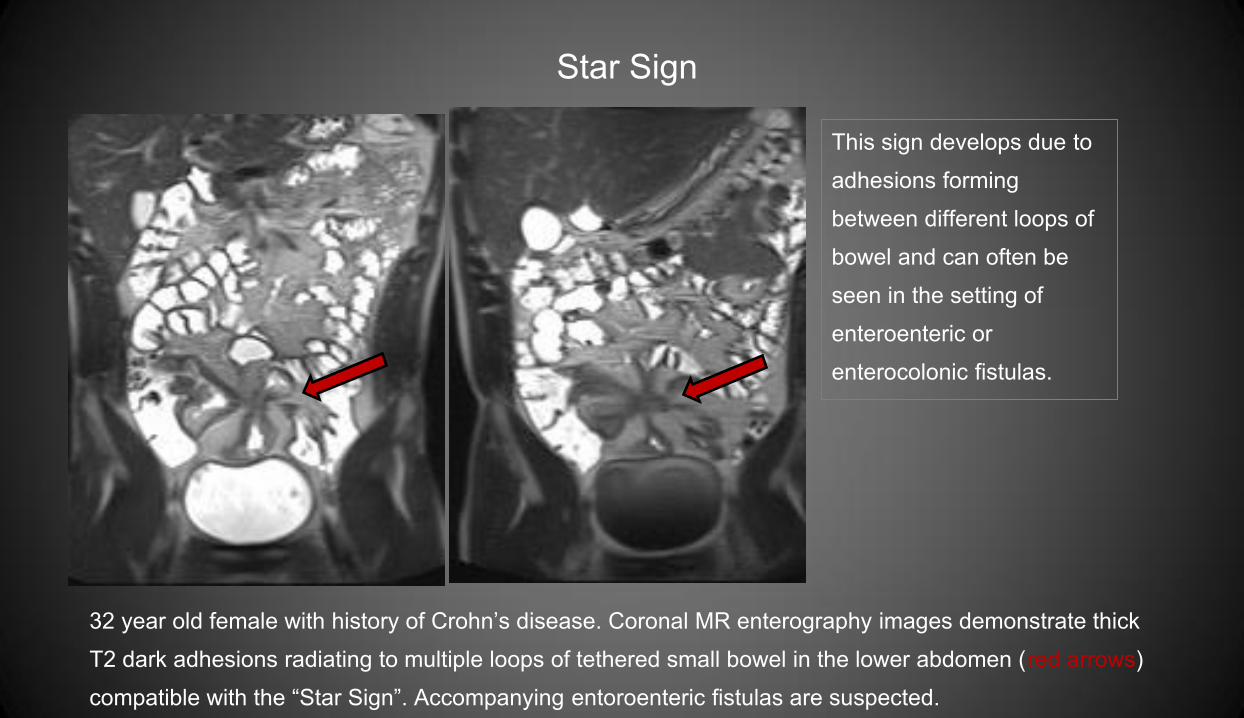
Star Sign
32 year old female with history of Crohn’s disease. Coronal MR enterography images demonstrate thick
T2 dark adhesions radiating to multiple loops of tethered small bowel in the lower abdomen (red arrows)
compatible with the “Star Sign”. Accompanying entoroenteric fistulas are suspected.
This sign develops due to
adhesions forming
between different loops of
bowel and can often be
seen in the setting of
enteroenteric or
enterocolonic fistulas.
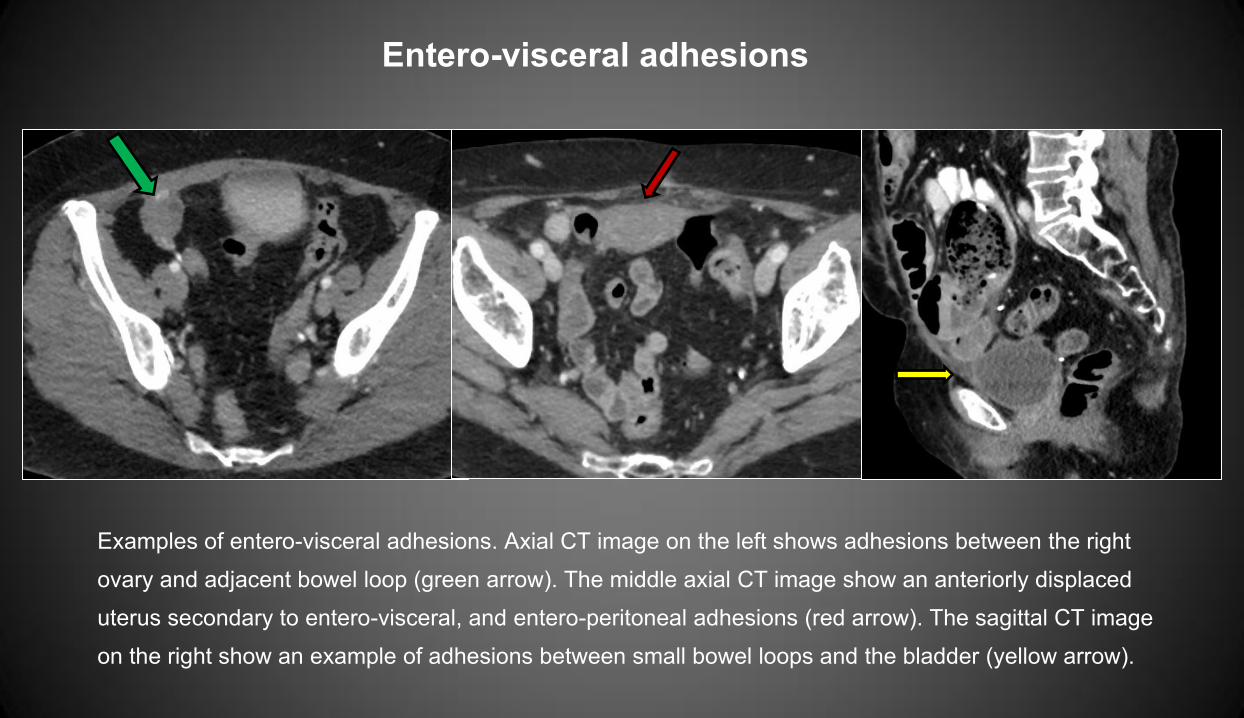
Entero-visceral adhesions
Examples of entero-visceral adhesions. Axial CT image on the left shows adhesions between the right
ovary and adjacent bowel loop (green arrow). The middle axial CT image show an anteriorly displaced
uterus secondary to entero-visceral, and entero-peritoneal adhesions (red arrow). The sagittal CT image
on the right show an example of adhesions between small bowel loops and the bladder (yellow arrow).
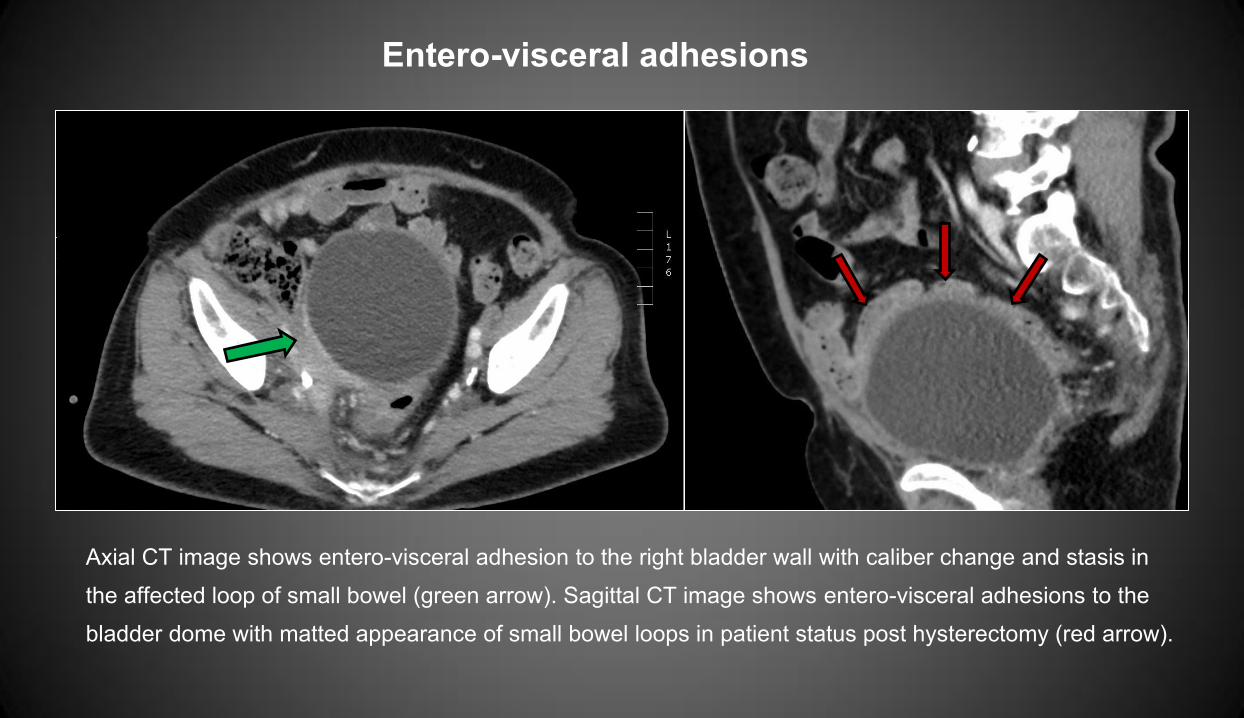
Entero-visceral adhesions
Axial CT image shows entero-visceral adhesion to the right bladder wall with caliber change and stasis in
the affected loop of small bowel (green arrow). Sagittal CT image shows entero-visceral adhesions to the
bladder dome with matted appearance of small bowel loops in patient status post hysterectomy (red arrow).

Focal increased attenuation of the Mesentery
Axial contrast enhanced CT images show localized increase in mesenteric attenuation in the right abdomen
when compared to normal mesenteric fat in the left abdomen, related to mesenteric congestion (red arrow)
secondary to underlying adhesions.

Mesenteric Vascular Crowding Associated with Adhesions
Axial contrast enhanced CT image on the right and coronal MR enterography image show localized vascular
crowding in the right abdomen related to mesenteric congestion (red arrows) secondary to underlying small bowel
adhesions.

Cocoon Abdomen
56 year old male, status post colonic surgery presents with abdominal pain and vomiting. Axial and coronal CT images
demonstrate a cluster of adherent fluid filled mildly dilated small bowel loops in pelvic region, enclosed by thickened
peritoneal lining ( red arrows), consistent with “cocoon abdomen” (green arrows).
Cocoon abdomen refers to
closely clustered bowel loops
adherent within thickened
peritoneum in a sac like manner.
This finding is classically
associated with peritoneal
dialysis, with presence of
underlying entero-parietal and
entero-enteric adhesions.
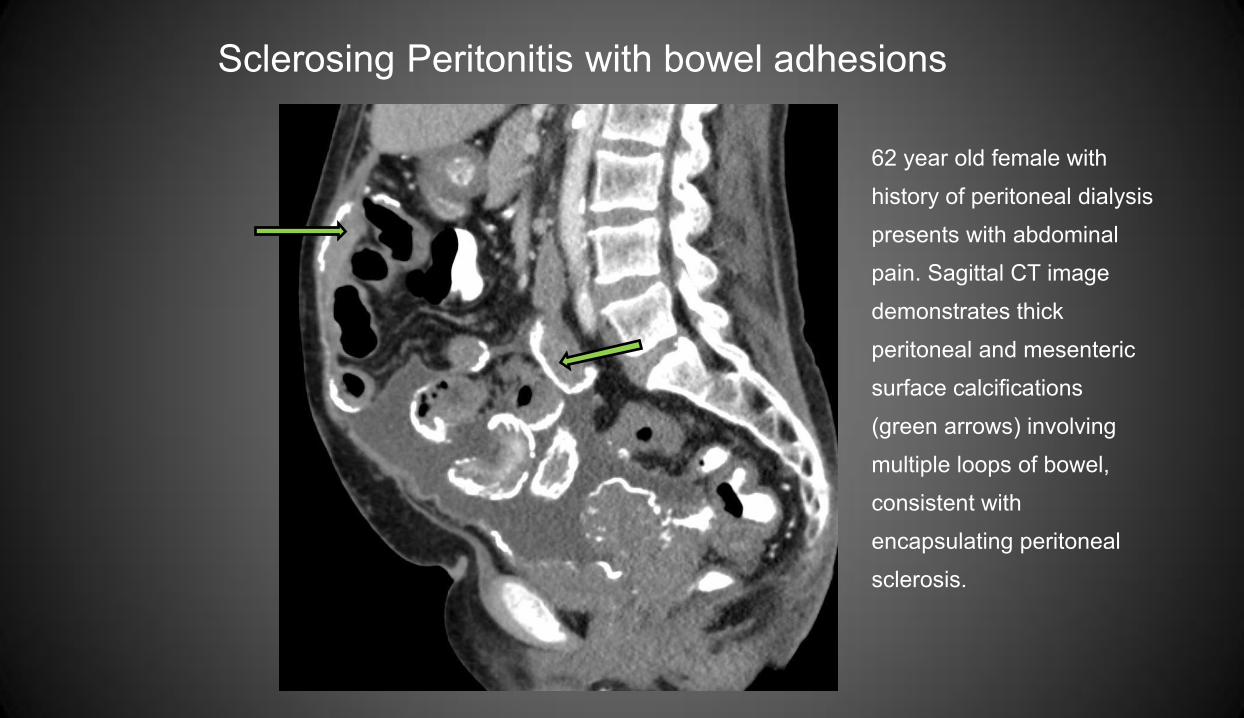
Sclerosing Peritonitis with bowel adhesions
62 year old female with
history of peritoneal dialysis
presents with abdominal
pain. Sagittal CT image
demonstrates thick
peritoneal and mesenteric
surface calcifications
(green arrows) involving
multiple loops of bowel,
consistent with
encapsulating peritoneal
sclerosis.
CONCLUSION
• It is essential for radiologist to recognize the varied imaging findings and specific signs
related to presence of bowel adhesions
• Radiologists should mention the presence of non-obstructing bowel adhesions, since this
has direct implications when future surgeries, especially laparoscopic procedures are
being considered, due to high risk of inadvertent bowel injury and prolonged surgical time
• Adhesions are the most common cause of small bowel obstruction!
• Adhesions can also result in infertility and chronic abdominal pain among other issues
References 1. Cheong YC, Laird SM, Li TC, Shelton JB, Ledger WL, Cooke ID. Peritoneal healing and adhesion formation/reformation. Human reproduction update. 2001;7(6):556-66.
2. Arung W, Meurisse M, Detry O. Pathophysiology and prevention of postoperative peritoneal adhesions. World journal of gastroenterology : WJG. 2011;17(41):4545-53.
3. Ellis H. The clinical significance of adhesions: focus on intestinal obstruction. The European journal of surgery Supplement : = Acta chirurgica Supplement. 1997(577):5-9.
4. Diamond MP, Freeman ML. Clinical implications of postsurgical adhesions. Human reproduction update. 2001;7(6):567-76.
5. Sulaiman H, Gabella G, Davis MC, Mutsaers SE, Boulos P, Laurent GJ, et al. Presence and distribution of sensory nerve fibers in human peritoneal adhesions. Annals of
surgery. 2001;234(2):256-61.
6. Attard JA, MacLean AR. Adhesive small bowel obstruction: epidemiology, biology and prevention. Canadian journal of surgery Journal canadien de chirurgie.
2007;50(4):291-300.
7. Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL. Peritoneal adhesions: etiology, pathophysiology, and clinical significance. Recent advances in prevention and
management. Digestive surgery. 2001;18(4):260-73.
8. Menzies D, Ellis H. Intestinal obstruction from adhesions--how big is the problem? Annals of the Royal College of Surgeons of England. 1990;72(1):60-3.
9. Monk BJ, Berman ML, Montz FJ. Adhesions after extensive gynecologic surgery: clinical significance, etiology, and prevention. American journal of obstetrics and
gynecology. 1994;170(5 Pt 1):1396-403.
10. Ray NF, Denton WG, Thamer M, Henderson SC, Perry S. Abdominal adhesiolysis: inpatient care and expenditures in the United States in 1994. Journal of the American
College of Surgeons. 1998;186(1):1-9.
11. Gutt CN, Oniu T, Schemmer P, Mehrabi A, Buchler MW. Fewer adhesions induced by laparoscopic surgery? Surgical endoscopy. 2004;18(6):898-906.
12. Zbar RI, Crede WB, McKhann CF, Jekel JF. The postoperative incidence of small bowel obstruction following standard, open appendectomy and cholecystectomy: a six-
year retrospective cohort study at Yale-New Haven Hospital. Connecticut medicine. 1993;57(3):123-7.
13. Moinuddin Z, Summers A, Van Dellen D, Augustine T, Herrick SE. Encapsulating peritoneal sclerosis-a rare but devastating peritoneal disease. Frontiers in physiology.
2014;5:470.
14. Catel L, Lefevre F, Lauren V, Canard L, Bresler L, Guillemin F, et al. [Small bowel obstruction from adhesions: which CT severity criteria to research?]. Journal de
radiologie. 2003;84(1):27-31.

Thank you for viewing!