
Borderline Personality Disorder Milton Brown Behavioral Research & Therapy Clinics University of...
44
Borderline Personality Disorder Milton Brown Behavioral Research & Therapy Clinics University of Washington
-
Upload
felix-thomas-wiggins -
Category
Documents
-
view
218 -
download
1
Transcript of Borderline Personality Disorder Milton Brown Behavioral Research & Therapy Clinics University of...

Borderline Personality DisorderMilton Brown
Behavioral Research & Therapy ClinicsUniversity of Washington

Borderline Personality Disorder
• What is BPD?
• How to assess BPD
• How does BPD develop?
• BPD in adolescence
• Intervention options
• How to respond to challenging BPD clients

What is a Personality Disorder? DSM-IV diagnostic criteria
A. An enduring pattern of inner experience and behavior that deviates markedly from the expectations of the individual’s culture. This pattern is manifested in two (or more) of the following areas:
(1) cognition (i.e., ways of perceiving and interpreting self, other people, and events)
(2) affectivity (i.e., the range, intensity, lability, and appropriateness of emotional response)
(3) interpersonal functioning
(4) impulse control

B. The enduring pattern is inflexible and pervasive across a broad range of personal and social situations
C. The enduring pattern leads to clinically significant distress or impairment in social, occupational, or other important areas of functioning
D. The pattern is stable and of long duration, and its onset can be traced back at least to adolescence or early adulthood
E. The enduring pattern is not better accounted for as a manifestation or consequence of another mental disorder
F. The enduring pattern is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., head trauma).
What is a Personality Disorder? DSM-IV diagnostic criteria
1. Frantic efforts to avoid real or imagined abandonment. Note: Do not include suicidal or self-mutilation behavior covered in Criterion 5
2. A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation
3. Identity disturbance markedly and persistently unstable self-image or sense of self
4. Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating). Note: Do not include suicidal or self-mutilation behavior covered in Criterion 5
Borderline Personality Disorder DSM-IV diagnostic criteria

5. Recurrent suicidal behavior, gestures, or threats, or self-mutilation
6. Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days)
7. Chronic feelings of emptiness8. Inappropriate, intense anger or difficulty
controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights)
9. Transient, stress-related paranoid ideation or severe dissociative symptoms
Borderline Personality Disorder DSM-IV diagnostic criteria

BPD is Prevalent and Chronic
Prevalence• 16% of adolescents• 10% of adults
Stability• 25% of adolescents still have BPD after 2 years
– 53% of severe BPD cases
• 60% of adults still have BPD after 6 years• 35% of adults still have BPD after 15 years

What is BPD
• The multidiagnostic, difficult-to-treat patient
• Chronic suicidality and self-harm
• A diverse patient population

Parasuicidal Behaviors in BPD
• 75% have a history of parasuicide• 10% lifetime suicide rate*• more repeated suicide attempts than other disorders• more likely to have persistent and intense suicide
ideation between parasuicide episodes, whereas…• individuals with only depression are more likely to
have long periods of normal mood and episodic suicide ideation/behavior.
• nonsuicidal self-injury is common in BPD, and rare in most other disorders (except mental retardation).

Diagnosis Lifetime Current
Depressive disorder* 97% 89%Substance abuse/depend. 60%* 31%PTSD 57% 51%Social phobia 22% 16%Panic disorder 52% 40%Eating disorder 41% 24%Antisocial PD - 11%Avoidant - 21%
Diagnoses for Parauicide Study

Diagnosis Current
Depressive disorder 39%Any anxiety disorder 52%Eating disorder 18%Antisocial PD 44%
Diagnoses for Substance Abuse Study
Diagnosis Current
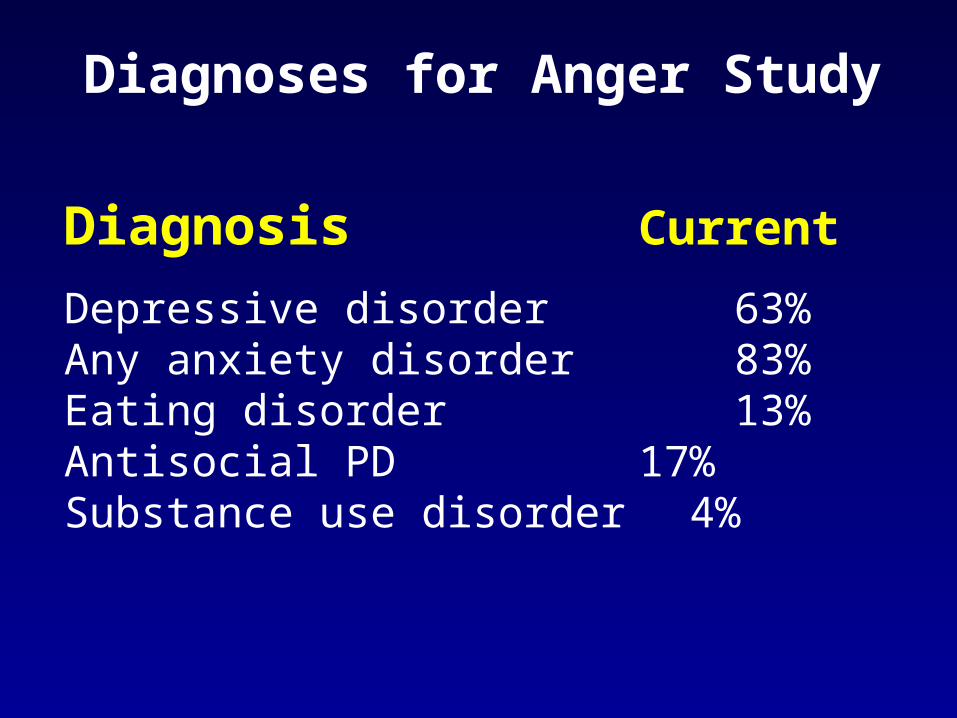
Depressive disorder 63%Any anxiety disorder 83%Eating disorder 13%Antisocial PD 17%Substance use disorder 4%
Diagnoses for Anger Study

The Core of BPD
• Emotion dsyregulation– High sensitivity– High intensity– Slow return to baseline– Pervasiveness– Chronicity
• Impulsive behaviors– Because emotions are “out of control”– Because the behaviors regulate emotions
• Pervasive experiential avoidance

Borderline Personality Disorder
EMOTION DYSREGULATION
Cognitive Dysregulation
Action DysregulationSelf
DysregulationInterpersonalDysregulation
Suicidal Action
-Death-Distraction-Sleep-Biochemical-Cue Removal

The Client’s View
Emotion DysregulationEmotion Dysregulation= Problem Behavior= Problem Behavior
Emotion DysregulationEmotion Dysregulation= Problem Behavior= Problem Behavior
Dysfunctional Behavior Dysfunctional Behavior = Problem Solution = Problem Solution
Dysfunctional Behavior Dysfunctional Behavior = Problem Solution = Problem Solution
CueCue
ConsequenConsequencesces

Basic ParadigmCueCue
ConsequenConsequencesces
Emotion Emotion DysregulatiDysregulati
ononProblem Problem BehaviorBehavior
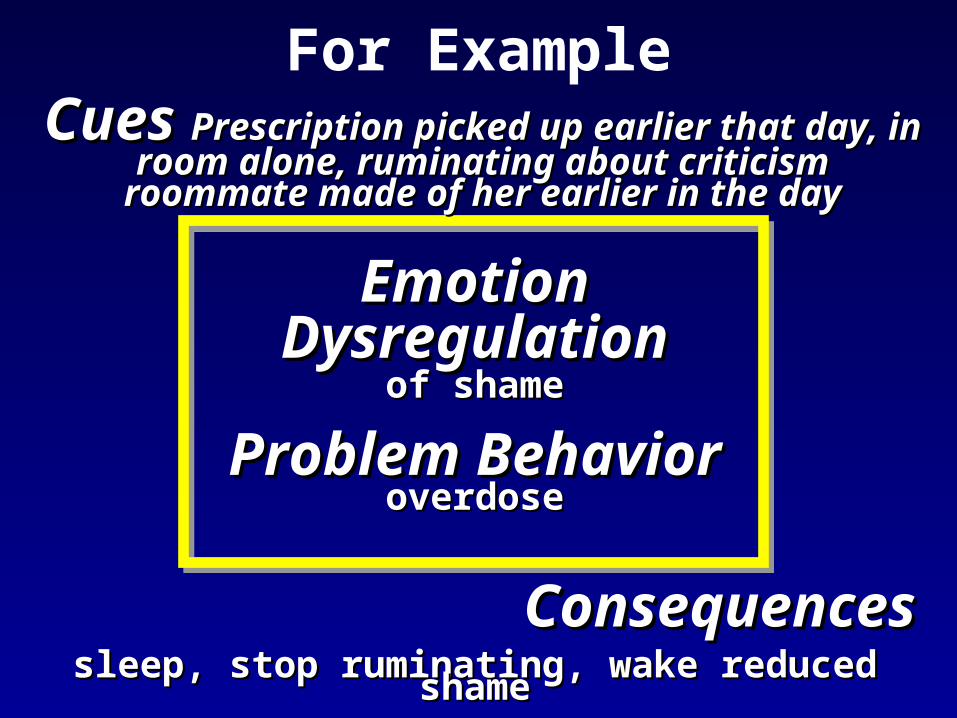
For ExampleCues Cues Prescription picked up earlier Prescription picked up earlier that day, in room alone, ruminating that day, in room alone, ruminating
about criticism roommate made of her about criticism roommate made of her earlier in the dayearlier in the day
ConsequencesConsequencessleep, stop ruminating, wake reduced sleep, stop ruminating, wake reduced
shameshame
Problem Problem Behavior Behavior
overdoseoverdose
Emotion Emotion DysregulatioDysregulatio
n n of shameof shame

Methods of Experiential Avoidance
Denial of problems (rather than problem-solving)
Dissociation and emotional numbing
Isolation
Drug and alcohol abuse
Suicide attempts (and suicide)
Nonsuicidal self-injury
Self-punishment, self-criticism
Secondary emotions to avoid primary emotions
Hospitalization to escape stressful circumstances
Reasons for Parasuicide
Emotion Relief (92%, at least one)• To stop bad feelings• To stop feeling angry or frustrated or enraged• To relieve anxiety or terror• To relieve feelings of aloneness, emptiness or
isolation• To stop feeling self-hatred, shame• To obtain relief from a terrible state of mindTo punish yourself (63% of nonsuicidal self-injury)

Development of BPD
BPD becomes noticeable in early adolescence, but begins long before that.
• A “difficult” temperament may be a sign of vulnerability during infancy
• Suicidal ideation, threats, and behavior during childhood and adolescence
• Conduct disorder, antisocial behavior, mood disorders, anxiety disorders
• 16% of adolescents meet BPD criteria

Development of BPDEnvironmental Factors
Pathological parenting is an important risk factor.
• emotional neglect
• parental over-involvement*
• inconsistent care by a primary caretaker*
• disrupted attachment patterns
• parental psychopathology
• physical and sexual abuse
• early separation and loss?

Development of BPDBiological Correlates
Biological correlates of emotional instability and impulsivity have been identified
• Patients with emotional instability may have higher levels of noradrenaline activity
• Patients with impulsive disorders may have lower levels of serotonin activity.
• Patients with major depressive disorder and BPD both have shorter and more variable REM latencies.
• Some brain differences have been found in BPD.• A twin study supports a psychosocial model more
than a genetic model of BPD transmission.
Development of BPD Linehan’s Biosocial Theory (1993)
Biological and environmental factors account for BPD.• BPD individuals are born with emotional vulnerability
– highly sensitive to emotional stimuli– more intense in their emotional reactions– slower to return to their emotional baseline
• BPD individuals grow up in invalidating environments– childhood abuse– poorness-of-fit between the child and the family
• Transactions between biological vulnerabilities and an invalidating environment lead to a dysfunction in the emotion regulation system.
Development of BPD Linehan’s Biosocial Theory (1993)
The path to BPD is a process of reciprocal influences.
• invalidating environments worsen dysregulation of vulnerable children.
• emotionally intense children may exacerbate the invalidating environment.
• mutual coercion can escalate emotion, violence, and self-harm.
Does it make sense to diagnose BPD in adolescence?
• BPD in adolescents accurately reflects current distress and dysfunction– Social impairment/isolation– School problems– Work problems– Comorbid axis I diagnosis– Contact with police for antisocial behavior
• As expected, BPD co-occurs with PTSD, conduct disorder, depression (construct validity)
• Overall, BPD diagnosis is not stable• 53% of moderate/severe cases of BPD persist
What to look for
• Caucasian female
• Severe BPD (predicts chronicity)
• Parasuicide, identity disturbance, intense anger (predicts chronicity)
• Co-occurring mood and conduct disorder
• Bipolar II disorder
• History of childhood maltreatment

Disability in BPD
• What are the functional limitations?
• What are reasonable accommodations in academic settings?

Treatment Options:The Main Dialectic
Short-term Long-termavoid stress block avoidance
tolerate distressremove cues challenge fearsisolation build a structured lifedistraction problem-solving
focus on emotionshospitalization alternative coping

An Ideal Treatment for BPD
is one that balances…
Acceptance and Change
Soothing versus pushing the client
Validation versus demanding

Most Good Treatments Don’t Work for BPD
BPD has been associated with worse outcomes in treatments of Axis I disorders such as
• major depression• anxiety disorders• eating disorders• substance abusebecause BPD patients have low tolerance for
change in the absence of validation

Treatment Goals
• Reduce out of control behavior• Build a structured/productive life consistent
with values• Change (increase tolerate for) emotions• Treat Axis I disorders• Treat effects of childhood trauma• Personal goals

Treatment Objectives
• Enhance capabilities• Reduce emotion vulnerability• Activate non-mood-dependent behavior• Enhance motivation• Generalization• structuring of the environment • Enhance capability and motivation of therapists
Treatment Strategies
Intervene early before maladaptive patterns become crystallized and refractory to treatment.– Problem-solving– Skills-focus*– Exposure and opposite action– Reinforcement– Cognitive modification– Support/Validation/Acceptance– Keep lethal means out of reach (e.g., pills)

Treatment of BPD:Commitment to not parasuicide
Verbal commitmentCommitment strengthening
Devil's advocateMotivational interviewingPros and cons analysis
Provide helpProvide incentives for no parasuicide

Problem-Solving
1. Understand the problem1. Identify the trigger (event)2. Identify the key emotions and thoughts3. What problem did the behavior solve?
2. Generate alternative solutions3. Practice solutions
Treatment of BPDSignificant Outcomes from DBT Study:
DBT vs. TAU
1. Parasuicide Episodes2. Treatment Drop Out3. Psychiatric Inpatient: Admissions/Days4. Anger5. Global Adjustment6. Social Adjustment
Treatment of BPD
• Effects of DBT were similar to the previous study despite– rigorous control condition of expert therapists
– high allegiance to the alternative treatment
• DBT is effective in six randomized controlled trials• DBT is particularly effective with suicidal behavior• Expert therapists are better than treatment as usual
UW Replication Study

Ways to fail with a BPD client
• Insufficient validation
• Judgmental attitude toward client
• Burnout
• Insight therapy
• Back down too easily
• Reinforce dysfunctional behavior
• No learning in context

How should a provider interact with a BPD client?
• Validate and acknowledge what is valid
• Adopt a compassionate and nonjudgmental view of the patient
• Don’t ignore your personal or institutional limits, but stay objective
• Believe in the patient
• Encourage mastery; provide practical help
• Get support and consultation

Levels of Validation
• Listen and pay attention• Show you understand – paraphrase• Communicate how their behavior/emotions
make sense– given their past experiences– given their thoughts/beliefs
• Communicate how their behavior/emotions are normal or make sense now
• Don’t “fragilize” them or treat them like a patient

When to Refer
• When the client’s problems exceed your skill
• When you are approaching burnout
• If you cannot control judgmental thinking about the client
• If the client does not improve

Medications for BPD
• SSRIs improve mood and impulsivity– May reduce nonsuicidal self-injury– May increase suicide attempts*
• Olanzapine improves irritability/anger• Anticonvulsants (Tegritol) decrease behavioral
dyscontrol• Alprazolam (Xanax) increases behavioral
dyscontrol and suicidality ratings• Opiate blockers
Medication Recommendations
• Combine pharmacotherapy with an active psychosocial treatment
• Focus on safety and effectiveness– Do not give lethal drugs to lethal people– Avoid benzodiazepines– Amitriptyline makes some subjects worse
• Attend to medication non-compliance• Consult with the patient

Medications for BPD
Dimeff, L.A., McDavid, J., Linehan, M.M. (1999). Pharmacotherapy for borderline personality disorder: A review of the literature and recommendations for treatment. Journal of Clinical Psychology in Medical Settings, 6(1), 113-138.
Grossman, R. (2002). Psychopharmacologic treatment of patients with borderline personality disorder. Psychiatric Annals, 32(6), 357-370.
Healy, D. (2003). Lines of evidence on the risks of suicide with selective serotonin reuptake inhibitors. Psychotherapy and Psychosomatics, 72(2), 71-79.


















