Bone infection dina patho
30
-
Upload
dina-alshayaa -
Category
Health & Medicine
-
view
41 -
download
0
Transcript of Bone infection dina patho

Proliferative periostitis. Cellular and reactive vital bone with individual trabeculae oriented perpendicular to the surface.

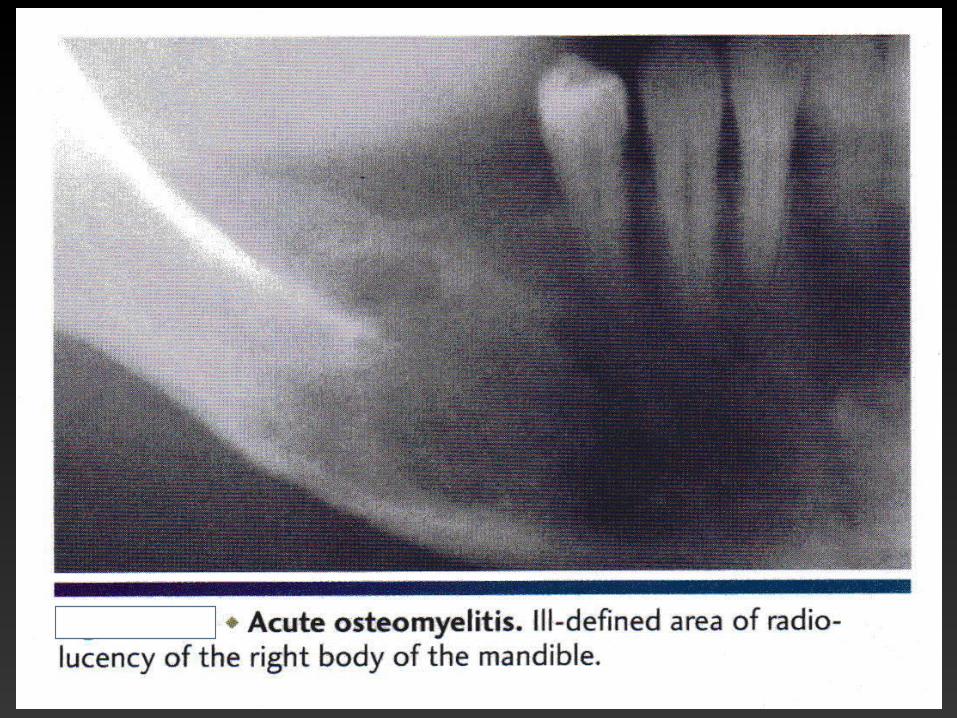
Chronic osteomyelitis, ill-defined area of radiolucency of the right body of the mandible
adjacent to a recent extraction site.
B, after the initial intervention. The patient failed to return for follow-up because of lack of
significant pain. An enlarged, ill-defined radiolucency of the
right body of the mandible was discovered 2 years after the initial surgery.
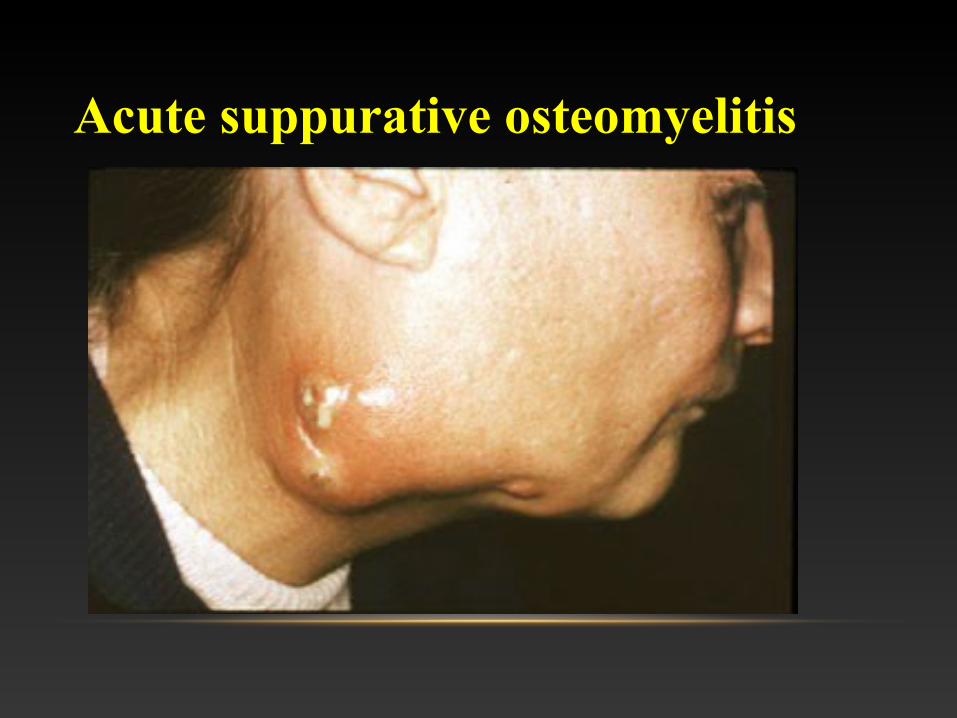
Acute suppurative osteomyelitis

Acute osteomyelitis with sequestrum. Radiolucencyof the right body of the mandible with central radiopaque massof necrotic bone.

CHRONIC OSTEOMYELITIS IN RADIATED MANDIBLE.

Chronic osteomyelitis of the mandible associated with periodontal disease. Note moth-eaten radiolucentappearance.


CHRONIC OSTEOMYELITIS OF THE MANDIBLE

CHRONIC OSTEOMYELITIS IN THE REGION OF THIRD-MOLAR EXTRACTION.

Acute steomyelitis. Nonvital bone exhibits loss of the osteocytes from the lacunae. Peripheral resorption. Bacterial colonization. And surrounding inflammatory response also can be seen .

CHRONIC OSTEOMYELITIS SHOWING FIBROUS MARROW AND OSTEOCLASTIC RESORPTION OF RESIDENT BONE.


Late-stage chronic osteomyelitis. A sequestrum trapped in acavity within the bone. It is surrounded by fibrous tissue containing aninfiltrate of inflammatory cells. Surgical intervention is needed to removean infected sequestrum such as this.

High power view of a sequestrum showing non-vital bone (theosteocyte lacunae are empty), and eroded outline with superficial lacunaeproduced by osteoclastic resorption, and a dense surface growth ofbacteria.

FOCAL SCLEROSING OSTEITIS.

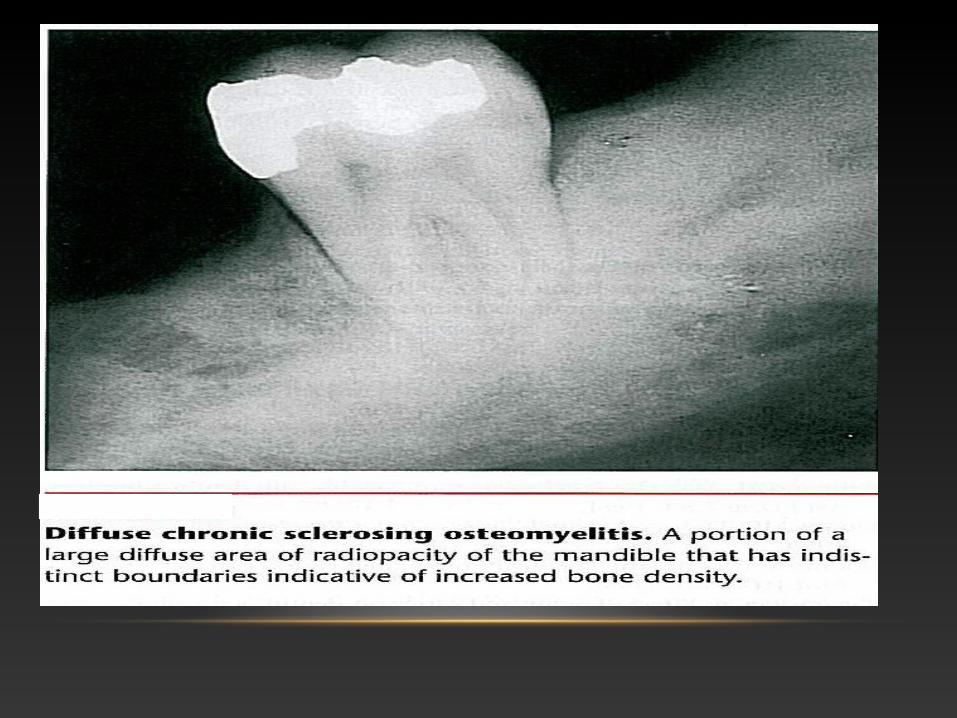
DIFFUSE SCLEROSING OSTEOMYELITIS.


Chronic osteomyelitis with proliferative periostitis (garré's osteomyelitis(

Chronic osteomyelitis with proliferative periostitis (garré's osteomyelitis(
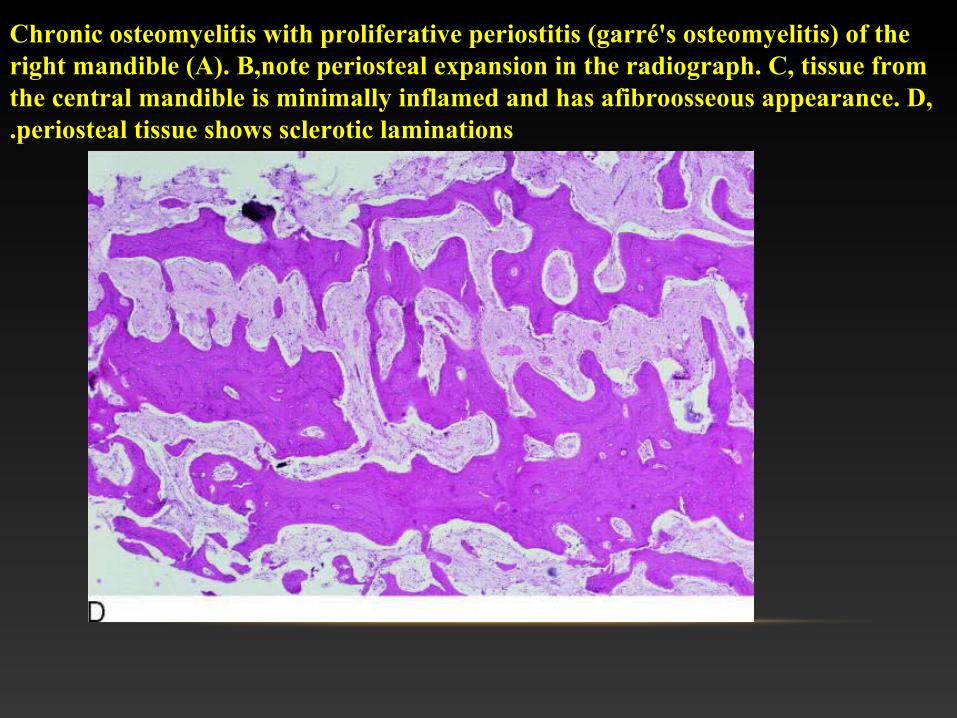
Chronic osteomyelitis with proliferative periostitis (garré's osteomyelitis( of the right mandible (A(. B,note periosteal expansion in the radiograph. C, tissue from the central mandible is minimally inflamed and has afibroosseous appearance. D, periosteal tissue shows sclerotic laminations.

Chronic osteomyelitis with proliferative periostitis (garré's osteomyelitis) of the right mandible (A). B,note periosteal expansion in the radiograph. C, tissue from the central mandible is minimally inflamed and has afibroosseous appearance. D, periosteal tissue shows sclerotic laminations.


Osteoradionecrosis. Same patient as depicted in note fistula formation of the left submandibular area resulting from osteoradionecrosis of the mandibular body.

Osteoradionecrosis. Ulceration overlying leftbody of the mandible with exposure and sequestration of superficial alveolar bone.

Osteoradionecrosis. Multiple ill-defined areas ofradiolucency and radiopacity of the mandibular body.

Osteoradionecrosis of the lingual mandible precipitated by trauma.

OSTEORADIONECROSIS OF THE MANDIBLE.

Dry socket. Typical appearances of chronic alveolar osteitis; thesocket is empty and the bony lamina dura is visible.
Sequestration in a severe dry socket. Almost the whole of the lamina dura and attached trabeculae have become necrotic, forming a sequestrum. Healing is delayed while the sequestrum remains in place. Most dry sockets are not associated with sequestration, or with only small sequestra.