Biochemistry for Dental Students Shreya Nigoskar
185
Biochemistry for Dental Students
-
Upload
leeminhoangrybird -
Category
Documents
-
view
261 -
download
65
description
biochem
Transcript of Biochemistry for Dental Students Shreya Nigoskar

Biochemistryfor
Dental Students


Biochemistryfor
Dental Students(Theory and Practical)
Shreya Nigoskar MSc PhD
Associate Professor of BiochemistryCollege of Dental Sciences &
Hospital, Rau, Indore (MP)
JAYPEE BROTHERSMEDICAL PUBLISHERS (P) LTD
New Delhi

Published by
Jitendar P VijJaypee Brothers Medical Publishers (P) LtdB-3 EMCA House, 23/23B Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021, +91-11-23245672, Rel: 32558559Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected] Visit our website: www.jaypeebrothers.com
Branches 2/B, Akruti Society, Jodhpur Gam Road Satellite, Ahmedabad 380 015
Phones: +91-079-26926233, Rel: +91-079-32988717, Fax: +91-079-26927094e-mail: [email protected]
202 Batavia Chambers, 8 Kumara Krupa RoadKumara Park East, Bangalore 560 001Phones: +91-80-22285971, +91-80-22382956, Rel: +91-80-32714073, Fax: +91-80-22281761e-mail: [email protected]
282 IIIrd Floor, Khaleel Shirazi Estate, Fountain PlazaPantheon Road, Chennai 600 008Phones: +91-44-28193265, +91-44-28194897, Rel: +91-44-32972089, Fax: +91-44-28193231e-mail: [email protected]
4-2-1067/1-3, 1st Floor, Balaji Building, Ramkote Cross RoadHyderabad 500 095, Phones: +91-40-66610020, +91-40-24758498, Rel:+91-40-32940929,Fax:+91-40-24758499, e-mail: [email protected]
No. 41/3098, B and B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala, Phones: 0484-4036109, +91-0484 2395739, +91-0484 2395740
1-A Indian Mirror Street, Wellington SquareKolkata 700 013, Phones: +91-33-22451926, +91-33-22276404, +91-33-22276415, Rel: +91-33-32901926Fax: +91-33-22456075, e-mail: [email protected]
106 Amit Industrial Estate, 61 Dr SS Rao RoadNear MGM Hospital, Parel, Mumbai 400 012Phones: +91-22-24124863, +91-22-24104532, Rel: +91-22-32926896Fax: +91-22-24160828, e-mail: [email protected]
“KAMALPUSHPA” 38, ReshimbagOpp. Mohota Science College, Umred RoadNagpur 440 009 (MS)Phone: Rel: 3245220, Fax: 0712-2704275e-mail: [email protected]
Biochemistry for Dental Students
© 2007, Jaypee Brothers Medical Publishers
All rights reserved. No part of this publication should be reproduced, stored in a retrieval system, or transmitted in any formor by any means: electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of theauthor and the publisher.
This book has been published in good faith that the material provided by author is original. Every effort is made toensure accuracy of material, but the publisher, printer and author will not be held responsible for any inadvertenterror(s). In case of any dispute, all legal matters are to be settled under Delhi jurisdiction only.
First Edition: 2007ISBN 81-8448-049-0Typeset at JPBMP typesetting unitPrinted at Rajkamal

Dedicated tomy Gurumaharaj
Shri Nana Maharaj Taranekar
andAll the students who have
inspired and encouraged me
'kkafr Lo:ik; fon~egs] Hkkxor Js"Bk; f/kefg] rUuksa ekr±M izpksn;kr~


PREFACE
Publishing of this book Biochemistry for Dental Students was not a long cherished dream likeother authors but a spontaneous thought.
While working as a Lecturer in Dept of Physiology and Biochemistry in College of DentalSciences and Hospital in the year 2004, I met an unfortunate road accident and was in bedsuffering from major head injury and a fractured limb. Neither I nor my kith and kin weresure that I would be even able to stand on my feet again.
Before, the aforesaid miserable span of my life began, the librarian Mr Ravish Verma,had told me that, there is no adequate study material available in biochemistry for studentsof BDS first year although in the past few years, a number of textbooks in biochemistry havebeen published, primarily for students of medicine but none for students of dentistry. Hesuggested me to inscribe a book which could be of sufficient use to the students of not onlythis institute but of every renowned university in India. I am extremely grateful to him forhis valuable advice.
When, I fully recovered and joined the college, I initiated and completed the work andthe editorial board of M/s Jaypee Brothers Medical Publishers (P) Ltd. New Delhi, becameready to publish the book. This book has been written to meet the needs of dental studentsin biochemistry, theory as well as practicals, while compiling, this book, I have consultedseveral syllabi so as to cover all the topics prescribed for BDS students of various universities.
This is my first effort and may not be without errors, I request the teachers as well asstudents to send me their precious comments so that I can enhance the matter as well asmanner of the book.
Shreya Nigoskar


ACKNOWLEDGEMENTS
First and foremost, I thank to the supreme power God, for giving me energy, inspirationand courage to complete this arduous task. Without His blessing nothing would have beenpossible.
I express my sincere gratitude to Mr Ajit Jhavar, Chairman, College of Dental Sciencesand Hospital, Dr HC Neema, Dean, College of Dental Sciences and Hospital, Dr HC Gupta,professor emeritus, Dept of Physiology and Biochemistry, College of Dental Sciences andHospital, Rau (Indore) for their constant support and encouragement.
I owe deep debt of gratitude to Dr (Mrs) Meena Verma, Professor and Head of Dept ofBiochemistry, MGM Medical College, Indore, for her constant encouragement in my academicpursuits.
How can I put in words my gratitude to express my feelings for my parents, Mr MMDixit and Mrs Madhuri Dixit, for bringing me up to this stage. It is not possible for me toexpress thanks to them in words as their good wishes and efforts for me can never bedelineated.
My limited vocabulary compels me to use all superlatives, which two members of myfamily deserve for this cooperation and association, my son Master Suryansh Nigoskar, whosuffered a lot, during the inscription of the book, but never complained and my husbandMr Manoj Nigoskar who was beside me, throughout the period of the work. The value oftheir sincerity towards me cannot be measured on chart; because without their encouragementand co-operation, this book could never have been published.


CONTENTS
Part–ITheory
1. Carbohydrates ........................................................................................................................... 32. Lipids ........................................................................................................................................ 173. Proteins ..................................................................................................................................... 264. Amino Acids ............................................................................................................................ 395. Enzyme ..................................................................................................................................... 476. Digestion, Absorption and Metabolism of Carbohydrates .......................................... 567. Digestion, Absorption and Metabolism of Lipids ......................................................... 818. Digestion, Absorption and Metabolism of Proteins ...................................................... 979. Vitamins ................................................................................................................................. 109
10. Minerals: The Inorganic Elements .................................................................................... 12811. Nutrition ................................................................................................................................ 142
Part–IIPractical
12. Carbohydrates ....................................................................................................................... 15313. Lipids ...................................................................................................................................... 15714. Proteins ................................................................................................................................... 15915. Urine ........................................................................................................................................ 163
Index ......................................................................................................................................... 171


INTRODUCTION
Life itself is full of a mystery which is tried to be solved by a chemistry which is termed asbiochemistry.
Biochemistry, it would like to introduce itself and to tell you something about it. It willnot only be interesting but useful too. It is a secondary branch of a huge tree in a hugegarden, i.e. in the garden of knowledge, there is a tree of Dental Science and Physiology andit is one of the primary branches of this tree and has many secondary branches includingitself.
The origin of biochemistry goes back to eighteenth century with Levostier’s explanationof respiration as biological oxidation of food and the experiments that showed that livingmatter contained proteins, carbohydrates and fats not found in mineral sources.
At the turn of century, many scientists settled various facts. Such as establishment ofstructure of carbohydrates and protein and recognition of specificity of enzyme action byEmil Fischer and exploitation by Harden and Young of the accidental observation by Buchnerbrothers that a cell free extract of yeast could ferment glucose with production of alcohol. Inthis way the development of biochemistry continued.
It was termed as biochemistry for the first time by Carl Neuberg in 1903.Biochemistry broadly deals with chemistry of life and living processes. There is no
exaggeration in the statement.The scope of biochemistry is as vast as life itself. Every aspect of life, birth, growth,
reproduction, ageing and death involves biochemistry.For that matter every movement of life is packed with hundreds of biochemical reactions.
Biochemistry is the most rapidly developing and most innovative subject in medical and dentalsciences.

PART–ITHEORY


Carbon + Hydrogen + OxygenFound in abundance in plant kingdom in the form of cellulose and starch besides this also
found in animal kingdom in the form of glucose and glycogen.
INTRODUCTIONCarbohydrate
Carbohydrates are neutral compounds made up of carbon, hydrogen and oxygen. H and Obeing in the same proportion as in water, the general formula is Cn (H2O)n.
But there are many exceptions, e.g. rhaminose (C6H12O5) is a carbohydrate in which H andO are present in different proportion.
Certain other compounds such as formaldehyde (HCHO) acetic acid (CH3COOH), lacticacid (CH3CHOCOOH) etc. which have got the same empirical formula but are notcarbohydrates.
Thus, chemically carbohydrates can be defined as the aldehyde and ketone derivative ofhigher polyhydric alcohol or polyhydroxy aldehydes or ketones or the compounds whichproduce them on hydrolysis.
Biomedical Importance
1. Carbohydrates are the main source of energy.2. They are constituents of compound lipids and conjugated proteins.3. Degradation products of carbohydrates act as promoters or catalyst.4. Certain carbohydrate derivatives are used as drugs like cardiac glycosides / antibiotics.5. Degradation products are utilized for synthesis of other substances such as fatty acid,
cholesterol, amino acids, etc.6. They are the constituents of mucopolysaccharides and form the ground substance of
mesenchymal tissues.
CHAPTER 1
Carbohydrates(Quick energy supplier)

4 Biochemistry for Dental Students
7. Ribose is a constituent of nucleic acid (DNA, RNA).8. Ribose, i.e. pentose sugar also constituents certain coenzyme, e.g. FAD, NAD, coenzyme A,
etc.9. Glucose is chief physiological sugar present in blood, i.e. about 0.1%.
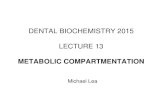
Fig. 1.1: Classification of carbohydrates
Carbohydrates are classified into three classes—
I. MonosaccharidesII. Oligosaccharides
III. Polysaccharides (Fig. 1.1).

Carbohydrates (Quick energy supplier) 5
I. Monosaccharides
Simplest class of carbohydrates which cannot be further hydrolysed. These are further classifiedinto two groups. On the basis of their functional group they are classified as oldoses and Aldoses
a. Aldoses—When the functional group is an aldehyde CH-O in a monosaccharide.b. Ketoses—In ketoses the functional group is a keto group C=O.
The number of carbon atoms in the monosaccharides are given in the Table 1.1.
Table 1.1: Monosaccharides and their number of carbon atoms
Sr. No. Monosaccharide No. of carbon atoms Aldoses Ketoses
1. Triose 3 Glyceraldehyde Dehydroxy acetone p2. Tetrose 4 Erythrose Erythrulose3 Pentose 5 Ribose Ribulose4 Hexoses 6 Glucose Fructose5 Heptoses 7 Glucoheptose Sedoheptulose
So, it can be remembered that glucose is a aldohexose and fructose is a ketohexose.
General Properties of Monosaccharides
1. Colourless, crystalline compound, having sweet taste, soluble in water, insoluble in benzeneand ether, sparingly soluble in alcohol.
2. Optical rotation—When a beam of polarised light is passed through a solution containingassymetric carbon compound then this light is rotated clockwise or to right side to bedextrorotatory represented by ‘d’ or (+) and is rotated anticlockwise or left then said to belevoratory represented by ‘l’ or (–).
The mixture containing d l isomers in equal proportion is called as recemic mixture.It does not exhibit any optical activity since both d and l activities cancel each other. Freshlymade solution of α glucose has specific rotation of 112°. When solution is made to stand thevalue falls and after 24 hours and stabilizes to 52.5°.
The initial optical rotation shown by sugar gradually changes until a fixed rotationcharacteristic of sugar is reached.
3. Sugars exist both in straight chain form and ring form.Six membered rings are called as pyranose.Five membered rings are called as furanose.

6 Biochemistry for Dental Students
MUTAROTATIONMutarotation—Mutarotation is defined as the change in optical rotation representing theinterconversion of α and β forms of D glucose to an equilibrium mixture (Fig. 1.2).
α D Glucose <=====> Equilliberim <=====> D Glucose+ 112.2° mixture + 18.7°
+ 52.7°*(Specific optical rotation).
Mutarotation of fructose—Fructose also exhibits mutarotation. It has a specific optical rotationof -92° at equilibrium. The conversion of dextroratatory sucrose to levoratatory fructose can beexplained in inversion.
Epimers
If two monosaccharides differ from each other in their configuration around a single specificcarbon (other than anomeric) atom, they are referred to as epimers to each other. For example—glucose and galactose are epimers (C4 epimers), glucose and mannose are (C2 epimers).
Fig. 1.2: Mutarotation of glucose representing α and β anomers
Fig. 1.3: Structures of epimers (glucose and galactose are C4 epimerswhile glucose and mannose are C2 epimers )

Carbohydrates (Quick energy supplier) 7
Anomers
The α and β forms of D glucose are known as anomers, they differ from each other in theconfiguration only around C1 known as anomeric carbon (hemiacetal carbon). In case of βanomer, the OH group held by anomeric carbon is on the opposite side of the group CH2OH ofsugar ring and vice versa with the α anomer (Fig. 1.2).
Tautomerization or Enolization
When a hydrogen atom is shifted from one carbon atom to another to produce enediols isknown as tautomerization. When glucose is kept in alkaline solution, it forms isomers D fructoseand D mannose which results in the formation of a common intermediate enediol for all thethree sugar. Enediols are highly reactive, hence sugars in alkaline solution are powerful reducingagents.
Reducing Properties
The sugars are classified as reducing or nonreducing. The reducing property is attributed tothe free aldehyde or keto group of anomeric carbon.
In lab many tests are employed to identify the reducing action of sugars. These includeBenedict’s test, Fehlings test. The reduction is much more efficient in alkaline medium .
The enediols or sugars reduce CuSO4 (Cu++) to (Cu+) cuprous ions which form(green <—> yellow) ppt of cuprous hydroxide or (orange<—>red) ppt of cuprous oxide dependingupon concentrations of sugar.This property cannot help for specific identification of any sugar. Since, it is general reaction.
Osazone Formation
It is the reaction with hydrazine to form hydrazones which are called as osazones.Glucose + H2N-NH-C6H5 - Phenyl glucose hydrazoneThese osazones are insoluble and crystallize in beautiful and characterstic form of different
sugars.As it is evident from the reaction, the first two carbon (C1 and C2) are involved in osazone
formation. The sugars that differ in their configuration on these two carbons give the sametypes of osazomes, since the difference is marked by reaction with phenyl hydrazine. Thus,glucose, fructose and mannose give same type of osazone crystal.
Glucose, fructose and mannose have identical osazone crystals arranged as bundle of hay.• (Broom stick) needle like• Lactose forms cotton wool like crystals puffy ball like crystals.• Maltose and galactose form sunflower platelet like structure.

8 Biochemistry for Dental Students
THE PICTURES CAN BE SEEN IN PART II PRACTICALSGlycosides
Glycosides are formed when the hemiacetal or hemiketal hydroxyl group (of anomeric carbon)of a carbohydrate reacts with a hydroxyl group of another carbohydrate. The bond so formedis known as glycosidic bond. The monosaccharides are held together by glycosidic bonds toresult in di-, oligo- or polysaccharides. It should be noted that the reducing property of aldehydeand keto group is lost, when these groups participate in glycosidic bond formation. However,many di-and polysaccharides are reducing due to presence of other potential aldehyde or ketogroups.
Naming of Glycosidic Bond
The nomenclature of glycosidic bonds is based on the linkages between carbon atoms and thestatus of the anomeric carbon (α or β). For instance, lactose which is formed by a bond betweenC1 of β galactose and C4 of glucose is named as β (1 – 4) glycosidic bond.
Dehydration—When monosaccharides are treated with concentrated acids, for example sulphuricacid, hydrochloric acid, etc. there occurs dehydration, thus pentoses give furfurals, and hecosesgive hydroxy methyl furfurel. These furfurals can condense with phenolic compounds like αnepthol. This is the chemical base for Molisch test, which is a group test for carbohydrates.
Selivanoff’s Test
This test is specific for fructose. Resorcinol dissolved in conc HCl is added to sugar then pinkcolour is formed due to reaction of furfural with reasorinol.
II Oligosachharides
These type of carbohydrates are composed of 2-10 monosachharide molecules which can beobtained on hydrolysis.
The important oligosaccharides are classified as (shown in Table 1.2):• Disaccharides• Trisaccharides• Tetrasaccharides• Pentasaccharides.
Depending on number of monosaccharide units. Among the oligosaccharides disaccharidesare most common. As the name suggests, a disaccharide unit consists of two monosaccharideunits (similar or dis similar) which are held together by glycoside bond. Diasaccharides are oftwo types—

Carbohydrates (Quick energy supplier) 9
1. Reducing.2. Non-reducing.
Disaccharide units produce two molecules of monosaccharide units on hydrolysis. The mostcommon disaccharides are—
Lactose — Glucose + Galactose β [ 1 – 4 ] Glycosidic bondMaltose — Glucose + Glucose α [ 1 – 4 ] Glycosidic bondSucrose — Glucose + Fructose [α1 - β2] Glycosidic bond
Table 1.2: Oligosaccharides and their monosaccharide molecules
Sr. No. Oligosaccharides No. of monosaccharides Type
1 Di 2 Lactose sucrose maltose2 Tri 3 Raffinose3 Tetra 4 Stachyose4 Penta 5 Verbascose
Sucrose
Surcose is sugar of commerce. Its source is cane sugar. It is dextrorotatory. Hydrolysis of it bydilute acid or enzyme invertase or sucrase produce 1 molecule each of glucose and fructosewhich results in change in optical rotation from positive to negative because fructose is morelevorotatory than D glucose.
SucraseSucrose + H2O ————→ Glucose + Fructose
Because of this sucrose is called as invert sugar. Honey contains a large proportion of sucrose.Sucrose is not a reducing sugar because the reducing groups of glucose and fructose are involvedin glycosidic bond formation. So, it can not form osazones.
Lactose
Lactose is formed by mammary glands and occurs to the extent of about 5% in milk. Therefore,it is most commonly known as milk sugar. Lactose of milk is the most important carbohydratein the nutrition of young mammals. It is hydrolsed by enzyme lactase in to glucose and galactose.
It may also be present in the urine during pregnancy. It is a reducing sugar. Souring of milktake place when lactose is converted to lactic acid. It gives osazone crystals [cotton wool shaped].
Maltose
Maltose is also called as malt sugar. Maltose is composed of two glucose units and is formedby hydrolytic action of enzyme amylase or diastase on starch It is a reducing sugar. In it theglucose units are held together by α (1 – 4) linkage. It gives osazone crystals [sunflower shaped].

10 Biochemistry for Dental Students
Isomaltose
It is formed during hydrolysis of certain polysaccharide also resembles maltose except that ithas one α-1, 6 glycosidic linkage.
Polysaccharides
Polysaccharides consist of repeated units of monosaccharides or their derivative held togetherby glycosidic linkages. They are primarily concerned with two important functions. Structuraland storage of energy. Polysaccharides are of two types—A. Homopolysaccharides.B. Heteropolysaccharides.
HOMOPOLYSACCHARIDESWhen polysaccharides are composed of same types of repeated units of surgars or theirderivatives they are refered to as, homopolysaccharides.
Starch
Starch is the carbohydrate reserve of plants which is the most important dietary source forhigher animals, including man. High content of starch is found in cereals, roots, tubers,vegetables, etc. Starch is a homopolymer composed of D-glucose units held by α-glycosidicbonds. It is known as glucosan or glucan .
Strach consists of two polysaccharide components-water soluble amylose (15-20%) and awater insoluble amylopectin (80-85%). Chemically, amylose is a unbranched chain with 200-1,000 D-glucose units held by α (1→4) glycosidic linkages. Amylopectin, on the other hand, isa branched chain with α (1→6) glycosidic bonds at the branching points and α (1→ 4) linkageseverywhere else. Amylopectin molecule containing a few thousand glucose units looks like abranched tree (20-30) glucose units per branch) (Fig. 1.4).
Starches are hydrolysed by amylase (pancreatic or salivary) to liberate dextrins and finallymaltose and glucose units. Amylase acts specifically on α (1→4) glycosidic bonds.
Dextrins
Dextrins are the breakdown products of starch by the enzyme amylase or dilute acids. Starchis sequentially hydrolysed to different dextrins and, finally, to maltose and glucose. The variousintermediates (indentified by iodine colouration) are starch (blue), amylodextrin (violet),erythrodextrin (red) and achrodextrin.
(no colour).

Carbohydrates (Quick energy supplier) 11
Inulin
Inulin is a polymer of fructose, i.e fructosan. It occurs in dahlia bulbs, garlic, onion, etc. It is alow molecular weight (around5,000) polysaccharide easily soluble in water. Inulin is not utilizedby the body. It is used for assessing kidney function through measurement of glomerular filtration
rate (GFR).
Glycogen
Glycogen is the carbohydrate reserve in animals, hence often referred to as animal starch. It ispresent in high concentration in liver, followed by muscle, brain, etc. glycogen is also found inplants that do not possess chlorophyll (e.g. yeast, fungi).
The structure of glycogen is similar to that of amylopectin with more number of branches.Glucose is the repeating unit in glycogen joined together by α (1→4) glycosidic bonds, andα (1→6) glycosidic bonds at branching points. The molecular weight (up to 25,000) vary inglycogen, depending on the source from which the glycogen is obtained (Fig. 1.5).
Cellulose
Cellulose occurs exclusively in plants and it is the most abundant organic substance in plantkingdom. It is a predominant consitituent of plant cell wall. Cellulose is totally absent in animalbody.
Fig. 1.4: Structures of amylose and amylopectin

12 Biochemistry for Dental Students
Cellulose is composed of β-D-glucose units linked by β (1 → 4) glycosidic bonds. Cellulosecannot be digested by mammals—including man due to lack of the enzyme that cleavesβ-glycosidic bonds (β amylase breaks β bonds only). Certain ruminants and herbivorous animalscontain microorganisms in the gut which produce enzymes that can cleave β-glycosidic bonds.Hydrolysis of cellulose yields a disaccharide cellobiose, followed by β-D-glucose.
Cellulose, though not digested, has great importance in human nutrition. It is a majorconstituent of fiber, the non-digestable carbohydrate. The functions of dietary fiber includedecreasing the absorption of glucose and cholesterol from the intestine, besides increasing thebulk of feces.
Chitin
Chitin is composed of N-acetyl D-glucosamine units held together by β (1→4) glycosidic bonds.It is a structural polysaccharide found in the exoskeleton of some invertebrates, e.g. insects,crustaceans.
HETEROPOLYSACCHARIDESWhen the polysaccharides are composed of different types of sugars or their derivatives, theyare referred to as heteropolysaccharides or heteroglycans.
MUCOPOLYSACCHARIDES
These are heteroglycans made up of repeating units of sugar derivatives, namely amino-sugarsand more commonly known as glycosaminoglycans (GAG) . Acetylated amino groups, besides
Fig. 1.5A: Showing general structure of amylose
Fig. 1.5B: Showing general structure of amylopectin which resembles with structure of glycogen

Carbohydrates (Quick energy supplier) 13
sulfate and carboxyl groups are generally present in GAG structure. The presence of sulfateand carboxyl groups contributes to acidity of the molecules, making them acidmucopolysaccharides.
Some of the mucopolysaccharides are found in combination with proteins to formmucoproteins or mucoids or proteoglycans. Mucoproteins may contain up to 95% carbohydrateand 5% protein.
Mucopolysaccharides are essential components of tissue structure. The extracellular spacesof tissue (particularly connective tissue cartilage, skin, blood vessels, tendons) consist of collagenand elastin fibers embedded in a matrix or ground substance. The ground substance ispredominantly composed of GAG. A diagrammatic representation of a proteoglycan complexis depicted in Figure 1.6.
The important mucopolysaccharides include hyaluronic acid, chondroitin 4-sulfate, heparin,dermatan sulfate and keratin sulfate (Fig. 1.7).
Hyaluronic Acid
Hyaluronic acid is an important GAG found in the ground substance of synovial fluid of jointsand vitreous humor of eyes. It is also present as a ground substance in connective tissues andforms a gel around the ovum. Hyaluronic acid serves as a lubricant and shock absorbent injoints.
Hyaluronic acid is composed of alternate units of D-glucuronic acid and N-acetyl D-glucosamine. These two molecules form disaccharide units held together by β (1→3) glycosidicbond. Hyaluronic acid contains about 250-25,000 disaccharide units (held by β 1→4 bonds)with a molecular weight up to 4 million.
Fig. 1.6: Digrammatic representation of proteoglycan complex

14 Biochemistry for Dental Students
Fig. 1.7: Figure of structure of common glycosaminoglycans the disaccharides as repeating units
Hyaluronidase is an enzyme that breaks (β 1→ 4 linkages) hyaluronic acid and other GAG. Thisenzyme is present in high concentration in testes, seminal fluid, and in certain snake and insectvenoms. Hyaluronidase of semen is assigned an important role in fertilization as this enzyme

Carbohydrates (Quick energy supplier) 15
clears the gel (hyaluronic acid) around the ovum allowing a better penetration of sperm intothe ovum. Hyaluronidase of bacteria helps their invasion into the animal tissues.
Chondroitin Sulfates
Chondroitin 4-sulfate (Greek: chondroscartilage) is a major constituent of various mammaliantissues (bone, cartilage, tendons, heart, valves, skin, cornea etc.) Structurally, it is comparablewith hyaluronic acid. Chondroitin 4-sulfate consists or repeating disaccharide units composedof D-glucuronic acid and N-acetyl D-galactosamine 4-sulfate.
Chondroitin 6-sulfate is also present in many tissues. As evident from the name, the sulfategroup is found on C6 instead of C4.
Heparin
Heparin is an anticoagulant (prevents blood clotting) that occurs in blood, lung, liver, kidney,spleen etc. Heparin helps in the release of the enzyme lipoprotein lipase which causes clearingthe turbidity of lipemic plasma.
Heparin is composed of alternating units of N-sulfo D-glucosamine 6-sulfate and glucuronate2-sulfate.
Dermatan Sulfate
The name dermatan sulfate is derived from the fact that this compound mostly occurs in theskin. It is structurally related to chondroitin 4-sulfate. The only difference is that there is aninversion in the configuration around C5 of D-glucuronic acid to form L-iduronic acid.
Keratan sulfate
It is a heterogeneous GAG with a variable sulfate content besides small amounts of mannose,fructose, sialic acid, etc. Kertan sulfate essentially consists of alternating units of D-galactosamineand N-acetylglucosamine 6-sulfate.
SUMMARY1. Carbohydrates are the aldehyde and Ketone derivative of higher polyhydric alcohol. The
term sugar is applied to carbohydrate soluble in water and sweet to taste. They are themain source of energy and play an important role in various other function.
2. Carbohydrates are classified into three groups—Monosaccharide, disaccharides andpolysaccharides.

16 Biochemistry for Dental Students
Monosaccharide are further divided on the basis of functional groups as oldeses and ketosesand on the basis of number of carbon atoms they are classified as trioses, tetroses, pentoses,hexoses and heptoses.
3. Glyceraldehyde is the simplest carbohydrate. If two monosaccharides differ in their structurearound a single carbon atom, they are known as epimers glucose and galactose are C4
epimers.4. Glucose is most predominant as far as the occurrence of monosaccharides in nature is
concerned. It exists in α and β anomeric forms. The interconversion of α and β forms iscalled as mutarotation.
5. Monosaccharides show various chemical properties including oxidation, reductiondehydration, osazone formation, formation of esters and glycosideic linkages.
6. Lactose, maltose and Sucrose. These three diasaccharides are the most commonoligosaccharides, maltose and lactose are reducing diasaccharides but sucrose isnonreducing sugar. It shows inversion.
7. The polymers of monosaccharides are called as polysaccharides, the monosaccharides areheld together by glycosides linkage.
8. Polysaccharides are classified as homopolysaccharides and heteropolysaccharides.9. Homopolysaccharides are composed of a single monosaccharides (example–starch,
glycogen).10. Heteropolysaccharides contain mixture of few monosaccharides, e.g. mucopolysaccharides.

CHAPTER 2
Lipids(The concentrated storage form of energy)
DEFINITION AND INTRODUCTIONLipids constitute very important group of organic substances in plants and animals.Chemically they are various types of esters of fatty acids with different alcohols.
Properties
Insoluble in water, readily soluble in ether, chloroform, benzene, carbon tetrachloride. Theyare good solvents for fats and fatty acids. These are tasteless, odourless, colourless and neutralin reaction.
Biomedical Importance
1. Lipids are important dietary constituent and acts as fuel in the body.2. To some respect lipids are superior to carbohydrates as a raw material for combustion, i.e.
when 1 gram of fat or lipid is burnt then 9.7 calories of energy or heat is produced. It yields9.7 cal/gm of energy while carbohydrates yield 4 cal/ gm.
3. Lipids can be stored in the body in almost unlimited amount as compared to carbohydrates.4. They exert an insulating effect in the body.5. Lipids present around internal organs, e.g. lipids protect the organ from mechanical shock.6. Break down products such as acetyl CoA are used for building complex biological active
materials like cholesterol which in turn can be utilized for synthesis of certain harmones,e.g. progesteron.
7. Lipids supply fatty acids essential in the diet for normal health and growth. (Those whichcannot be synthesized in the body).
8. The nervous system is particularly rich in phospholipids. Non-polar lipids acts as electricalinsulators allowing rapid propogation of depolarization waves along myelinated nerves.
9. Fats are also components of vitamins like A, D, E and K (nepthoquinone).10. Lipoprotein and phospholipids are important constituents of many natural membranes
such as cell walls and cell organelles like mitochondrion.

18 Biochemistry for Dental Students
11. Lipoproteins serve as carriers of triglycerides, cholesterol and phospholipid in the body.Knowledge of lipid is important in understanding many current biomedical areas of interest
e.g. obesity, atherosclerosis and role of various polyunsaturated fatty acids in nutritional health.
Classification of Lipids
Lipids are classified into three classes (Fig. 2.1)1. Simple lipids.2. Compound lipids.3. Derived lipids.
I. Simple Lipids
Simple lipids are esters of fatty acids with alcohols.These are mainly of two types—A. Fats and oils or neural fats.B. Waxes.
A. Fats—Triacylglycerol or triglycerides (Fig. 2.2)
A. Fats and oils: These are the esters of fatty acids with glycerol. Triacylglycerol are the mostabundant group of lipids which acts as fuel reserve in animals and human.
Fig. 2.1: Classification of lipids

Lipids (The concentrated storage form of energy) 19
Fig. 2.2: Structure of triacylglycerol
Triacyl glycerols are of two types—simple triacylglycerol and mixed triacylglycerol.
Simple Triacylglycerol
These type of triacylglycerol contain the same type of fatty acids at the three carbon atoms.
Mixed Triacylglycerol
These are more common. These contain two or more types of different residues. In generalfatty acids attached to C1 is saturated while FA attached to C2 is unsaturated while in case of C3
that can be either.
Properties of Triacylglycerols
A few important properties of triacylglycerol have been discussed below.
1. Hydrolysis: In triglycerides there occurs step wise hydrolysis to form fatty acids and glycerol.This occurs by lipases. It is important for digestion of fat in gastrointestinal tract and mobilizationof fat from adipose tissues.
2. Saponification: The hydrolysis of triacylglycerols to produce glycerol and soaps is known assaponification.
Triglycerides + Alkali ______> Glycerol + Soap
3. Rancidity: It is the term used for deterioration of fats and oil resulting in unpleasant taste and smell. Fats containing unsaturated fatty acids are more susceptible to rancidity.When fats and oils are exposed to air moisture, light or bacteria, rancidity occurs.Rancidity is of two types—
Rancidity
Hydrolytic Oxidativerancidity rancidity

20 Biochemistry for Dental Students
Hydrolytic Rancidity
It occurs due to hydrolysis (partial) of triglycerides in presence of bacterial enzymes.
Oxidative Rancidity
It occurs due to oxidation of unsaturated fatty acids to form dicarboxylic acid, aldehydes ketones,etc. which are very unpleasant products.
The oils and fats after rancidity are called as rancid oils and rancid fats which are veryunsuitable for human consumption.
Antioxidants
The substances which prevent the occurance of oxidative rancidity are called as antioxidant.These are tocopherol (Vit. E), hydroquinone, α nepthol. These are added in the commertialpreparation of fats and oils.
Lipid peroxidation
By oxidation of lipids in living cells, there occurs formation of peroxides and free radicalswhich cause inflammatory diseases, aging, cancer, atherosclerosis and therefore, we must takeVit. E in diet, although the cells themselves have Vit. E, urate, superoxide dismutase to fightagainst peroxidation.
B. Waxes
These are the esters of fatty acids usually long chains of fatty acids with alcohol other thanglycerol. The alcohol may be aliphatic or alicyclic. Cetyl alcohol is most common in waxes.
COMPOUND LIPIDSCompound lipids are esters of fatty acids with alcohol containing an additional group such asphosphate, nitrogenous base, carbohydrates, proteins, etc.
I. Phospholipids: These are the compound lipids which contain phosphoric acid complexedwith lipids.There are of two types of phospholipids glycerophosphatides or phosphoglycerides andsphingomyelins (containing sphingosine as alcohol).
Glycerophosphatides: These are the major lipids occurring in biological membrane. Theycontain glycerol 3 phosphate esterified with fatty acids at C1 and C2, C1 contain saturatedfatty acid while C2 contain unsaturated fatty acid.

Lipids (The concentrated storage form of energy) 21
I. Phosphatidic Acid
This is the simplest phospholipids or we can say that it is the intermediary product betweentriglycerides and phospholipids. There occurs addition of nitrogen bases or other groups toform the compounds like lecithin cephalin and plasmalogens.
A. Lecithins—Also called as phosphalidyl cholin containing phospholidic acid with cholineas base. These are also found in liver and sperm.
B. Cephalins—Also called phospholidyl ethanol amine as it contains ethanolamine as basethese are also found in milk and these are identical with thrombokinase which initiatesthe blood clothing.
C. Phasmalogens—When a fatty acid is attached by ether linkage at C1 of glycerol inglycerolphosphatide there occurs formation of plasmalogens. They are chemicallyphosphatidal ethnolamine. These are also found in liver and muscles.
II. Sphingomyelin
Instead of glycerol, these contain sphingosine as alcohol they do not contain glycerol at all.These are called as sphingomyelins as they are abundant in the myelin sheaths of nerve fibres.
2. Nonphosphorylated Lipids
A. Glycolipids: Also called as cerebrosides found in white matter of brain composed ofshingosine fatty acids and brain sugar, i.e. galactose and sphingosine attached with fattyacid is called. as ceramide, galacto cerebrosides and glucocerebroside are most importantglycolipids, gangliosides found in ganglion of brain are derived from these cerebrosides.
b. Lipoproteins or proteolipids: These are the molecular complexes of lipids with proteins.They are the transport vehicles for lipids in circulation. There are five types oflipoproteins, they are chylomicrons, very low density lipoporteins, low density lipo-proteins (LDL), high density lipoproteins (HDL) and free fatty acid albumin complexes.
3. Steroids
Steroids are the compounds containing a cyclic steriod nucleus or 4 ring fused structure (Fig.2.3). The name of the nucleus is cyclopanteno perhydro phenanthrene it contains phenanthrenenucleus to which cyclopanteno ring is attached. There are several steroids found in biologicalsystem. These include cholesterol, bile acids, the structure of steroid neccleus is given in Figure2.3, with two examples, cholesterol and ergosterol, vit D, sex hormones, adrenocorticalhormones.

22 Biochemistry for Dental Students
Cholesterol
Cholesteral is exclusively found in animals and is most abundant animal sterol. Sterol meanssolid alcohol. It is widely distributed in all cells and is major component of cell membranescholesterol (Greek : chole bile) was first isolated from bile so, cholesterol means solid alcoholfrom bile.
Fig. 2.3: Structures of steroids
Cholesterol contains cyclopanteno perhydrophenen thrine with hydroxyl group.
Functions of Cholesterol– Its function is to act as insulating cover in the nervous tissues. Cholesterolperforms several biochemical functions which include synthesis of bile acids, hormones (sexand cortical) and Vitamine D.
Ergosterol— Found in plants and performs the function to produce ergocalciferol which is acompound containing vit D activity.
DERIVED LIPIDS
Derived lipids are the derivatives obtained during hydrolysis of simple and compound lipids.They are fatty acids and glycerol.

Lipids (The concentrated storage form of energy) 23
1. Glycerol: It is commonly called as glycerin, simplest trihydroxy alcohol.
It is colourless oily fluid with a sweetish test.
Sources
1. Endogenous.2. Exogenous.
Endogenous source—It is obtained by lipolysis of fats in adipose tissues.
Exogenous source—Approximately 22% of glycerol is directly absorbed to portal blood fromgut.
It has definite nutritive value. It can be converted to glucose and glycogen bygluconeogenesis.
Biomedical Importance
In Medicine
1. Nitroglycerine is used as vasodilator.2. Glycerol is given orally as well as intravenously in cerebrovascular disease.3. Intra-venous drip of mannitol is given to patients to reduce cerebral oedema.
2. Fatty acids: Fatty acids are carboxylic acids with hydrocarbon side chain. They are the simplestform of lipid.
Fatty acids are divided into two classes—saturated and unsaturated.Saturated fatty acids contain only single bond, e.g. acetic acid, butyric acid—it is butter fat,
palmitic acid, steroic acid (selected example of saturated fatty acids are given in the Table 2.1).Unsaturated fatty acids contain one or more double bonds, e.g. oleic acid.Unsaturated fats are more common in living organisms than saturated fats. Fatty acids
containing more than one double bond are called as polyunsaturated fatty acids, i.e. PUFA.For example• Linoleic acid—Found in peanut oil, soyabean oil, cotton seed oil, egg yolk, etc.• Linolenic acid—Found in soyabean oil linseed oil, cod liver oil, etc.• Arachidonic acid—Found in peanut oil and liver fat.

24 Biochemistry for Dental Students
These 3 polyunsaturated fatty acids are called as essential fatty acids. EFA as these are Notsynthesized in body, and therefore must be supplied in the diet. (Essential fatty acids withother unsatarated fatty acids are given in the Table 2.1).
Table 2.1: Selected examples of biochemically important fatty acids
Common name Systematic name Abbreviation* Structure
I. Saturated fatty acidsAcetic acid Ethanoic acid 2:0 CH3COOHPropionic acid n-Propanoic acid 3:0 CH3CH2COOHButyric acid n-Butanoic acid 4:0 CH3(CH2)2COOHValeric acid n-Pentanoic acid 5:0 CH3(CH2)3COOHCaproic acid n-Hexanoic acid 6:0 CH3(CH2)4COOHCaprylic acid n-Octanoic acid 8:0 CH3(CH2)6COOHCapric acid n-Decanoic acid 10:0 CH3(CH2)8COOHLauric acid n-Dodecanoic acid 12:0 CH3(CH2)10COOHMyristic acid n-Tetradecanoic acid 14:0 CH3(CH2)12COOHPalmitic acid n-Hexadecanoic acid 16:0 CH3(CH2)14COOHStearic acid n-Octadecanoic acid 18:0 CH3(CH2)16COOHArachidic acid n-Cicosanoic acid 20:0 CH3(CH2)18COOHBehenic acid n-Docosanoic acid 22:0 CH3(CH2)20COOHLignoceric acid n-Tetracosanoic acid 24:0 CH3(CH2)22COOH
II. Unsaturated fatty acidsPalmitoleic acid cis-9-Hexadecenoic acid 16:1;9 CH3(CH2)5CH=CH(CH2)7COOHOleic acid cis-9-Octadecenoic acid 18:1;9 CH3(CH2)7CH=CH(CH2)7COOHLinoleic acid*** cis, cis-9 12-Octadecadienoic 18:2;9,12 CH3(CH2)4CH=CHCH2CH=CH
acid (CH2)7COOHLinolenic acid*** All cis-9, 12, 18:3;9, CH3(CH2)CH=CHCH2CH=
15-Octadecatrienoic acid 12,15 CHCH2CH=CH(CH2)7COOHArachidonic acid*** All ciAll cis-5,8,11,14- 20:4;5,8, CH3(CH2)4CH=CHCH2CH=CH
Eicosatertraenoic acid 11,14 CH2CH=CHCH2CH=CH(CH2)sCOOH
* Total number of carbon atoms, followed by number of double bonds and the first carbon position of thedouble bond(s).
*** Essential acids synthesized in the body.
FUNCTION OF PUFA OR (EFA) ESSENTIAL FATTY ACIDS1. They are structural elements of tissues gonads and mitochondrial membrane.2. Involved in synthesis of prostaglondins and leukotrienes.3. Serum level of cholesterol is lowered by fats with high content of PUFA.4. They play role in vision and enhance the electrical response of the photo receptors of
illumination.

Lipids (The concentrated storage form of energy) 25
Deficiency Manifestations or Symptoms
1. Stopage or slow growth rate.2. Skin lessions, hyperkeratosis eczema like dermatitis.
One seterik is showing abbrivation which means total no. of carbon atoms, followed bydouble bonds and the first carbown position of double bonds in case of unsaturated fattyacid. I am putting sign there and three asteiks are representing essential futty acids in thetable.
3. Skin becomes abnormally permeable to water i.e. increased loss of water increases BMR–Basal Metabolic rate.
4. Abnormalities in pregnancy.5. Fatty liver accompanied by increased rates of fatty acids synthesis.6. Lessened resistance to stress.7. Kidney damage.8. Degenerative changes in arterial wall.
SUMMARY1. Lipids are chief concentrated storage form of body.2. Lipids are organic substances selectively insoluble in water and soluble in organic solvants.3. They are classified as simple lipids (facts and waxes) compound lipids (phospholipids and
nonphospho lipids ) and derived lipids (fatty acids glycerol and ketone bodies).4. Simple fats are also called as triacylglycerol. These are the esters of fatty acids with glycerol
primarily they are the major fuel reserve of animals.5. Phospholipids are the compound lipids containing phosphoric acid while nonphospholipids
do not contain phosphoric acid, e.g. glycolipids.6. Cerebrosides are simplest form of glycolipids which occur in the membranes of nervous
tissues.7. Steroids contain cyclicring known as cyclopantenoperhydrophenenthrene. Biologically
important steroids are cholesterol, bile acids, vit D, sex hormones, etc.8. The derived lipids are fatty acids glycerol and ketone bodies.9. Fatty acids are divided into two groups saturated fatty acids and unsaturated fatty acids.
The poly unsaturated fatty acids namely linoleic acid, linolenic acid and arachidonic acidwhich need to be supplied in the diet.

CHAPTER 3
Proteins(The structural and functional basis of life)
I. Definition of Proteins
This term is derived from a Greek word “PROTEIUS” means primary or holding first place orpre-eminent because they are the most important biological substances. The proteins can bedefined as the nitrogenous macromolecules composed of many amino acids.
II. Biomedical or Clinical Importance
1. Proteins are main structural component of cytoskeleton.2. Proteins are the sole source to replace nitrogen of body (since 15 g of nitrogen is lost everyday
by a well fed normal adult chiefly as urinary urea). Therefore proteins are chief dietarysources or constituent for supply of nitrogen as well as phosphorus.
3. All enzymes which are called biological catalysts are proteinous in nature.4. Proteins called as immunoglobulins serve as first line of defence against bacterial and viral
infection.5. Several hormone are proteinous in nature. These regulate many aspects of cell functions
e.g. estrogen, progesterone, etc.6. Structural protein provide mechanical support and some proteins are called as contractile
proteins, e.g. actin and myosine provide movements to muscles and therefore to body.7. Some proteins are present in cell membrane cytoplasm and nucleus which are called as
receptors. They bind specific substances such as vitamins, harmones, etc. and mediatetheir cellular action.
8. The transport protein carry out the function of transporting specific substances either acrossthe membrane or body fluids.
9. Storage proteins bind with specific substances and store them, e.g. iron is stored as ferritin.10. Few Proteins are constituents of respiratory pigments and occur in election transport chain
or respiratory chain, e.g. cytochromes, Hb, myoglobins11. Under certain conditions proteins can be catabolized to supply energy when lipids
carbohydrates stores of body are exhausted.

Proteins (The structural and functional basis of life) 27
12. Proteins by means of exerting osmotic pressure help in maintenance of electrolyte andwater balance in body.
COMPOSITION OF PROTEINSProteins are essential constituents of protoplasm. They differ from carbohydrates and lipidsby always containing nitrogen and sometimes sulphur and phosphorus. The elementarycomposition of protein is as follows :
Carbon - 54%Hydrogn - 7%Nitrogen - 16%Oxygen - 22%Some may contain sulphur - 1% while others phosphorus - 0.6%.
Classification of Proteins
The proteins are classified on three basis.I. Classification based on nutritional basis.II. Classification based on chemical nature.III. Classifications based on functions.
Classification Based on Nutritional Basis
Class I Proteins
Protein that contain all the essential amino acids in addition to nonessential amino acids arecalled as Class I proteins. All animal proteins, e.g. meat, fish, milk, egg, etc. are class I or typeI proteins.
Proteins in which one or more amino acids are missing are called as class II proteins, e.g.All proteins of vegetable origin exception rice protein is class I protein.Supplementary Proteins: Wheat contains gliadin and glutenin. Gliadin lacks in lysine butglutenin is rich in lysine.
One eats wheat as a whole and the requirement is fulfilled.
Classification of Proteins Based on Chemical Nature (Table 3.1)
1. Simple protein: They are composed of only amino acid residue.2. Conjugated proteins: Besides amino acids these proteins contain a non-proteinousmoiety
called as prosthetic group or conjugating group.3. Derived proteins: These are denatured or degraded products of simple or conjugated
proteins.

28 Biochemistry for Dental Students
I SIMPLE PROTEINS: These are classified into two classes.
A) Globular: spherical or oval shaped, soluble in water or other solvent, easily digestibleB) Scleroproteins: These are fibrous proteins i.e. fiber like in shape insoluble in water andresistant to digestion.
Table 3.1: Classification of proteins
Simple
(Not Combined with Anything)
1. Protamines – Sperm Proteins
CONJUGATED1. Nucleoproteins: Protein group with nucleic acids (DNA and RNA).
2. Glyco proteins: Protein is found in combination with carbohydrates which is less than 4%and if carbohydrate content is more than 4% then called as muco protein, e.g. mucin,glucosamine.
3. Lipoprotein: Serum lipoprotein, membrane lipoprotein.
4. Phosphoprotein: Phosphoric acid, casinogen milk.
5. Chromoprotein: Coloured natured protein, e.g. Hb, cytocromes.
6. Metalloprotein: Protein group with metal ion e.g. Fe, Co, Zn, e.g. carbonic anhydrase,ceruloplasmin.
2. Histones – Thymus histone, Hb.3. Albumin – Serum albumin, oval
(egg) lactalbumin.4. Globulin – Serum globulin vitulline
(eggyolk).5. Prolamines – Gliadin (wheat) zein
(maize)6. Glutelins – Wheat
Conjugated
(These remain combined with nonProtein-prosthetics)1. Chromoproteins – Hb, cytocrome,
visual purple.2. Phosphoproteins – caesinogen of
milk.3. Nucleoproteins – Nucleic acid.4. Glycoproteins – Mucin (saliva)
hexosamine.5. Lipoproteins – Phospholipids, egg,
yolk.6. Metalloproteins – Enzymes, e.g.
carbonic, anhydrase.
Derived
1. Proteins2. Meta proteins3. Proteoses4. Peptones5. Polypeptide6. Dipeptide7. Amino acids
Scleroproteins
2. Elastictissue e.g.Tendons andarteriesproteins
3. Keratin
Nailshorns, etc.
1. Collagen
ConnectivetissueProteins

Proteins (The structural and functional basis of life) 29
CLASSIFICATION BASED ON FUNCTIONSS = Structural proteins, e.g. keratin of hair, nail.E = Enzyme proteins – Hexokinase, pepsinogen.T = Transport proteins – Serum albumin, Hb.G = Genetic proteins – DNA, RNA.D = Defence proteins – Serum globulins, immunoglobulins.R = Receptors proteins – Receptors for hormone.S = Storage proteins - Glutelins, ovalbumin.C = Contractite proteins - Actin, myosin.H = Hormonal Proteins - Insulin, growth hormone.
STRUCTURE OF PROTEINStructural hierarchy of proteins is comparable to a building. The amino acids can be comparedto the bricks, the wall can be considered as primary structure, the twists in walls as secondarystructure, a full pledged self-contained room as tertiary structure. The building with similarand dissimilar room may be considered as the quarternary structure.
The structure of protein is rather complex and it can be divided into four levels oforganization.
I. Primary Structure: The linear sequence of amino acids forming the back bone of proteins(polypeptide).
II. Secondary Structure: The special arrangement of protein by twisting of the polypeptidechain
III.Tertiary Structure: The three dimensional structure of a functional protein.
IV. Quaternary Structure: Special arrangement of subunits, i.e. if a protein contains 2 or morepolypeptide chains then these chains are called as sub units. So the special arrangement ofthese subunits is called as the quaternary structure.

30 Biochemistry for Dental Students
Primary Structure
Primary structure of protein involves the amino acids which are the building blocks of proteinthey are held together by means of a covalent bond which is k/a peptide bond. These peptidebonds are very stronger in nature and can be considered as the cementing material betweenthe brick as shown in Figure 3.1.
Formation of a peptide bond: When the amino group of an amino acid combines with thecarboxyl group of another amino acid, a peptide bond is formed (as shown in the Figure 3.1). Itshould be noted here that depeptide will have two amino acids and one peptide bond (nottwo). Peptides containing more than 10 amino acids (deca peptides) are referred to aspolypeptides.
II. Secondary Structure
The confirmation of protein by twisting or folding is called as secondary structure of protein.Two types of secondary structures are proposed (a) α helical structure (b) β pleatical
structure.A. α-Helix:– α-helix is the most common spiral structure of proteins. It is a stabilized by
extensive hydrogen bonding. It is formed between H atom attached to peptide N and Oatom attached to peptide C. The individual hydrogen bond is weak, but collectively hydrogenbonds are very strong enough to stabilize secondary structure (α-helix) of proteins. As it isshown in Figure 3.2.
B. Parallel and antiparallel β Sheets:– In this type of arrangement, the polypeptide chains arearranged in parallel (in some direction) or antiparallel (in opposite direction). β-pleatedsheets may be formed either by interchain hydrogen bonding means the hydrogen bondingbetween the two different polypeptide chains or by intrachain hydrogen bonding means asingle polypeptide chain folding back to itself. As given in Figure 3.3.The secondary structure of protein involves hydrogen bonding between the neighbouring
segments of a polypeptide chains.
Fig. 3.1: Formation of a peptide bond

Proteins (The structural and functional basis of life) 31
Fig.3.2: Secondary structure (α-Helix)
Fig. 3.3: A. Beta pleated sheet, B. Parallel β sheet, C. Antiparalled β sheet

32 Biochemistry for Dental Students
III Tertiary Structure
The three dimensional arrangement of protein structure is referred to as the tertiary structure.This structure involves besides hydrogen bonding disulfide bonds. Electrostatic bonds andhydrophobic bonds. The term domain is used to represent the basic unit of protein structure(upto tertiary stage structures) (Fig. 3.4).
IV Quarternary Structure
Several manomer units join together to form oligomer which is a quartarnary structure ofprotein, e.g. Hb is tetramer and several isozyme like lactic dehydrogenase (tetramer) or creatinephosphokinase (a dimer). Disintegration of monomeric subunits results in loss of biologicalactivity of protein (Fig. 3.4).Bonds responsible for quarternary structure of proteins: The quarternary structure of proteininvolves, the non-covalent bonds namely hydrogen bonds, hydrophobic interaction and ionicbonds.
PROPERTIES OF PROTEINSPhysical Properties
1. Proteins are colloidal in nature but many of them can be crystallized.2. Proteins vary in their M. weights and shapes.3. Each protein has got a particular iso-electric pH or iso-electric point at which it is precipitated.
During this precipitation they do not undergo any intramolecular changes they areprecipitated because the pH is not suitable for them.
4. Soluble in water or weak salt solution dilute acid and alkalies.
Fig. 3.4: Digrammatic representation of protein structure

Proteins (The structural and functional basis of life) 33
Group Tests of Proteins
There are three group tests by which they are identifiedI. Precipitation reaction: Proteins exist in colloidal form of polar groups (-Co, NH2, - OH) Proteinscan be precipitated by dehydration or neutralization of polar groups, several methods areused to achieve protein precipitation.
i. Precipitation by salt of heavy metals – FeCl3.ii. Precipitation by acids – Nitric acids – Hiller’s test.
iii. Precipitation by alkaloids – Sulphosalysilic acid.ppt= precipitation
II. Coagulation reaction
III. Colour reaction.
Salting outPrecipitation of protein by
Salting in
I. Precipitation Reaction
Proteins are precipitated by following as shown in Table 3.2.Table 3.2: Agents that help in precipitation of protein
Salts of heavy metals Certain acids Concentrated solution of AlcoholHgCl2, FeCl3 (alkaloidal reagents) (NH4)2SO4, Na2SO4, NaCl Acetone(dehydrating
e.g. picric acid, reagent) these causetannic acid denaturation of proteins
and also dehydration.
FOR DETAILS ONE CAN REFER PART II- PRACTICALSII. Coagulation Reaction
Coagulation of protein is caused by denaturation of protein structure.
Denaturation
The phenomenon of disorganization of native structure of proteins is known as denaturaiton.Denaturation results in the loss of secondary, tertiary and quarternary structure of proteins.This involves change in physical, chemical and biological properties of proteins. The physicalagents for denaturation are heat, violent shaking, X-rays, etc. and chemical agents are: Acids,alkalies, salts of heavy metals, etc.
III. Colour Reactions
The proteins give several colour reactions which are often useful to identify the nature ofamino acids present in them.

34 Biochemistry for Dental Students
A. Biuret reaction: Biuret is a compound formed by heating urea to 180°C. When biuret istreated with dilute CuSO4 in alkaline medium a purple colour is obtained. It is believedthat this colour is due to formation of a copper coordinated complex.
Biuret test is answered by compounds containing two or more CONH group or peptidebonds. The principle of Biuret test is conveniently used to detect presence of proteins in biologicalfluids (oxamide) CONH2 + Biuret.
B. Ninhydrin Test: This test is used to detect presence of α - amino acids in a powder. It ispositive for proteins, peptones, peptide including ammonia. The triketohydrantin hydrateforms a complex with amino or carboxylic group of amino acids or other primary aminedeveloping a blue colour.
Requirement of ProteinProtein requirement for different section of the people is shown in Table 3.3.
Table 3.3: Requirement of protein
Category Age Protein Requirement in gm
Infant 0-5 months 13 gm/ day5 months - 1 year 14 gm
Children 1-3 years 164-6 years 247-10 years 28
Males 11-14 years 4515-18 years 5919-24 years 5825-50 years 6351+ 63
Females 11-14 years 4615-18 years 4419-24 years 4625-50 years 5051+ 50
Pregnant women 60Lactating First 6 months 65
second 6 months 62
PLASMA PROTEINSThe total volume of blood in adult is around 4-5.5 lit. Blood performs several classified functions.These include respiration, excretion, acid base balance, water balance, transport of metabolites,hormones and drugs body defense and coagulation.

Proteins (The structural and functional basis of life) 35
The name and function of plasma proteins can be listed as under Table 3.4.
Table 3.4: Name and function of plasma protein
Contd...
the α1 globulinfraction of plasmaproteins
Globulins antitrypsinor anti proteinaseupon electrophorasisthis protein occupies
i. Osmotic pressure: Albumin because oftheir high concentration and lowmolecular weight contributes to theplasma osmotic pressure. A decrease inthis pressure leads to excess fluidaccumulation in tissue space causingoedema. This occurs in the patientssuffering from Kwashiorkar (A proteinenergy malnutrition disorder) is due toa decrease in the plasma albumins.
Normal value in plasma is 3.5 to 5 gm /dl. Decreased level of albumin is seen inhypoalbuminemia.i. Decreased protein intake.ii. Cirrhosis of liver (liver is in the site
of albumin synthesis.iii. Nephrotic syndrome due to loss of
albumin in urine is calledalbumineria.
iv. During burns albumin is lost throughthe unprotected skin surface.ii. Transport functions: Albumin is
involved in the transportation ofimportant compounds like bilirubin freefatty acids, steroid hormones, calciumand copper. Several drugs like aspirin,penicillin, etc. are also transportedthrough circulation after binding withalbumin.
iii. Buffering action: Albumin act as buffersand maintain the acid base balance inthe body. They are the most powerfulbuffer amongst the other plasmaproteins, but their buffering action isnegligible compared to bicarbonatebuffer system.Reverse source of aminoacids for tissue during nutritional
Normal level in plasma less than 0.2 gm/dl. Antitrypsin deficiency has beenassociated with following disorers.Emphysema this disease is characterizedby abnormal distension of lungs withair.During lung infection likepneumonia, the alveolar macrophagesrelease elastase which destroys lungtissues. Under normal circumstanceselastase is inhibited by L1. Antitrypsinbut its deficiency leads to uncontrolledelastase activity causing destruction tolarge amount of lung tissues.Liver disease: Due to a defect in genecoding of α1 AT mutant α1 AT isproduced which aggregate to form
deprivation of amino acids.
It is serine protease inhibitor, i.e. it inhibitsall the proteolytic enymes having serine intheir active center, e.g. plasmin, thrombin,trypsin, chymotrypsin, elastase, etc.
Name Functions of plasma proteins Clinical significance
Albumin

36 Biochemistry for Dental Students
α2
MacroglobulinIt inactivates all proteases. It is an important invivo anticoagulant.
polymers. These polymers cause liverdamage and to subsequent cirrhosis.
Haptoglobin uponelectrophoresis thisprotein occupiesthe globulin frac-tion of plasmaproteins.
Some amount of Hb during hemolysis spillsinto plasma. This is called extracorpuscular Hb.This free Hb can easily penetrate through thefiltering membrane of glomeruli of nephrons.Haptoglobin combines with this free Hb to forma haptoglobin-hemoglobin complex whichcannot pass through the filtering membrane.
90% copper in plasma is bound to ceru-loplasmin. It is involved in transport of copperand oxidation of Fe+++
C e r u l o p l a s m i nupon electro-phoresis thisprotein occupies.The L2 globulinfraction of plasmaproteins.
Iron is transported in plasma after it combineswith transferin.
Name Functions of plasma proteins Clinical significance
Contd...
Transferin–These proteinoccupy the Bglobulinfraction ofplasma proteinuponelectrophorosis
Immunoglobulin–These proteinsoccupy the γglobulin fraction ofplasma proteinsupon electro-phoresis they are of5 different typesnamely IgG, IgA,IgM, IgE, IgD. Canbe remembered as(GAMED) [IgG].
It is most abundant Ig. It is the only Ig whichcan cross the placental barrier and transfer themother’s immunity to foetus.IgG can bind withmicrobes and sensilizse them for killing bylymphocytes and macrophages a process calledopsonization.
Erythroblastosis foetalis or HDN(hemolytic disease of new born). Thiscondition occurs when the mother isRh-ve and the foetus is Rh+ve during thesecond pregnancy.
Contd...
Normal plasma concentration of α2macroglobulin is 0.2 to 0.3 g/dl. Its levelsare elevated in nephrotic syndrome,because other proteins of low molecularweight are lost through urine.
Normal plasma concentration is <0.3g/dl concentration decreases inhemolytic anemia.
Normal plasma concentration.ceruloplasmin is 0.25 to 0.5 g/dl levelsare decreased in Wilson’s disease. Thisdisease is characterized by increasedaccumulation of copper
i. In liver leading to cirrhosisii. In basal ganglia leading to
neurological symptoms andnecrosis.
iii. In kidney causing renal failureiv. In bone marrow causing hemolytic
anemia.

Proteins (The structural and functional basis of life) 37
Name Functions of plasma proteins Clinical significance
Contd...
IgM i. These are large Ig which are very effectiveagainst invading microbes.
ii. First antibodies to be produced againstinvading microbes.
iii. Natural antibodies like ABO systemantibodies are IgM in nature.
Because of their large size they cannotcross the placenta hence the foetusthough if it has an incompatible bloodgroup antigen is protected from thenatural antibodies of the mother.
IgD
IgA These are referred to as secretory antibodiesbecause they are present in bodily secretions likesaliva, tears, sweat, secretions of GIT,nasopharynx, urogenital tract, etc.
IgE Penicillin anaphylaxis; when pencillinis injected a few times IgE antibodiesare produced which anchor themselvesto mast cells when it is injected nexttime, the antigen present in it will fixthemselves to the antibodies causingdegranulation and release of histaminefrom mast cells. Histamine causeshypofenium, bronchoconstriction,vasodilatation.
These antibodies are involved in allergy,hypersensitively and anaphylasis. They fixthemselves to basophils and mast cells and bringabout degranulation histamine which causesvasodialation and bronchoconstriction.
Fibrinogen–It is a solubleglycoprotein
The plasma is liquid medium of blood in which the cell components namely erythrocytes,leukocytes and platelets are suspended. If blood containing anticoagulants e.g heparinpotassium oxalate is centrifuged, the plasma separated out as a separatant while the cells remainat the bottom. The names and functions of plasma proteins can be listed as under.
The term serum is applied to the liquid medium which separates out after the bloodcoagulates. Serum does not contain fibrinogen and other clotting factors. This is the maindifference between plasma and serum (The presence and absence of fibrinogen).
Its function is not known for certain, lust it is believedthat it is involved in antigen recognition.
Fibrinogen undergoes proteolyticcleavage catalysedby thrombin to release small fibrinopeptides. Thisresults in the formation of fibrin monomers whichcan stick together to form hard clots
Its concentration in plasma is 0.2 – 04g/dl. Fibrinogen is blood coagulationfactor I. It should be noted that thenumber represent the order of discoveryand not the order of action.

38 Biochemistry for Dental Students
SUMMARY1. Proteins are nitrogeneous macromolecules composed of many amino acids.2. Proteins are most abundant organic macromolecules widely distributed in plants and
animals.3. They perform several dynamic functions in the oraganisms.4. Proteins are polymers of α amino acids.5. Proteins are classified in three bases—
a. On the basis of chemical nature.b. On the nutritional basis.c. On functional basis
6. The structure of proteins is divided into four levels of organization. The primary structurerepresents linear sequence of acids. Twisting of peptide chain in secondary structure.Tertiary structure is equal to the three dimensional structure of a functional protein andthe quarternary structure constitutes the assembly of similar dissimilar polypeptidesubunits.
7. The proteins possess physical as well as chemical properties.8. There are three group tests employed in lab to detect proteins. These are precipitation
reactions, coagulation reaction and colour reactions.9. Heat coagulation test is most commonly employed to detect the presence of albumin in
urine.10. The total concentration of plasma protein is about 7 – 7.5 gm.11. Electrophoresis seperates plasma proteins into five distinct bands namely albumin, α1,α2,
β and γ globulins.12. Albumin is the major constituent of plasma proteins with a concentration 3.5 – 5 gm /dl.
Albumin performs cosmotic, transport and nutritive functions.13. α1-antitrypsin is a major constituent of α1 globulin fraction. It’s deficiency has been
emplicated in emphysema.14. Haptoglobin (Hp) binds with free hemoglobin (Hb) that spills into plasma due to hemolysis.15. Immunoglobulins are specialized proteins to defend the body against the foreign substances.
They are associated with globulin fraction of plasma proteins.16. Five classes of immunoglobulins namely IgG , IgA, IgM, IgD and IgE are found in humans.
IgG is most abundant and is mainly responsible for humoral immunity. IgA protects bodysurfaces. IgM serves as first line of defense for humoral immunity while IgEis involved inallergy, hypersensitivity and anaphylasis.
17. Blood clotting is the body’s major defense mechanism against blood loss. Fibrinogen isblood coagulation factor number I. Finally, fibrinogen is converted fibrin clot.

CHAPTER 4
Amino Acids(The building blocks of proteins)
The human body produces an impressive amount of macromolecules which are the polymersmade up of monomer units.
These large polymers may be carbohydrates, lipids, nucleic acids or proteins. In case ofcarbohydrates the monomer units are sugar derivatives. In case of lipids, these are fatty acids,in case of nucleic acids the monomers are nucleotides and in case of proteins these monomerunits are amino acids.
So, the amino acids as the name implies have got amino as well as carboxylic group.The amino acids can be defined as monomeric units or building blocks of proteins.Although about 300 amino acids are present in nature, but complete hydrolysis of proteinproduces about 20 L-α amino acids. The same 20 amino acids are present in all the forms oflife.
The L-α amino acids have a general formula.
R is called side chain. In case of glycine the side chain is H.
The 20 L-α amino acids are glycine, alanine, serine, cystiene, threonine, valine, lucine,isoleucine, aspartic acid, glutamic acids, lysine, hydroxy lysine, phenylalanine, tyrosine,methionine, arginine, tryptophan, histidine, proline, hydroxyproline.
CLASSIFICATION OF AMINO ACIDSThe classification and structure of amino acids is inter related.I. On the basis of nature of R.II. On the basis of their reaction in solution.III. On the basis of number of amino and acidic group.

40 Biochemistry for Dental Students
IV. On the basis of their chemical nature.V. On nutritional basisVI. On the basis of Fate.
I. On the Basis of Nature of R
On the basis of nature of R the amino acids are classified as:
Classification on the basis of nature of side chain
1. Side chain is H (R=H)–Glycine2. R=CH2–Alanine3. Alcoholic–Serine threonine4. Sulphur containing–Cysteine, cystine, methionine5. Acidic–Aspartic acid, glutamic acid6. Basic–Lysine, hydroxyl lysine7. Branched–Valine, leucine, isoleucine8. Heterocyclic–Tryptophan, histidine, arginine9. Aromatic–Tyrosine, phenylalanine, tryptophan
10. No free NH2 group proline, hydroxyproline11. Dimers–Cystine
II. Reaction in Solution
III. On the Basis of number of Amino and Acidic Group.
1. Monoamino monocarboxylic acids–Neutral2. Diamino monocarboxylic acids–Basic3. Monoamino dicarboxylic acids–Acidic4. Diamino dicarboxylic–Neutral

Amino Acids (The building blocks of proteins) 41
IV. On the Basis of Chemical Nature the Amino Acids are Classified as Below
Aliphatic Aromatic Heterocylic
GALVI Phenylalanine HeterocyclicSerine Tyrosine TryptophaneTheonine ArginineCysteine HistinineMetholine Proline
Hydroxypraline
GALVI = Glycine,alanine,lysine,valine,isoleucine
V. On Nutritional Basis
Essential and nonessential amino acids.a. Essential amino acids are those which cannot be synthesized by our body and which should
be taken in our diet.They include, methionine, arginine, threonine, tryptophan, valine, isoleucine, leucine,phenylalanine, lysine.
b. Non-essential amino acids: These are synthesized by our body and not to be taken in ourdiet essentially. The remaining all except this are belonging to this category.
c. Semi-essential: They are the growth promoting factors. During pregnancy lactation thesebecome essential because they are synthesized in our body and the quality during.GPL = Growth pregnancy lactation is insufficient. They are the growth promoting factors.During pregnancy and lactation these become essential.G – GrowthP – PregnencyL – Lactation.
VI. On the Basis of Fate

42 Biochemistry for Dental Students
Occurrence of Amino Acid
Till the standard amino acids are present in almost all protiens, primary wheat is rich in acidicamino acids, e.g. glutamate, asparate while collagen is rich in basic amino acids, e.g. lysine,histidine.
The amino acids which do not occur in proteins:
Due to lack of codon for protein synthesis. There are some compounds which do not occur orwhich never occur in proteins but they have got the same basic skeleton of amino acids. Theseare :–1. α amino butyrate – a neurotransmitter.2. β alanine (β amino acid (found in CoA)3. Orithine, citrulline (metabolites of urea cycle).4. DOPA (Dihydroxy phenylalanine) precursor for a pigment called as melanin.5. Tri-Iodo teraiodothyronine (T3-T4) thyroid hormones.6. Taurine (Bile salt).
Function of Amino Acids
Apart from monomeric constituents of protein and peptides amino acids serve variety offunctions.a. Some amino acids are converted to carbohydrate and called as glucogenic amino acids.
Some amino acids are converted to fats and are ketogenic amino acids as we have seen inclassification.
b. Specific amino acids give rise to specializedi. Tyrosine forms hormones, like thyroid hormones (T3-T4). Epinephrine. Non-epinephrine
and pigment called melanin and catecholamine (Nervous regulator).ii. Tryptophan synthesizes a vitamin called niacin.
iii. Glycine, arginine and methionine synthesize creatine.iv. Glycine and cystine help in synthesis of bile salts.v. Glutamate, cystine and glycine synthesize glutathione (glu, cys, gly).
vi. Histidine changes to histamine (vasodilation).vii. In addition to tripeptide formation glycine also used in synthesis of heme.viii.Pyrimidines and purines use several amino acids for their synthesis such as aspartate,
glutamate for pyrimidines and glycine, serine, aspartic acid and glutamine for purinesynthesis.
c. Some amino acids are used as detoxicants of specific subject such as glycine, cysteine.d. Metheonine transfers methyl group to various group of transmethylation.e. Cysteine and methionine are sources of sulphur.

Amino Acids (The building blocks of proteins) 43
PROPERTIES OF AMINO ACIDSPhysical Properties (Fig. 4.1)
1. They are colourless, crystalline substances more soluble in water then in other polar solventssuch as ethanol and insoluble in non-polar solvent.
2. They have high melting point usually more than 200°C.3. The aromatic amino acids absent UV light.4. Taste: Amino acids may be sweet, e.g. glycine; alanine valine, tasteless, e.g. leucine, bitter
e.g. arginine. Sodium glutamate is salt of glutamic acid which is used in flavouring agentin food industry which increases taste and flavour.
5. Optical properties: All the amino acids except glycine show optical isomerism because almostall have one asymmetric carbon.
6. Ampholytes: As we know that amino acids have NH2 as well COOH group so they canaccept as well as donate one proton. Hence, they are regarded as ampholytes.
7. Zwitterion: Amino acids have a property that in highly acidic pH they act as cation (+vecharged) while in highly alkaline medium they act as anion (-ve charged). So they are Zwittermolecules i.e. hybrid of + (positive) and – (negative) charges at a particular pH i.e. isisoelectric pH (As we can see in Fig 4.1).
8. Chemical properties : The amino acids show following chemical properties1. Due to COOH group2. Due to NH2 group3. Due to both of them.
Fig. 4.1: Existence of amino acids as cation, anion and zwitteion

44 Biochemistry for Dental Students
I. Reactions Due to COOH Group
a. Amino acids form esters alcohol with bases when COOH group is esterified
b. Decarboxylation: They undergo decarboxylation to form amines. This reaction is of significance
because many biologically imp amines are formed by decarboxylation reactions.
Examples are;Histidine to histamine: It is formed in injured tissues. It’s liberation is related to traumaticshock.Tyrosine to tyramine: It is involved in increasing blood presure.
c. Reaction with NH3 — The amino acids react with NH3 to form amide.e.g. aspartic acid + NH3 – asparagineglutamic acid + NH3 – glutamine.
d. Reduction to amino alcohol: This is achieved by the presence of lithium, aluminium hydride.
II. Properteis Due to NH2 Group
a. Salt formation with acids: The basic amino group reacts with mineral acids such as HCl toform salts like hydrochlorides.
Glycine + HCl ===> Glycinehydrochloride
b. Formation of acyl derivatives: Amino group reacts with acyl anhydride or acyl halidessuch as benzoyl chloride and give acyl amino acids like benzoyl glycine (Hippuric acid)Incidentally this is one of the mechanism of detoxification in which glycine is used. Thisalso forms the basis of liver function test.
c. Oxidation: Potassium permanganate or H2O2 oxidizes the NH2 group and converts theamino acid into imino acid which reacts with water to form NH3 and α keto acid.
d. Reaction with Formaldehyde: Formaldehyde reacts with NH2 group to form methylenecompound.

Amino Acids (The building blocks of proteins) 45
III. Properties of Amino acids
Due to both amino as well as carboxylic groups.Both cations and anions of amino acids react with certain heavy metals and other ions to
form chelated complexes (Fig. 4.2).
Fig. 4.2: Calcium glycinate
Clinical Applications
Chelates are nonionic, therefore amino acids can be used to remove calcium from bones andteeth.
It is possible that amino acids resulting from break down of enamel and dentine could inthis way form soluble calcium complexes, thereby causing Loss of calcium and formation of dental
caries.
PEPTIDESA peptide consists of two or more amino acid residues linked by a peptide bond which is acovalent bond(A peptide of more than 10 called as polypeptides.)
Biologically Active Peptides
Some small peptides which have significant biological activity are formed as a result ofhydrolysis of large proteins while some are formed during synthesis. Some importantbiologically active peptides are—1. Angiotensin I: When the kidney enzyme renin acts on plasma globulin fraction to liberate
a decapeptide known as angiotensin I which has got a slight effect on blood pressure.2. Angiotensin II: It consists of 8 amino acids and is formed by splitting of 2 amino acids from
angiotensin I. It has a prominent effect on blood pressure. It also stimulates thirst, dilationof blood vessels of voluntary muscles and brain increased secretion of aldosterone takesplace.
3. Angiotensin III: It is of seven amino acids formed from angiotensin II by removal of asparticacid has a role in pathology of hypertension.
4. Antibiotics: Panicillin, actinomycines, chloramphenicol are all peptides. Tyrocidine andgranulene contain D phenylalanine and ornithine which is absent in protein.
5. Bradykinin: It is a nonapeptide consisting of 9 amino acids and the most potent painproducing substance has shown to mediate production of prostaglandins E2 from arterialwalls.

46 Biochemistry for Dental Students
6. Kellidin: One and two are decapeptides and show the relaxant effect on smooth muscles.7. Carnosine: Dipeptide (Histidine and alanine ) of voluntary muscles.8. Glutathione: It is a tripeptide consisting of glutamic acid, cystiene and glycine.
1. It is easily converted to disulphide form and involved in oxidation-reduction reaction.2. By donating H2 it helps to destroy H2O2 and other peroxides in cells.3. Many –SH group containing enzymes are also protected by glutathione against oxidation.
9. HormonesGastrin secretion pancreozymin: Hormones of digestive tract. These stimulate secretion ofbile and other digestive enzymes.Oxytocin vasopressin: Octapeptide containing 8 amino acids found in pitutary gland oxytocinacts on uterine muscles and involved in parturation and ejection of milk while vasopressininfluences reabsorption of water by distal and collecting tubules.
SUMMARY1. Amino acids are monomeric constituents of proteins.2. There are 20 amino acids which are obtained on complete hydrolysis of proteins found in
nature.3. Amino acids possess two functional groups namely (-COOH) and amino (-NH2). In the
physiological system, they exist as dipolar ions commonly refered to as zwitterions.4. The amino acids are classified into different groups based on their structure, chemical nature,
nutritional requirement and metabolic fate.5. Besides the 20 standard amino acids present in proteins, there are several non-standard
amino acids. These include ornithine citrulline and dopa.6. All amino acids show properties due to amino groups, carboxlic groups and due to both of
them.7. In addition to protein and amino acids, several peptides perform, biologically important
function. These include glutathione, oxytocin, vasopressin.

CHAPTER 5
Enzyme(The living catalysts)
Definition
Enzymes are organic catalytic agents, protein in nature, produced by living cells but for theirwhole action presence of living cells is not necessary.
Special Features of Enzymatic Activity
1. If oxidation-reduction or hydrolytic action is done in laboratory, it will require a great dealof heating and addition of corrosive quantity of acids or alkalies, and yet long time, Butwithin our body the enzymes accomplish hydrolysis, oxidation, reduction, etc.a. At body temperature b. Without injuring cells c. Speedily.
Chemical reactions usually produce side products but enzymatic catalysis does notproduce any side products. Thus, we can say that enzyme catalysis is much more efficientthan man made catalysis.
2. Enzymes are highly specific, thus sucrase splits sucrose not maltose although both of themare closely similar in structure, similarly maltase splits maltose but not the sucrose. However,some enzymes are there which can act on chemically close substrates (where substrate acompound on which the enzyme acts).
3. The enzymes also show optical specificity thus the enzymes in our body which can act onL-amino acids cannot act on D amino acids.
Factors Influencing Enzyme Activity
I. Temperature.II. pH.III. Effect of ion.IV. Concentration of substrate.V. Concentration of enzyme

48 Biochemistry for Dental Students
I. Temperature: Most of enzymes in our body act best around our body temperature around38°C. If the temperature decreases, the efficiency of enzymes also falls at around 0°C, theenzymes become remarkably inactive around – 20°C, but at normal temperature again theefficiency is regained.
The optimal temperature is that temperature at which the enzyme acts best (Fig. 5.1).
II. Effect of PH: Every enzyme has an optimal pH, that is a PH in which, the enzyme acts best.The PH for pepsin, trypsin and salivary amylase are 1.5, 8.0, 6.8 respectively.
Outside its optimal PH the enzyme loses its activity or efficiency.It is well known that acidosis is dangerous and if not concerned with treatment lead to
death. The reason is that as acidosis advances, most of the enzymes in our body becomeinsufficient and eventually all chemical reactions stop which lead to death.
III. Effect of Ions: Some enzyme reactions cannot proceed unless ions like mg++, zn++, mn++
are present in reactions medium, e.g. Cl– ions enhance the action of salivary amylase.
Fig. 5.1: Showing effect of temperature on enzyme activity
Fig. 5.2: Showing effect of substrate concentration on enzyme activity

Enzyme (The living catalysts) 49
IV. Concentration of substrate: The concentration of substrate is directly proportional to thevelocity of reaction. Further increase of substrate does not cause increase of the rate of reaction(Fig. 5.2).
V. Concentration of enymes: Within fairly wide limits the speed of an enzymatic reaction isproportional to the enzyme concentration. This can be shown to hold for many enzymes systems,provided interfering conditions do not develop and the substrate concentration is maintainedconstant (Fig. 5.3).
Fig. 5.3: Showing effect of enzyme concentration on enzyme activity
Mechanism of enzyme action: The enzyme combines with its substrate to form enzymesubstrate complex within the complex the substrate breakdown into products and then theenzyme dissociates from the substrate. Using symbol it can be expressed as:
E + S ________>ES<________
E S ________>E+S<________
Where letter E, S and P stand for enzyme, substrate and products respectively. The symbolstands for reversibility.
This theory originally was introduced by machalies manton which is not universally agreed.VI. Koshald hypothesis(Induced fit model). D.E. Koshald has introduced a hypothesis called, the induced fit hypothesis.
An enzyme when, not occupied by the substrate has a particular geometrical shape whenthe enzyme is attached with substrate, the shape of enzyme molecule alters slightly and becauseof this alteration of substrate (a molecule which also has a fixed geometrical shape) can fit inproperly into the enzyme molecule. This is called an induced fit. In this altered configurationhowever the enzyme is unstable (As shown in Fig 5.4).

50 Biochemistry for Dental Students
Enzyme Enhibition
Suppression of enzyme action is called as enzyme inhibition. The inhibition is classified asfollows—
a. Competitive inhibition: The inhibitor molecule which usually has a very closely resemblingchemical configuration with the substrate molecule and yet is chemically a separate moleculehas affinity for the active sight of the enzyme, therefore both the normal substrate moleculeas well as the inhibitor molecule compete for the same active site and the active site may beoccupied by the inhibitor molecules. As a result the normal substrate molecule cannot getattached with enzyme molecule forming a complex instead of ES , EI , speaking symbolically.
E + I ———→ EIb. Uncompetitive inhibition: In this type of inhibition , the binding between the enzyme andnormal subsrate occurs as usual , but now an inhibitor molecule becomes attached to theenzyme substrate complex and this stops the breaking down of the substrate. Enzymecomplex symbolically it can be written as–
E + S ______> ESES + I ______> ES I
Fig. 5.4: showing induced fit hypothesis

Enzyme (The living catalysts) 51
(c) Noncompetitive Inhibition: A non-competitive inhibitior binds with the enzyme at a siteother than the active site and as a result causes deformation of the enzyme molecule andthere occurs inhibition of enzyme. E+I —— E IIrreversible: Treatment with iodo acetic acid causes alkylation of some enzyme and enzymaticactivity. So in this type of inhibition the enzymatic power is permanently destroyed.
Nomenclature of Enzyme
In the past, some names entered into use, thus pepsin, trypsin and chymotrypsin are wellestablished names. In some cases the suffix-ase is added to the name of substrate on which, theenzyme acts. Thus, there are such names like—
Sucrase → Acts on sucroseMaltase → Acts on maltoseUrease → Acts on ureaArginase → Acts on arginineLecithinase → Acts on lecithin
CLASSIFICATION OF ENZYMES
The enzymes are classified into six major classes. Each class on its own represents the generaltype of reaction bought about by the enzyme of that class (Fig. 5.5 and Table 5.1).
1. Oxidoreductase: These enzymes catalyse the oxidation and reduction of their substratese.g. succinic, dehydrogenase, oxidizing succinic acid into fumaric acid.
2. Transferase: These enzymes catalyse the transfer of some groups or radical from onemolecute to another molecule, e.g. glutamate pyruvate transaminases transfers NH2 (amino)group from glutamic acid to pyruvic acid. As a result glutamic and pyruvic acids areconverted into α ketoglutaric acid and alanine respectively.
3. Hydrolases: These enzyme cause splitting of molecule by hydrolysis, e.g. pepsin, trypsin,lipase
4. Lyase: They remove groups from the substrates by methods other than hydrolases, e.g.aldehyde lyases (aldolases).
5. Isomerases: They cause conversion of substrate into its isomer.Phosphoisomerase
Glyceraldehyde 3p <____________________________> Dihydroxy acetone phosphate.Phospho isomerase
Fig. 5.5: Showing classification of enzymes

52 Biochemistry for Dental Students
[OTHILL(First letter of each class) is the word which can be memorized to remember six classesof enzymes in the correct order.]
Table 5.1: Showing enzyme class with example
1. OxidoreductasesAlcohol dehydrogenase (alcohol:NAD+ Oxidation ———> ReductionOxidoreducatase E.C. 1.1.1.1) AH2 + B ———> A + BH2
2. Transferases Group transferHexokinase (ATP: D-hexose 6- A – X + B ———> A + B – Xphosphotransferase, E.C. 2.7.1.1),Transaminases, transmethylases,phosphorylase
3. Hydrolases HydrolysisLipase (triacylglycerol acyl hydrolase E.C. A – B + H2O ———> AH + BOH3.1.1.3), Choline esterase, acid andalkaline phosphatases, pepsin, urease
4. Lyases Addition ———> EliminationAldolase (ketose 1-phosphate aldehyde- A – B + X – Y ———> AX - BYlyase, E.C. 4.1.2.7), fumarase, histidase
5. Isomerases Interconversion of isomersTriose phosphate isomerase A ———> A’(D-glyceraldehyde 3-phosphate etoisomerase,E.C. 5.3.1.1), retinine isomerase, glucosephosphate isomerase
6. Ligases Condensation (usually dependent on ATP)Glutamine synthetase (L-glutamate A + B———> A – Bammonia ligase, E.C. 6.3.1.2), acetyl CoAcarboxylase, succinate thiokinase
• For one enzyme in each class, systematic name along with E.C. number is given in the brackets
Division of Enzymes
Chemically the enzymes can be divided into two groups.
6. Ligase: Two substrates are linked together by the action of ligase

Enzyme (The living catalysts) 53
A. Simple protein enzyme consisting of simple proteinB. Complex protein enyme or conjugated enzyme consisting of a protein part apoenzyme and
a prosthetic group coenzyme. Combination of apoenzyme with conenzyme constitutes theholoenzymes, thus holoenzyme is a conjugated enzyme.
COENZYMESDefinition
Coenzymes are heat stable dialyzable, nonprotein organic molecules and the prosthetic groupsof enzyme (Fig. 5.6).
Fig. 5.6: Classification of coenzymes
Functions of Coenzymes (Table 5.2)
1. The function of coenzymes is usually to accept atoms or groups from a substrate and transferthem to other molecules.
2. They are less specific than enzymes. Some coenzyme can act as such in No. of differentreactions.
3. The coenzymes are attached to the position at a different but adjacent site so as to be in aposition to accept the atoms or groups which are removed from substrate.

54 Biochemistry for Dental Students
Table 5.2: Increases in plasma (serum enzymes in the diagnosis of diseases
Enzymes Normal value Diseases in which increased
I. Digestive enzymesAmylaseLipase
80-180 Somogyi units/dl or2.5 – 5.5 μKat0.2 – 1.5 IU/ I
Acute pancreatitis, mumps (acuteparotitis), obstruction in pancreatic duct,severe diabetic ketoacidosis. Acutepancreatitis, moderate elevation incarcinoma of pancreas.
II. TransaminasesAlanine transaminase ALT)or serum glutamatepyruvate transminase(SGPT)Aspartate transaminase(AST )or serum glutamateoxaloacetate transaminase(SGOT)
3-40 IU/I or 40-250 nKat Acute hepatitis (viral or toxic), jaundice,cirrhosis of liver.
III. PhosphatasesAlkaline phosphatase(ALP)(pH) optimum 9-10)
In adults 3-13 KingArmstrong (KA) units/dl or25-90 IU/I or 500-1400 nKat
Bone diseases (related to higherosteoblastic activity)-rickets, Pagetsdisease, hyperparathyroidism, carcinomaof bone.
IV.Enzymes of carbohydratemetabolismAldolase isocitratedehydrogenase (ICD)Lactate dehydrogenase(LDH)
2-6 IU/I1-4 IU/I50-200 IU/I or 1-5 μKat
Liver diseases obstructive jaundice(cholestasis), infective hepatitis, cirrhosisof liver.Prostatic carcinoma, i.e. cancer of prostategland (tartarate liabile ACP serves as amarker for diagnosis and follow up)Paget’s disease, Gaucher’s disease.
V. Miscellaneous enzymesCreatine kinase (CK)
4-45 IU/I or 50-320 nKat Myocardial intarction, liver diseases, livercancer, cirrhosis of liver.
In children 15-30 KA/dl(due to higher 0.5-4 KAunits/ dl or 2.5 -12 IU/I or10-100 nKat. Tartarate labileACP 0-0.9 KA units/dl
Acid phosphatase (ACP)(pH optimum 4 – 6)
Creatine Phosphokinase(CPK)
Muscular dystrophy, liver diseases,myocardial infarction, myasthenia gravis,leukemias .Liver disease (inflammatorytoxic or malignant)Myocardial infarctionactue infective hepatits, musculardystrophy, leukemia, pernicious anaemia.
10-50 IU/I
2-10 IU/I
Choline esterase (ChEI)
5 Nucleotidase or nucleo-tide phosphatase (NTP)
Glutamyl transpeptidase(GGT)
5-40 IU/I
20-50 mg/dl
Myocardial infarction (CK useful for earlydetection), muscular dystrophy,hypothyroidism, alcoholism.
Nephroidism, alcoholism.
2-15 IU/I Nephrotic syndrome, myocardial infarction
Hepatitis, obstructive jaundice, tumors.
Alcoholism, infective hepatitis ,obstructive jaundice.
Ceruloplasmin(ferro-oxidase)
Bacterial infections, collagen diseases,cirrhosis, pregnancy

Enzyme (The living catalysts) 55
4. NAD and NADP coenzymes function as hydrogen acceptors in dehydrogenation reactions.5. The chief function of COA is to carry acyl groups and they are used in acetylation
decarboxylation of pyruvic acid and synthesis of fatty acid and in acelytation reactions.6. The function of TPP (cocarboxylase) is to cartry active aldehyde (R CH OH)- group is
involved in transamination reaction.7. The chief function of tetrahydrofolic acid is as a carrier of formate and it is used in the
synthesis of peruvines and pyramidenes.8. The chief function of pyridoxal phosphate is involved in the transmination reaction.
SUMMARY1. Enzymes are biocatalysts, proteinous in nature.2. Enzyme catalysis is much more efficient than man made catalysts.3. They are classified into six major classes—oxidoreductases, transferases, hydrolases, lyases
isomerases, and ligases.4. Factors like concentration of enzymes, substrate concentration, temperature, pH, influence
enzyme activity.5. Enzyme activities are inhibited by reversible (competitive, uncompetitive and non-
competitive) and irreversible manner.6. Many enzymes require, the presence of non-protein substances called (cofactor) coenzymes
for their action, most coenzymes are derivative of B-complex vitamins (NAD+ , FAD, TPP).7. The mechanism of enzyme action is explained by lock and key model and more recently
induced fit model (of Koshald).

CHAPTER 6
Digestion, Absorption andMetabolism of Carbohydrates
(Burning of instant fuel)
DIGESTION AND ABSORPTION OF CARBOHYDRATESDietary carbohydrates principally consist of the polysaccharides, (starch and glycogen). It alsocontains disaccharides (sucrose lactose, and maltose) and in small amount monosaccharideslike fructose; and glucose–Liquid food materials like milk, soup, fruit juice escape digestion inmouth as they are swallowed, but solid food stuffs are masticated thoroughly before, and thenthey are swallowed.
Digestion in Mouth
Digestion of carbohydrate starts in the mouth, where they come in contact with saliva; duringmastication saliva contains a carbohydrate splitting enzyme called salivary amylase (ptyalin).
Action of Ptyalin (Salivary Amylase)
It is α amylase which requires Cl– ions for activation and optimum pH 6.7 (range 6.6 to 6.8).The enzyme hydrolyses α- 1 —> 4 glycosidic linkage at random, deep inside polysaccharidemolecules like starch, glycogen and dextrins, producing smaller molecules maltose, glucoseand trisaccharide maltotriose. Ptyalin action stops is stomach when pH falls to 3.0.
AmylaseStarch glycogen and dextrins —————> Glucose, maltose maltotriose
(As shown in Fig 6.1)
Digestion in Stomach
Practically no action. No carbohydrate splitting enzymes available in gastric juice. Some dietarysucrose may be hydrolyzed to equimolar amounts of glucose and fructose by HCl.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 57
Digestion in Duodenum
Food bolus reaches duodenum from stomach, where it meets the pancreatic juice. Pancreaticjuice contains carbohydrate splitting enzyme pancreatic amylase (also called amlyopsin) similarto salivary amylase.
Action of Pancreatic Amylase (Fig. 6.1)
It is also an amylase optimum pH 7.1, like ptyalin, it also requires Cl– for activity. The enzymehydrolyses α - 1- 4 glycosidic linkage situated well inside polysaccharide molecule. Other criteriaand end products of action similar to ptyalin.
Digestion in small intestine: Action of intestinal juice
• Intestinal amylase: This hydrolyses terminal α - 1- 4 glycosidic linkage in polysaccharideand oligosaccharide molecules liberating free glucose molecule.
• Lactase:– It is αβ galactosidase, its pH range is 5.4 to 6.0. Lactose is hydrolysed to equimolaramounts of glucose and galactose.
LactaseLactose ——————> Glucose + Galactose
• Isomaltase: It catalyses hydrolysis of α - 1- 6 glycosidic linkage, thus splitting limit dextrinat the branching points and producing maltose and glucose.
Fig. 6.1: Showing digestion of carbohydrates

58 Biochemistry for Dental Students
• Maltose:– The enzyme hydrolyses the α - 1 – 4 glycosidic linkage between glucose units inmaltose molecule liberating equimolar quantities of two glucose molecules. Its pH range is5.8 to 6.2.
MaltoseMaltose ———————— Glucose + Glucose
• Sucrase:– pH range 5.0 to 7.0. It hydrolyses sucrose molecule to form equimolar quantitiesof glucose and fructose.
SucraseSucrose ———————— Glucose + Fructose
ABSORPTION OF CARBOHYDRATESIt is observed from above that carbohydrate digestion is complete when the food materialreach small intestine and all complex dietary corbohydrates like starch and glycogen and thedisaccharides are ultimately converted to simpler monosaccharide. All monosaccharideproducts of digestion of dietary carbohydrates are practically completely absorbed almostentirely from the small intestine.
It is observed that some disaccharides which escape digestion may enter the cells lining theintestinal lumen and hydrolyzed within cells. No carbohydrates higher then the monosaccharidecan be absorbed directly into the bloodstream in normal health and if administered parenterally,they are eliminated as foreign bodies.
Glucose and galactose are absorbed very fast, fructose and mannose at intermediate rateand pentoses are absorbed slowly. A galactose is absorbed more rapidly than glucose.
Mechanism of Absorption
There are two mechanisms suggested:I. Active transport mechanism.II. Simple diffusion
I. Active Transport Mechanism
• Glucose and galactose are absorbed very rapidly and hence, it has been suggested that theyare absorbed actively and it requires energy.
• Fructose absorption is also rapid but not so much as compared to glucose and galactose butit is definitely faster than pentoses. Hence, fructose is not absorbed by simple diffusionalone and it is suggested that some mechanism facilitates its transport called facilitatediffusion. It requires a carrier protein but no requirement of energy.
II. Simple Diffusion
This is dependent on sugar concentration gradients between the intestinal lumen, mucosalcells and blood plasma. All the monosaccharide are probably absorbed to some extent by simplepassive diffusion sugars like pentose.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 59
• Sugars like pentoses are passively absorbed by simple diffusion, no requirement of carrierprotein as well as energy.
Metabolism of Carbohydrates
Carbohydrates are the major source of energy for living cells. The monosaccharide glucose isthe central molecule in carbohydrate metabolism since all the major pathways of carbohydratemetabolism are connected with it major pathways of carbohydrate metabolism:1. Glycolysis: Oxidation of glucose to pyruvate and lactate.2. Citric acid cycle: The oxidation of acetyl CoA to CO2.3. Gluconeogenesis: The synthesis of glucose from non carbohydrate sources.4. Glycogenesis: The formation of glycogen from glucose.5. Glycogenolysis: The breakdown of glycogen to glucose and then to lactate and pyruvate.
GLYCOLYSIS
It is derived from a greek word glycose–sweet, Lysis – breakdown. It is defined as the sequenceof reactions converting glucose to pyruvate or lactate with production of ATP. Glycolysis is auniversal pathway in the living cells. It takes place in all cells of the body. It takes place inpresence of oxygen (aerobic) and in absence of oxygen (anaerobic) All enzymes are found inthe cytosomal fraction of all cells.
The end products are pyruvate and lactate in aerobic and anaerobic condition respectively.
Reaction of Glycolysis
The pathway of glycolysis can be divided into three distinct phases—I. Energy investment phase or priming phases.II. Splitting phaseIII. Energy generation phase.
I. Energy Investment Phase
• Glucose is phosphorylated to glucose 6P in presence of enzyme hexokinase or glucokinase.This is an irreversible reaction depending upon ATP and Magnesium ion.
• Glucose 6P undergoes isomerization to fructose 6P in presence of an enzyme phosphohexoseisomerase.
• Fructose-6-phosphate is again phosphorylated to fructose 1, 6, biphosphate the enzymerequired for it is phosphofructokinase again ATP is converted to ADP.
II. Splitting Phase
• The six carbon compound fructose 1, 6 biphosphate in spits to two 3 carbon compoundglyceraldehyde 3P and dihydroxy acetone phosphate by the enzyme aldolase.

60 Biochemistry for Dental Students
• In presence of enzyme isomerase, there occurs isomerization of dihydroxy acetone phosphateinto glyceraldehyde 3P. Thus now there are two molecules of glyceraldehyde 3 P.
III.Energy Generation Phase
• Glyceral dehyde 3P dehydrogenase converts glyceraldehydes 3P to 1, 3 bisphosphoglyceratehere NAD+ is converted to NADH+H. Thus now 6ATP are synthesized.
Fig. 6.2: Showing reaction of glycolysis

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 61
• Phosphoglycerate kinase acts on 1, 3 bisphosphoglycerate resulting in synthesis of ATPand formation of 3 phosphoglycerate.
• Three phosphoglycerate is converted to 2 phosphoglycerate by phosphoglycerate mutaseMg++ is required.
• By enolase phosphoenol pyruvate is generated from 2 phosphoglycerate Mg++ are requiredfor this reaction.
• Phosphoenol pyruvate is converted to pyruvate by pyruvate kinase. Mg++ ions are requiredADP is converted to ATP.Three steps where the enzyme kinase is utilized (i) hexokinase (ii) phosphofructokinase
(iii) pyruvate kinase are irreversible, rest all reactions are reversible (Fig. 6.2 and Table 6.1).
Table 6.1: Energetics of glycolysis in aerobic condition
Energy Steps Enzymes required for reactions
Investment 2 ATP 1st Step Hexokinase3rd Step Phosphofructokinase
Generation 6 ATP 6th step Glyceraldehyde 3P dehydrogenase2 ATP 7th Step Phosphoglycerate kinase2 ATP 10th step Pyruvate kinase
Energy consumption is 10 ATPsubtracted from total -2 ATPenergy productionNet gain 8 ATP
Conversion of Pyruvate to Lactate
Depending upon the presence or absence of oxygen, i.e. aerobic and anaerobic conditionsrespectively, the fate of pyruvate produced in glycolysis is either towards Krebs’ cycle (aerobic)or it is reduced to lactate by NADH in presence of an enzyme lactate dehydrogenase. TheNADH utilized in this step is obtained from the reaction catalysed by glyceraldehyde3-phosphate dehydrogenase. The formation of lactate allows the regeneration of NAD whichcan be reused by glyceraldehyde 3P dehydrogenase so that the glycolysis can take place evenin absence of oxygen to supply ATP.
PRODUCTION OF ATPThe details of ATP generated in aerobic condition is given in the above chart, that is 8 ATP, aresynthesized in aerobic condition while in anaerobic condition 2 ATP are synthesized becauseNADH is utilized by lactate dehydrogenase to carryout conversion of pyruvate to lactate.

62 Biochemistry for Dental Students
Oxidation of pyruvate to Acetyl CoA
Pyruvate is oxidatively decarboxylated to acetyl CoA before entering the Krebs’ cycle. Thereaction is catalysed by a multienzyme complex PDH that is pyruvate dehydrogenase complexwhich is found only in mitochodria. The multienzyme complex PDH requires five coenzymesnamely TPP, lipomide, FAD, coenzyme A, and NAD (Fig. 6.3).
CITRIC ACID CYCLEThere are four names of same cycle and these are citric acid cycle, Krebs’ cycle, and tricar-boxylic acid cycle, or TCA – Cycle.
This cycle is the most important metabolic pathway as far as the supply of energy isconcerned because about 65 – 70% energy is synthesized in TCA cycle.
Definition
This cycle may be defined as the oxidation of acetyl CoA to CO2 and H2O essentially in aerobicconditions and it utilizes about two-third of total oxygen consumed by the body.
Citric Acid Cycle
The Centre of Metabolism
We call the TCA cycle as the centre in metabolism because it is the final common metabolicpathway for carbohydrates, proteins and fats (Refer to Fig. 6.7).
Reaction of TCA Cycle (Fig. 6.4)
After oxidation of pyruvate to acetyl CoA which is supposed to be a connecting link betweenglycolysis and Krebs’ cycle by a few authors but others describe this step as a first step of TCAcycle. The steps of citric acid cycle are described hereunder.1. Formation of citrate: Citric acid cycle properly starts with the combination or thecondensation of acetlyl CoA and oxaloacetic acid to form citrate. This reaction is being catalysedby the enzyme citrate synthase.
Fig. 6.3: Connecting link between glycolysis and Krebs’ cycle

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 63
2-3. Isomerization of citrate to isocitrate: This reaction is catalysed by an enzyme aconitase.This is achieved in two steps. First there occurs dehydration which is followed by hydrationthrough the formation of an intermediate cisaconitate.4-5. Oxidative decarboxylation of isocitrate to ααααα ketoglutarate: Again this reaction takes placein two steps. There occurs oxidative decarboxylation of isocitrate to ketoglutarate through theformation of oxalosuccinate in between. At this stage the synthesis of NADH which is equal tothe gain of 3ATP, and liberation of CO2 takes place.6. Conversion of ααααα ketoglutarate to succinyl CoA: The reaction occurs through oxidativedecarboxylation catalysed by α ketoglutarate dehydrogenase complex. Like pyruvatedehydrogenase complax, this enzyme is also dependant on five cofactors namely TPP, lipomide,NAD, FAD and CoA at this stage of the cycle, second NADH is produced and second CO2 isliberated.7. Formation of succinate: Succenyl CoA is converted to succinate by succinate thiokinase.This reaction is coupled with phosphorylation of GDP to GTP. GTP is converted to ATP byenzyme phosphokinase.8. Conversion of succinate to fumerate: Succinate is oxidized by succinate dehydrogenase tofumerate. This reaction results in production of FADH2 and not NADH. This is due to theinadequate power of succinate to reduce NAD, hence FAD is utilized and 2ATP are gained.9. Formation of Malate: With addition of water fumerate is converted to malate, enzymefumarase catalyses the reaction.10. Conversion of malate to oxaloacetate: Malate is oxidized to oxaloacetate by malatedehydrogenase. The third and final synthesis of NADH occurs at this stage and oxalo-acetateis regenerated which can combine with another malecule of acetyl CoA and the cycle can becontinued.
Table 6.2: Energetics of TCA cycle
Reactions No. of ATP generated Enzymes responsible
1. Isocitrate to oxalo succinate 3 ATP IDH2. α keto glutarate to succinyl CoA 3 ATP α Ketoglutarate DH3. Succinyl CoA to succinate 1 ATP Succinic,thiokinase4. Succinate to fumerate 2 ATP Succinic dehydrogenase5. Malate to oxaloacetate 3 ATP Malate DH
Total 12 ATP
So, during the process of oxidation of one molecule of acetyl CoA, total twelve ATP areproduced in TCA cycle. But we have already studied that during glycolysis, there occurs

64 Biochemistry for Dental Students
isomerization of dihydroxyacetone phosphate into glyceraldehyde 3P so now there is formationof two glyceraldehyde 3P and thus, there is production of 2 pyruvate molecules undergingoxidative decarboxylation to form two acetyl CoA molecules and then these two acetyl CoAmolecules undergo oxidation to CO2 and H2O producing energy and we have seen that onemolecule of acetyl CoA gives twelve ATP but we know that there are two acetyl CoA moleculeswhich undergo oxidation through TCA. Therefore, there is production of 24 ATP in TCA,6 ATP in oxidative decarboxylation of pyruvate and 8 ATP in glycolytic pathway. So the netgain in carbohydrate metabolism from one molecule of glucose is 38 ATP (Table 6.2).
Reaction of TCA Cycle
Fig. 6.4: Showing reactions of citric acid cycle

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 65
Glycogen Metabolisms
I. GlycogenesisII. Glycogenolysis.
Glycogenesis
This process is an anabolic process.
STEPS OF GLYCOGENESIS (FIG. 6.5)1. Step I: First step is the phosphorylation of glucose to glucose-6-occurs phosphate. This
occur by enzyme hexokinase in muscles and by glucokinase in liver. This reaction requiresATP and Mg.++
2. Step II: Glucose-6 phosphate is then epimerized to from glucose-1 phosphate byphosphoglucomutase.
3. Step III: Now this glucose-1 phosphate reacts with UTP to convert this high energycompound into UDPG that is uredine diphosphate glucose. This reaction is catalysed byenzyme UDPG phosphorylase. The pyrophosphate released during the process is hydrolysedinto two molecules of inorganic phosphate by enzyme pyrophosphatase.
4. Step IV: From UDPG the molecule of glucose is transferred on a pre-existing fragment ofglycogen which is called as glycogen primer so there is requirement of glycogen primer toinitiate glycogen syntheses. It is recently found that in the absence of glycogen primer aspecific protein – namely glycogenin can accept glucose from UDPG. The enzyme requiredfor this particular reaction is glycogen synthetase or (glycogen synthase).
Role of glysogen synthase: Glycogen synthase is responsible for formation of 1-4 glycosidiclinkage. It is a key enzyme of glycongenesis, it transfers glucose from UDP glucose to non-reducing linkages.
5. Step V: When a chain length has been increased by 8-10, molecules, a part of this 1-4 chain,a minimum length of six glucose molecules is transferred by the branching enzyme (namelyglucosyl α-4-6 transferase )on to the neighbouring chain in such a way that it forms a newbranching point (1-6 linkage). In this way the branch again groups further by addition ofglucose molecules at 1-4 linkage and branching with 1-6 linkage and Now a branched treelike polymer of glucose namely glycogen is ready.

66 Biochemistry for Dental Students
Pathway for Glycogenesis
Fig. 6.5: Showing steps of glycogenesis

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 67
II. Glycogenolysis
(Glycogen + Lysis) Lysis means breakdown. The degradation of stored glycogen in liver andmuscles constitutes glycogenolysis. The pathways for the synthesis and degradation ofglycongen are not reversible glycogen is degraded by breaking of 1-4 and 1-6 linkages.Steps of glycogenolysis (Fig. 6.6).1. Step I: In the first step glucose molecules are sequentially removed as glucose-1 P. This
reaction is catalyzed by the enzyme phosphorylase. This enzyme removes glucose unitsfrom glycogen until approximately four glucose residue units are left on the chain. Theglycogen so formed is called as limit dextrin which cannot be further degraded byphosphorylase.
2. Step II: Glucan transferase transfers a trisaccharide unit out of four molecules of glucosefrom the outermost chain to the nearly branch and thereby exposing the branch point.
3. Step III: In the third step there starts action of debraching enzyme. It removes glucosemolecule from branch point. This molecule of glucose is removed as free glucose not glucose1 P as it is removed by the action of phosphorylase. Now with the removal of last glucosefrom branching point again by the action of phosphorylase there occurs sequential removalof glucose as glucose-1 P. Thus, through the combined action of glycogen phosphorylaseglucan transferase and debranching enzyme, glucose 1 P and free glucose in a ratio of 8:1are produced.
4. Step IV: Glucose-1 P so produced is converted into glucose-6 P by the action ofphosphoglucomutase. This is the end product in muscles and brain. Here there startsglycolytic pathway and glucose is utilized to give energy during excercise.
5. Step V: Liver, kidney and intestine contain the enzyme glucose-6 phosphatase that cleavesglucose-6 P into glucose, this enzyme is absent in muscles and brain hence free glucose cannot be produced.
Gluconeogenesis/Neoglucogenesis (Genesis: Formation, Neo: New, Gluco: Glucose) Thesynthesis of glucose or glycogen from noncarbohydrate compounds is called asgluconeogenesis or neoglucogenesis. The precursors for gluconeogenesis are lactic acid,pyruvic acid, glycogenic amino acids and glycerol.
I. Significance of Gluconeogenesis
As we know that glucose is the center point or key molecule in carbohydrate metabolism anda continuous supply of glucose is very necessary for vital functioning of the body becauseglucose is the only fuel which supplies energy to the body in anaerobic conditions. Brain, CNS,erythrocytes, tastes and kidney medulla are dependent on glucose for continuous supply ofenergy.

68 Biochemistry for Dental Students
Fig. 6.6: Pathway for glycogenolysis

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 69
II. Occurrence of Gluconeogenesis
In mammals, the gluconeogenesis occurs in the cytosol (although some procursers are presentin mitochondria) of livers and kidney.
III. Reactions of Gluconeogenesis
Gluconeogenesis closely resembles the reversed pathway of glycolysis but it is not the completereversal of glycolysis. Essentially 3 out of 10 reactions are same for both glycolysis andgluconeogenesis.The energy barriers obstruct a simple reversal of glycolysis
i. Between pyruvate and phosphoenol pyruvateii. Between fructose-1,6 biphosphate and fructose 6 phosphate, and
iii. Between glucose-6 phosphate and glucose.
These barriers are over come by following reactions (Fig. 6.8):i. Conversion of pyruvate to phosphoenol pyruvate: Pyruvate cannot be converted directly
into phosphoenol pyruvate but this reaction takes place in 2 steps. In first step pyruvate isconverted to oxaloacelate in presence of an enzyme pyruvate carboxylase which is a biotindependent enzyme, ATP and CO2 are also required for the reaction.
This oxaloacelate is synthesized is mitochondrial matrix but this has to be transportedto cytosol to be used in gluconeogenesis but oxaloacelate is impermeable to the membranethat is why it, in mitochondrial matrix first converted in to malate and this malate can bediffused out of the mitochondria and reaches into cytosol where there occurs reconversionof malate to oxaloacelate. This reversible conversion between oxaloacelate and malate takesplace in presence of an enzyme melate dehydrogenase (MDH) which is present in cytosolas well as in mitochondria.
Now in the cytosol oxaloacelate is converted into phosphoenol phruvate in presence ofan enzyme called as phosphoenol pyruvate carboxy kinase. GTP is used in this reactionand CO2 is liberated for this reaction.
Fig: 6.7: An overview of formation and utilization of acetyl CoA

70 Biochemistry for Dental Students
Fig. 6.8: Pathway of gluconeogenesis showing the synthesis of glucose from(a) lactate (b) gluconeogenic amino acids and (c) glycerol
ii. Conversion of fructose-1,6 biphosphate into fructose 6 P : Until fructose-1,6 biphosphate,phosphoenol pyruvate undergoes the reversal of glycolysis. again it was a irreversiblereaction in glycolysis means synthesis of fructose-1,6 biphosphate from fructose -6phosphate was irreversible, therefore, here in presence of fructose-1,6 biphosphatase thereoccures conversion of fructose-1,6 biphosphate in to fructose-6 phosphate. This enzymerequires Mg ++ ions.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 71
iii. Conversion of glucose-6 phosphate into glucose: The first step in glycolysis where thereoccured conversion of glucose to glucose-6 phosphate was irreversible and, therefore, theconversion of glucose-6 phosphate to glucose requires another enzyme and the name ofthis enzyme is glucose-6 phosphatase. In this way glucose is synthesized from non-carbohydrates.
GLUCONEOGENESIS FROM LACTATE (CORI CYCLE)Lactate produced by active skeletal muscle is a major precursor for gluconeogenesis. Underanaerobic conditions, pyruvate is reduced to lactate by lactate dehydrogenase (LDH)
LDHPyruvate + NADH + H+ <———————> Lactate + NAD+
Lactate is a dead end in glycolysis, since it must be reconverted to pyruvate for its furthermetabolism. The very purpose of lactate production is to regenerate NADH so that glycolysisproceeds uninterrupted in skeletal muscle. Lactate or pyruvate produced in the muscle cannotbe utilized for the synthesis of glucose due to the absence of the key enzymes of gluconeogenesis(glucose-6 phosphatase and fructose-1, 6-bisphosphatase).
The plasma membrane is freely permeable to lactate. Lactate is carried from the skeletalmuscle through blood and handed over to liver, where it is oxidized to pyruvate. Pyruvate, soproduced, is converted to glucose by gluconeogenesis, which is then transported to the skeletalmuscle.
The cycle involving the synthesis of glucose in liver from the skeletal muscle lactate and thereuse of glucose thus synthesized by the muscle for energy purpose is known as Cori cycle(Fig. 6.9).
Fig. 6.9: Showing steps of Cori cycle

72 Biochemistry for Dental Students
REGULATION OF BLOOD SUGARNormal blood sugar level ranges between 80 -120 mg%. Following a carbohydrate containingmeal, concentration of sugar in blood may rise transiently to about 150 mg/dl, which usuallyreturns to normal within 2 hours.
The concentration of glucose in blood is the net resultant of the following two processes:a. Rate of glucose entrance into the blood stream.b. Rate of glucose removal from the blood stream.
Means by Which Sugar is Added to the Blood
1. By absorption from the intestines.2. By glycogenolysis (by breakdown of liver glycogen)3. By gluconeogenesis (Fig. 6.10).
Means by Which Sugar is Removed from the Blood
1. Glycogenesis (glucose is converted into liver glycogen and muscle glycogen)2. In the synthesis of fats (i.e., triglycerides)3. In the synthesis of glycoproteins, nucleic acids, lactose (during lactation), etc.4. Loss in urine (Fig. 6.10).
• A balance of above these two processes will keep the blood sugar within normal range.• Balance between the ‘in’ and ‘out’ of sugar may be summarized as in figure.• These two processes are influenced by a number of factors under physiological conditions.• The blood glucose level is most efficiently regulated by a mechanism in which liver,
extrahepatic tissues and a battery of hormones play an important role.
Fig. 6.10: Showing input and output of glucose in blood stream

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 73
1. Role of Liver
Liver, being the centre of all metabolic activities is mainly responsible for the regulation ofblood glucose level. In liver, exist:
i. The developed mechanism for uptake of glucose from the blood.ii. Mechanism for the conversion of glucose to glycogen (glycogenesis)
iii. Mechanism for the release of glucose from glycogen (glycogenolysis), andiv. Mechanism for the denovo synthesis of glucose from non-carbohydrate precursors
(gluconeogenesis).
2. Role of Extrahepatic Tissues
A. Role of muscles: Muscle glycogen does not contribute directly to the blood sugar due tothe absence of the enzyme, i.e. glucose-6-phosphatase. Glycogenolysis in the muscles provides
glucose to blood only through the formation of lactic acid which by Coris’ cycle is converted to
glucose in the liver.
B. Role of kidneys: These also exert a regulatory effect by reabsorbing glucose through thereabsorptive system of the renal tubules. When the blood glucose level rises above therenal threshold, then the excess glucose is expelled through urine (glucosuria).
3. Role of Hormones
Several hormones play an important role in the homeostatic mechanism of blood sugar level.Out of these, insulin is the only hypoglycaemic hormone whereas rest are hyperglycaemic. (tendencyto raise blood sugar level) in nature.Insulin: It plays an important role in the regulation of blood sugar level. It’s secreted in theblood in response to hyperglycaemia. Insulin increases the transport of glucose across the cellmembrances. It decreases the level of blood sugar by increasing the utilisation of glucose byglycolysis, by decreasing hepatic glycogenolysis and by increasing glycogenesis.Hormones which raise the blood sugar level include (Fig. 6.11):
1. Epinephrine2. Glucagon3. Glucocorticoids4. Thyroxine5. Growth hormone,etc.
Mechanism by which these hormones increase the blood sugar level are:1. By increasing the absorption of glucose from the intestines.2. By decreasing the oxidation of glucose at the tissue level.3. By stimulating glycogenolysis.4. By stimulating gluconeogenesis5. By decreasing glycogenesis.

74 Biochemistry for Dental Students
Fig. 6.11: Showing hormonal regulation of blood glucose
Blood sugar level is kept normal by insulin by opposing the action of hyperglycaemichormones. Hormonal regulation can be compared with tug of war as showing Figure 6.12.Glucagon: It’s a polypeptide of 29 amino acids. Its secreted by the α-cell of the pancreaticislets. It produces rapid hepatic glycogenolysis by activating hepatic phosphorylase. Glucagonhas been regarded as part of a first line defence against hypoglycaemia.Epinephrine (Adrenaline): It stimulates the release of glucose from its store houses by activatingthe enzymes of the glycogenolytic pathway and it may be regarded as a hormone in the firstline of defence against hypoglycaemia. Gluconeogenesis is also stimulated by the influence ofadrenaline on the enzmes of this pathway.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 75
HORMONAL REGULATION OF BLOOD GLUCOSEGrowth Hormone
It’s hyperglycemic character was observed for the first time by Houssay in Argentina and FGYoung in London in 1924.
Adrenal Cortex hormones
Adrenal cortex secretes glucocorticoids which increase the rate of gluconeogenesis by increasingthe rate of breakdown of proteins and also by increasing the activity of transaminases.
Glucocorticoids also inhibit glucose utilization in extrahepatic tissues.
Thyroid hormones (T3 and T4)
These hormones are responsible for increasing gluconeogenesis, glycogenolysis and aminoacids production from proteins and so tend to elevate blood sugar level. However, side byside, the also stimulate insulin secretion with resulatant glucose uptake by peripheral tissuesand promotion of lipid biosynthesis. Thus, overall, they have got little effect on blood sugarlevel.
Hypothyroidism has a tendency to elevate blood sugar level and is a cause of diabetesmellitus and aggravates it.
DIABETES
Diabetes mellitus is a disease syndrome characterized by persistent hyperglycemia with orwithout glucosuria. This is the commonest endocrine disorder
Fig. 6.12: Tug of war showing hormonal action on blood glucose regulation

76 Biochemistry for Dental Students
Definition
Diabetes mellitus is defined as a state of chronic hyperglycemia which may be a result ofgenetic or environmental factors.
Classification
Diabetes mellitus is classified into two major clinical classes, i.e. insulin dependent [IDDM]and non-insulin dependent diabetes mellitus [NIDDM].
Insulin Dependent Diabetes Mellitus
It is due to the deficiency of insulin due to gradual depletion of β cells of islets of langerhans ofpancreas.
This type of diabetes mellitus is also called as type I diabetes mellitus.It is not associated with obesity and may be associated with acidosis or ketosis IDDM can
occur at any age of life. But, it usually occurs before 40 years of age. If it occurs at infancy (dueto congenital disorder) or in child hood, it is called Juvenile diabetes.
Causes of Type I Diabetes
1. Degeneration of β cells in the islets of Langerhans of pancreas.2. Destruction β cells by viral infection.3. Congenital disorder of beta cells4. Destruction of beta cells during autoimmune diseases due to development of antibodies
against beta cells.
Symptoms of Type I
Patients with IDDM can usually be recognized by the abrupt appearance of polyuria, (frequenturination), polydipsia (excessive thirst ) and polyphagia (excessive hunger) after triggered bystress or on illness.
These symptoms are usually accompanied by fatigue, weight loss and weakness.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 77
The diagnosis is confirmed by fasting blood glucose (greater than 14 g/100) commonlyaccompanied by ketoacidosis.
Blood glucose concentration rises to more than 200 mg/100 ml following the oraladministration of 75-100 g of glucose.
Glucose also appears in urine at this stage. In contrast, normal end individuals show fastingblood glucose level of 70-90 mg/100 ml and a rise to only about 130-140 mg/100 ml after aglucose load.
How to Control IDDM?
Patients with IDDM have virtually no functional B cells and rely only on exogenous insulininfected subcutaneously, in order to control the hyperglycemia and ketoacidosis. Insulininfection, does not cure the disease, but promotes glucose uptake by the tissues and inhebitsgluconeoginesis lipolysis and proteolysis.
NIDDM [Non-insulin dependent diabetes mellitus]: It usually occurs after 40 years ofage in the people who are obese so, it is called as maturity onset dialetes mellitus. It is veryrarely associated with ketosis.
This type of diabetes is also called as type II diabetes mellitus.
CAUSES FOR TYPE II DIABETES MELLITUSThe structure and function of β cells and the blood level of insulin are normal. The diabetesdevelops due to the absence or reduced number of insulin receptors in the cells of the body. Itis mostly on inherited disease.
Symptoms of Type II Diabetes Mellitus
NIDDM develops gradually without obvious symptoms. It is characterized by hyperglycemiaaften with hypertriglyceridemia.
Inspite of high levels of insulin, glucose levels are poorly controlled because of the lack ofnormal response to insulin, insulin resistance in these patients may be due to the increasedexpression of tumor necroses in adipocytes of the obese individuals.
In addition to insulin resistance, the disease is caused by impaired β cell function resultingin relative insulin deficiency. Hyperglycemia is mainly a result of poor peripheral utilizationof glucose, especially in muscle. Ketoacidosis does not develop because the adipocytes remainsensitive to the effect of insulin on lipolysis.

78 Biochemistry for Dental Students
Two forms of diabetes mellitus can be shown as Table 6.3
Table 6.3: Difference between two froms of diabetes mellitus
IDDM or Juvenile Onset NIDDM or Maturity Onset
Generally occurs below 40 years of age Occurs above 40 yearsNormal to wasted, means there occurs weight loss Patients are generally obese.Plasma insulin is absent due to destruction of B cell There occurs insulin resistancePlasma glucagon level is high (supressible) Plasma glucagon level is high (resistant)Ketoacidosis is acute complication Ketoacidosis is rare, hyperglycemia is acute
complicationPatients are responsive to insulin therapy but In this type patients are resistant to insulin therapyunresponsive to oral hyperglycemica drugs but responsive to oral hyperglycemia drugs.
How to Control NIDDM?
Blood glucose concentration is greater then 140 mg/100 ml, weight reduction and dietarymodification may correct the hyperglycemia of type II diabetes.
Hypoglycemic agents (sulphonylurea ) drugs or insulin therapy may be required to achievesatisfactory fall in blood glucose levels.
For any from of diabetes the metabolite derangements are due to an increased glucagon/insulin ratio. The patients usually present with 3 P, i.e.• Polyurea (increased excretion of urine)• Polydypsia (abnormal thirst)• Polyphagia (increased appetite)
GLUCOSE TOLERANCE TESTAlthough frank diabetes can usually be diagnosed by hyperglycemia in fasting condition, thediagnosis is not so clear in mild incipient cases. Because of no significant hike in glucose levelof blood in such cases. Under such doubtful conditions and certain other disorders, the diagnosiscan be ascertained more definitely by means of a glucose tolerance test.
The usual procedure of GTT is to determine the levels of blood glucose in fasting state andat various intervals after 75 g glucose load.
Administer orally a solution of pure glucose (75 g glucose should be dissolved in 250-350ml of water and should be asked to drink within 2-3 minutes; whereas in children the regimenis to give 1.75 g. glucose per kg body weight upto a maximum of 75 g) and determine theconcentration of glucose in the blood at intervals of 30,60,120 and 180 minutes after the glucoseis administered. Simultaneous samples of urine should also be collected, i.e. after 30,60,120 and 180
minutes for the detection of sugar qualitatively by Benedict’s test. In this way, in all, 5 blood and 5 urine
samples are collected.

Digestion, Absorption and Metabolism of Carbohydrates (Burning of instant fuel) 79
Precautions to be Taken before Performing OGTT
i. The oral carbohydrate intake should be 150 g on each of the three das immediately precedingthe test.
ii. Patient must not fast longer than 16 hours.iii. Patient must rest for 30 minutes before and also during the test.iv. All tests should be carried out in the morning because of diurnal variation in OGTT with
decreasing tolerance in the afternoon and evening.v. A wide range of drugs may affect OGTT which include steroids, oral contraceptives,
diuretics, nicotinic acid thyroid hormones, dilantin, etc. Ascorbic acid in high dose andother agents may also interfere with glucose estimation.
vi. Smoking is not permitted for at least one hour before and during the test.
Typical curves are shown below in Figure 6.13 for different conditions/disorders.
Fig. 6.13: Time in hours after glucose meal
SUMMARY1. Digestion is process in which there occurs converstion of complex food stuffs into simpler
ones which can be easily absorbed by gastrointestinal tract.2. The digestion of carbohydrates is initiated in the mouth by salivary α amylase and is
completed in the small intestine by pancreatic a amylase, oligosaccharides and disaccharides.3. The digestion is stopped in stomach due to infavorable pH.4. Monosaccharide are final absorbable products of carbohydrate digestion glucose is
transported into intestinal mucosal cells by carrier mediated Na+ dependent energyrequiring process.
5. The major pathways for carbohydrate metabolism are glycolysis, citric acid cycle,gluconeogenesis, glycogenesis, and glycogenolysis.

80 Biochemistry for Dental Students
6. Glucose the central molecule in carbohydrate metabolism is oxidized in glycolysis. Thiscycle takes place in aerobic or in an aerobic condition reducing in formation of pyruvatewith 8 ATP and lactate with 2 ATP respectively.
7. When glucose aerobically is converted into pyruvate then pyruvate is oxidativedecarboxylated in presence of pyruvate dehydrogenate complex to acetyl CoA.
8. Acetyl CoA is then completely oxidized in citric acid cycle which takes place in mitochondriain strict aerobic condition.
9. TCA.cycle is a common metabolic pathway for all food stuffs. Finally, one molecule ofglucose generates 38 ATP.
10. Gluconeogenesis is the conversion of non-carbohydrates into carbohydrates; the precursorsare amino acids, glycerol and lacticacid. It is a reversal of glcolysis with alternatearrangements for the irreversible steps.
11. When the precursor is lactate the pathway is called as Cori cycle.12. Glycogen is the storage form of glucose. Glycogenolysis in muscles takes place to meet
immediate energy requirements, while the liver glycogen maintains blood glucose level.13. Stable blood glucose level is maintained by the role of liver, muscles, kidney, muscular
exercise and a, b cells of Langerhans.14. The hormones like insulin is secreted as a direct response to hyperglycemia. It stimulates
liver to store glucose as glycogen and facilitates uptake of glucose into extrahepatic tissues.The hormones estrogen and progesteron cause increased liberation of insulin and thusdecrease the blood sugar level.
15. Glucagons is secreted as a response to hypoglycemia and activates both glycogenolysisand gluconeogenesis in liver causing release of glucose in blood.
16. The hormones of anterior pituitary, adrenal cortex, epinephrine and thyroid hormones areantagonists to insulin.
17. Diabetes mellitus is a state of chronic hyperglycemia.18. It is classified into IDDM or Juvenile diabetes mellitus and NIDDM or maturity onset
diabetes mellitus.

CHAPTER 7
Digestion, Absorption andMetabolism of Lipids(Consumption of fat depots for
energy generation)
Digestion of Lipids [Digesion Through Emulsification,Absorption Through Micelles Formation]
The most abundant fat in the human diet is triglycerides or neutral fats with smaller proportionof some phospholipids and cholesterol (mainly in the forms of esters).
Fats are digested due to hydrolysis by the action of enzyme lipase into fatty acids plusglycerol; in case of cholesterol ester, it is fatty acid+steroid.
Digestion of lipids starts in the stomach by lingual lipase which is acid stable enzyme.Gastric lipase digests small amount of fat in the stomach which is mostly tributyrin (butter
fat). Most of the fat is digested in the intestines by pancreatic lipase which remains present inbulk in the pancreatic secretion. There is some enteric lipase also secreted in the intestine, therole of which is not important.
The enzyme lipase is soluble in water but its substrates, the lipids are water-insoluble. So,lipase can attack on a lipid only at the water-oil interface. This is facilitated by emulsificationof lipids by bile supplied form the liver, it is present in the aqueous medium of the intestinallumen.The process of emulsification is brought about by three complementry mechanisms:1. Detergent action of bile salts.2. Surfactant action of degraded lipids.3. Mechanical mixing due to peristalsis.
1. Detergent action of bile salts: Bile salts are most effective biological emulsifying agents.They interact with lipid particles and the aqueous duodenal contents and convert them intosmaller droplets further, bile salts stabilize the smaller particle from preventing them fromcoalescing.

82 Biochemistry for Dental Students
2. Surfactant action of degraded lipids: The initial digestive products of lipids (catalysed bylipase) namely free fatty acids and monoglycerides promote emulsification. These compoundalong with phospholipid are known as surfactants. They are characterized by pocessing polarand non-polar groups. Surfactants get absorbed in the water lipid interfaces and increase theinterfacial area of lipid droplets. Thus initial action of lipase helps in further digestion of lipids.
3. Mechanical mixing due to peristalsis: Besides the action of bile salts and surfactants themechanical mixing due to peristalsis also helps in the emulsification of lipids.
Emulsification and Micelle Formation by Bile Acids
As a result, an emulsion is formed by the dispersion of the minute fat globules in the aqueousmedium, thus increasing the surface area of the fat by nearly 1000 fold. So, the emulsificationof fat is phenomenon of dispersion of lipids into smaller droplets due to reduction in surfacetension.
The attack of lipase, therefore, gets immediately increased though it is not in a commonsolvent with its substrate. The action of pancreatic co-lipase and phospholipase A2 (both arereleased from their precursor by the action of enzyme trypsin) in the presence of Ca++ ionsfacilitates the firm binding of the enzyme pancreatic lipase to the substrate at the Water-oilinterface. In this way, by the action of pancreatic lipase ester bonds are hydrolysed in theα - positions of a neutral fat, i.e. a triglyceride is rapidly hydrolysed firstly forming one moleculeeach of α-β - diglyceride and a fatty acid and finally one molecule each ofβ - monoglyceride and a fatty acid. Now by the action of yet another enzyme known as intestinalisomerase β-monoglyceride is converted to α-monoglyceride which in turn by the action ofenzyme intestinal lipase in the presence of water molecule in finally broken down to yield onemolecule each of glycerol and a fatty acid.
Phospholipase A2 has got a tendency to hydrolyse ester bond of phospholipids at β-positionforming free fatty acid and a lysophospholipid. Cholesterol esterase enzyme which is found inpancreas hydrolyses cholesterol esters yielding free fatty acid and free cholesterol. Thesedigested products are also ‘carried’ to the brush border by the bile salt micelle (Fig. 7.1).
Absorption of Lipids
Lipids are mostly absorbed in the duodenum and the jejunum. Lipids are hydrolysed yieldinga mixture of glycerol, diglycerides, monoglycerides and free fatty acids. Dietary lipids arenever digested completely in the alimentary canal. Hydrolysis of the trigycerides to diglyceridesand β- monoglycerides is relatively very difficult. The mixture of these intermediary hydrolyticproducts promotes the process of emulsification of the unhydrolysed dietary fats.

Digestion, Absorption and Metabolism of Lipids 83
Glycerol is fairly water-soluble and hence no difficulty is faced in its absorption. As soon asglycerol is formed, it is quickly absorbed. Most of the glycerol is absorbed through the bloodcapillaries.
Generally, fatty acids up to the chain length of 10 carbon atoms are primarily absorbedthrough the blood capillaries but fatty acids of higher chain length are primarily absorbedthrough the lymphatic route. The low molecular weight fatty acids are absorbed without muchdifficulty but the complexity goes on increasing as the molecular weight of the fatty acids goeson increasing. This is due to the fact that low MW fatty acids are relatively hydrophilic whereasthe high MW fatty acids are hydrophobic. The hydrophobic fatty acids can not be absorbed tillthese are brought into some soluble form. This is brought about by the formation of fatty acid-bile salt complexes which are more soluble and can be absorbed without much difficulty. Fattyacids can also be absorbed in combination of the steroids by forming more soluble esters.Thefatty acid present in the β-monoglycerides is hydrolysed within the mucosal cells by a distinctlipase which is found in these cells.
The short chain fatty acids (upto 10 carbon atoms) are transported directly into the bloodstream in the free form and get bound to the plasma albumin. These fatty acids comprisenonesterified fatty acid (NEFA) fraction. The fate of the longer chain fatty acids is different.These are converted into triglycerides by intermediate formation of the phosphatidic acidsand then carried away by the lymphatic system to the venous blood. The triglyceride thussynthesized in the mucosal cells are transported into the lymphatic circulation in two forms,namely, chylomicrons and invisible fatty particulates. An enzyme lipoprotein lipase presentin the blood stream is responsible for splitting of the complexes of chylomicrons and thusremoves milky appearance of blood. Previously, the name clearing factor was given to thisenzyme.
Fig. 7.1: Digestion of lipids

84 Biochemistry for Dental Students
Fig. 7.2: Absorption of lipids
Metabolism of Lipids
After absorption, lipids are either oxidised mainly in the liver or are stored in the depots (adiposetissue). For its utilization by the body. Triglycerides are first hydrolysed by lipases to releaseglycerol and free fatty acids. Glycerol is either converted to hexoses by gluconeogenesis orafter phosphorylation enters the glycolytic pathway. Fatty acids are oxidised to CO2 and H2Owith the liberation of large amount energy.
The undigested fat is finely emulsified by the intestinal movement in the presence of bilesalts, monoglycerides and diglycerides cholesterol and phospholipids to give fine particles ofthe dimensions of 0.1 to 0.5 μ. These particles have been named as micelles. The micelles havea disk shaped structure with lipid, monoacylglycerol, fatty acid, cholesterol and phospholipidsat the interior and bile salts at the periphery. The hydrophilic groups of lipids are oriented tothe outside and hydrophobic group towards inside. In this fashion, the bile salt micelles exerta solublizing effect on the lipids. Theses micelles can be easily absorbed as such withoutundergoing any further hydrolysis. The micelles thus absorbed get accumulated in the spaceof the endoplasmic reticulum of the mucosal cells and are subsequently discharged into theintercellular space and corium of the villus. the diglycerides and monoglycerides absorbed inthis manner are resynthesized into triglycerides. These triglycerides are then transported bythe lymphatic circulation. Thus, about 95% of the total ingested lipids may be absorbed byboth the mechanisms (Fig. 7.2).
Cholesterol has been shown to be absorbed mostly in the free state and not as esters as wasbeing previously believed. However, absorption of cholesterol is followed by itsre-etherification.

Digestion, Absorption and Metabolism of Lipids 85
Oxidation of Fatty Acids
Oxidation of fatty acids takes place in mitochondria where the various enzymes for fatty acidoxidation are present close to the enzymes of the electron transport chain. β-oxidation of fattyacid is the oxidation of fatty acid at β carbonation, resulting in the elimination of the twoterminal carbons atoms as acetyl CoA leaving fatty acyl CoA which has two carbon atoms lessthan the original fatty acid.The β-oxidation of fatty acid involves three stages.
I. Activation of fatty acid in cytosol.II. Transport of fatty acids into mitochondria.
III. β-oxidation proper in mitochondrial matrix (Fig. 7.3).
I. Activation of Fatty Acids
First step in the oxidation of fatty acid is the activation of fatty acid, in cytoplasm. Fatty acidactivation occurs in presence of ATP and is catalysed by a thiokinase (acyl CoA synthetase.)Thiokinases are found both inside as well as outside of the mitochondria. Several thiokinasesare known, each of which is specific for a group of fatty acids, these are:
i. Acetyl CoA thiokinase for activating acetic, propionic and acrylic acids,ii. Short chain fatty acid activating enzyme for fatty acids with 4-12 carbon atoms, and
iii. Long chain fatty acid activating enzymes for unsaturated as well as long chain saturatedfatty acids. This reaction occurs in two steps. Fatty acid reacts with ATP to formacyladenylate which then combines with CoA to produce acyl CoA (Role of β-hydroxyγ trimethyl amino butyrate (carnitine).
II. Transport of Acyl CoA into Mitochondria
Role of β-hydroxy γ trimethyl aminobutyrate (carnitine). Fatty acyl CoA is impermeable throughinner mitochondrial membrane while enzyme for β-oxidation are present in the mitochondria.Therefore, after activation, the fatty acid (fatty acyl CoA) interacts with carnitine which helpsin its translocation across the inner mitochondrial membrane.
In the presence of carnitine palmityl acyl transferase I, present on the outer surface of theinner mitochondrial membrane, fatty acyl CoA interacts with carnitine and froms acylcarnitine.It passes through the inner membrane and is transferred to intramitochondrial CoA to reformfatty acyl CoA. This reaction is catalysed by carnitine palmityl transferase II present on theinner surface of the inner mitochondrial membrane (Fig. 7.4).
It should be noted that the coengzme used for activation is different from the one thatcombines with fatty acid in the nitochondria to form acyl CoA. Thus the cell has two saperatepools of CoA [Cytosolic and mitochondrial].

86 Biochemistry for Dental Students
Fig. 7.3: Showing reactions of β-oxidation of fatty acids (example is palmitic acid)

Digestion, Absorption and Metabolism of Lipids 87
III. βββββ-Oxidation Proper
1. After activation and entry of fatty acid into mitochondria, flavoprotein containing acylCoA dehydrogenase removes two hydrogen atoms from the α- and β-positions forming α,β-unsaturated fatty acyl CoA. Or Δ2 trans enoyl CoA.
2. Hydration: Enoyl CoA hydratase adds a molecule of water at the double bond as result ofwhich α, β- unsaturated fatty acyl CoA is converted to β-hydroxyacyl CoA.
3. Oxidation: In the presence of NAD+, β-hydroxyacyl CoA dehydrogenase oxidises β-hydroxyacyl CoA to from β-ketoacyl CoA.
4. Cleavage: Thiolase, in presence of CoA results in the cleavage of β-ketoacyl CoA to yieldacetyl. CoA and newly formedacyl CoA with two carbon lesser than the old one.The newly formed acyl CoA can again undergo similar set of reactions starting from the
second reaction and is finally degraded to acetyl CoA molecules (Fig. 7.3).
ATP Production During βββββ-oxidation of Palmitic Acid
If palmitic acid (C15 H31 COOH) undergoes β-oxidation it releases 8 molecules of acetyl CoA inseven rounds of the oxidative process. In each round of β-oxidation one molecule of FADH2
and one molecule of NADH+H+ are produced which generates 2 and 3 ATP molecules,respectively. Thus a total of 35 ATP are obtained in 7 rounds of the oxidative process. In addition,each acetyl Co’A molecule, when oxidised in citric acid cycle, gives 12 molecules of ATP.
Therefore, additional 96 molecules of ATP are produced from 8 molecules of acetyl CoA.Thus a total of 131 molecules of ATP are formed from palmitic acid.
Fig. 7.4: Carnitine shuttle for transport of activated fatty acids

88 Biochemistry for Dental Students
As two high energy phosphate bonds are hydrolysed (form one molecule of ATP which ischanged to AMP), 2 molecules of ATP are used in the activation of a molecule of fatty acid.Therefore, there is a net yield of 129 molecules of ATP when a molecule of palmitic acid (fattyacid with 16 carbons) is completely oxidised.
Oxidation of unsaturated fatty acids: Unsaturated fatty acids also activated transportedacross the inner mitochondrial membrane and undergo β-oxidation as the saturated fatty acids(Fig. 7.4). But since the presence of double bonds possess problem for the β-oxidation to proceed.This is overcome by two additional enzymes an isomerase and an epimerase. Due to presenceof double bond the oxidation of unsaturated fatty acids in general provides lesser energy thanthat of saturated fatty acids.
Metabolic Fates of Acetyl CoA
In the normal metabolic processes, as discussed above, oxidation of glucose in glycolysis aswell as the oxidation of fatty acids via β-oxidation produces acetyl CoA. It is mainly used inthe Kreb cycle. The other fates of acetyl CoA include the synthesis of fatty acids and cholesterol.Besides, a small quantity of acetyl CoA is also converted to ketone bodies in the liver (Fig. 7.5).
Fig. 7.5: Showing metabolic fate of acetyl CoA
Biosynthesis of Fatty Acid
Mammals can synthesize major portion of the saturated as well as the mononusaturated fattyacids. There are three systems for the synthesis of fatty acids:
I. Synthesis of fatty acids in cytoplasm.II. Chain elongation in mitochondria.
III. Chain elongation in microsomes.
I. Synthesis of Fatty Acids in Cytoplasm
This is the actual process for the biosynthesis of fatty acids in liver, mammary gland and adiposetissue. The enzyme system uses acetyl CoA as the starting material for the synthesis of medium

Digestion, Absorption and Metabolism of Lipids 89
chain fatty acids (such as palmitic acid). Synthesis occurs in cytoplasm mostly by the reversalof the β-oxidation process.
Acetyl CoA —————————> Fatty acids.
Acetyl CoA is produced in mitochodria from different sources such as pyruvate obtained fromcarbohydrates (aerobic glycolysis) and glucogenic amino acids, or directly from lipids(β-oxidation) and ketogenic amino acids. Since mitochondrial membrane is impermeable toacetyl CoA, it condenses with oxaloacetate and froms citrate. Citrate enters the cytoplasm andis degraded to acetyl CoA and oxaloacetate by ATP citrate lyase.
In cytoplasm acetyl CoA is first converted to malonyl CoA by biotin containing enzyme,acetyl CoA carboxylase, irreversibly. This reaction occurs in the presence of NADPH, ATP andCO2 (Fig. 7.6).
Biosynthesis of fatty acids requires fatty acid synthetase which is a multienzyme complexcontaining 6 enzymes and an acyl carrier protein (ACP). Six subunits of the multienzymecomplex are acetyl transacylase, malonyl transacylase, β- ketoacyl-ACP synthetase (condensingenzyme), β-ketoacyl-ACP reductase, β-hydroxyacyl–ACP dehydratase, and enoyl-ACPreductase.
The acyl carrier protein (ACP) has two – SH groups called pantotheinyl – SH group and thecysteinyl-SH group.1. Fatty acid synthesis starts with the transfer of an acetyl CoA to the cysteinyl – SH group of
ACP with the help of acetyl transacylase subunit of the fatty acid synthetase complex andforms acetyl –S synthetase (Fig. 7.7).
Fig. 7.6: Conversion of acetyl CoA to malonyl CoA
Fig. 7.7: Formation of acetyl–S synthetase

90 Biochemistry for Dental Students
Malonyl transacylase transfers malony CoA onto the pantothenyl–SH group of ACP toform malonyl-S-ACP (Fig. 7.8).
Fig. 7.8: Formation of malonyl-S-ACP
2. In the next step, the condensing enzyme (β-ketoacyl-ACP synthetase) causes condensationof acetyl-S synthetase with malonyl–S-ACP and forms acetoacetyl-S-ACP from acetoacetyl–S-ACP (acetoacetyl enzyme or β-ketoacyl enzyme) (Fig. 7.9).
Fig. 7.9: Formation of acetoacetyl enzyme
3. β-ketoacyl-ACP reductase with NAKPH+H+ reduces acetoacetyl-S-ACP to formβ-hydroxybutyryl-S-ACP (β-hydroxyacyl-S-ACP) (Fig. 7.10).
Fig. 7.10: Formation of β-hydroxybutyryl-S-ACP
4. β-hydroxyacyl-ACP dehydratase removes H2O from β-hydroxyacyl-S-ACP formingcrotonyl-S-ACP (Fig. 7.11).
Fig. 7.11: Formation of crotonyl-S-ACP
5. Crotonyl–S-ACP is reduced by enoyl-ACP reductase utilizing NADPH+H+ and is convertedto butyryl-S-ACP (Fig. 7.12).
Fig. 7.12: Formation of butyryl-S-ACP

Digestion, Absorption and Metabolism of Lipids 91
Butyryl-S-ACP again accepts a molecule of malonyl CoA and with the repeated rounds,chain elongation continues and finally palmityl CoA is synthesised. Deacylase removes CoAand forms palmitate
The reducing equivalents (NADPH+H+) used in the biosynthesis of fatty acids are derivedfrom HMP shunt reactions.
II. Chain Elongation in Mitochondria
De novo synthesis forms plamitic acid which is used as starting material for the synthesis ofhigher fatty acids in mitochondria.
Chain elongation of palmitic acid in mitochondria takes place by the successive additionsof acetyl CoA. Condensation of palmityl CoA with acetyl CoA forms β-ketostearyl CoA whichutilises NADPH+H+ and is reduced to β-hydroxystearyl CoA. Removal of a molecule of waterconverts β-hydroxystearyl CoA to α, β-unsaturated stearyl CoA which is reduced to stearylCoA by using NADPH+H+.
III. Chain Elongation in Microsomes
The process of chain elongation in microsomes is similar to fatty acid biosynthesis (De novo
synthesis) in the cytoplasm. Although it also utilizes malonyl CoA but uses CoA insterad ofACP as the acyl carrier. Medium chain saturated fatty acids and monounsaturated fatty acidswith C18 (oleic acid) are used for chain elongation.
METABOLISM OF CHOLESTEROLThe metabolism of cholesterol includes• Synthesis of cholesterol• Metabolic fates of cholesterol.For chemistry of cholesterol, Its properties and occurance/distribution refer to chapter onchemistry of lipids.
Biosynthesis of Cholesterol
1. Site of synthesis: Essentially all tissues form cholesterol. Liver is the major site of cholesterolbiosynthesis, other tissues are also active in this regard, e.g. adrenal cortex, gonad, skin andintestine are most active brain of new born can synthesize cholesterol while the adult braincannot synthesize cholesterol.2. Enzymes: Enzyme system involved in cholesterol biosynthesis are associated with
a. Cytoplasmic particles “microsomes.”b. Soluble fraction cystol.

92 Biochemistry for Dental Students
3. Acetate: “Active acetate (acetyl CoA) is the starting material and principal precirsor.” Theentire carbon skeleton, all 27 –C of cholesterol in humans can be synthesized from active acetate(Fig. 7.13).
Fig. 7.13: Biosynthesis of cholesterol
Steps of Biosynthesis
The synthesis of cholesterol may be learn in five stages:1. Synthesis of HMG CoA.2. Formation of mevalonate (6C)3. Production of isoprenoid units (5C)4. Synthesis of squalene (30C)5. Conversion of squalene to cholesterol (27C).
1. Synthesis of β-hydroxy β-methylglutaryl CoA (HMG CoA)
Two moles of acetyl CoA condense to form acetoacetyl CoA. Another molecule of acetyl CoAis then added to produce HMG CoA.
2. Formation of Mevalonate
HMG CoA reductase is the rate limiting enzyme in cholesterol biosynthesis. This enzme ispresent in endoplasmic reticulum and catalyses the reduction of HMG CoA to mevalonate.
3. Production of Isoprenoid Units
In the three step reaction catalysed by kinases, mevalonate is converted to 3-phospho 5-pyrophosphomevalonate which on decarboxylation forms isopentenyl pyrophosphate (IPP).The latter isomerizes to dimethylallyl pyrophosphate (DPP). Both IPP and DPP are 5-carbonisoprenoid units.
4. Synthesis of Squalene
IPP and DPP condense to produce a 10-carbon geranyl pyrophosphate (GPP). Another moleculeof IPP condenses with GPP to form a 15-carbon farnesyl pyrophosphate (FPP). Two units offarnesyl pyrophosphate unite and get reduced to produce a 30-carbon squalene.

Digestion, Absorption and Metabolism of Lipids 93
5. Conversion of Squalene to Cholesterol
Squalene undergoes hydroxylation and cyclization utilizing O2 and NADPH and gets convertedto lanosterol. The formation of cholesterol from lanosterol is a multistep process with a seriesof about 19 enzymatic reactions. These enzymes are associated with endoplasmic reticulum.
DEGRADATION OF CHOLESTEROLCholesterol is converted into several compounds such as bile acids, steroid hormones andvitamin D3. Cholesterol is mainly excreted in the form of bile salts. While a large portion of thebiliary excretion of the bile salts undergoes enterohepatic circulation, unabsorbed bile salts areexcreated in the faeces (Fig. 7.14).
Fig. 7.14: Metabolic fates of cholestrol
Increased plasma cholesterol results in the accumulation of cholesterol under the tunicintima of the arteries causing atherosclerosis (arteriosclerosis). Progression of the disease resultsin narrowing of the blood vessels which may lead to intravascular thrombosis. High caloriediet or diet rich in saturated fats and cholesterol, hypercholestermia, sedentary life, stress andstrain, obesity, hypertension and smoking are the important contributory factors favorable forthe development of atherosclerosis. Dietary intake of fats rich in PUFA helps in transport andmetabolism of cholesterol and prevents atherosclerosis.
Ketone Bodies
Acetoacetate, β-hydroxybutyrate and acetone are collectively known as ketone bodies (acetonebodies). The process of the formation of ketone bodies is called ketogenesis. In a normal man,concentration of ketone bodies in blood is usually less than 3 mg/100 ml. In certain conditionssuch as during prolonged starvation or in impaired glucose oxidation (such as in diabetesmellitus), fat becomes the source of energy and its degradation is greatly accelerated. It resultsin the excessive production of acetyl CoA which cannot be fully utilised by the liver throughKreb’s cycle due to lack of oxaloacetate and is converted to ketone bodies. The clinical conditionresulting from the increased biosynthesis of ketone bodies is called ketosis. These abnormalmetabolites are diffused into the blood in greater concentrations (ketonemia) and appear inurine (ketonuria).

94 Biochemistry for Dental Students
Formation of Ketone Bodies
Formation of ketone bodies occurs mainly in the liver mitochondria since liver has highlyactive systems for the production of acetoacetate. Ketone bodies are formed by variousmechanisms:1. In liver, firstly 2 molecules of acetyl CoA condense and form acetoacetyl CoA which further
reacts with one more molecule of acetyl CoA producing HMG CoA, as already discussedunder cholesterol biosynthesis. HMG CoA lyase present in mitochondria splits HMG CoAto acetyl CoA and free acetoacetate.
2. Acetoacetyl CoA can also be converted directly to acetoacetate by CoA deacylase.3. In some of the extrahepatic tissues (kidney and muscle) acetoacetate is formed from
acetoacetyl CoA by transacylation with succinate.Acetoacetate is the parent compound synthesized in the body. It is subsequently reduced
by NADH dependent β-hydroxybutyrate dehydrogenase to from β-hydroxybutyrate. Some ofthe acetoacetate is also spontaneously decarboxylated by a nonenzymatic reaction and isconverted to acetone (Fig. 7.15).
Fig. 7.15: Synthesis of β-hydroxybutyrate and acetone
Both acetoacetate and β-hydroxybutyrate are strong acids. These may slowly deplete thealkali reserve of the body causing metabolic acidosis called ketosis.
Utilization of Ketone Bodies
Acetoacetate and β-hydroxybutyrate can be used as a source of energy in kidney and muscle.Although glucose is a major fuel for brain in the well nourished state but during starvationeven brain utilizes ketone bodies. These are transported from liver to the extrahepatic tissuesand are oxidised by Kreb cycle. the oxidation of ketone bodies to CO2 and H2O is called ketolysis.
Firstly, β-hydroxybutyrate dehydrogenase oxidises β-hydroxybutyrate to acetoacetate.Acetoacetate is then oxidised after its activation to acetoacetyl CoA either by transacylase orby thiokinase.1. Acetoacetate reacts with succinyl CoA in the presence of a transacylase also calledthiophorase to form acetoacetyl CoA and succinate (Fig. 7.16).

Digestion, Absorption and Metabolism of Lipids 95
Fig. 7.16: Reaction of acetoacetate with succinyl CoA
2. Acetoacetate thiokinase can directly activate acetoacetate (Fig. 7.17).
Fig. 7.17: Formation of acetoacetyl CoA
Thereafter acetoacetyl CoA thiolase splits acetoacetyl CoA to two molecules of acetyl COA(Fig. 7.18).
Fig. 7.18: Division of acetoacetyl CoA thiolase
Acetone is oxidised very slowly. It may be converted to acetoacetate by a reversal ofdecarboxylation. Acetone may also be converted to propionic acid via propane-diol.
Role of Liver in Lipid Metablism
Lipis are though mainly stored in the adipose tissue, liver has a central role in lipid metabolism.1. Liver is the important site for the synthesis of fatty acids from acetyl CoA, obtained from
the oxidation of glucose.2. It is also the important site for the biosynthesis of cholesterol from acetyl CoA, obtained
from the oxidation of carbohydrates, fatty acids and certain amino acids.3. Liver is also the site for the synthesis of the various plasma lipoproteins and phospholipids
as well as for their removal.4. Formation of ketone bodies occurs in liver.5. It is also the site for fatty acid chain elongation, shortening of fatty acid chain, and for the
removal as well as introduction of the double bond in a fatty acid.6. Liver is the sole site for the synthesis of bile acids from cholesterol.7. Liver is also important for the oxidation of fatty acids (β-oxidation )

96 Biochemistry for Dental Students
Hormonal Control of Lipid Metabolism
Various hormones may have important effects on lipid metabolism.
Insulin—Insulin stimulates HMP shunt reactions and increases the supply of NADPH whichis essential for the synthesis of long chain fatty acids and cholesterol. Insulin also increases thesynthesis of triglycerides in liver as well as adipose tissue. Since insulin is the main hormonewhich stimulates glucose utilization, it also depresses ketogenesis and increases the supply ofoxaloacetate for utilization of acetyl CoA via Krebs cycle.
Glucocorticoids—These hormones increase the rate of release of fatty acids from adipose tissuewhich in turn leads to ketogenesis and increases cholesterol synthesis.
Thyroid hormones—Administration of thyroid hormones reduces plasma lipoproteins, cholesteroland phospholipids but in insulin deficiency thyroid hormones increase the release of fattyacids from the adipose tissue and cause ketogenesis.
SUMMARY1. Triacylglycerols (TG) are highly concentrated form of energy, stored in adipose isssues.
Lipase the hormone sensitive enzyme cleaves TG to free fatty acids. Lipid absorption occursthrough mixed micelles formed by association with products of lipid digestion.
2. Fatty acids are activated (Acyl COA) and transported by carnitine to mitochondria wherethey get oxidized (mostly β type).
3. Fatty acid biosynthesis occurs from acetyl CoA in the cytosol through the involvement ofa multienzyme complex associated with acetyl carrier protin. (ACP).
4. Cholesterol is synthesized from acetyl CoA in aseries of reactions involving HMG CoA,mevalonate, isoprenoid units and squalene as intermediates cholesterol serves as a precursorfor bile acids, steroid hormones and vitamin D.
5. Excessive utilization of fatty acids occurs in uncontrolled diabetes mellitus and starvation.This results in over production of ketone bodies (in liver), namely acetone acetoacetic acidand β hydroxybutyric acid. The last two ketone bodies serve as energy source for peripheraltissues.
6. Liver has a central role in lipid metabolism.7. The hormones like insulin, glucocorticoids and thyroid hormones regulate lipid metabolism.

CHAPTER 8
Digestion, Absorption andMetabolism of Proteins
PROTEIN TO AMINO ACIDS TO CELLSThe proteins which are subjected to digestion are obtained from two sources—dietary andendogenous.
Proteins are degraded by a class of enzymes namely hydrolases which specifically cleavethe peptide bonds therefore known as peptidases which are divided into two groups.1. Endopeptidases: These are a type of hydrolases which attack on the internal peptide bondsto release peptide fragment, e.g. pepsin, trypsin.2. Exopeptidases: These enzymes act on the peptide bonds of terminal amino acids they aresubdivided into carboxypeptidases (C terminal end) and aminopeptidases (N terminal ends).
The proteolytic enzymes responsible for digestion of proteins are produced by stomachpancreas and intestine. Proteins are not digested in mouth due to lack of digestive enzymes insaliva.
DIGESTION IN STOMACH BY GASTRIC ENZYMESProtein digestion starts in stomach. Gastric juice produced by stomach contains HCl, pepsinogenand renin in infants and children.
HCl
The pH of stomach is less than 2 due to presence of HCl which is secreted by oxyntic or parietalcells of stomach. It has got two functions:1. Denaturation of proteins and killing of microorganisms2. Activation of pepsinogen to pepsin.
Pepsin
Pepsin in Greek pepsis means digestion, is produced by serous cells of stomach as pepsinogenand it is activated either by HCl or by autocatalysis. It is active at an optimum PH-2. Pepsinbelongs to the endopeptidase class of enzyme. It is acid stable enzyme.

98 Biochemistry for Dental Students
Digestion of proteins results in the formation of proteose, peptones and polypeptides and afew amino acids which are responsible for the secretion of a hormone cholecystokinin fromduodenum.
Renin
This enzyme is also called as chymosin, it is found in the stomach of infants and children andit is involved in the curdling of milk it converts casein to calcium paracaseinate renin is absentin adults.
DIGESTION OF PROTEINS BY PANCREATIC ENZYMESThe enzymes of pancreatic juice are secreted in inactive form. The processes are initiated byrelease of two hormones secretin and cholecystokinin from intestine.
The key enzyme for activation of zymogen to their active form is enteropeptidase orenterokinase from intestinal mucosal epithelial cells (Duodenum).
Enteropeptidase activate trypsinogen to trypsin which is an important endopeptides ofpancreatic juice. Further trypsinogen is activated by autocatalysis.
Other pancreatic enzymes responsible for protein digestion are chymotrypsinogen, andcarboxypeptidase. Both of them are activated by trypsin.
Trypsin and chymotrypsin are endopeptidases and active at neutral pH. The gastric HCl isneutralized by pancreating NaHCO3 which creates a favorable pH for the activity of theseenzyme. Carboxypeptidase breaks the terminal bonds of protein molecule. It is an exopeptidaseclass of enzyme. By the action of carboxypeptidase the dipeptides, tripeptides and poly peptidesare converted into amino acids.
DIGESTION OF PROTEINS BY SMALL INTESTINAL ENZYMESThe terminal; surface of small intestine contain amino peptides dipeptides and tripeptides.These enzyme act on large polypeptides and some of the left over dipeptides and tripeptidesand convert these proteins into final stage of single amino acid which can be easily absorbed.
Aminopeptidase cleave the amino terminal ends and other two enzymes of pancreatic juiceare elastase and collagenase, Elastase acts on elastic fibres and collagenase on colleagens (Fig.8.1).
ABSORPTION OF AMINO ACIDSThe free amino acids and to some extent di-and tripeptides are also absorbed by intestinalepithelial cells. The di-and tripeptides are hydrolysed in to free amino acids in to the cystol ofepithelial cells.

Digestion, Absorption and Metabolism of Proteins 99
The small intestine possesses an efficient system for absorption of amino acids. Aminoacids are absorbed more rapidly than D amino acids. The transport of L amino acid occurs byactive transport mechanism while that of D amino acid occurs by passive transport.
There are about six transport systems which are responsible for absorption are:1. For short chain neutral amino2. For long chain neutral amino3. For acidic amino4. For basic amino5. For imino acids6. For β amino acids (β alanine, taurine).
Fig. 8.1: Showing summary of digestion of proteins

100 Biochemistry for Dental Students
Mechanisms for absorption1. By Na dependant active transport linked with transport of Na along concentration gradient,sharing a common carrier.2. By γ glutamyl cycle where glutathione is responsible for active transport.
ABSORPTION OF INTACT PROTEIN AND POLYPEPTIDESFor a short period immediately after birth the small intestine of infants can absorb intact proteinsand polypeptides. The uptake of protein is occurred by endocytosis or pinocytosis. It is veryimportant for the transfer of maternal immunoglobulins to the off springs (Fig. 8.2).
Fig. 8.2: Digramatic presentation of digestion of proteins

Digestion, Absorption and Metabolism of Proteins 101
METABOLISM OF PROTEINSWhen we eat something it is first digested and then matabolized and finally excreted.As we know that the proteins are formed from repeated units of amino acids, we can say
that the metabolism of proteins is the metabolism of amino acids that is protein metabolismcan be more appropriately learnt as metabolism of amino acids.
In our body it is supposed that there is an imaginary pool which is called as amino acidpool. It includes the places like plasma, tissue fluid, etc. The amino acid pool is the simplificationof facts, there is no any particular compartment in body which is said to be amino acid pool100 gm of amino acids are there which are always free and contribute to the pool of aminoacids. In the amino acid pool of the body the concentration of amino acids or the amount ofamino acids is maintained to be constant.
There are some sources that contribute (Input) and there are some metabolic path wayswhich utilize (output) the amino acids, so inpuit is equal to out put to maintain the constancyof the pool (Fig. 8.3).
Fig. 8.3: Overview of body’s amino acid pool-sources and utilization

102 Biochemistry for Dental Students
INPUTI. Sources of Amino Acid Pool
1. Breakdown of body proteins: It is estimated that about 300-400 gm of proteins are degradeddaily for example plasma proteins, digestive enzymes are rapidly degraded.
2. Dietary proteins:– This is the other source of body amino acid pool. The dietary protein isrequired to maintain the nitrogen balance because due to degradation of amino acids thereis a loss of nitrogen from the body and purpose of dietary protein is to supply amino acidsspecially essential amino acids, to synthesize proteins and other nitrogenous compounds.
3. Non-essential amino acids: The amino acids which can be synthesized in the body belong tothe third source for the body amino acid pool.
II. Utilization of the Amino Acids (Output) from Amino Acid Pool
1. Synthesis of body proteins: Most of the proteins which are degraded daily are resynthesizedfrom the amino acids which are present in amino acid pool.
2. Many non-proteineous compound, e.g. purines and pyramidines are synthesized by theamino acids of amino acid pool.
3. About 10-15% of body energy requirement is met by the amino acids of amino acid pool4. The amino acids can be converted to carbohydrates (gluconeogenesis) and fats (ketogenesis)
from the pool.
CATABOLISM OF AMINO ACIDS
In this topic we shall consider how nitrogen is removed from amino acids. Amino acid catabolismstarts with the removal of amino group as ammonia. Although it takes place is several tissues,liver is major site of removal of ammonia from amino acids.
Biomedical Importance
Ammonia derived mainly from amino nitrogen of amino acid is very toxic to humansspecially the CNS of human beings, therefore they convert ammonia to the highly solublenontoxic substance urea, and these higher mammals are called as ureotelic, similarlyorganisms like fish, they excrete free ammonia as the end product, therefore they are calledas ammonatelic, and the organism which excrete uric acid (birds and amphibians) are callsas uricotelic animals.

Digestion, Absorption and Metabolism of Proteins 103
Biosynthesis of Urea
The biosynthesis of urea is divided into four stages for discussion:1. Transamination2. Deamination3. Transport of ammonia4. Reactions of urea cycle.
Definition of Transamination
Transamination is a reversible reaction in which NH2 group of one amino acid is transferred toa ketoacid resulting is formation of new amino acid and new ketoacid.
Transamination as the name suggesting, is transfer of NH2 group. It is the inter conversionof amino acids and ketoacid, they react together and they will form another amino acid andanother ketoacid, so the former amino acid and ketoacid are converted to later amino acid andketoacid. This reversible set of reactions is catalysed by the enzyme called as transminases andrecently these are called as aminotransferases (Figs 8.4A and B).For example:
Fig. 8.4A: Showing transamination reaction calalysed by enzyme SGOT. B6 = Pyridoxal phosphate
Fig. 8.4B: Showing transamination reaction catalysed by SGPT where B6 is pyridoxal phosphate

104 Biochemistry for Dental Students
In this reaction pyridoxal phosphate acts as coenzyme, this mechanism plays a part both inbreakdown of amino acid and in formation of new amino acids (Non-essential type). Most ofthe amino acids (but not all) take part in transamination reaction where glutamic acid andaspartic acids are most reactive. Lysine and threonine do not take part in this transamination.This process is reversible and it is very important for the redistribution of amino groups andproduction of non-essential amino acids as per requirement in the cell (Fig. 8.5).
Diagnostic significance of transaminases:
Enzyme More raised inGOT [AST] Cardiac disorders (Myocardial infarction)GPT [ALT] Liver disorders (Viral hepatitis)
Deamination
It is the process by which amino group of amino acid is removed in the form of ammonia. Themain organs responsible for deamination are liver and kidney.
Deamination may take place as a result of the removal of electrons which requires oxygen(oxidative deamination) or without the transfer of electrons (non-oxidative deamination).
Oxidative Deamination: Oxidative deamination is liberation of free NH3 from amino acid coupledwith oxidation. Liver and kidney contain several enzymes which catalyze the deamination ofamino acids such as glutamic acid is the only amino acid which undergoes oxidativedeamination at an appreciable rate and therefore through Transmination, the amino group ofmost of the amino acid is transferred to α ketoglutarate to produce glutamic acid and thusglutamic acid is termed as collection centre. L Amino acid oxidases, D amino acid oxidases andglutamate dehydrogenase are the enzymes responsible for it.The process of oxidative deamination takes place in two steps:1. The amino acid is first dehydrogenated by amino acid oxidases forming a keto acid.2. In the second step water molecule is added spontaneously and decomposes to the
corresponding a keto acid with loss of a imino nitrogen as NH3 (Ammonia).
Fig. 8.5: Showing summarized transamination reaction

Digestion, Absorption and Metabolism of Proteins 105
Removal of L amino group from L glutamate is catalysed oxidatively, by L glutamatedehydrogenase, since in this reaction the process of transamination is coupled with oxidativedeamination, it is called transdeamination.
Non-oxidative Deamination: Some amino acids can be deaminated without undergoing oxidation.Deamination of some of the amino acids such as serine, cysteine and histidine is catalised bydehydratase, desulphydrases, and histidase, respectively. These enzymes also require pyridoxalphosphate as a coenzyme. The enzyme causes dehydration of the amino acid followed by thespontaneous deamination non-oxidatively resulting in removal of NH3 (Fig. 8.6).
Fig. 8.6: Showing nonoxidative deamination
Transport of Ammonia
Ammonia is absorbed from the intestine in to portal venous blood which contains relativelyhigh concentration of NH3 as compared to systemic blood. Under normal conditions liverremoves the NH3 from the portal blood so that, blood leaving the liver is free from ammonia,this is essential since ammonia even in minute quantity is toxic to CNS.Normal blood concentration of NH3.
Normal NH3 level is 40-70 μg/100 ml free NH4 + (ammonium ion) concentration of freshplasma is < 20 μg/100 ml.
Such low concentration suggests that the mechanism for removal of this highly toxicsubstance is extremely efficient.
UREA CYCLEThe major pathology of nitrogen excretion in humans is as urea synthesized in liver, releasedinto blood and cleared by kidneys. Urea cycle was the first metabolic cycle which was elucidatedby Hanskrebs and Hart Henseleit hence it is also known as Krebs-Henseleit cycle.
Urea cycle includes formation of urea from one molecule each of ammonium ion, CO2
(activated with mg++ and ATP), and of L amino nitrogen of aspartate. The overall process,

106 Biochemistry for Dental Students
requires 3 molecules of ATP ( 2 of which are converted to ADP + Pi and 1 is converted to AMP+ ppi), and the successive participation of 5 enzymes catalyzing reaction of 6 amino acidsinvolved in urea synthesis. One (N acetyl glutamate) functions as an enzyme activator, ratherthan as an intermediate.
Urea formation is a five step cyclic process with five distinct enzymes. The ornithine usedin reaction 2, is regenerated in reaction 5. There is consumption of NH4
+, CO2, ATP and aspartate.
Fig. 8.7: Flow chart for urea cycle
Reaction of Urea Cycle (Fig. 8.7)
Step 1: In the first step ammonia is activated by ATP and combined with carbon dioxide toform carbamoyl phosphate in the mitochondrial matrix. The reaction is catalyzed by carbamoylphosphate synthetase which require N acetyl glutamate as the enzyme activator.Step 2: Ornithine transcarbamoylase transfers the carbamoyl group from carbanoyl phosphateto ornithine to produce citrulline. This reaction also takes place in mitrochondrial matrix ofliver.Step 3: In presence of argino succinic acid synthetase and ATP, citrulline combines with Laspartate to form arginosuccinic acid. This step requires ATP which is cleaved into AMP andpyrophosphate (PPI) which is immediately brokendown to inorganic phosphate.

Digestion, Absorption and Metabolism of Proteins 107
Step 4: Subsequently, arginosuccinase hydrolyses arginosuccinic acid to liberate arginine andfumeric acid the latter is converted into malate by an enzyme fumerase. Malate is acted uponby malate dehydrogenase to produce exaloacetate which is transaminated to aspartate bytransaminase which is utilized again in synthesis of arginosuccinate.Step 5: In the last step, arginine is hydrolysed by arginase to form ornithine and urea. Thisornithine again enters the cycle. Arginase is mostly found in liver, while the rest enzymes ofUrea cycle are present in other tissues. For this reason arginine synthesis may occur to varyingdegree in other tissues but ultimate urea production can occur only in liver.
Fate of Carbon Skeleton of Amino Acid
After removal of the L amino group as ammonia and it’s conversion into urea, the carbonskeletons of the amino acids form amphibolic intermediates and are either converted to glucoseor to fats and ketone bodies.The end products of catabolism of different amino acids as well as their amphibolic nature isgiven in Table 8.1.
Table 8.1: Catabolism of different amino acids and their amphibolic nature
Amino acids End product of catabolism
Glucogenic amino acidsGly, Ala,Ser,Thr,Cys, ————————> pyruvateHis,Pro,Glu,Arg ————————> a ketoglutarateVal, met ————————> Succinyl CoAAsp ————————> Oxaloacetate
Glucogenic and ketogenic
phenylalaine, Tyrosine ————————> Fumerate and acetyl CoATryptophan ————————> Pyruvate and acetyl CoALysine ————————> a ketoglutarate and acetyl CoA
Ketogenic Levcine ————————> Acetyl CoA andAcetoacetyl CoA
Overall Reaction and Energetics of Urea Cycle
Urea cycle is irreversible and consumes 4 ATP. Two ATP are utilized for synthesis of carbamoylPhosphate. One ATP is converted to AMP and PPI to produce arginosuccinate which equals 2ATP. Hence, 4 ATP are actually consumed.

108 Biochemistry for Dental Students
Disposal of Urea
Urea is produced in liver after this urea is freely diffused and transported through blood intokidneys and excreted. A small amount of urea enters intestine where it is brokendown to CO2
and NH3 by bacterial enzyme Urease. Ammonia is either lost in faces or absorbed in to blood.So, it is observed that in patients of renal failure the blood urea level is increased (uremia)which results in more diffusion of urea in to intestine and more breakdown of urea to NH3 andCO2 which causes hyperammonemia, i.e. increased level of ammonia in blood which is veryvery toxic for the body.
SUMMARY1. Protein digestion beings in the stomach by pepsin which is aided by gastric HCl, pancreatic
proteases (trypsin, chymotrypsin and elastase) and intestinal amino peptidases anddipeptidases complete the degradation of proteins to amino acids and some dipeptides.
2. The intestinal absorption of amino acids occurs by different transport systems (six known).The up take of amino acids is primarily occurs by Na+ dependent energy requiring process.
3. Direct intestinal absorption of protein and polypeptides is observed in infants, immediately,after birth. This is important for the transfer of maternal immuonoglobulins (Via breastfeeding) to the offspring.
4. The body proteins are in dynamic state (degradation and synthesis) and there is an activeamino acids pool maintained for this purpose.
5. The amino acids under go transamination and deamination to liberate ammonia for thesynthesis of urea which is the non-toxic end product of protein metabolism.
6. Urea is excreted in urine and the carbon skeleton of amino acids is involved either in thesynthesis of glucose (glycogenic) or fat, (ketogenic) or both glucose and fat (glycogenic aswell as ketogenic).

Vitamins are essential compounds which are organic in nature present in natural foods,synthesized in body, required in minute amounts for normal growth development andreproduction, etc.They are classified as:
FAT SOLUBLE AND WATER SOLUBLE VITAMINS
COMMON PROPERTIES
A. Fat Soluble Vitamins
i. The fat soluble vitamins are apolar, hydrophobic molecules.ii. Bile, salts and fats are essential for their absorption.
iii. They are generally stored in liver.iv. Normally they are not exerted in urine.
B. Water Soluble Vitamin
i. They are soluble in water.ii. They are easily absorbed.
iii. They are not stored in body.iv. They have a threshold for urinary excretion.
CHAPTER 9
Vitamins(The accessory factors)

110 Biochemistry for Dental Students
Classification of Vitamins (Fig. 9.1)
VITAMIN AVitamin A is an aldehyde (Retinal) derived from β carotene.
Sources
i. Plant sources: All pigmented vegetables and food, e.g. sweet potatoes, carrots, pumpkins,papayas, tomatoes, apricots and peaches and leafy vegetables which supply pro-vitaminA (carotene) in the diet. Cereals also contain vitamin A.
ii. Animal Sources: Vitamin A is also supplied by foods of animal origin; they are liver, milk,butter, eggs, kidney, the fats of muscle, meats and fish liver, etc.
Daily Requirements
• Adults – 5000 IU• Pregnancy and lactation – 6000-8000 IU• Children – 2000-3000 IU• Infants – 1500 IU• 1 IU = 0.3 mg of retinal = 0.6 ug. of β carotene• Normal concentration in blood 24-60 IU/dl
Fig. 9.1: A chart for classification of vitamins

Vitamins (The accessory factors) 111
PHYSIOLOGICAL FUNCTIONS1. Role in vision: Vitamin A plays very important role in vision. Vitamin A is responsible for
physiological mechanism of vision specially in dim light. It plays a role in Wald’s visualcycle (Fig. 9.2).
Rods and cones: The retina of the eye possesses two types of cells rods and cones. The humaneye has about two million rods and 5 million cones. The rods are in the periphery and conesare at the centre of retina. Rods are involved in dim. Light vision, whereas cones are responsiblefor bright light and colour vision.Animals – such as owls and cats for which night vision is more important – possess mostlyrods.
Fig. 9.2: Wald’s visual cycle
Wald’s Visual Cycle
Rhodopsin (mol wt 35,000) is a conjugated protein present in rods. It contains 11-cis-retinaland the protein opsin. The aldehyde group (of retinal) is linked to ε-amino group of lysine (ofopsin).
The primary event in visual cycle, on exposure to light, is the isomerization of 11-cis-retinalto all-trans-retinol. This leads to a conformational change in opsin which is responsible for thegeneration of nerve impulse. The all-trans-retinol is immediately isomerized by retinal isomerase(of retinal epithelium) to 11-cis-retinol. This combines with opsin to regenerate rhodopsin andcomplete the visual cycle. However, the conversion of all trans-retinal to 11-cis-retinol is

112 Biochemistry for Dental Students
incomplete. Therefore, most of the all-trans-retinol is transported to the liver and converted toall-trans-retinol by alcohol dehydrogenase. The all-trans-retinol undergoes isomerization to11-cis retinal which is then oxidized to 11-cis retinal to participate in the visual cycle (Fig. 9.2).Dark adaptation time: When a person shifts from a bright light to a dim light (i.e. entry into acine theatre); rhodopsin stores are depleted and vision is impaired. However, within a fewminutes, known as dark adaptation time, rhodopsin is resynthesized and vision is improved.Dark adaptation time is increased in vitamin A deficient individuals.1. Vitamin A helps in maintaining the integrity of epithelial tissues as epithelial layers of skin,
respiratory mucosa, oesophagus and genitourinary tract.2. It helps in preservation of structural integrity and normal permeability of the cell membrane.3. It accelerates the normal formation of bones and teeth.4. Retinoic acid is more involved in glycoprotein synthesis. Thus vitamin A is involved in
development and maintenance of ground substances in collagen tissues.5. Vitamin A is involved in the synthesis of chondroitin sulphate.
Deficiency of Vitamin A
1. Xerophthalmia- Thickening and loss of transparency of bulbar conjunctiva.2. Follicular conjunctivitis.3. Keratomalacia or softening of cornea. Defective vision due to keratinization of epithelium
of cornea.4. Night blindness- (Nictalopia) – This is one of the earliest symptoms of it’s deficiency. It is
actually impairment of dark adaptation.5. Follicular hyperketosis of skin.6. Formation of renal calculi.
VITAMIN D [CALCITRIOL]The vitamin D are a group of compound. All the sterols occurring chiefly in animal organisms.They give rise to a hormone knows as calcitriol. Calcitriol has a role in calcium and phosphatemetabolism. Ergocalciferol [D2] is obtained from ergosterol and is present in plants, and [D3]cholecalciferol is found in animals (Fig. 9.3).
Sources: Liver and viscera of fish, milk, butter some amounts may be obtained by increasingadditional vitamin D in cow’s milk. Cheapest source is sun light which forms D3 from 7dehydrocholesterol in the skin. Biosynthesis of active form of vitamin D can be seen in Figure9.3.
Daily Requirements
• Infants and children – 400 IU• Adults – 200 IU

Vitamins (The accessory factors) 113
• Women during pregnancy and lactation – 400 IU• 1 IU = 0.025 μgm of cholecalciferol• Normal concentration in blood:
In adults – 700-3100 IU/LIn children – 860-2100 IU/L.
Physiological Functions
1. Vitamin D directly stimulates the intestinal absorption of calcium and indirectly that ofphosphate.
2. The major function of Vitamin D is to stimulate transcription of the mRNA for a calciumtransport protein. Thus, it is concerned with intestinal absorption, renal excretion and bonemetabolism of calcium.
3. It decreases the pH in lower intestinal tract which aids in increasing the absorption of calciumand phosphorus.
4. It is necessary for the development of bones and normal growth of the body.5. It stimulates the calcification of bones in both adults and growing children.6. It increases the citrate level of blood, bones, kidney and heart tissues and also the excretion
of citric acid.7. It stimulates the activity of phytase which catalyses the hydrolysis of phytic acid in the
intestine.
Deficiency Symptoms
1. During the period of skeletal growth vitamin D deficiency results in rickets with acharacteristic defect in endochondral bone growth. There occurs twisting of bones.
2. In fully grown bone in adults, the deficiency leads to osteomalacia. In osteomalaciademineralization of bones occurs because of which bones become softener which causeeasy fracturability.
VITAMIN EVitamin E refers to a group of compound known as tocopherols.
Sources
Good sources: Eggs, meats, liver, fish, chicken, oat meal, corn oil and cotton seed oil nuts.Daily requirements – 25-30 mg.Normal concentration in blood is 10 mg/ L

114 Biochemistry for Dental Students
Physiological Functions
1. Vitamin E protects the polyunsaturated fatty acid from oxidation by molecular oxygen inthe form of peroxides.
2. Vitamin E and other antioxidant such as vitamin C are important in inhibiting damage tolung tissue from antioxidants in air.
3. The tocopherols play part in the sterilization of cellular membrane and play some part inelectron transport together with appropriate protein.
4. The tocopherols prevent oxidation of vitamin A.
Fig. 9.3: Biosynthesis of active form of vitamine D

Vitamins (The accessory factors) 115
5. Vitamin E protects enzymes in muscle, nerves or gonads from destruction.6. It prevents the hepatic necrosis.7. It prevents development of cerebral disorders.8. It seems to be involved in heme synthesis.
Deficiency Manifestations
1. Increased susceptibility of erythrocytes to hemolysis by H2O2 and decrease in the erythrocytelife span in human adult males.
2. Anaemia, edema and skin changes are observed in infants.3. Permanent sterility in males.4. Increased oxygen consumption.5. Hepatic necrosis.
VITAMIN KVitamin K is a coagulation vitamin. It is nepthoquinine derivative
Sources
Best sources: Green leaf vegetables, e.g. alfalfa, spinach, cabbage, etc.Good sources: Cauliflower, Soya bean, wheat germ.Fair sources: Milk, meat and fish.Vitamin K is produced by most bacteria present in human intestine if it is not supplied in thediet.
Daily Requirement
The daily requirement of vitamin K is not reported yet.The average diet contains an adequate amount of vitamin K being synthesized by bacteria
in the intestine. So the vitamin K deficiency has not been reported in healthy individuals exceptin newborn infants fed on mother’s milk when the mother’s diet has a low vitamin K content.
Physiological Function
1. Vitamin K catalyses the synthesis of prothrombin by the liver.2. It reduces the prothrombin time.3. It regulates the synthesis of plasma clotting factors (Factors VII, IX and X)4. Vitamin K is an essential component involved in photosynthesis in green plants.5. Vitamin K is involved in the maintenance of normal levels of blood clotting factors II, VII,
IX and X.6. Vitamin K acts as cofactor of the carboxylase.

116 Biochemistry for Dental Students
Deficiency Manifestation
1. The deficiency of vitamin K lead to lowering of prothrombin level and increasing clottingtime.
2. Vitamin K deficiency cause hemorrhagic disease of newborns.3. Sterilization of large intestine by antibiotics can result in deficiency when dietary in take is
limited.
WATER SOLUBLE VITAMINSThe water soluble vitamins are synthesized from plant tissue except cobalamine which is storedin liver and not synthesized in plant tissues.
Ascorbic Acid (Vitamin C)
Properties
1. Ascorbic acid is a white crystalline water soluble substance with sour taste.2. It is chemically an enedeol actone which is oxidized to dehydroascorbic acid.3. The oxidation of ascorbic acid is catalysed by copper and silverions and the oxidation is
faster at higher temperature, for example during cooking of foods.4. It is a powerful reducing agent which can reduce Fehlings solution.5. It is easily destroyed by cooking.6. It is stable below pH 6.8 at room temperature but readily oxidized in an alkaline medium.
Sources
Richest sources: AmlaGood sources Citrus food, tomatoes, ray cabbage, guava, cauliflower, grapes. Apple, freshraw fish, etc.
Daily Requirements
• Infants – 35 mg• Children – 40 mg• Adults – 45 mg• Pregnant women – 60 mg• Lactating women – 80 mg
Normal concentration in blood:• 0.6-1.5 mg/100 ml of blood plasma.

Vitamins (The accessory factors) 117
Physiological Function
1. Since it is very sensitive to reversible oxidation, it is involved in oxidation reduction reactionof the cells.
2. It is involved in conversion of folic acid to folinic acid.3. It is involved in hydroxylation of steroids in adrenal cortex.4. It is required in the metabolism of tyrosine and phenylalanine and also in tryptophan.5. It is required for absorption of iron.6. It is involved in formation of norepinephrine.7. It is essential for normal regulation of colloidal condition of intercellular substances including
the fibrils and collagen of connective tissue, osteroid tissue, dentine and intercellular cementsuch of capillaries.
8. It is concerned in the hydroxylation of proline to hydroxy proline which is an importantconstituent of collagen.
9. It has an inhibitory effect on the hyaluronidase – hyaluronic acid system.
Deficiency
Since ascorbic acid deficiency produces scurvy. The signs of it’s deficiency entirely confined tobones, cartilages, dentine and connective tissues.
Scurvy is characterized by failure in the formation and maintenance of intercellular materialswhich cause typical symptoms such as:1. Internal hemorrhages.2. Loosening of teeth.3. Poor healing of wounds.4. Swelling of long bones.5. Easy fracturability of bones.6. Swelling, sponginess, tenderness and bleeding of gums.7. Anemia.8. Susceptibility to infections.9. General weakness.
THE VITAMINS OF B COMPLEX1. Thiamine (vitamin B1 anti-Beriberi substance)2. Riboflavin (vitamin B2, lactoflavin)3. Niacin (vitamin B3 nicotinic acid pellagra preventing factors)4. Pyridoxin (vitamin B6 rat anti-dermatitis, factors)5. Pantothenic acid – (B5 filterate factor, chick anti-dermatitis factor)6. Lipoic acid –(thicoctic acid protogen).7. Biotin (B7 vitamin H anti-egg white injury factor).

118 Biochemistry for Dental Students
8. Folic acid (vitamin B8, vitamin M)9. Inositol (Mouse anti-alopecia)
10. Vitamin B12 (cynocabalamin, cobamide, anti-pernicious anemia factor.)
Thiamine (Vitamin B1)
Sources
• Rich sources: Rice polishing wheat germs and yeast.• Other sources: Cereals, pulses, nuts, oil seeds, meat, fish, eggs, vegetables and fruits.• Thiamine is practically present in all plants and animal tissues commonly used as food.• Thiamine contained in this food is destroyed with improper cooking.
Daily Requirement
• Infants – 0.3-0.5 mg• Children – 0.7-1.2 mg• Adult (males) – 1.2-1.5 mg
(females) – 1.0-1.1mg• Pregnant and lactating women – 1.3-1.5 mg
Normal concentration of B1 in Blood.• About 1 ug/100 ml of plasma.
Physiological Role
1. Thiamin is essential for growth.2. It is essential for maintaining the nerves in normal condition.
Coenzyme Activities
Thiamine is converted to it’s active form thiamine pyrophosphate (TPP) by ATP dependentThiamine pyrophosphokinase which is present in brain and liver.
There are Three Types of Reaction
1. An oxidative decarboxylation of a ketoacids (α ketoglutarate, pyruvate and α ketoanalogsof leucine, isoleucine and valine).
2. Succinyl CoA formed from α ketoglutaric acid plays an important role in the biosynthesisof the porphyrin ring of haemoglobin and certain oxidases.
3. Transketolase reactions in (Pentose phosphate pathway).
All of these reactions are inhibited in thiamine deficiency.
Deficiency Manifestation
1. It’s deficiency causes beriberi, wet beriberi, dry beriberi and neurological beriberi.

Vitamins (The accessory factors) 119
2. The early clinical features in both froms of beriberi are common. The first symptoms are:a. Anorexia and dyspepsia associated with heaviness and weakness of legs.b. The subjects feel weak and get easily exhausted.c. If not treated, the subjects develops wet or dry beriberi.
WET BERIBERIa. Oedema is the important feature.b. Palpitation and breathlessness.c. The pulse is fastd. The heart becomes weak.
DRY BERIBERIa. The muscles become wasted and difficult to walk.b. The subject needs stick to stand and walk and finally becomes bedridden.c. The concentration of pyruvic acids and lactic acid are increased.d. The transketolase activity of red cells is decreased.
RIBOFLAVIN (Vitamin B2)
Sources
Richest sources: Anaerobic fermenting bacteriae, milk, liver, kidney,fish roots, germinatingwheat.
Physiological Functions
1. Riboflavin is involved in the regulatory function of some hormones connected withcarbohydrate metabolism.
2. The free riboflavin present in retina is converted by light to a compound involved instimulation of optic nerve.
Coenzyme Activities
1. It is constituent of some enzymes called flavoproteins which are involved in intermediatorymetabolism. They play role in the electron transport system in mitochondria.
2. Riboflavin in the form of FMN and FAD is a coenzyme in oxidation reduction reactions.3. It is also the prosthetic group of acyl CoA dehydrogenase which is involved in oxidation of
fatty acid (The role of FMN and FAD in different metabolisms can be studeed in Table 9.1).

120 Biochemistry for Dental Students
Deficiency Disorders
1. Characteristic lesion of the lips.2. Fissures at the angle of month (Cheilosis).3. Dermatitis of the faces.4. Certain functional disorder of organ and disorders of eyes.
NIACIN (Also called as B3)
(Nicotinic acid)
Sources
Richest sources: Yeast, rice polishing.Other sources: Meat, liver, eggs, tomatoes, green leafy vegetables.The amino acid tryptophan present in dietary proteins is converted into niacin in the body.
Daily Requirement
• Infants – 5-8 mg• Children – 9-16 mg• Adult (males) – 16-20 mg
(females) – 12-16 mg• Pregnant women – 14-18 mg• Lactating women – 16-20 mgNormal connection of niacin in whole blood – 0.5-0.8 mg/100 ml.
Table 9.1: Selected examples of FAD and FMN dependent enzymes along with their respective reactions
Enzyme Reaction
FAD DEPENDENTI. Carbohydrate metabolism
a. Pyruvate dehydrogenase complex Pyruvate ————> Acetyl CoAb. α-ketoglutarate dehydrogenase complex* α-ketoglutarate ————> Succinyl CoAc. Succinate dehydrogenase Succinate ————> fumarate
II. Lipid metabolism
d. Acyl CoA dehydrogenase Acyl CoA ————> α,β-unsaturated acyl CoAIII. Protein metabolism
e. Glycine oxidase Glycine ————> Glyoxylate + NH3
f. D-amino acid oxidase D-amino acid————> α-keto acid + NH3
IV. Purine metabolism
g. Xanthine oxidase Xanthine hypoxanthineFMN dependentL- amino acid oxidase L-amino acid ————> α-keto acid + NH3
• Dihydrolipoyl dehydrogenase component requires FAD.

Vitamins (The accessory factors) 121
Physiological Functions
1. Nicotinic acid is essential for the normal functioning of skin; intestinal tract and the nervoussystem.
Coenzyme Activities
1. Nicotinic acid principally occurs as nicotinamide is component of two coenzymes NADand NADP.
2. These coenzyme play an important role in metabolism by acting as hydrogen and electrontransfer agent. (The selected examples of NAD dependent enzymes in different metabolismscan be seen in Table 9.2).
Table 9.2: Selected examples of NAD+ dependent enzymes along with their respective reactions
Enzyme Reaction
NAD+ dependentI. Carbohydrate metabolism
a. Glyceraldehyde 3-phosphate Dehydrogenase Glyceraldehyde 3-phosphate ————> 1,3 -Bisphosphoglycerate
b. Lactate dehydrogenase Pyruvate ————> Lactatec. Pyruvate dehydrogenase complex Pyruvate ————> Acetyl CoAd. α-ketoglutarate dehydrogenase complex α-ketoglutarate ————> Succinyl CoA
II. Lipid metabolism
a. β-hydroxy acyl CoA dehydrogenase β-Hydroxy acyl CoA ————> β-keto acyl CoAb. β-hydroxybutyrate dehydroigenase β-Hydroxybutyrate ————> Acetoacetatec. Alcohol dehydrogenase Alcohol ————> Acetaldehyde
III. Protein metabolism
a. Branched chain α-keto acid dehydrogenase α-keto acids of branched chain amino acids (Leu,b. Tyramine dehydrogenase Lie,Val) ———> Corresponding acyl CoA
thioestersTyramine p-Hydroxyphe acetate
NAD+ or NADP+ dependenta. Glutamate dehydrogenase Glutamate ————> α-ketoglutarate + NH3
b. Isocitrate dehydrogenase Isocitrate ————> OxalosuccinateNADP+ dependent
a. Glucose 6-phosphate dehydrogenase Glucose 6-phosphate ————>b. Malic enzyme 6-phosphogluconolactone
Malate ————> PyruvateNADPH dependent
a. 3-ketoacyl reductase 3-ketoacyl enzyme ————> 3-hydroxy acyl enzymeb. hMG CoA reductase hMG CoA ————> Mevalonatec. Squalene epoxidase Squalene ————> Squalene oxided. Cholesterol 7 α-hdroxylase Cholesterol ————> 7α-Hydroxycholesterole. Phenylalanine hydroxylase Phenylalanine ————> Tyrosinef. Dihydrofolate reductase Folic acid ————> Tetrahydrofolic acid

122 Biochemistry for Dental Students
Deficiency Disorders
The deficiency of niacin causes the disease Pellagra. The clinical features include 3 D dermatitis,diarrhoea, and dementia (Headache, depression, anxiety, insomnia, forgetfulness).
PYRIDOXINE [B6]Sources
• Yeast, rice, polishing, cereals like wheat and corn.• Other sources: Milk, meat, eggs, leafy vegetables.
Daily Requirement
• Infants – 0.3 mg• Children – 0.6-1.2 mg• Adult (males) – 1.6-2.0 mg
(females) – 1.6-2.0 mg• Pregnant and lactating women – 2.5 mg
Physiological Functions
1. Phridoxine is essential for the growth of infants.
Coenzymes Activity
1. The active derivative of pyridoxine is pyridoxal phosphate functions as codecarboxylase.2. The deaminases (dehydrase) for serine and threonine are also catalysed by pyridoxal
phosphate acting as coenzyme.3. Pyridoxal pO4 is involved in the synthesis of CoA from pentothenic acid.4. Pyridoxal phosphate is concerned with immune response.
Deficiency Disorders
Deficiency gives rise to irritability and depression in some cases there is; lymphopenia andPeripheral neuropathy.
PANTOTHENIC ACID (B5)Sources
Richest sources: Jelly, yeast, rice polishing, wheat germ, eggs and leafy vegetables.

Vitamins (The accessory factors) 123
Daily Requirement
• Infants-1-2 mg• Children – 4-5 mg• Adult (males) – 5-10 mg
(females) – 5-10 mg• Pregnant and lactating women –10-15 mg
Physiological Functions
1. Pantothenic acid is essential for the growth of infants and children.
Coenzyme Activities
a. Pantothenic acid as the constituent of CoA is required for several fundamental reactions inmetabolism.
b. Coenzyme A combines with acetate to form active acetate (Acetyl coenzyme A) which isdirectly utilized by combination with oxaloacetic acid to form citric acid which initiatescirtric acid cycle.
c. Acetyl CoA derived from carbohydrates fats or many of the amino acids undergoes furthermetabolism through the “common metabolic pathway”.
d. Coenzyme A in the form of acetyl CoA is also required for the synthesis of cholesterol andthus of the steroid hormones.
Deficiency Symptoms
1. Deficiency of this vitamin results in nausea, vomiting, certain gastrointestinal disorders,anemia.
2. Burning foot syndrome in this disease there is reduced capacity of acetylation.
FOLIC ACIDSources
Richest sources – Yeast, liver, kidneyOther sources – Meat, fish, green leafy vegetables.
Daily Requirement
• Infants – 50 ug• Children – 100-300 ug

124 Biochemistry for Dental Students
• Adult – 400 ug• Pregnant – 800 ug• Lactating women – 600 ug.• Normal level– 3-25 ug/l of serum
Physiological Functions (Coenzyme Activities)
1. Folic acid as a coenzyme is involved in the transfer and utilization of single carbon moiety.2. Since folic acid coenzyme take part in the synthesis of purines and pyrimidines of DNA
they are fundamentally involved in growth and reproduction of cells.3. Folic acid coenzymes not only confined to the hemopoietic system but also generalized
throughout the body.4. Involved in development of RBC.
Deficiency Symptoms
The deficiency of folic acid gives rise to megaloblastic anemia. The nuclei of the nutrophilcontain more than the normal number of lobes. Megaloblastic anemia is associated withmacrocytic changes which include abnormally large RBC. Other deficiency symptoms includeretardation of growth, weakness, infertility, etc.
VITAMIN B12
Sources
Vitamin B12 is present in foods of animal origin. It is not present in foods of plant origin. Bacterialsynthesis of cobalamine occurs in human intestine richest sources: liver kidney. Other sourcesare: Meat, fish, eggs, etc.
Daily Requirements
• Infants –0.3 μg• Children – 1.2 μg• Adult – Males – 3.0 μg
Female – 3.0 μg• Pregnant and lactating women – 4.0 μg• Normal concentration in blood – 160-1000 μg/ml
Physiological Functions
1. Vitamins B12 along with folic acid is required for the development of red blood cells beyondmegaloblast stage.

Vitamins (The accessory factors) 125
2. It stimulates the appetite and general health of human beings.3. It cures the neurological symptoms of pernicious anaemia.4. It acts as supply the total methionine requirement and therefore, this amino acid is a member
of essential amino acid.5. The vitamin is also involved in maintenance of sulfhydral group.
Deficiency
The deficiency of B12 may result from poor dietary intake which occurs in strict vegetarians,Deficiency of B12 causes:1. Pernicious anemia: It is charcterized by low HB level, decreased numbers of RBC and
neurological symptoms in this type of anemia, there is autoimmune destruction of gastricparietal cells that secrete intrinsic factor (IF) in absence of IF, vitamin B12 cannot be absorbed.
2. Mucosal atrophy and inflammation of tongue and mouth glossitis.3. Severe disease of nervous system both central as well as peripheri.4. Common psychiatric symptoms.
BIOTIN (B7)Antiegg white injury factor.Sources:– widely distributed in both animals and plants foods. The rich sources are liver, kidney,egg yolk, milk, tomatoes, grain, etc.
Daily requirements 100-300 mg for adults. Normally synthesized by intestinal bacteria.Physiological functions/Coenzymes activities.1. Conversion of pyruvate to oxaloacetate by biotin dependent co carboxylase
(Gluconeogenesis)2. Acetyl CoA is the starting material for fatty acid synthesis.
BiotinAcetyl CoA ——————————> Malonyl CoA
Acetyl CoA carboxylase
Deficiency Symptoms
1. High consumption of raw egg while confers the deficiency of biotin due to formation ofavidin biotin complex. Avidin is a protein which is present in raw egg white and when thecomplex avidin biotin is formed the absorption of biotin is inhibited which leads to thedeficiency but it is very rare.
2. Anorexia, nausea, glossitis.3. Destruction of intestinal flore Table 9.3.

126 Biochemistry for Dental Students
Table 9.3: Summerized representation of vitamin B complex with functions,deficiency and Daily requirement
Vitamin Coenzyme form Biochemical function Deficiency Daily
requirement
Thiamin [B1] TPP Oxidative decarboxylation Beriberi 1.2-1.8 mg
Riboflavin [B2] FMN FAD Oxidation reduction Lesions on lips 1-2 mgand chiulosis
Niacin [B3] NAD+, NADP+ Hydrogen Transfer Pellagra 12-20 mg
Pantothenic Coenzyme A Formation of CoA & Muscle cramp 5-10 mgacid [B5] derivatives burning feot syndrome
Pyridoxine[B6] Pyridoxal Transamination, Peripheral neuritis 1-2 mgPhosphate Decarboxylation
Biotin [B7] Carboxybiocytin CO2 fixation Anaemia Dermatitis 150-300 mg
Folic acid [B8] FH4 One carbon metabolism Megaloblastic 100-300 μg(Tetrahydrofolate) microcytic anemia
Cynocobalamine Cobamide Transmethylation Pernicious anaemia 1-3 μg[B12] Coenzyme with FH4
Vit C L ascorbate Hydroxylation Scurvy 25-30 mg(Ascorbic acid)
SUMMARY1. Vitamins are essential compound required in the diet. They are classified as fat soluble
(A,D,E,K) and water soluble vitamins (vitamin C and B complex).2. Vitamin A in involved in vision, proper growth. It’s deficiency results in night blindness.3. The active form of vitamin D is calcitriol which function like a steroid hormone. It’s
deficiency leads to Rickets in children and osteomalacia in adults.4. Vitamin E acts as an antioxidant and it is necessary for the normal reproduction.5. Vitamin K converts the clotting factors II, VII, IX and X to their active form.6. Vitamin B complex or the member of B complex family act as coenzymes.7. Thiamine pyrophosphate (TPP) is coenzyme form of thiamin, acts as coenzyme in oxidative
decarboxylation reactions it deficiency causes beriberi.8. The coenzymes of riboflavin are FMN and FAD are involved in oxidation reduction
reactions. Play a role in Electron transport chain.9. NAD and NADP both of these are the coenzyme forms of niacin. The act as hydrogen and
electron transfer agents. It’s deficiency causes pellagra.10. Pyridoxal phosphate is a active derivative of pyridoxine. It functions as co-carboxylase
and acts as a coenzymes in transamination and deamination reactions.

Vitamins (The accessory factors) 127
11. (CoA) is a active form of pentothenic acid is required for the several reactions in metabolismof carbohydrates, lipids and proteins.
12. Folic acid is involved in the transfer of single carbon C-1 moiety. It’s deficiency causesmegaloblastic anemia.
13. Vitamin B12 the cynocobalamine acts as a coenzyme with tetrahydrofolate in synthesis ofmethionine. Pernicious anemia is caused by it’s deficiency.
14. Vitamin C (ascorbic acid) is involved in the hydroxylation reactions. It is also involved inoxidation-reduction reactions in the cells. It’s deficiency causes scurvy.

The mineral elements presents in the human body are supplied by the diet. Minerals performseveral vital functions which are essential for the existence of the organism.
The minerals are classified as principal elements and trace elements.The principal elements constitute 60-80% of the body’s inorganic material. These are calcium,
phosphorus, magnesium, sodium, potassium, chloride and sulfur.The trace elements are subdivided into three categories: Essential, possibly essential and
non-essential.1. Essential trace elements include– Iron, copper, iodine, manganese, zinc, fluorine, selenium,
molybdenum, chromium, cobalt.2. Possibly essential trace elements– Nickel, vanadium, cadmium and barium.3. Non-essential trace elements– Aluminium, lead, mercury, boron, silver, bismuth, etc.
The metabolism of important minerals are discussed here under.
CALCIUMCalcium is the most abundant among the minerals in the body. The total content of Ca2+ in anadult man is about 1 to 1.5 kg.
Physiological Functions
1. Development of bones and teeth—Calcium ion (Ca++) along with phosphate is requiredfor the formation and physical strength of skeletal tissue.
2. Calcium interacts in triggring muscle contraction by increasing the interaction betweenactin and myosin.
3. Ca++ is necessary for the transmission of nerve impulse.4. Ionized calcium is required in blood coagulation process.5. It regulates permeability of membrane for transport of water and several ions across it.6. Essential for maintaining the integrity of intracellular material.
CHAPTER 10
Minerals: The InorganicElements
(Mineral metabolism)

Minerals: The Inorganic Elements (Mineral metabolism) 129
7. It is required for the activation of several enzymes such as dehydrogenase, and certainproteolytic enzymes.
8. It also acts as a messenger for the action of certain hormones, e.g. epinephrine in liverglycogenolysis.
Sources
Richest source is milk and cheese. Other sources include – Egg yolk, nuts, figs, beans, cabbage,cauliflowers, turnip greens, green leafy vegetables sparages.
Daily Requirements
Adults – 800 mg/dayWomen during pregnancy – 1.2 gm and 1.5 gm/dayand lactation respectively.Infants under 1 year – 360 – 540 mg/dayChildren 1-18 years – 0.8 – 1.2 gm/day
Absorption
Calcium ion (Ca++) is taken in diet as calcium phosphate, carbonate and oxalate calcium isactively absorbed in the upper small intestine in duodenum by an energy dependent activeprocess. It is influenced by several factors.
Factors promoting Ca2+ absorption
1. Vitamin D (through its active form calcitriol) induces the synthesis of Ca2+ binding proteinin the intestinal epithelial cells and promotes Ca2+ absorption.
2. Parathyroid hormone (PTH) enhances Ca absorption through the increased synthesis ofcalcitriol acidity (low pH) is more favourable for Ca absorption.
3. Calcium phosphorus ratio of 1:1 (2:1 OR 1:2) is the most convenient for the absorption ofboth.
Distribution of Calcium in Body
Serum – 9-11 mg/100 mlCSF – 4.5-5 mg/100 mlMuscle – 70 mg/100 gmNerve – 15 mg/100 gm

130 Biochemistry for Dental Students
Blood Calcium
• The serum calcium level is 9-11 mg%. Average volume is 10 mg %.• Calcium exists in the plasma in 3 fractions ionized or diffusible calcium, calcium non
diffusible calcium and complex (citrate and phosphate).• About 2 mg of the total calcium occurs in ionized form it is physiological active form of
Ca about 5 mg occurs in nonionized form and about 2 mg in the complex form.• The hormones calcitriol, parathyroid hormone (PTH) and calcitonin are the major factors
that regulate the plasma calcium level.
Calcitriol
The physiologically active form of vitamin D induces the synthesis of a specific calcium bindingprotein in the intestinal cells. This protein increases the intestinal absorption of Ca as well asphosphates. This leads to increase the blood Ca levels. It also stimulated Ca uptake by osteoblastsof bone and promote calcification or mineralization and remottling.
Parathyroid Hormone
The prime function of PTH is to elevate serum Ca2+ level.Action on the bone–It causes decalcification or demineralization of bone, a process carried outby osteoblasts.
Calcitonin
The action of calcitonin on calcium metabolism is antagonist to then parathyroid hormone.
Disorders of Calcium Metabolism
Hypocalcemia
A decrease in serum Ca++ concentration is called as hypocalcemia, hypocalcemia may lead tofaulty calcification of bone, such as seen in rickets (in children) and osteomalacia (in adults). Itmay also affect the motor nerves which become over susceptible to stimule which results inneuromuscular hyperexcitability. The condition is a syndrome called as Tetany.
Hypercalcemia
Hipercalcemia may be due to the increased dietary intake of calcium, raised level of plasmaalbumin or increased renal re-absorption of Ca++ and hyperactively of parathyroid gland. Itmay cause loss of appetite, vomiting, constipation, weaknes, sluggish reflex activity of CNS.

Minerals: The Inorganic Elements (Mineral metabolism) 131
PHOSPHORUSAn adult body contains about 1 kg phosphate and it is formed in every cell of the body. Mostof it (about 80%) occurs in combination with Ca in the bones and teeth.
About 10% of body phosphorus is found in muscles and blood in association with proteins,carbohydrates and lipids. The remaining 10% is widely distributed in various chemicalscomponents.
Biochemical Importance
1. It is essential for the development of bones and teeth.2. It plays a central role for the formation and utilization of high energy phosphate and
utilization of high phosphate components e.g. ATP,GTP, creatine phosphate, etc.3. Phosphorus is required for the formation of phospholipids, phosphoproteins and nucleic
acids (DNA and RNA).4. It is an essential component of several nucleotide coenzymes e.g., NAD+ NADP+, pyridoxal
phosphate, ADP,AMP.5. Several proteins and enzymes are activated by phosphorylation.6. Phosphate buffer system is important for the maintenance of pH in the blood as well as in
the cells.7. Phosphate is necessary for the absorption and metabolism of carbohydrates.
Daily Requirements
Infants – 240- 400 mgChildren – 800-1200 mgAdults – 800 mgWomen during – 1.2 gmpregnancy and lactation.
Sources
Milk, cereals, leafy vegetables, meat eggs, nuts, cheese, etc.
Serum Phosphate Level
The phosphate level of the whole blood is around 40 mg/dl while serum contains about 3-4mg/dl.
Phosphorus occurs in the blood in the following forms.Inorganic phosphorus – 2.5 mg/100 mlOrganic phosphorous – 14–29 mg/100 mlPhospolipids – 8–18 mg/100 ml

132 Biochemistry for Dental Students
Disease State
1. Serum phosphate level is increased in hypoparathyroidism and decreased inhyperparathyroidism.
2. In severe renal diseases, serum phosphate, content is elevated causing acidosis.3. Vitamin D deficient rickets is characterized by decreased serum phosphate (1-2 mg/dl).4. Renal rickets is associated with low serum phosphate levels and increased alkaline phosphate
activity.5. In diabetes mellitus, serum content of organic phosphate is lower while that of inorganic
phosphate is higher.
MAGNESIUMThe adult body contains about 20 gm magnesium 70% of which is found in bones in combinationwith calcium and phosphorus. The remaining 30% occurs in the soft tissues and body fluids.It is the principal cation of the soft tissues.
Biochemical Functions
1. It is required for the formation of bones and teeth.2. Mg2+ serves as cofactor for several enzymes requiring ATP, e.g. Hexokinase, glucokinase,
phosphofructokinase, adenylate cyclase.3. Mg2+ is necessary for proper neuromuscular function. Low Mg2+ level leads to
neuromuscular irritability.
Dietary Requirements
Infants – 100 – 150 mgChildren – 150 – 200 mgAdults – 200 – 300 mgAdult men – 350 mg/dayAdult women – 300 mg/day
Sources
Cereals, nuts, beans, vegetables (cabbage, cauliflower, meat, milk, fruits).
Serum Mg Level
Normal serum concentration of Mg is 2-3 mg/dl. 60% as ionized form 10% as combined formwith ions and 30% as bound form with proteins.

Minerals: The Inorganic Elements (Mineral metabolism) 133
Disease States
1. Magnesium deficiency causes neuromuscular irritation, weakness and convulsions. Thesesymptoms are similar to that observed in tetany (Ca deficiency) which are relieved only byMg). Malnutrition, alcoholism and cirrhosis of liver may lead to Mg deficiency.
2. Low levels of Mg may be observed in uremia, rickets, abnormal pregnancy, growth hormonetreatment, hypercalcemia and the recovery phase of diabetic coma.
SODIUMIt is the major component of the cations of the extracellular fluid and exists in the body inassociation with the anions chloride, bicarbonate, phosphate and lactate.
Biochemical Functions
1. It is largely associated with chloride and bicarbonate in regulation of acid-base-equilibrium.2. It maintains the osmotic pressure of the body fluid and thus, protects the body against
excessive fluid loss.3. Sodium ions plays an important role in the absorption of glucose and galactose as well as
amino acids from the small intestine.4. It maintains the normal water balance and distribution.5. Sodium ion is involved in initiating and maintaining the heart beat.6. It maintains the normal neuromuscular function.7. It plays an important role in maintaining the resting membrane potential (RMP) and the
action potential.8. It functions in the permeability of the cells.
Dietary requirements – 5 to 15 gm/day
Sources
Principal sources – Sodium chloride used in cooking and seasoningRich sources – Bread, cheese, wheat germ, whole grains and oysters, etc.Good sources – Carrots, cauliflowers, eggs, milk, nuts, spinach and turnips, etc.Normal level of – The normal level of sodium is 310-340 mg/100 mlsodium in blood
Disease State
Hyponatremia
This is a condition in which serum sodium level falls below the normal concentration.Hyponatremia may occur due to diarrhea, vomiting, chronic renal diseases, adrenocorticalinsufficiency (Addisons disease). Administration of salt free fluid may cause hyponatremia.

134 Biochemistry for Dental Students
Decreased serum sodium concentration is also observed in edema which occurs in cirrhosisor congestive heart failure. The manifestation of hyponatremia include reduced blood pressureand circulatory failure.
Hypernatremia
This condition is characterized by an elevation in the serum sodium level. It may occur due tohyperactivity of adrenal cortex (cushing’s syndrome), prolonged administration of cortisone,ACTH and or sex hormones. Loss of water from the body causing dehydration as it occurs indiabetes insipictus, results in hypernatremia.
Rapid administration of sodium salts also increased serum sodium concentration. Inpregnancy, steroid and placental hormones cause sodium and water retention in the body,leading to edema.
The symptoms of hypernatremia include increase in blood volume and blood pressure(hypertension).
POTASSIUMPotassium is largely present in the intracellular fluid and it is also present in small amounts inthe extracellular fluid because it influences cardiac muscle activity.
Physiological Functions
1. It maintains intracellular osmotic pressure.2. It is required for the regulation of acid base balance and water balance in the cells.3. Essential for protein biosynthesis by ribosomes.4. Required for transmission of nerve impulse5. The glycolytic enzyme pyrurate kinase requires K+ for maximal activity.
Daily Requirement: 3–4 gm/day
Sources
Banana, orange, pineapple, carrots, cauliflower, potato, beans, chicken, liver, coconut water isa rich source of potassium.
Disease States
1. Potassium deficiency causes neuromuscular irritation, weakness and convulsions.These symptoms are similar to that observed in tatany (Ca deficiency) which are relievedonly by mg.Malnutrition, alcoholism and cirrhosis of liver may lead to K deficiency.

Minerals: The Inorganic Elements (Mineral metabolism) 135
2. Low levels of K may be observed in uremia, rickets, abnormal pregnancy, growth hormonetreatment, hypercalcemia and the recovery phase of diabetic coma.
IRONThe total content of iron in an adult body is 3–5 g. About 70% of this occurs in the erythrocytesof blood as a constituent of hemoglobin. At least 5% of body iron is present in myoglobin ofmuscle. Heme is the most predominant iron containing substance. It is a constituent of severalproteins/enzymes (hemoproteins)- hemoglobin, myoglobin, cytochromes, xanthine oxidase,catalase, tryptophan pyrrolase, peroxidase. Certain other proteins contain non-heme iron, e.g.transferrin, ferritin, hemosiderin.
Biochemical Functions
1. Iron mainly exerts its functions through the compounds in which it is present. Hemoglobinand myoglobin are required for the transport of O2 and CO2.
2. Cytochromes and certain non-heme proteins are necessary for electron transport chain andoxidative phosphorylation.
3. Peroxidase, the lysosomal enzyme, is required for phagocylosis and killing of bacteria byneutrophils.
4. Iron is associated with effective immunocompetence of the body.
Dietary Requirements
Adult man – 10 mg/dayMenstruating woman – 18 mg/dayPregnant and lactating woman – 40 mg/day
Sources
Rich – Organ meats (liver heart, kidney)Good sources – Leafy vegetables, pulses, cereals, fish,
apples, dried fruits, molasses.Poor sources – Milk, wheat, polished rice.
Disease States
1. Iron deficiency anemia: This is the most prevalent nutritional disorder worldover, includingthe well developed countries (e.g. USA) Several factors may contribute to iron deficiencyanemia. These include inadequate intake or defective absorption of iron, chronic bloodloss, repeated pregnancies and hookworm infections.

136 Biochemistry for Dental Students
Iron deficiency anemia mostly occurs in growing children, adolescent girls, pregnant andlactating women. It is characterized by microcytic hypochromic anemia with reduced bloodhemoglobin levels (< 12 g/dl). The other manifestations include apathy (dull and inactive),sluggish metabolic activites, retarded growth and loss of appetite.
2. Hemosiderosis: This is a less common disorder and is due to excessive iron in the body. Itis commonly observed in subjects receiving repeated blood transfusions over the years, e.g.patients of hemolytic anemia, hemophilia. As already stated, iron is a one-way compound,once it enters the body, it cannot escape. Excessive iron is deposited as ferritin andhemosiderin. Hemosiderin deposits in cells can be observed under the microscope withsuitable staining while ferritin cannot be identified.Hemosiderosis is commonly observed among the Bantu tribe in South Africa. This isattributed to a high intake of iron from their staple diet corn and their habit of cookingfoods in iron pots.
3. Hemochromatosis: This is a rare disease in which iron is directly deposited in the tissues(liver, spleen, pancreas and skin). Hemosiderosis is sometimes accompanied byhemochromatosis. Bronzed-pigmentation of the skin, cirrhosis of liver, pancreatic fibrosisare the manifestations of this disorder. Hemochromatosis causes a condition known asbronze diabetes.
COPPERCopper in our body is distributed in different organs.
Physiological Functions
1. It has important role in hemoglobin synthesis.2. It is required for melanin formation, phospholid and collagen synthesis.3. It has role in bone formation and in maintenance in the integrity of myelin sheeth and
formation of bone.
Sources
Liver, kidney, meat, shellgish, nuts and dried legumes.
Other Source
Milk and its products.
Daily Requirements
Adults – 2-3 mg/day infants and children 0.5–2 mg/dayThe normal blood serum copper level is about 100–200 μg/dl.

Minerals: The Inorganic Elements (Mineral metabolism) 137
Disease State
Menke’s disease: This disorder is due to defect in the intestinal absorption of Copper.Symptoms include decreased Copper in plasma and urine, anemia and depigmentation ofhair.
Wilson’s Disease
It is a rare disorder. Intestinal absorption of CU is very high. This leads to hepatic cirrhosis,brain necrosis and renal damage.
IODINEIn our body about 20 mg of Iodine is present most of it is present in the thyroid gland.
Physiological Functions
It is required for the formation of thyroxine (T4) and triiodothyronine hormones (T3) of thethyroid gland.
Sources
Seafoods, drinking water, vegetables, fruits (grown on seaboard), iodine is added in table saltand this iodised salt is easily available source.
Dietary Requirments
Adults—100–150 μg/dayPregnant women—200 μg/dayThe normal concentration of plasma iodine is 4–10 μg/dl.
Disease state
• In adults the thyroid gland is enlarged, producing the disease goiter. If treatment is startedvery early, the thyroid becomes normal.
• If treatment is delayed, the enlargement of the gland persists.• In children severe iodine deficiency results in the extreme retardation of growth which is
known as cretinism.
MANGANESEThe total body content of manganese is about 15 gm. Liver and kidney are rich in Manganesewithin the cells, it is mainly found in the nuclei in association with nucleic acids.

138 Biochemistry for Dental Students
Biochemical Functions
1. Manganese serve as cofactor for several enzymes, e.g. isocitrate dehydrogenase.2. Manganese is required for the formation of bone proper reproduction and normal
functioning of nervous system.3. Manganese is necessary for the synthesis of mucopolysaccharides and glycoproteins.4. Hemoglobin synthesis involves Mn.5. Manganese inhibits lipid peroxidation.6. Manganese is necessary for cholesterol biosynthesis.
Sources
Rich sources – Nuts and whole grains and tea.Other sources – Include vegetables and fruits.
Daily requirements: 2-9 mg/day:
Serum Mn→ Manganese in the serum is bound to a specific carrier protein- transmagnanim(a β globulin). The normal blood contains about 4-20 μg/dl.
Disease State
Mn deficiency in animal causes.1. Retarded growth, bone deformities and in severe deficiency, sterility.2. Accumulation of fat in liver.3. Increased activity of serum alkaline phosphate.4. Diminished activity if β-cells of pancreas (low insulin).
ZINCIn our body zinc is present to about 2 g. Prostrate gland is rich in zinc.
Physiological Functions
1. Zinc is an essential constituent of many enzymes.2. The retina contains Zn metalloenzymes (retinene reductase which is required for the
formation of retinene).3. If maintains normal concentration of vitamin ‘A’ in plasma.4. It is required for the mobilization of vitamin ‘A’ from the liver.5. It is required for preparation of insulin.6. It is concerned with healing of wounds.

Minerals: The Inorganic Elements (Mineral metabolism) 139
7. It is essential for normal growth and reproduction of animals.8. Zinc therapy is essential in some cases of atherosclerosis. The concentration of Zn of human
blood is 0.8 mg/100. Plasma – 0.12 mg/100 ml. erythrocytes – 1.44 mg/100 ml.
Daily Requirement
– Infants 3–5 mg– Children – 70 mg– Adolescents – 13 mg– Adults – 15 mg– Pregnancy – 30 mg– Lactation – 25 mg.
Deficiency Disorders
1. Zinc deficiency in man results in dwarfism and hypogonadism.2. Delayed closure of the epiphyses of the long bone and anemia.3. Deficiency of zinc obstructs the storage and secretion of insulin causing diabetes mellitus.4. Zinc level is decreased in acute myocardial infarction, cirrhosis of liver.5. Liver zinc concentration is highly increased in malignancies.6. Zinc deficiency produces skin lesions.
FLUORINE [MAIN ROLE IN DENTAL CARE]It is mostly found in bones and teeth.
Biochemical Functions
1. In trace amount essential for the development of teeth and bones.2. In combination with vitamin ‘D’ required for the treatment of osteoporosis.3. Role in tooth development and dental health. Fluorine is present in human tooth in trace
amounts and helps in tooth development. Normal maintenance and hardening of dentalenamel.
4. Fluoride prevents the development of dental caries. It forms a protective layer of acidresistant, fluoroapatite with hydroxyapatite, on the enamel and prevents the tooth decayby bacterial acids. Further, fluoride inhibits the bacterial enzymes and reduces the productionof acids.
Dietary Requirements
An intake of less than 2 rpm of fluoride is recommended.

140 Biochemistry for Dental Students
Sources
Drinking water is the main source.
Disease States
1. Dental caries: Water containing less than 0.5 rpm of fluoride is associated with thedevelopment of dental caries in children and adults.
2. Fluorosis: Excessive intake of fluoride is harmful to the body.An intake greater than 2 rpm of fluoride (particularly >5 rpm) in drinking water of in childrenmay reduce to deposition in those tissues and may causes mottling of enamels discoloration(in newly erupted permanent teeth). Corrosion and stratification of enamel includingformation of pits are observed. The teeth are weak and become rough with characteristiccorrosion destroy gradually decay brown or yellow patches on their surface. This conditionis referred to as dental fluorosis.
3. An intake of fluoride above 20 rpm is toxic and causes pathological changes in the bones.Hypercalcification, increasing the density of the bone limbs, pelvis and spine is acharacteristic feature.Even the ligaments of spine and collagen of bones get calcified.
4. Neurological disturbances are also commonly observed these conditions constitute skeletalfluorosis. In the advanced stages, the individuals are crippled and cannot perform theirdaily routine work due to stiff joints.This condition of advanced fluorosis is referred to as genu valgum.Fluoridation of water and use of fluoride tooth have been started in order to prevent the
dental caries in children but excess of this may exert toxic effects.
SELENIUMSelenium in very small amount is biologically important.
Biochemical Functions
1. Selenium along with vitamin D prevents the development of hepatic necrosis and musculardystrophy.
2. It is involved in maintaining structural integrity of biological membranes.
Deficiency in Humans
Keshan Diseases
• This disease affects mainly children and younger women.• It symptoms include cardiac enlargement and ECG changes.

Minerals: The Inorganic Elements (Mineral metabolism) 141
Kashin-Beck Diseases
• The disease is characterized by degenerate osteoarthrosis affecting children between 5 and13 years of age.
• It retards growth by shortening fingers and bones with severe enlargement and dysfunctionof the joints.
SUMMARY1. The mineral or inorganic elements are required for normal growth and maintenance of the
body. They are classified as principle elements and trace elements.2. Calcium is one of the minerals which has the main role in dental care. It is required for the
development of bones and teeth muscle contraction, blood coagulation, nerve transmission,etc.
3. Phosphorus is another mineral essential for the development of bone and teeth. It is also aconstituent of high energy phosphates compounds (ATP, GTP) and the coenzymes like(NAD+, NADP+).
4. Sodium and potassium are involved in regulation of acid base equillibrium.5. Magnesium is also required for development of bones and teeth.6. Iron is mainly required for Oxygen transport and cellular respiration. It is stored as ferritin
in liver, spleen and bone marrow. Iron deficiency causes microcytic, hypochromic anemia.7. Copper has again a role in bone formation and maintenance of myelin sheeth. Wilson’s
disease is due to abnormality in copper metabolism.8. Iodine is important component of thyroid hormones [T3 and T4].9. Zn is required for secretion and storage of Insulin.
10. Flourine in a trace amount is required to prevent dental caries while it’s higher intakeleads to fluorosis. It is the most important mineral to be discussed as mineral having mainrole in dental care.

FOR HUMAN HEALTH AND WELFARESome people eat for living and some people live for eating but one thing is universally agreedand that is food is everyone’s prime concern.
Definition
• Nutrition may be defined as utilization of food by living organisms.• Nutritional study may be classified into three classes:
a. Ideal nutritionb. Under nutritionc. Over nutritionIdeal nutrition is the concern of everyone, under nutrition is the prime concern of developing
countries while over nutrition is a serious concern of developed countries.It is very essential to have a knowledge of chemistry and metabolism of food stuffs including
carbohydrates, lipids proteins, vitamins and minerals for under standing nutrition.
Nutrition and Energy
As all of us know that food is fuel source of body. The food we eat undergoes metabolism toliberate energy which is required for the vital activities of the body.
Energy Content of Foods
The colorific value of food is calculated from the heat released by the total consumption offood in a calorimeter. Calorie is the unit of heat. One calorie represents the amount of heatrequired to raise the temperature of 1 gm of water by 1°C.
Calorific Value of Foodstuffs
ApproximateFood stuffs Enery value (Cal/g) in the bodyCarbohydrates 4Fats 9Proteins 4
CHAPTER 11
Nutrition

Nutrition 143
It must be noted that the nutrients, namely vitamins and minerals, have no calorific valuesalthough they are involved in several important body functions, including generation of energyfrom carbohydrates, fats and proteins.
RESPIRATORY QUOTIENTThe respiratory quotient is the ratio of volume of CO2 produced to the volume of O2 utilized inthe oxidation of foodstuffs.
Carbohydrates
The carbohydrates are completely oxidized and their RQ is close to 1.
Fats
Fats have relatively lower RQ Since they have a low O2 content. For this reason fats requiremore O2 for oxidation.
The R.Q. for fat is approximately 0.7.
Proteins
The chemical nature of proteins is highly variable and this cannot be represented by any specificformula.
Mixed Diet
The RQ of the diet concerned is dependent of the relative composition of carbohydrates, fatsand proteins. For normally ingested diet is just around 0.8.
UTILIZATION OF ENERGY IN MANThere is consumption of energy to meet the fuel demands of three ongoing processes in thebody.
1. Basal metabolic rate.2. Specific dynamic action.3. Physical activity.Besides the above three, additional energy supply is needed during, growth, pregnancy
and lactation.

144 Biochemistry for Dental Students
BMR:-[Basal metabolic rate]
Definition
BMR is defined as the minimum amount of energy required by the body to maintain life atcomplete physical and mental rest in the post-absorptive state ( i.e., 12 hr after the last meal).• Units of BMR: BMR is expressed as calories per square meter of the body surface area per
hr i.e., cal/sq.m/hr.• Normal values of BMR: For adult man 35-38 cal/sq.m/hr• For adult women 32-35 cal/sqm/hr.
Factors Affecting BMR
1. Surface area: The surface area is directly proportional to the BMR, more the surface area,more will be BMR and vise versa.
2. Sex: Men have higher BMR (above 5%) than women.3. Age: In infants and growing children with lean muscle mass, the BMR is higher. In adults
the BMR is decreased at the rate of about 2% per decade of life.4. Physical Activity: BMR is increased in persons with regular exercise.5. Hormones: Thyroid hormones (T3 and T4) have a stimulatory effect on the metabolism of
body and therefore, BMR. Thus, BMR is raised in hyperthyroidism and reduced inhypothyroidism.
6. Environment: In cold climates, the BMR is higher, as compared to warm climates.7. Starvation: During the period of starvation, the energy intake has an inverse relation with
BMR. A decrease upto 50% has been reported. This may be a adaptation by the body.8. Fever: Fever causes an increase in BMR. An elevation by more than 10% in BMR is observed
at every 1ºC rise in body temperature.9. Diseased states: BMR is elevated in various infections but in Addisons disease BMR is
marginally lowered.10. Racial variations: The BMR of Eskimo’s is much higher than the other races.
Significance of BMR
BMR is important to calculate the calorie requirement of an individual and planning of diets.Determination of BMR is useful for the assessment of thyroid function.
SPECIFIC DYNAMIC ACTIONThe phenomenon of extra-heat production by the body, over and above the calculated caloricvalue, when a given food is metabolized by the body, is known as specific dynamic action(SDA). It is also known as calorigenic action or thermic action of food.

Nutrition 145
Specific dynamic action for different foods: For food containing 25 g of protein, the heatproduction from the caloric value is 100 cal, when 25 g of protein is utilized by the body, 130cal of heat is tabulated. The extra 30 cal is SDA of proteins. Similarly, 100 cal of fats results in113 cal and 100 cal of carbohydrates in 105 cal, when metabolized in body.
So, the SDA for protein, fats and carbohydrates is 30%, 13% and 5% respectively.Thus, the SDA for food stuffs containing carbohydrates, protein and lipids. SDA ofprotein > fat > carbohydrates.
Significance of SDA: For utilization of food by the body certain amount of energy is consumedfrom the body stores. This is actually expenditure by the body for utilization of foodstuff forenergy. The SDA for mixed diet is around 10%. It is, therefore, essential to add 10% additionalcalories to the total energy needs of the body towards SDA (SDA is quite comparable to thehandling charged levied by a bank for an outstation cheque).
The higher SDA for proteins indicates that it is not a good source of energy.
Mechanism of SDA: The exact cause of SDA is not known. This is generally believed that SDA offoods is due to energy required for digestion, absorption, transport, metabolism and storage offoods in the body.
As we know that the SDA for protein is highest so, it is a common experience thatconsumption of protein rich diet makes us feel warm and comfortable in cold weather.
Physical Activity: The amount of energy required by an individual depends upon the physicalactivity which depends upon the duration and intensity of muscular activity.
Energy Requirement: As all of us know that the three factors, basal metabolic rate, specific dynamicaction and physical activity determine the energy needed by the body.
For the sake of convenience the individuals are grouped into three categories with regardto their physical activity and energy requirement shown in Table 11.1.
Table 11.1: Energy requirement of different types of physical activites
Physical activity Energy requirement (cal/day)
Light Work – 2200-2500(Teachers, office workers, doctors)Moderate work – 2500-2900(Housewives, students) Heavy Work – 2900-3500(Agricultural labours, Miners)Very Heavy Work – 3500-4000(Construction workers, Rickshaw pullers).
The Nutritional importance of carbohydrates lipids, protein, vitamin and minerals havebeen discussed in the previous pages so the reader can refer the related chapters.

146 Biochemistry for Dental Students
Nutritional Importance of Fibres
The complex carbohydrates, which are not digested by human enzymes are collectively referredto us dietary fibre. These include cellulose, hemi-cellular, pectin, lignin, gums and mucilage.
For a long time fibre was regarded as nutritional wastage but now nutritionist pay a lot ofattention towards the role of fibres in human health.
Beneficial Effects of Fibres
1. Prevention of constipation: Fibre helps to maintain the normal motility of GIT thus preventsconstipation.
2. Elimination of bacterial toxin: Fibres absorb about large quantity of water and also the toxiccompounds produced by intestinal bacteria that leads to increase the fecal mass and itseasier expulsion.
3. Importance of glucose tolerance: Fibres improve glucose tolerance by the body bydiminishing rate of glucose absorption from the intestine.
4. Reduction of Plasma cholesterol level: Fibres decrease the absorption of dietary cholesterolfrom the intestine apart from this fibres also bind with bile salts and reduce theirenterohepatic circulation.
5. Satiety values: Dietary fibres significantly add to the weight of food stuff ingested and givea sensation of stomachfullness. Therefore, satiety is achieved with out consumption of excesscalories.
Sources of dietary fibres: Fruits, leafy vegetables, whole wheat legumes, rice bran, etc.
Recommended Dietary Allowances (RDA)
RDA is the representation of qualities and quantities of the nutrients to be provided in the dietdaily for maintaining good health and physical efficiency of the body.
Recommended dietary allowance of important nutrients for an adult man having bodyweight 70 kg is given in Table 11.2.
Table 11.2: Dietary requirement of a normal adult person
Nutrients RDA
Carbohydrates 400 gFats 70 gProteins 5.6 gEssential fatty acids 4 gVit A 1000 μgVit D 5 μg
Contd...

Nutrition 147
Vit E 10 μg
Vit K 70 μgAscorbic acid 60 mgThiamin 1.5 mgRiboflavin 2 mgNiacin 20 mgPyridoxine 2 mgFolic acid 150 μgCobalamine 2 μgCalcium 800 mgPhosphorus 800 mgIron 10 mg
Balanced Diet
After discussing nutritional importance of protein carbohydrates and lipids, fibres, vitaminsand minerals, now we have to formulate a diet for a man.
Definition
A balanced diet is defined as a diet which contains different types of foods possessing thenutrients—carbohydrates, fats, proteins, vitamins and minerals—in a proportion to meet therequirements of the body. A balanced diet invariably supplies a little more of each nutrientsthan the minimum requirement to withstand a short duration of starvation and keep the bodyin a state of good health.
The basic composition of balanced diet is highly variable, it various with cultural and socialhabits it differs from country to country, availability of foods, economic status, age, sex, physicalactivity of the individual.
The Indian balanced diet is composed of cereals, pulses, vegetables, roots, tubers, fruits,milk and milk products, fats oils, sugar and groundnuts. Meat, fish and eggs are present innon-vegetarians diets. In case of vegetarians, an additional intake of milk and pulses isrecommended. The balanced diet for Indian man and woman are given in Tables 11.3A and11.3B respectively.
Contd...
Nutrients RDA

148 Biochemistry for Dental Students
Table 11.3A: Balanced diet for an adult man
Sedentary work Moderate work Heavy work
Vegetarian Non- Vegetarian Non- Vegetarian Non-
vegetarian vegetarian vegetarian
(g) (g) (g) (g) (g) (g)
Creals 400 400 475 475 650 650Pulses 70 55 80 65 80 65Green leafy vegetables 100 100 125 125 125 125Other vegetables 75 75 75 75 100 100Roots and tubers 75 75 100 100 100 100Fruits 30 30 30 30 30 30Milk 200 100 200 100 200 100Fats and oil 35 40 40 40 50 50Meat and fish – 30 – 30 – 30Eggs – 30 – 30 – 30Sugar and jaggery 30 30 40 40 55 55Groundnuts – – – – 50 50
Table 11.3B: Balanced diet for an adult woman
Sedentary Work Moderate work Heavy work Additional allowance
during pregnancy
Vegetarian Non- Vegetarian Non- Vegetarian Non- Vegetarian Non-Vegetarian Vegetarian Vegetarian Vegetarian
Cereals 100 300 350 350 475 475 50 100Pulses 60 45 70 55 70 55 10Green 125 125 125 125 125 125 25 25vegetablesOther 75 75 75 75 100 100 – –vegetablesRoots and 50 50 75 75 100 100 – –tubersFruits 30 30 30 30 30 30Milk 200 100 200 100 200 100 125 125Fats and oil 30 35 35 40 40 45 15Sugar and 30 30 30 30 40 40 10 20jaggeryMeat and fish – 30 – 30 – 30 – –Eggs – 30 – 30 – 30 – –Groundnuts – – – – 40 40 – –

Nutrition 149
Nutritional Disorders
There is a effect of under nutrition and over nutrition on individuals. Some of the importantnutritional diseases are discussed here under.
Protein Energy Malnutrition: It is also called as protein calorie malnutrition. It is the most commonnutritional disorder of developing countries. Protein energy malnutrition is widely observedin infants and preschool children. Kwashiorkar and Marasmus are the two extreme forms ofPEM.
Kwashiorkar: Kwashiorkar literally means sickness of child specially disposed child that is adisease the child gets when next baby is born.
Occurrence: 1 to 5 years of age due to insufficient intake of proteins as the diet of weaning childmainly consists of carbohydrates.
Clinical Symptoms: Stunted growth, edema, diarrhea, anemia, moonface. Decreasedconcentration of Plasma albumin.
Marasmus: Marasmus literally means “to waste.” It mainly occurs in children under one yearage. Marasmus is predominantly in the children given watery gruels to supplement mothersbreast milk.
Growth retardation, emaciation, weakness, anemia.No edema, the concentration of albumin is not decreased in plasma.
SUMMARY1. Nutrition deals with the utilization of food by living organism.2. The calorific value of food stuffs including carbohydrates, fats and protein is approximately
4, 9 and 4 respectively.3. The utilization of energy occurs for the three ongoing processes in th body including BMR,
SDA and physical activity.4. The BMR is the minimum amount of energy required by the body in the complete physical
mental rest and in post absorptive state.5. The SDA is then extra-heat production in body over and above the calculated calorific value
of that food stuff. It is highest for proteins.6. Recommended dietary allowance represents the quantities of nutrients to be provided daily
in the diet for maintaining good health and physical efficiency.7. A balanced diet is the diet which contains different type of foods namely carbohydrates
fats, protein, vitamin, minerals in proportion into meet body requirements.8. Protein energy malnutrition is the most common nutritional disorder in the developing
countries. Kwashiorkar and Marasmus are two extreme fronts of PEM.

PART–IIPRACTICAL


Molisch’s Test [Group Test for Carbohydrates]
Principle: Alcoholic alpha naphthol forms furfural derivatives, such as hydroxymethyl furfural,by the concentrated sulphuric acid acting on the sugar. This compound forms a reddish-violetcolored ring at the junction of the two liquids.
Molisch’s Reagent: A 5% solution of alpha naphthol in alcohol.
Procedure: Add 2 drops of Molisch’s reagent to 2 ml of sugar solution in a test tube. Mixthoroughly. Add 2 ml of conc. H2SO4 by the side of the test tube slanting the tube. Then erectthe test tube slowly. The formation of reddish-violet ring at the junction of the two liquidsindicates the presence of carbohydrate.
Discussion: Concentrated solution of organic compounds may give a red instead of a violetcolour due to charring action of the sulphuric acid. In case of doubt, the experiment should berepeated on a more diluted solution of the substance to be tested.
Iodine Test [Test for Polysaccharides]
Principle: The composition of the blue- or-red wine red-colored substance is not well defined.This may be an adsorption complex of starch or dextrin or glycogen with iodine rather than adefinite compound.
Iodine Reagent: The 0.5 ml. of iodine diluted to 5 ml with distilled water.
Procedure: Add 1-2 drops of dilute iodine solution to 2-3 ml of dilute starch or dextrin orglycogen, respectively, in case of starch, the blue colour disappears on heating and reappearson cooling. But the red colour and the brown colour in cases of dextrin and glycogen,respectively, do not reappear on cooling as in the case of starch.
Reduction tests: Carbohydrates with free aldehyde or ketone groups have the ability to reducesolutions of various metallic ions. These properties are mentioned below.
CHAPTER 12
Carbohydrates

154 Biochemistry for Dental Students
Fehling’s Test
Principle: Carbohydrates with free aldehyde or ketone groups reduce copper sulphate tocuprous oxide forming a yellow or brownish—red coloured precipitate.
Fehling’s reagent: Prepare freshly by mixing equal volumes of two stock solutions A and B.
Solution A: The 6.93 gm of CuSO4. 5H2O per 100 ml of water.
Solution B: The 20 gm of KOH and 34.6 gm of sodium potassium tartar ate (Rochelle salt) per100 ml solution.Procedure: Add a few drops of sugar solution at a time to 5 ml of Fehling’s solution and heatthe mixture after each addition. The production of yellow or brownish—red cuprous oxideprecipitate indicates the presence of reducing sugars.
Benedict’s Test
Principle: Carbohydrates with free aldehyde or ketone groups reduce copper sulphate ofbenedict’s solution to cuprous oxide on boiling forming a red, yellow or green colouredprecipitate depending on the concentration of the sugar.
Benedict’s qualitative solution: Dissolve with heat 173 gm. of sodium citrate and 100 gms. ofanhydrous sodium carbonate in 600 ml of water in a beaker. Into this with constant stirring,run slowly a solution of copper sulphate (CuSO4 5H2O) containing 17.3 gm dissolved in about100 ml. of water. Cool and transfer to a litre flask and make to the mark with water.
Procedure: Add 8 drops of sugar solution to 5 ml of the Benedict’s qualitative reagent in a testtube. Boil vigorously for 2 minutes or place in a water bath for 3 minutes. Allow to coolspontaneously (do not cool it by immersion in cold water). A red, yellow or green precipitatedevelops depending on the concentration of sugar present.
Colour Approximate amount of reducing sugar
No change of blue colour Absence of reducing sugarBlue changes to green ppt. 0.1-0.5 gm% of reducing sugarBlue changes to yellow ppt. 0.5-1 gm% of reducing sugarBlue change orange-red ppt. 1-2.0 gm% of reducing sugarBlue changes to brick-red ppt. Over 2.0 gm% of reducing sugar
Barfoed’s Test
Principle: The monosaccharides with free aldehyde or ketone groups can cause the reductionof copper sulphate to cuprous oxide with the development of a red precipitate.

Carbohydrates 155
Barfoed’s Solution: Dissolve 66.5 gm of neutral crystalline copper acetate in 1000 ml of distilledwater, add 9.0 ml of glacial acetic acid.
Procedure: Add 8 drops of sugar solution to 5 ml of Barfoed’s solution. Heat to boiling for 30seconds. A red precipitate appears indicating the presence of monosaccharides.
Discussion: This test is a reduction test for mososacchardies and the reduction is broughtabout in an acid solution. If the solution with the sugar is boiled for a few minutes, thedisaccharides also are hydrolysed giving a positive. This test is specific for monosaccharides.
Selivanoff’s Test
Principle: Fructose is acted on by hydrochloric acid to from a derivative of furfuraldehydewhich gives a red coloured compound when linked with resorcinol.
Seliwanoff’s Reagent: Dissolve 50 mg of resorcinol in 33 ml of concentrated hydrochloric acidand dilute to 100 ml with water.
Procedure: Add a few drops of sugar solution (0.5ml) to 5 ml of Seliwanoff’s reagent in a testtube. Heat to boiling for 30 seconds. Formation of red colour indicates the presence of fructose.The test may be positive for sucrose also if it is hydrolyzed during the course of the test.
Discussion: A similar colour may also develop in case of glucose or maltose if the boiling isprolonged due to the transformation of glucose into fructose by the catalytic action of thehydrochloric acid.
Osazone Test
Principle: A solution of reducing sugar when heated with phenylhydrazine, characteristicyellow crystalline compounds called osazone are fromed. Simple sugars like glucose, fructoseand mannose produce the same osazone because of the similarities in their molecular structures.
Table 12.1: Characteristic features of osazone crystals
Osazones Times of formation of crystals Appearence of crystals
Glucosazones 5 minutes Broomstick likeFructosazone 2 minutes Broomstick likeMaltosazone 10-15 minutes Sunflower likeGalactosazone 7 minutes Rhombic likeLactosazones 10-12 minutes Powder puff like
Procedure: Add 10 drops of glacial acetic acid to 5 ml of sugar solution in test tube. Then adda knife point of phenylhydrazine hydrochloride and double the amount of sodium acetatecrystals. Mix and warm a little to see that the solids are dissolved. Filter the solution in another

156 Biochemistry for Dental Students
Fig. 12.1: Osazones for glucose/fructos, lactose, maltose, galactose respectively
test tube and keep the filtrate in a boiling water bath for 20 minutes. Allow the tube to coolslowly in the water bath without cooing it hurriedly under the tap to have better crystals andexamine the crystals under the microscope.
Discussion: Formation of osazone crystals of different sugars depends on the time schemedbelow (Table 12.1 and Fig. 12.1).
Sucrose does not produce osazone crystals when the solution is kept in the boiling waterbath for 30 minutes because of the hydrolysis of sucrose to glucose and fructose.

EMULSIFICATIONPrinciple: Oil or liquid fat becomes finely divided and is dispersed in water when shaken withwater to form emulsification. Emulsification is permanent and complete in the presence ofemulsifying agents. The important emulsifying agents are bile salts, proteins, soaps, mono-and diglycerides. Emulsification is important in the processes of fat digestion in the intestine.Emulsifying agents lower surface tension of the liquid.
Procedure: Take 2 clean and dry test tubes. In one, add 2 ml water and in the other 2 ml dilutebile salt solution. Now to each add 2 drops of mustard oil and shake vigorously for about oneminute. Allow the tubes to stand for 2 minutes and floats on the surface, whereas, in bile saltsolution, the oil can be seen in minute droplets suspended in the liquid (e.g., permanentemulsification).
SAPONIFICATIONPrinciple: Oil or liquid fat when boiled with an alkali is hydrolyzed and the liberated fattyacids form salt with alkali (soap). This process said to be saponification. Saponification numberis the number of milligrams of KOH required to saponify one gram of fat.
Procedure: Take 4 ml. 2% sodium carbonate solution in a test tube and add 2 drops of mustardoil. Shake vigorously and boil. A clean soapy solution is formed. Cool and divide it into threeparts for further study on the properties of soap.
I. In one test tube, add a few drops of conc. HCl and observe that the fatty acid separates outand floats up. This is due to the hydrolysis of soap by the acid.
II. In another test tube, dissolve sufficient amount of finely powdered NaCl. White precipitatesof soap separate out and float on the surface. This process is called ‘salting out’ of soap.
III. In the third test tube, add a few drop CaCl2 solution. A precipitate of insoluble calciumsoap is obtained.
GREASE-SPOT TESTProcedure: Put a drop of oil over a piece of ordinary writing paper (not filter paper). Thetranslucent spot indicates the presence of fat.
CHAPTER 13
Lipids

158 Biochemistry for Dental Students
UNSATURATION TESTPrinciples: All neutral fats contain glycerides of some unsaturated fatty acids. These unsaturatedfatty acids become saturated by taking up iodine. If the fat contains more unsaturated fattyacids, it will take up more iodine.
Procedure: Add 10 drops of Huble’s iodine reagent (Alcoholic solution of iodine containingsome mercuric chloride) to 10 ml. chloroform. The chloroform shows pink colour due to thepresence of free iodine. Divide this solution equally into 4 test tubes.
I. To one test tube, add mustard oil drop by drop shaking the tube vigorously for about 30seconds after addition of each drop until the pink colour is discharged and count the numberof drops. The pink colour is discharged owing to the taking up of iodine by the unsaturatedfatty acids of the oil.
II. Repeat the above experiment with the remaining three test tubes taking fats (coconut oil,dalda and groundnut oil). Now compare their unsaturation. It should be remembered thatmore the number of drops required to discharge the pink colour, the less is the unsaturation.lodine value: It is the number of grams of iodine taken up by 100 grams of fat.
CHOLESTEROL1. Salkowski’s Test
Procedure: Dissolve a little cholesterol in 2 ml. choloroform in a dry test tube. Add an equalvolume of conc. H2SO4, Shake gently. The upper layer of chloroform turns red and the sulphuricacid layer shows a yellow colour with a green fluorescence.
2. Formaldehyde–H2SO4 Test
Procedure: Add 2 ml of formaldehyde-H2SO4 solution (1 Part of 40% formaldehyde to 50 partsof the acid) to 2 ml of choloroform solution in a dry test tube. The cherry colour is developed inthe chloroform. Pour off the chloroform into another test tube and add 2 to 3 drops of aceticanhydride. The blue colour is developed.
This test is said to be more delicate than Salkowski’s test.

CHAPTER 14
Proteins
Proteins
Proteins are identified by three group tests.
COLOUR REACTIONS OF PROTEINSProteins respond to some colour reactions due to the presence of one or more radicals or groupof the complex proteins molecule. All proteins do not contain the same amino acids and hencethey do not respond to all colour reactions giving positive findings. The material underexamination should, therefore, be subjected to several tests before concluding its nature.
1. Biuret Test
Principle: This test positive for all compounds containing more than one peptide linkage(-CO-NH-) e.g. Proteins and their hydrolytic products (metaproteins, proteoses, peptones,polypeptides except dipeptides and amino acids). This test is alsopositive for substances whichcontain two carbamyl (-CONH2) groups joined directly or through a single atom of nitrogen orcarbon and similar substances which contain –CSNH2, C(NH)NH2 or – CH2NH2 group alsorespond to this biuret test. Hence, nonproteins, e.g. oxamide.

160 Biochemistry for Dental Students
Procedure: To 2 ml. of protein solution add 1 ml of 40% NaOH solution and 1 or 2 drops of 1%CuSO4 solution. A violet colour indicates the presence of peptide linkage of the molecule.
Note: Care must be taken that not more than 2 drops of dilute copper sulphate (1%) beadded,otherwise blue colour will develop instead of violet colour.
2. Ninhydrin Test (The Triketohydrintene hydrate test)
Principle: This test is positive for all aminoacids containing free amino and carboxylic groups.Hence, it is positive for proteins, peptones and peptides. It is also positive with other primaryamines including ammonia. The triketohydrintene hydrate forms a complex with the amino orcarboxylic group of the amino acids or other primary amino developing a blue colour on heating.
Procedure: To 1 ml of protein solution add 2 drops of freshly prepared 0.2% ninhydrin solutionheat. A blue colour develops indicating the presence of proteins, peptides or amino acids.
3. Millon’s Test (Test for Tyrosine)
Principle: The neutral protein solution reacts with acidified mercuric chloride to from a yellowprecipitate of mercury-protein complex. This complex forms a nitrite complex with sodiumand nitrite solution on warming, developing a red colour. This test is given by phenols orphenolic substances such as salicylic acid.
Procdure: Add 1 ml of protein solution acidified with H2SO4 to 1 ml of acid mercuric sulphatesolution (10% HgSO4 in 10% H2SO4). Boil gently for about one minute. A yellow precipitateforms. Cool under the tap and add a drop of 1% of NaNO2 (Sodium nitrite) solution. On gentlewarming it turns red. This indicates the presence of hydroxyl group. Tyrosine is the only aminoacids which respond positively to this test. Millons reagent is available in market add 1 mlprotein solution to 2 ml Millon’s reagent on gentle warming it turns red and now tyrosine isconfirmed.
Note: Excess of chloride interferes by forming unionized HgCl2. If so, more HgSO4 must beadded.
4. Xanthoproteic Reaction (For Tyrosine, Phenylalanine and Tryptophan)
Principle: Proteoses and Peptones do not form precipitate with HNO3 but their solutions becomeyellow and then orange when made alkaline.
The white precipitate of protein after the addition of HNO3 is due to the formation ofmetaproteins insoluble in HNO3. The nitro-compounds from the proteins molecule containingbezene ring develop a yellow colour. These nitro-compounds in alkaline medium ionize freelyand produce deep yellow or orange colour.

Proteins 161
Procedure: To 2 ml of protein solution, add carefully 1ml of conc. HNO3 A white precipitateforms. Boil and the colour change to yellow cool the test tube and add 20% of NaOH, thecolour changes to orange indicting the presence of aromatic amino acids.
Note: Phenylalanine does not respond to this test as it is ordinarily performed. This test is notsatisfactory one for use in urinary examination because of the colour of the end reaction.
COAGULATION REACTIONPrinciple: Coagulation of protein is caused by the denaturation of protein structure by heat oracids.
1. Heat Coagulation
Procedure: Take protein solution of about two thirds of the test tube and heat the upper portionof the solution. An opalescent appears which becomes deep on the addition of a few drops of2% acetic acid. This indicates the presence of albumin.
2. Coagulation with Conc HNO3
Procedure: Take 2 ml of conc HNO3 In a test tube and add the protein solution by the side ofthe test tube. A white ring appears at the junction of the two liquids. This test is called asHeller’s nitric acid test.
3. Precipitation Reaction
Principle:i. Proteins are precipitated by salts of the heavy metals (e.g. HgCl2, AgNO3, CuSO4, etc.).
ii. These may be precipitated by certain acids some of which are called alkaloidal reagents(Picric acid, phospho tungstic acid, tannic acid and meta-phosphoric acid, etc.).
iii. These may also be precipitated by concentrated solutions of ammonium sulphate, sodiumsulphate and sodium chloride. These salts precipitate proteins by ‘salting out’ methods.
iv. The proteins are precipitated by dehydrating agents such as alcohols and acetone. Theseagents convert them into suspensoids which upon the addition of a few drops of saltsolution. Alcohol also causes denaturation of proteins. Alcohols bring protein solutioninto isoelectric point at which it is precipitated.
1. Precipitation by Salts of Heavy Metals
A. Procedure: To 2ml of dilute protein solution (solution of egg white) add a few drops ofdilute solution (1%) of zinc sulphate drop by drop. A white precipitate is formed indicating thepresence of protein.

162 Biochemistry for Dental Students
B. Procedure: To 2 ml of dilute protein solution (solution egg white) add a few drops of 0.5%ferric chloride solution drop by drop. An opalescent appears which disappears on addition ofexcess of ferric chloride solution.
2. Precipitation by Alkalodial Regent
A. Procedure: Add 1 ml. of Esbach’s reagent (solution of picric acid and citric acid) to 1 ml ofprotein solution. A yellow precipitate is formed indicating the presence of protein.
B. Procedure: To 2 ml of protein solution add a drop or two of 2% solution of sulphosalicylicacid (a solution of salicylic acid in sulphuric acid). The formation of white precipitate indicatesthe presence of protein.
3. Precipitation by Neutral Salts
A. Full Saturation
Procedure: Take 5 ml of protein solution in a test tube and add solid ammonium sulphate untilit becomes saturated. A gelatinous precipitate forms which indicates the presence of albumin.
B. Half Saturation
Procedure: Prepare a saturated solution of ammonium sulphate in a test tube. Add 3 ml ofsaturated solution to 3 ml of protein solution. Shake vigorously. A gelatinous precipitate formedindicates the presence of globulin.
4. Precipitation by Alcohol
A. Procedure: To 1 ml. of protein solution (concentrated egg white solution) add 2 to 3 ml ofalcohol. A white opalescent forms indication the presence of protein. Filter after10 minutes. Try to dissolve the residue by water. The ppt. does not dissolve.
B. Procedure: Take 1 ml of protein solution in a test tube and 2 to 3 ml. of alcohol in another testtube. Keep both the tubes in the freezing mixture for 10 minutes and them mix the contentsof the two tubes. A white opalescent appears. Filter at once. Try to dissolve the residue onthe filter paper and observe that the precipitate redissolves.

CHAPTER 15
Urine
PHYSICAL CHARACTERISTICSFrequency of Urination
i. It is generally dependent upon the amount of urine in bladder.ii. The frequency is increased in the inflammation of the urinary tract, in the infections of the
spinal cord and in weakening of the sphincter.
Preservation of the Urine Sample
i. Toluene is a very satisfactory preservative for urine.ii. Formaldehyde (2 drops per 50 ml of urine) or a bit of camphor or thymol are also satisfactory
preservative.
Volume
i. Normally, the volume of urine excreted by an adult individual ranges from 1200 to1800 m per day.
ii. Polyuria causes the increased output of urine but oligouria causes diminished excretion.iii. Certain pathological conditions such as diabetes mellitus diabetes, insipidus, cause increase,
volume of urine.iv. A decreased volume is also observed in acute nephritis, diarrhea, vomiting and diseases of
the heart and lungs.
Colour
i. Normal human urine is yellow in colour. This colour is due to pigment urochrome whichis compound of urolilien and uobilinogen.
ii. The urine may be deeper yellow when it gets concentrated as in case of low out put ofurine.
iii. In chyluria, the urine appears milky and in alkaptonuria, the urine becomes dark onstanding.

164 Biochemistry for Dental Students
Specific Gravity
i. The specific gravity of urine of normal individuals varies between 1.006 and 1.025.ii. Following copious water or beer drinking the specific gravity may go down to 1.002 but in
case of excessive perspiration, it may go upto 1.040.iii. The specific gravity depends on the amount of solutes present in urine. When large amounts
of glucose or albunin is passed in urine, the specific gravity rises.iv. The determination of specific gravity is done by Urinometer. This instrument is calibrated
at a specific temperature.
Appearance
i. Normal urine is perfectly clear and transparent when freshly voided. On standing for avariable time, the appearance becomes turbid due to the formation of the crystals ofphosphates or urates or oxalates and also for the formation of nucleoproteins or mucoidand epithelial cells.
ii. The phosphates are deposited in alkaline urine (or sometimes in slightly acid urine). Calciumoxalate is deposited in all urines. Uric acid and urates are deposited when the urine coolsand redissolved on warming. Phosphates dissolve in dilute acetic acid.
iii. The turbidity also appears in the presence of WBC, RBC or bacteria. A coloured deposit isalso observed in the presence of RBC.
Odour
i. Fresh normal urine has an aromatic odour.ii. On standing for a long time, it undergoes bacterial decomposition producing a very
unpleasant ammoniacal odour.iii. Under normal conditions, the urine possesses a peculiar odour due to the ingestion of
certain drugs or vegetables.
CHEMINAL CHARACTERISTICSA. Reaction
i. Freshly voided normal human urine has PH6 (acidic to litmus).ii. On standing for a long time, it may be alkaline due to the formation of ammonia from
bacterial decomposition.iii. Ingestion of acid fruits (orange lemons, etc. ) causes the formation of alkaline urine because
the ash of such fruits is alkaline. Bread, cereals meat, etc. produce an acid urine.B. Urine contains normal or abnormal constituents which are detected by chemical tests. Thenormal constituents can be divided into nitrogenous and non-nitrogenous constituents of urineare excited in abnormal amounts.

Urine 165
THE CHIEF NITROGENOUS CONSTITUENTS OF NORMAL URINE
I. Biuret Test
Principle: Urea when heated decomposes with the liberation of ammonia and the formation ofbiuret is dissolved in water and develops a violet colour forming a complex with the alkalinecopper sulphate solution.
Procedure: Place a small amount of urea crystals in a dry test tube and heat it in a low flame.Urea melts with the liberation of ammonia. On further heating it solidifies (In case of urine, theurine is heated to solidify). Cool the tube. Add 3 ml. Of water and shake.
Add to it 1 ml of dil NaOH and 1 or 2 drops of 1% CuSO4 solution. The pink colour developsindicating the presence of urea.
Precaution: More drops of CuSO4 should not be added, otherwise CuSO4 will form Cu (OH)2
with NaOH forming a blue colour. This is sometimes mistaken for a positive biuret test.
II. Benedict’s Test for Uric Acid and Urates
Principle: Uric acid is solube in alkali. The blue colour is developed due to the reduction ofphosphotungstic acid by uric acid.
Procedure: To 2 ml of urine add a few drops of Benedict’s uric acid reagent and a pinch ofanhydrous solium carbonate. Mix A deep blue colour indicates the presence of uric acid.
Discussion: Uric acid is formed from adenine and guanine of nucleic acids. Ordinarily itoccurs in urine as urates. Alkalis dissolve uric acid in the from of urates. It is insoluble inwater. In gout, the kidney loses the power of eliminating uric acid properly and it is collectedin blood in high concentration. This is accompanied by the deposition of uric acid in the joint.Uric acid is highly excreted in urine in leukemia.
III. Jaffe’s Test for Creatine
Principle : Creatinine, the anhydrids of creatine forms creatinine picrate in alkaline mediumdeveloping a deep reddish orange colour.
Procedure: To 4 ml saturated solution of picric acid add 2 ml of 10% NaOH. Divide it equallyinto two test tubes. Add 3 ml of urine to one test tube and 3 ml of water to the other.
The test tube containing urine produces a deep reddish orange colour due to the formationof creatnine picrate. But this does not happen in other test tube containing water.
Discussion: Creatine occurs in small amounts in the urine of normal adults. It is found inlarger amounts in the urine of children and pregnant women, till it is taken to be the normalconstituent.

166 Biochemistry for Dental Students
It is increased in fasting and after high water ingestion. Increased amount are found inmalnutrition, disintegration of muscular tissue and in carcinoma of the liver.
A decrease of cretinine excretion is found in anemia, paralysis leukemia, etc. Under normalconditions about 1 to 1.8 grams of creatnine are excreted by an adult male per day.
The Chief Non-nitrogenous Constituents of Normal urine
1. Chlorides
Principle: A white precipitate of AgCl is formed when acidified reacts with AgNO3 solution.
Procedure: Acidify 2 ml of urine with two drops of conc. HNO3 and add to it 2 ml of AgNO3.A white precipitate of silver chloride indicates the presence of chlorides.
2. Sulphates
Principle: Urine being acidified with HCl forms a white precipitate of barium sulphate by thereaction with barium chloride solution.
Procedure: Add a few drops of Conc. HCl and 1 ml. of barium chloride solution to about 3ml.of urine. A white precipitate of barium sulphate indicate the presence of sulphates.
Note: The presence of HCl prevents precipitate of phosphates.
3. Phosphates
Principle: Phosphates of calcium and magnesium are precipitated by ammonium hydroxideon boiling and these phosphates are dissolved in hot dilute acetic acid. This forms yellowprecipitate of ammonium phosphomolybdate reacing with ammonium molybdate.
Procedure: Add a little ammonium hydroxide to a test tube containing urine three-fourth ofthe test tube and then boil. A white flaky precipitate of phosphates of calcium and magnesiumis formed.
Filter this precipitate and wash the residue on the filter paper with water. Dissolve theresidue in about 3 ml. of hot dilute acetic acid by pouring the acid on the filter paper. Collectthe solution in a clean test tube and divide it into two parts. Retain one part for detectingcalcium.
To the other part add a drop of conc. HNO3 and a few drops of ammonium molybdatesolution. Boil. a lemon yellow precipitate indicates the presence of phosphates.

Urine 167
Abnormal Constituents of Urine
Substances which are not present in easily detectable amounts in urine of normal healthyindividuals but are present in urine under certain diseased conditions are said to be “Abnormal”or “Pathological” constituents of urine.
Before detecting the abnormal constituents of urine, note the physical characteristics (colour,volumes, odour, appearance, specific gravity and sediment) and chemical reaction with litmuspaper.
The abnormal constituents for routine purpose are reducing sugars, acetone bodies, proteins,blood pigments, bile salt, bile and pus.
1. Reducing Sugars
To detect reducing sugars in urine Benedict’s test and Fehling’s test are done. To be sure of thepresence of glucose, lactose, pentose, fructose and glucose, etc. osazone test is to be performed.
Benedict’s test is preferred than Fehling’s test on the fact that the strong alkalinity of Fehling’ssolution destroys traces of sugar; whereas Benedict’s solution with its weak alkalinity respondsto a little amount of sugar present in urine. Hence, it is more sensitive then Fehling’s test.
Presence of streptomycin and certain preservatives such as chloroform and formaldehydegive Benedict’s test positive.
Benedict’s Test
Principle: Copper sulphate of Benedict’s qualitative solution is reduced by reducing substanceson boiling to form the coloured precipitate of cuprous oxide depend on the concentration ofreducing substances present in urine.
Benedict’s Qualitative Reagent
Copper sulphate + sodium carbonate + sodium citrateProcedure: To about 5 ml Benedict’s qualitative reagent add 0.5 ml (8 drops) of urine and boilfor 2 minutes holding the test tube firmly with a test tube holder. A light green, green, yellowand brick red precipitate indicates the presence of reducing substances in urine.
The various coloured precipitate depends on the concentration of reducing sugars in urinewhich gives a rough estimate of the concentration given below.
Light green precipitate 0.1 to 0.5 of reducing sugars.Green precipitate 0.5 to 1.0% of reducing sugars.Yellow precipitate 1 to 2 % of reducing sugars.Brick red precipitate above 2 % of reducing sugars.
Note: The variation in coloured precipitate relating to the concentration of reducing sugar isfound in urine only; whereas this variation does not occur in pure sugar solution in water. Thisdifference may possibly be due to the presence of creatinine and other constituents of urine.

168 Biochemistry for Dental Students
Precautioni. Boil the urine for at least 2 minutes.
ii. During boiling, the contents of the test tube get a tendency to spurt out. Hence, it is wise tokeep the test tube shaking after holding it in the inclined position near the flame whichdoes not cause over boiling.
Discussion
i. Normal urine also contains a trace of glucose and glucuronates; but their amount is toosmall to cause reduction in Benedict’s test.
ii. Benedict’s test is not necessarily indicative of glucose in urine only but it too indicates thepresence of other reducing sugars such as lactose ( in case of pregnant women and lactatingmothers), fructose (in fructosuria), galactose (in glactosuria), pentose (In pentosuria),homogentisic acid (in alkaptonuria), glucuronates and mucin. In diabetes mellitus and inrenal glycosuria, glucose is found in urine. This gives a Benedict’s test positive.
2. Ketone Bodies
Rothera’s TestPrinciple: Acetoacetic acid forms a complex with sodium nitroprusside in alkaline solutiondeveloping a permanganate colour.
Procedure: Saturate 5 ml of urine with solid ammonium sulphate by shaking it vigorously.then add 2 drops of freshly prepared 5% solution of soldium nitroprusside and 1 ml ofammonium hydroxide. Allow it to stand in the rack for a while. A permaganate colour developsjust above the layer of the undissolved ammonium sulphate crystals indicating the presence ofketone bodies.
Discussion
i. In diabetes mellitus and in prolonged starvation, fat is catabolised to produce acetoaceticacid, acetone and B-hydroxybutyric acid which are together termed as acetone or ketonebodies. These acetone bodies are accumulated in blood and excreted in urine. This conditionis called ketosis. The excretion of ketone bodies in urine is called ketonuria.
ii. Ketosis also occurs in the acetonemic vomiting of childhood, and frequently in pregnancy,fevers, ether and chloroform anesthesia, malnutriton, prolonged feeding of a carbohydratepoor diet, high in meat and fat.
iii. Total ketone bodies are found in normal urine to the extent of about 20 mg. In 24 hours.Pathologically, values from 0.02 to 6 grams or more per day have been observed.
iv. B-hydroxybutyric acid, as such, does not give Rother’s or Gerhardt’s test positive unlessconverted to acetoacetic acid and then to acetone oxidation.

Urine 169
3. Albumin
a. Sulphosalicylic acid testPrinciple: Albumin, the protein, is denatured by sulphosalicylic acid causing a coagulation.
Procedure: Add a few drops of sulphosalicylic acid to 2 ml of clear urine (filter if not clear). Aturbidity indicates the presence of albumin.
This test is used for routine work.
Discussion
i. A trace of protein which is less than 250 mg, in 24 hours urine found in normal urine. Thisamount is so slight that it escapes detection by any or the simple tests.
ii. Some proteins (albumin and globulin) are found in the urine under pathological conditionsknown as albuminuria.
iii. In kidney disturbance and in altered high blood pressure, albumin is found in urinesignificantly.
iv. Benign proteinuria (usually transitory), appears in severe exercise or cold baths, particularlyin young people.
4. Blood Pigments (Benzidine test)
Principle: Hemoglobin of blood decomposes hydrogen peroxide catalytically and liberatesoxygen. This oxygen oxidizes benzidine to a blue or green compound.
This colour changes to brown within a few minutes on exposure to air.Procedure: Take a pinch of solid benzidine in a test tube and 2 ml. of glacial acetic acid till thebenzidine dissolves. Add 2 ml of hydrogen peroxide (H2O2) to it. Divide it into two portions.
To one portion add urine drop by drop with shaking. The appearance of deep blue colourindicates the presence of blood pigments. This quickly changes to brown within a few minutes.
To the other part add water drop by drop. No. blue colour appears. This part is treated ascontrol.
Discussion
1. Blood occurs in urine under hematuria and hemoglobinuria hematuria consists ofhaemoglobin and unruptured corpuscles. Hematuria is brought about by blood into theurine because of some lesion of the kidney or of the urinary tract. Hemoglobinuria resultsfrom hemolysis. This occurs in malaria, typhoid, haemolytic jaundice, yellow fever and intransfusion with incompatible blood.

170 Biochemistry for Dental Students
2. The presence of high concentration of ascorbic acid in urine is oxidized more readily thembenzidine by oxygen liberated from hydrogen peroxide. The benzidine reaction then becomesnegative although sufficient blood is present in urine.
3. The benzidine test is a very sensitive test.
Hays Test for Bile salts
Principle: Bile salts reduce the surface tension of the urine because of which sulfur powdersinks.Procedure: Fill half of a test tube with urine and another test tube with water, sprinkle gentlypinch of sulphur powder on the surface of two liquids.
The sulphur powder spontaneously sinks in the test tube containing urine which indicatesthe presence of bile salts but in the other test tube containing water no sulfhur powder sinks.
Discussion: Bile duct obstruction by inflammation orgall stones in gallbladder leads to theobstruction of bile into the general circulation. The subcutaneous tissues are deeply stainedresulting in the yellow complection which is the charcterstistic of jaundice. In such case bilesalts and bile pigments are detected in urine.
Abnormal Constituents of Urine
Constituent Conditions in which appear in large quantity
Glucose Diabetes mellitus, Renal glycosuriaKetone bodies On prolonged starvation, Low.
Carbohydrate high–fat diet, severe diabetes mellitus(Diabetic ketosis)
Protein Nephrotic syndrome,Glomerulonephritis
Blood Haematuria,Haemoglobinuria
Bile salts and pigments Obstructive jaundiceUrobilinogen Obstructive jaundice.

INDEX
AAmino acid pool 102Amino acids 39
absorption 98catabolism 102classification 39clinical applications 45function 42occurrence 42properties 43
Angiotensin 45Anomers 7Antibiotics 45Antioxidants 20Antiparallel b sheets 30, 31
BBalanced diet 147Barfoed’s test 154Basal metabolic rate 144Benedict’s test 154, 165, 167Benzidine test 169Biuret reaction 34Biuret test 159, 165Blood calcium 130Bradykinin 46
CCalcitriol 130Calcium 128
absorption 129daily requirements 129disorders of calcium
metabolism 130distribution 129physiological functions 128
Calorigenic action 144Carbohydrate 3
absorption 56, 58biomedical importance 3classification 4digestion 56
metabolism 59Cellulose 11Cephalins 21Chitin 12Cholesterol 22, 91, 158
degradation 93metabolic fates 93metabolism 91
biosynthesis 91, 92Chondroitin sulfates 15Citric acid cycle 62
energetics 63reaction 62, 64
Coenzymes 53Conversion of pyruvate to lactate
61Copper 136Cori cycle 71
DDark adaptation time 112Deamination 104Decarboxylation 44Dehydration 8Denaturation 33Dermatan sulfate 15Dextrins 10Diabetes mellitus 75
insulin dependent 76non-insulin dependent 77
causes 77control 78symptoms 77
EEmulsification 157Emulsification and micelle 82Energy content of foods 142Enolization 7Enzymes 47
classification 51division 52
enzyme activity 47enzyme enhibition 50mechanism of enzyme action
49nomenclature 51
Essential fatty acids 24
FFats and oils 18
properties 19Fatty acids 23
biosynthesis 88chain elongation inmicrosomes 91chain elongation inmitochondria 91synthesis in cytoplasm 88
oxidation 85activation 85metabolic fates 88β-oxidation 87transport of acyl CoA 85
Fehling’s test 154Fibres 146Fluorine 139Fluorosis 140Formaldehyde–H2SO4 test 158
GGluconeogenesis 67
occurrence 69reactions 69significance 67
Glucose tolerance test 78Glutathione 46Glycerol 23Glycerophosphatides 20Glycogen 11Glycogenesis 65
pathway 66Glycogenolysis 67Glycolipids 21

172 Biochemistry for Dental Students
Glycolysis 59energetics 61pathway 59
energy generation phase60energy investment phase59splitting phase 59
Glycosaminoglycans 12Glycosides 8Glycosidic bond 8Grease-spot test 157
Hα-Helix 30Hays test for bile salts 170Hemochromatosis 136Heparin 15Hormones 46Human health and welfare 142Hyaluronic acid 13Hyaluronidase 14Hydrolysis 19Hypercalcemia 130Hypernatremia 134Hypocalcemia 130Hyponatremia 133
IInulin 11Iodine 137Iodine test 153Iron 134Iron deficiency anemia 135Isomaltose 10
KKashin-Beck diseases 141Kellidin 46Keratan sulfate 15Keshan diseases 140Ketone bodies 93, 94, 168Koshald hypothesis 49
LLactose 9Lecithins 21
Lipids 17biomedical importance 17classification 20
compound lipids 20derived lipids 22simple lipids 18
digestion 81absorption 82detergent action of bilesalts 81mechanical mixing due toperistalsis 82metabolism 84surfactant action ofdegraded lipids 82
peroxidation 20properties 17
Lipoproteins or proteolipids 21
MMagnesium 132Maltose 9Manganese 137Menke’s disease 137Metabolism of proteins 101Millon’s test 160Molisch’s test 153Monosaccharides 5Mutarotation 6
NNinhydrin test 34, 160Nutritional disorders 149
OOligosaccharides 8Osazone
formation 7test 155
PPancreatic enzymes 98Parathyroid hormone 130Pepsin 97Peptide bond 30Peptides 45
Phasmalogens 21Phosphatidic acid 21Phospholipids 20Phosphorus 131
biochemical importance 131serum phosphate level 131
Plasma proteins 34Polysaccharides 10
hetero 12homo 10muco 12
Potassium 134Production of ATP 61Protein and polypeptides 100Proteins 26, 159
classification 27conjugated 28plasma protein 34simple 28
clinical importance 26composition 27digestion 97group tests 33
coagulation reaction 33,161colour reactions 33, 159precipitation reaction 33,161
properties 32structure 29
primary 30quarternary 32secondary 30tertiary 32
Proteoglycan complex 13
RRancidity 19
hydrolytic 20oxidative 20
Recommended dietaryallowances 146
Regulation of blood sugar 72hormonal regulation 75
adrenal cortex 75growth 75thyroid 75
role of extrahepatic tissues 73role of hormones 73role of liver 73

Index 173
Renin 98Respiratory quotient 143Rhodopsin 111
SSalivary amylase 56Salkowski’s test 158Saponification 19, 157Selenium 140Selivanoff’s test 8, 155Sodium 133Sphingomyelin 21Starch 10Steroids 21Sucrose 9
TTautomerization 7Transamination 103Transport of ammonia 105Triacylglycerol or triglycerides
18
UUnsaturation test 158Urea cycle 105
disposal of urea 108energetics 107reaction 106
Urine 163abnormal constituents 167
albumin 169
blood pigments 169ketone bodies 168reducing sugars 167
chemical characteristics 164nitrogenous constituents
creatine 165uric acid and urates 165
non-nitrogenous constituents166
physical characteristics 163appearance 164colour 163frequency 163odour 164preservation 163specific gravity 164volume 163
Utilization of energy in man 143
VVitamins 109
ascorbic acid (vitamin C)daily requirements 116deficiency 117physiological function 117
fat soluble 109vitamin A 110
daily requirements 110deficiency 112physiological functions111
vitamin D [calcitriol]daily requirements 112deficiency symptoms 113
physiological functions113
vitamin E 113deficiency 115physiological functions114
vitamin Kdaily requirement 115deficiency 116physiological function 115
vitamins of B complex 117biotin (B7) 125folic acid 123niacin 121pantothenic acid 123pyridoxine 122riboflavin (vitamin B2)119thiamine (vitamin B1) 118vitamin B12 124
water soluble 109, 116
WWald’s visual cycle 111Waxes 20Wilson’s disease 137
XXanthoproteic reaction 160
ZZinc 138Zwitterion 43