BILIARY AND DUODENAL STENTING - …eradiology.bidmc.harvard.edu/LearningLab/gastro/Deol.pdfFindings...
36
Satjeet Deol, DMCH, Ludhiana, INDIA V Year Gillian Lieberman, MD April 2013 Satjeet Deol, V YEAR Gillian Lieberman, MD BILIARY AND DUODENAL STENTING
Transcript of BILIARY AND DUODENAL STENTING - …eradiology.bidmc.harvard.edu/LearningLab/gastro/Deol.pdfFindings...

Satjeet Deol, DMCH, Ludhiana, INDIA V Year
Gillian Lieberman, MD
April 2013
Satjeet Deol, V YEAR
Gillian Lieberman, MD
BILIARY AND DUODENAL
STENTING

2
OVERVIEW
• PATIENT REVIEW
• STEPS OF BILIARY STENTING
• COMPLICATIONS
• REVIEW OF MANAGEMENT OF UNRESECTABLE
PANCREATIC CANCER
• OUTCOMES
• ALTERNATIVES
Satjeet deol, V year
Gillian Lieberman, MD

3
HPI
• Patient presented with nausea, vomiting and diarrhea since 1 month
PAST MEDICAL HISTORY-
• Diabetes( dx1995),hyperlipidemia
PAST SURGICAL HISTORY-
• vitrectomy, cataract removal
Medications- Metformin, Glyburide, Simvisatatin
PATIENT REVIEW
Satjeet deol, V year
Gillian Lieberman, MD

4
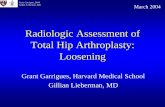
Axial C+ CT scan-Ill defined mass in the head of pancreas
Gastric dilatation(PACS BIDMC)
Satjeet deol, V year
Gillian Lieberman, MD
Our Patient: Pancreatic mass on CT

5 Axial C+ CT scan-Multiple liver metastasis
Gastric dilatation (PACS BIDMC)
Satjeet deol, V year
Gillian Lieberman, MD
Our Patient: Liver metastasis on CT

6
MRCP(Axial view)-Ill defined mass in the head of pancreas
Duodenal and gastric dilatation(PACS
BIDMC)
Satjeet deol, V year
Gillian Lieberman, MD
Our patient: Pancreatic mass on MRCP

7
Our patient: Dilated CBD on MRCP
Dilated CBD along with
gastric dilatation
Satjeet deol, V year
Gillian Lieberman, MD
Liver metastasis

Findings on MRCP
• There is 4.6 cm ill defined mass centered on head of
pancreas causing obstruction of the pancreatic duct and
CBD.
• The lesion is compressing the duodenum resulting in
duodenal and gastric dilatation.
• The lesion tethered and flattened SMV consistent with its
involvement.
• Multiple liver metastasis were present which were further
evaluated with US guided liver biopsy.
8

Our Patient:ULTRASOUND GUIDED LIVER
BIOPSY
9
Satjeet deol, V year
Gillian Lieberman, MD
USG: Lesion seen in right lobe of liver
(PACS BIDMC)

LIVER BIOPSY NEEDLE
10
Satjeet deol, V year
Gillian Lieberman, MD
USG:Biopsy needle going inside lesion(PACS BIDMC)

STAGING OF PANCREATIC
CANCER PRIMARY TUMOR(T)
• T1 Tumor limited to the pancreas, 2 cm or less in greatest dimension
• T2 Tumor limited to the pancreas, more than 2 cm in greatest dimension
• T3 Tumor extends beyond the pancreas but without involvement of the celiac
axis or the superior mesenteric artery
• T4 Tumor involves the celiac axis or the superior mesenteric artery
(unresectable primary tumor)
Regional Lymph Nodes (N)
• NX Regional lymph nodes cannot be assessed
• N0 No regional lymph node metastasis
• N1 Regional lymph node metastasis
Distant Metastasis (M)
• M0 No distant metastasis
• M1 Distant metastasis
11
Satjeet deol, V year
Gillian Lieberman, MD

Unresectable Metastatic Pancreatic
cancer
• Diagnosis of metastatic pancreatic cancer
was made based on imaging and was
confirmed by liver biospy consistent with
metastasis of pancreatic origin.
• For the palliation of obstruction,duodenal
stent was placed under ERCP
12
Satjeet deol, V year
Gillian Lieberman, MD

Coronal and axial C+ CT scan-Duodenal stent in 2nd part of
duodenum (PACS BIDMC) 13
Satjeet deol, V year
Gillian Lieberman, MD
Our Patient:Duodenal stent on CT

Our patient:Clinical course
• After placement of duodenal stent under ERCP patient
started developing increasing jaundice and raising bilirubin
levels.
• PTBD was performed and 8F internal external biliary drain
was placed in IR.
• But patient’s condition was not improving so the patient
underwent biliary stenting for distal CBD obstruction. • Sebsequently the patient’s condition improved
14
Satjeet deol, V year
Gillian Lieberman, MD

15
Our Patient:Percutaneous Transhepatic
Cholangiogram
Satjeet deol, V year
Gillian Lieberman, MD
Obstruction at distal CBD resulting in proximal
dilatation(PACS BIDMC)

PTBD using 8F biliary drain
16
Satjeet deol, V year
Gillian Lieberman, MD

STEPS OF BILIARY
STENTING
17 Insertion of guide wire through prexisting
biliary drain
Satjeet deol, V year
Gillian Lieberman, MD

Constrast showing distal CBD
obstruction
18
Satjeet deol, V year
Gillian Lieberman, MD

Dilatation of CBD by 8mm x4
cm balloon
19
Satjeet deol, V year
Gillian Lieberman, MD

Balloon fully inflated
20
Satjeet deol, V year
Gillian Lieberman, MD

Insertion of 8 mm wall stent
21
Satjeet deol, V year
Gillian Lieberman, MD

Contrast going into bowel
22
Satjeet deol, V year
Gillian Lieberman, MD

Coronal C+ CT showing duodenal and biliary stent along
with anchor drain(PACS BIDMC) 23
Satjeet deol, V year
Gillian Lieberman, MD
Our Patient:Duodenal and biliary stent
on CT

• BLEEDING
• HEMOBILIA
• CAPSULAR HAEMATOMA
• BLOCKAGE
• CHOLANGITIS
24
COMPLICATIONS OF BILIARY
STENTING
Satjeet deol, V year
Gillian Lieberman, MD

Complications of advanced pancreatic
cancer
• Gastric outlet obstruction
• Duodenal and biliary obstruction
• Abdominal pain
• Back pain
25
Satjeet deol, V year
Gillian Lieberman, MD

Management of unresectable metastatic
pancreatic cancer
• Palliative chemotherapy-
First line- Gemcitabine and capecitabin
Second line-5FU and oxaliplatin
• Palliation of obstructive symptoms- Palliative
surgical bypass,endoscopic duodenal stent,
percutaneous radiologic biliary stent placement, or
endoscopic biliary stent placement
• DROP Trial compared stenting versus
gastrojejunostomy for the palliation of obstructive
symptoms
26
Satjeet deol, V year
Gillian Lieberman, MD

OUTCOMES 1.Endoscopic placement of self-expandable metal stents
(SEMSs) is the most effective palliative treatment for
inoperable malignant gastroduodenal or biliary strictures
2.Endoscopic stenting of combined duodenal and biliary
malignant obstructions remains techanically difficult and
percutaneous approach for biliary stenting is preferred
27
Satjeet deol, V year
Gillian Lieberman, MD
A-Central type SEMS
B-Lateral type SEMS

What is Known: SEMS and DO
• Rapid relief of symptoms
• Technical success and clinical success 96% and
90%
• Reintervention for occlusion 20% (time related).
• Comparative retrospective and randomized trials
of SEMS vs. palliative bypass with GJ – better for
survival > 3 months
28
Satjeet deol, V year
Gillian Lieberman, MD

What is Evolving: Combined Biliary and
Duodenal Palliation
29
Satjeet deol, V year
Gillian Lieberman, MD

Type 1 with duodenal stent in duodenal
bulb
30
Satjeet deol, V year
Gillian Lieberman, MD

31
Satjeet deol, V year
Gillian Lieberman, MD
Duodenal stent

ALTERNATIVE-ARGON PLASMA
COAGULATION
32
Exposing ampulla for endoscopic cannulation of CBD with
duodenal stent in place
Satjeet deol, V year
Gillian Lieberman, MD

Endoscopic stenting of CBD
33
Satjeet deol, V year
Gillian Lieberman, MD

Alternative-Open cell design stents
• Duodenal stricture : 87% success and 10%
complications
34
Satjeet deol, V year
Gillian Lieberman, MD

35
References
• Barish MA, Yucel EK, Ferruci JT. Magnetic resonance
cholangiopancreatography. N Engl J Med 1999
• BMC Gastroenterology 2007 7:18
• Gastrointestinal endoscopy volume 70
• Staging of pancreatic adenocarcinoma (AJCC)
• Rosewicz S, Wiedenmann B. Pancreatic carcinoma.
Lancet 1997; 349: 483-89.

36
Acknowledgements
Dr Gillian Lieberman
Dr Ian Brennan