Xanthogranulomatous cholecystitis vs Gallbladder...
30
Xanthogranulomatous Cholecystitis: Ultrasound, CT, and MRI findings Julia T. Chu, HMS IV Laura Avery, M.D. Gillian Lieberman, M.D. Ultrasound MRI CT
Transcript of Xanthogranulomatous cholecystitis vs Gallbladder...

Xanthogranulomatous Cholecystitis:
Ultrasound, CT, and MRI findings
Julia T. Chu, HMS IVLaura Avery, M.D.
Gillian Lieberman, M.D.
Ultrasound MRICT

Agenda
•
Patient:
53yo M with RUQ abd
pain•
DDx: RUQ abd
pain
•
Imaging Modalities: available to image our patient•
Radiologic Findings:
US, CT, MRI
gangrenous cholecystitis, adenomyomatosisreview of anatomy and pathophysiology
•
Pathology Dx: Xanthogranulomatous
cholecystitis•
Management: Depends on radiologic Dx!
•
Take-Home Points
Our Patient: History & Physical Exam
•
Hx:
53yo M with intermittent RUQ abd
pain for 2 years; no fever/chills, nausea/vomiting, weight loss, or food association
•
PMH:
DM 2, hyperlipidemia, HTN•
Meds:
Metformin, ASA, lisinopril, atorvastatin
•
SH:
Plumber married w/ children; (+) smoking, (-) EtOH
•
Exam:
(+) Murphy sign, (+) guaiac•
Labs:
Leukocytosis, ↑
Alk
Phos, ↑
LFTs, ↑
GGT

VascularInfarct
Pyelophlebitis
Mesenteric thrombosis
Adrenal infarct
Occlusion
Embolism
Renal vein thrombosis
Clinical DDx:
RUQ abd
pain (by mnemonic)
“V I N D I C A T E”
Inflammation/InfectionCellulitis, Osteomyelitis
Diaphragmatic abscess
Trichinosis, TB, Herpes zoster
Hepatitis, Hepatic abscess
Cholecystitis, Cholangitis
Duodenitis, Diverticulitis, Colitis
Pancreatitis, Pyelonephritis
Ulcer, Mesenteric adenitis
Waterhouse-Friderichsen
syndrome
NeoplasmCarcinoma
Cholangioma
Pancreatic carcinoma
Hodgkin disease
Lymphosarcoma
Neuroblastoma
Adrenal carcinoma
Multiple myeloma
Intoxication/ IdiopathicAlcoholic hepatitis
Ulcer
Gout
DegenerativeOsteoarthritis
Allergic/ AutoimmuneRheumatoid spondylitis
Congenital/
Acquired AnomalyVentral hernia
Incisional
hernia
Diverticulum
Obstruction
Cyst
Hydronephrosis
TraumaContusion
Cough
Hemorrhage
Laceration
Rupture
Herniated disc
Spine fracture
EndocrineHyperparathyroidism
www.wrongdiagnosis.com

Gallbladder carcinoma
Cholecystitis
and cholelithiasis
Hepatic flexure syndrome
Carcinoma of the colon with obstruction
ColitisDiverticulitis
Pyelonephritis
Embolic nephritis
Renal calculus
Carcinoma of the pancreas
Pancreatic calculus
Pancreatitis
Duodenal ulcer
Common duct stone
Cholangitis
LacerationBudd-Chiari
syndromeCarcinoma
Subphrenic
abscess
Hepatitis
Liver abscess
DDx:
RUQ abd
pain (by anatomy)
Legend:
Liver Pancreas
Bile duct Small bowel
Gallbladder Large Bowel
Renal System Others
Budd-Chiari
syndrome
Liver abscess
Laceration
Hepatitis
Carcinoma
Common duct stone
Cholangitis
Pancreatitis
Pancreatic calculus
Carcinoma of the pancreas
Duodenal ulcer
ColitisDiverticulitis
Carcinoma of the colon with obstruction
Hepatic flexure syndrome
Cholecystitis
and cholelithiasis
Pyelonephritis
Embolic nephritis
Renal calculus
Gallbladder carcinoma
Subphrenic
abscess
Pneumonia/empyema
pleurisy
www.wrongdiagnosis.com
Our patient’s main DDx, based on:
RUQ pain
(+) Murphy Sign
leukocytosis,
would be most likely centered on which organ?
Thus, would involve which conditions?
Imaging Modalities: Available/Applicable to Our Patient
with RUQ pain, ↑
WBC, (+)Murphy•
Ultrasound (US): abdomen/gallbladder
to look for gallstones, aneurysm•
Nuclear Medicine: cholescintigraphy
(or
HIDA scan)
with or w/out cholecystokinin
to evaluate the function of the gallbladder and the bile ducts
•
X-ray: Upper GI series
to rule out stomach/duodenum conditions; abdomen; colon barium enema; chest x-ray to rule out pneumonia
•
Computed Tomography (CT): abdomen to further evaluate the gallbladder for mass/carcinoma as well as other abd
organs such as the nearby pancreas
•
Magnetic Resonance Imaging (MRI): T1 with fat saturation, T2 to assess soft tissue changes such as fluid, inflammation, edema; MR cholangiopancreatography
(MRCP) to visualize the biliary
tract and pancreatic ducts
•
Invasive: cholangiography, percutaneous
cholecystostomy, endoscopic retrograde cholangiopancreatography
(ERCP)
American College of Radiology, www.acr.org
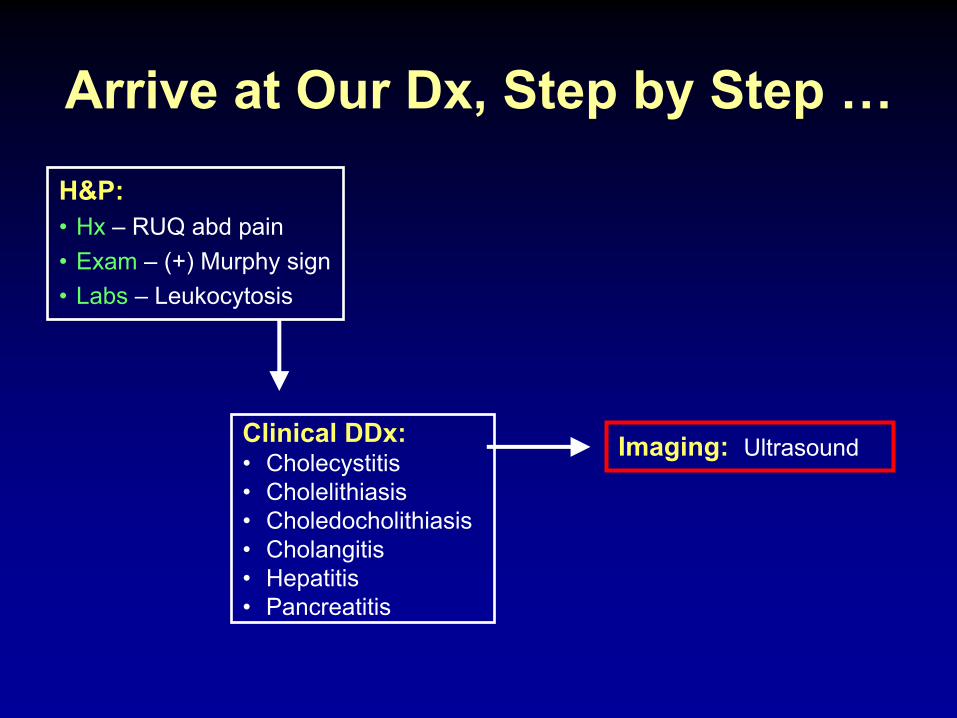
Arrive at Our Dx, Step by Step …
Clinical DDx:•
Cholecystitis•
Cholelithiasis•
Choledocholithiasis•
Cholangitis•
Hepatitis•
Pancreatitis
Imaging: Ultrasound
H&P:•
Hx
–
RUQ abd
pain•
Exam –
(+) Murphy sign•
Labs –
Leukocytosis

Our Patient: Findings on Ultrasound
Patient
√
Marked irregular GB wall thickening √
Cholelithiasis
with (+) US Murphy sign
Abd
aorta
Impression:
Gangrenous cholecystitis
vs GB carcinoma
Partners CAS
Normal Liver
Gallbladder
Courtesy of Dr. MaryEllen
Sun (BIDMC PACS)
Hyperechoic
fatty liver with abnormality in the region contiguous to gallbladder
Film Findings: hyperechoic
fatty liver, markedly thickened gallbladder wall, cholelithiasis
with (+) US Murphy sign
SagittalSagittal

Arrive at Our Dx, Step by Step …
Clinical DDx:•
Cholecystitis•
Choledocholithiasis•
Cholangitis•
Hepatitis•
Pancreatitis
Imaging: CT to evaluate gallbladder wall thickening vs “mass”; why?
•
gallbladder carcinoma has a poor prognosis of 85% mortality within 1 year of diagnosis
•
need to further evaluate the US findings with more imaging studies before embarking on any treatment
H&P:•
Hx
–
RUQ abd
pain•
Labs –
Leukocytosis•
Exam –
(+) Murphy sign
US DDx:•
Gangrenous cholecystitis•
Gallbladder carcinoma
US Findings:•
Irregular gallbladder wall thickening

Our Patient: Findings on CT scan
Partners CAS
Axial, oral C+
Cystic structure
Cystic duct
Common hepatic duct
Common bile duct
Gallbladder
Neck
BodyFundus
www.wiltshiresurgery.com
Heterogeneous low density in the adjacent liver
Irregular wall thickening involving the gallbladder fundus
Film Findings:
Irregularly thickened wall at the gallbladder fundus, low attenuation in liver adjacent to the gallbladder, cyst at the fundus.

Partners CAS
Impression:
CT findings suspicious for malignancy. Infection much less likely given no pericholecystic
fluid
or inflammation.
Our Patient: Pertinent negative findings on CT scan
Coronal, oral and IV C+
No wall thickening in the inferior and medial aspect of the gallbladder
No pericholecystic
fluid or inflammation
No intra or extrahepatic
biliary
ductal
dilatation
Cystic structure
Irregular wall thickening involving the gallbladder fundus

Arrive at Our Dx, Step by Step …
Clinical DDx:•
Cholecystitis•
Choledocholithiasis•
Cholangitis•
Hepatitis•
Pancreatitis
CT Findings: •
Irregular wall thickening at the gallbladder fundus•
Cystic structure at the gallbladder fundus•
No pericholecystic
fluid or inflammation•
No biliary
ductal
dilatation
H&P:•
Hx
–
RUQ abd
pain•
Labs –
Leukocytosis•
Exam –
(+) Murphy sign
US DDx:•
Gangrenous cholecystitis•
Gallbladder carcinoma
US Findings:•
Irregular gallbladder wall thickening
CT DDx: gallbladder malignancy
Imaging: MR to further evaluate soft tissue changes in the gallbladder and the adjacent liver to assess inflammatory changes and confirm or rule out malignancy

Our Patient: Findings on MR imaging
Axial T1-weighted Gradient Echo with Fat Sat; Post-Gadolinium Arterial Phase
Partners CAS
Axial T1-weighted Hi-Resolution with Fat Sat; Post-Gadolinium
Partners CAS
Wall thickening along the fundus
measuring up to 15mm in maximum thickness
Slight enhancement of GB wall mucosa, most prominently involving the fundal
portion
Film Findings: thickened gallbladder wall with hyper-intensity of the mucosa mostly involving the fundus

Our Patient: Findings on MR imaging
Axial T1-weighted Gradient Echo with Fat Sat; Post-Gadolinium, Arterial Phase
Partners CAS
Axial T1-weighted Hi-Resolution with Fat Sat; Post-Gadolinium
Partners CAS
Small cystic area adjacent to the fundus
measuring up to 2.0 cm, (+) rim enhancement
No clear communication between the fundus
and this cystic collection could be demonstrated
Film Findings: small cyst at the fundus
with ? communication to the gallbladder that cannot be clearly identified on MR

Axial T2-weighted with Fat Saturation
Partners CAS
Our Patient: Findings on MR imaging
Gallbladder sludge and stones
Coronal T2-weighted Single-Shot Fast Spin Echo (SSFSE)
Partners CAS
Irregular wall thickening involving the gallbladder fundus
Film Findings: Gallstones and, again, irregularly thickened gallbladder wall involving the fundus

Our Patient: Findings on MR imaging
Partners CAS
Coronal 2D Thick-Slab Abdomen (MR Cholangiopancreatography, or MRCP)
Copyright ®
The McGraw-Hill Companies, Inc.
Gallbladder
Duodenum
Cystic duct
Right hepatic duct Left hepatic duct
Common hepatic duct
Common bile duct
Gallbladde
r
carcinoma
Common hepatic duct
CommonCommon bile duct
Common
CommonR and L
hepatic ducts
Cystic duct
CoGallbladder
ComMain pancreatic duct
ComHepatopancreatic
ampulla
ComMajor duodenal papilla
ComDuodenum
(1)
(2)
(3)(4)
Pancreatic duct
Hepatopancreatic
ampullaMajor duodenal papilla
http://academic.kellogg.cc.mi.us/herbrandsonc/bio201
McKinley/Digestive%20System.htm
Film Findings: No biliary/pancreatic duct obstruction/dilatation Impression:
Normal biliary/pancreatic ductal
system.

(1) R and L hepatic ducts merge to form a common hepatic duct
Quick Review: The Biliary
and Pancreatic Ducts
Copyright ®
The McGraw-Hill Companies, Inc.
Gallbladder carcinoma
Common hepatic duct
CommonCommon bile duct
Common
CommonR and L
hepatic ducts
Cystic duct
CoGallbladder
ComMain pancreatic duct
ComHepatopancreatic
ampulla
ComMajor duodenal papilla
ComDuodenum
(2)
(3)(4)
(1)
(4)
Bile and pancreatic juices enter duodenum at the major duodenal papilla
(2)
Common hepatic and cystic ducts merge to form a common bile duct
(3)
Pancreatic duct merges with common bile duct at the hepatopancreatic
ampulla
http://academic.kellogg.cc.mi.us/herbrandsonc/bio201_McKinley/Digestive%20System.htm
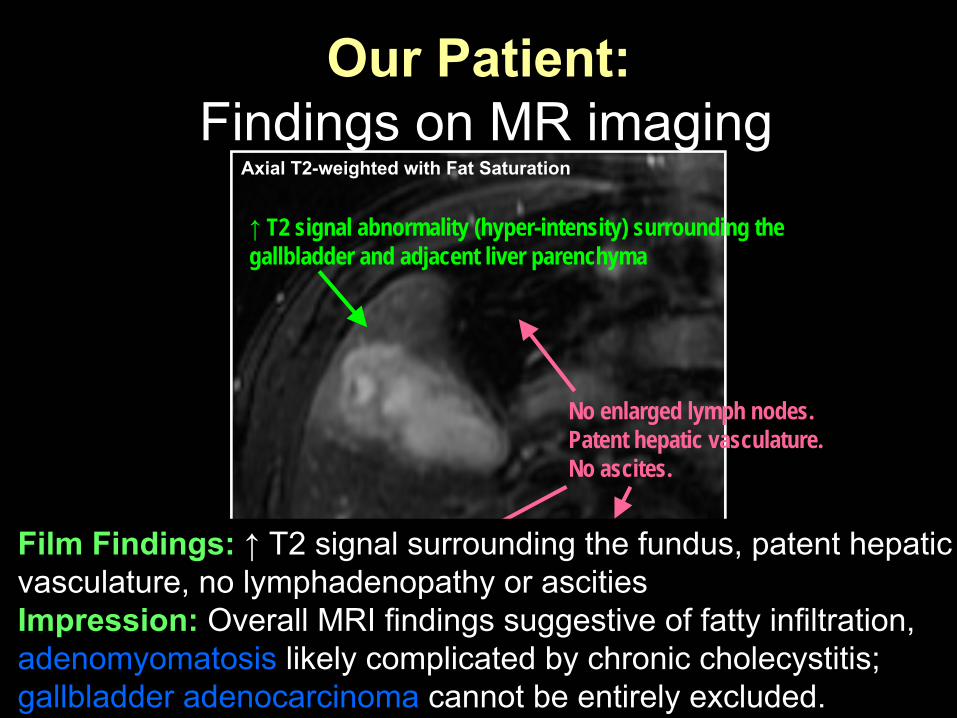
Our Patient: Findings on MR imaging
Axial T2-weighted with Fat Saturation
Partners CAS
↑
T2 signal abnormality (hyper-intensity) surrounding the gallbladder and adjacent liver parenchyma
No enlarged lymph nodes. Patent hepatic vasculature. No ascites.
Film Findings: ↑
T2 signal surrounding the fundus, patent hepatic vasculature, no lymphadenopathy
or ascities
Impression:
Overall MRI findings suggestive of fatty infiltration, adenomyomatosis
likely complicated by chronic cholecystitis;
gallbladder adenocarcinoma
cannot be entirely excluded.

MRI Dx:
What is Adenomyomatosis?
•
Definition:
benign, abnormal though non-premalignant gallbladder mucosal hyperplasia, muscular wall thickening, and formation of intramural diverticula
or sinus
tracts called Rokitansky- Aschoff
sinuses
•
Radiologic Finding:
Pearl Necklace Sign
uodenumuodenum
Haradome, H. et al. Radiology 2003. 227(1): 80-8.
Very small cystic
structures
Very small cystic
structures
(Pearl Necklace Sign)
(Pearl Necklace Sign)
Multiple Multiple gallbladder stonesgallbladder stones

Arrive at Our Dx, Step by Step …
Clinical DDx:•
Cholecystitis•
Choledocholithiasis•
Cholangitis•
Hepatitis•
Pancreatitis
H&P:•
Hx
–
RUQ abd
pain•
Labs –
Leukocytosis•
Exam –
(+) Murphy sign
US DDx:•
Gangrenous cholecystitis•
Gallbladder carcinoma CT DDx: gallbladder malignancy
Pathology/Management: Open cholecystectomy to make the definitive, final Dx by histology and determine future management of our patient
MR DDx:•
Adenomyomatosis•
Gallbladder adenocarcinoma
MR Findings:•
Thickened gallbladder wall•
Fundus
cyst with ?communication•
Gallbladder stones•
No biliary
obstruction/dilatation•
↑
T2 signal surrounding the fundus

Our Companion Patient: Findings on Gross Pathology
Diffuse wall thickening
Serosa
covered with dense fibrous adhesions
Ulcerated mucosal surface
Yellow nodules/plaques, or Yellow nodules/plaques, or xanthogranulomatousxanthogranulomatous
foci, extend into foci, extend into adjacent liver through the walladjacent liver through the wall
Levy, A. et al. Radiographics. 2002. 22(2): 387-413.
Cross section of the Cross section of the resectedresected
gallbladdergallbladder
Disruption of the gallbladder wall
Gross Pathology Findings:
(1) fibrosis and wall thickening (2) disruption of gallbladder wall (3) xanthogranulomatous
foci

Our Companion Patients: Findings on Histology
Varadarajulu
S, et al. Up-to-Date
Fibroblasts, Fibroblasts, inflammatory cellsinflammatory cells
SpindleSpindle--shaped cells shaped cells with more granular with more granular cytoplasm and cytoplasm and elongated nucleielongated nuclei
Lipid-laden mø: 2 morphological types
Levy, A. et al. Radiographics. 2002. 22(2): 387-413.
XanthogranulomatousXanthogranulomatous
cholecystitischolecystitis
focus (focus (blackarrowsblackarrows
above)above)
H&E stainH&E stain
Thickened, fibrotic wall
Contains: (1) bile pigment (2) chronic inflammatory cells (3) foamy pigment-laden macrophages (mø)
No dysplasia or malignancy!
Rounded foamy Rounded foamy macrophagesmacrophages
(1)(1)
(2)(2)

Arrive at Our Dx, Step by Step …
Clinical DDx:•
Cholecystitis•
Choledocholithiasis•
Cholangitis•
Hepatitis•
Pancreatitis
H&P:•
Hx
–
RUQ abd
pain•
Labs –
Leukocytosis•
Exam –
(+) Murphy sign
US DDx:•
Gangrenous cholecystitis•
Gallbladder carcinoma CT DDx: gallbladder malignancy
MR DDx:•
Adenomyomatosis•
Gallbladder adenocarcinoma
Pathology (Final) Dx: Xanthogranulomatous
cholecystitis
Gross/Histologic
Findings:•
Wall thickening with fibrotic serosa•
Xanthogranulomatous
foci•
Bile extravasation
through disrupted wall•
Lipid-laden macrophages•
Chronic inflammatory cells
Dx:
What is Xanthogranulomatous
Cholecystitis?
•
Definition:
unusual form of benign, chronic cholecystitis
with focal or diffuse destructive
inflammatory process•
Signs and symptoms: RUQ abd
pain, fever,
leukocytosis, vomiting, (+) Murphy sign•
Hallmarks:(1) thickened, fibrotic, disrupted gallbladder wall(2) foamy histiocytes(3) bile extravasation

Dx:
What is Xanthogranulomatous
Cholecystitis?
•
Pathophysiology: gallbladder or cystic duct obstruction ↑ gallbladder intraluminal pressure rupture of Rokitansky-Aschoff sinuses or mucosal ulceration extravasation of bile into the gallbladder wall
s63.jpgs63.4x1.jpg
bile
biles63.jpg
http://anatomy.iupui.edu/courses/histo_D502/D502f04/Labs.f04/digestive%20III%20lab/Lab13index.htm

Management:
Significance of Xanthogranulomatous
Cholecystitis
•
Significance: may simulate malignancy clinically, radiologically, and pathologically
•
Management of XG cholecystitis: open cholecystectomy
with complete resection of the
gallbladder due to dense fibrosis, extensive inflammation, ?coexistent malignancy
•
Management of GB carcinoma: (1) aggressive surgery
–
partial/segmental hepatic
resection or Whipple procedure(2) no resection
at all with chemo/radiation instead

•
XG cholecystitis: benign yet focally/diffusely destructive inflammatory gallbladder disease with (1) fibrosis and wall thickening, (2) bile extravasation, (3) lipid-laden mø, (4) acute/chronic inflammatory cells
•
XG cholecystitis
vs GB carcinoma:
Patients with carcinoma are more likely to present with anorexia, weight loss, palpable mass, and jaundice
•
Preoperative Dx
by radiographs:
may significantly alter therapy and patient prognosis –
be careful!
Take Home Points:

What happened to Our Patient?
•
Our patient underwent an exploratory laparoscopy that was converted to open cholecystectomy, which went successfully without any complications
•
His gallbladder was diagnosed with xanthogranulomatous
cholecystitis
without
any associated malignancy by pathology and histology
•
Our patient is alive and well as of today in June, 2008

Acknowledgements
•
Gillian Lieberman, M.D.•
Laura Avery, M.D.
•
James Kang, M.D. (resident)•
Karen Lee, M.D. (fellow)
•
Maryellen Sun, M.D. (fellow)

ReferencesChun KA, Ha HK, Yu ES, Shinn KS, Kim KW, Lee DH, Kang SW, Auh
YH. Xanthogranulomatous
cholecystitis: CT features with emphasis on differentiation from gallbladder carcinoma. Radiology. 1997 Apr; 203(1): 93-7.
Guermazi
A. Are there other imaging features to differentiate xanthogranulomatous
cholecystitis
from gallbladder carcinoma? Eur
Radiol. 2005 Jun; 15(6): 1271-2.Haradome
H, Ichikawa T, Sou
H, Yoshikawa T, Nakamura A, Araki T, Hachiya
J. The pearl necklace sign: an imaging sign of adenomyomatosis
of the gallbladder at MR cholangiopancreatography. Radiology. 2003 Apr; 227(1): 80-8.
Levy AD, Murakata
LA, Rohrmann
CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001 Mar-Apr; 21(2): 295-314.
Levy AD, Murakata
LA, Abbott RM, Rohrmann
CA Jr. From the archives of the AFIP. Benign tumors and tumorlike
lesions of the gallbladder and extrahepatic
bile ducts: radiologic-pathologic correlation. Armed Forces Institute of Pathology. Radiographics. 2002 Mar-Apr; 22(2): 387-413. Review.
Shuto
R, Kiyosue
H, Komatsu E, Matsumoto S, Kawano K, Kondo Y, Yokoyama S, Mori H. CT and MR imaging findings of xanthogranulomatous
cholecystitis: correlation with pathologic findings. Eur
Radiol. 2004 Mar; 14(3): 440-6.
Srivastava
M, Sharma A, Kapoor
VK, Nagana
Gowda
GA. Stones from cancerous and benign gallbladders are different: A proton nuclear magnetic resonance spectroscopy study. Hepatol
Res. 2008 May 27.Varadarajulu
S, Zakko
SF. Xanthogranulomatous
cholecystitis. Up-to-date. 2007.Slides 16 and 17 –
http://academic.kellogg.cc.mi.us/herbrandsonc/bio201_McKinley/Digestive%20System.htm
Slide 25 –
http://anatomy.iupui.edu/courses/histo_D502/D502f04/Labs.f04/digestive%20III%20lab/Lab13index.htm