Benign and Malignant Lesions in Respiratory Cytology MISS SURUTTAYA CHINNAWONG.
43
Benign and Benign and Malignant Lesions Malignant Lesions in Respiratory in Respiratory Cytology Cytology MISS SURUTTAYA CHINNAWONG MISS SURUTTAYA CHINNAWONG
-
Upload
bruce-rose -
Category
Documents
-
view
231 -
download
2
Transcript of Benign and Malignant Lesions in Respiratory Cytology MISS SURUTTAYA CHINNAWONG.

Benign and Malignant Benign and Malignant Lesions in Respiratory Lesions in Respiratory
CytologyCytology
MISS SURUTTAYA CHINNAWONGMISS SURUTTAYA CHINNAWONG

Respiratory CytologyRespiratory Cytology
• Major role:– Diagnosis of malignant neoplasms
involving lung both primary and metastatic
• Minor role:– Opportunistic infection– Specific inflammatory process– Benign neoplasms, some

Sampling techniquesSampling techniques
• Exfoliative methods– Sputum cytology– Bronchial cytology (BW and BB)– Bronchoalveolar lavage (BAL)
• Fine needle aspiration (FNA)

Exfoliative methodsExfoliative methods
• Factors influences diagnostic yields– Tumor mass
• Location, size, histologic type
– Infiltrative lesion: inflammation• Diffuse process or localized process
• Sensitivity and specificity• False negative diagnoses

Sputum CytologySputum Cytology
• Symptomatic patients• Techniques:
– ”pick and smear”– Saccomanno– Cytospin or monolayer
• Advantages:• Disadvantages

Advantages of sputumAdvantages of sputum• Noninvasive• Reflect constituents from many regions of
lung• Useful for centrally located malignancies
(Squamous cell/Small cell CA)• High diagnostic yields: induced sputum, 3-5
samples continuously examined• Chronic inflammations: Asthma, COPD• Respiratory infections

Disadvantages of Disadvantages of sputumsputum
• Alveolar macrophages: lower respiratory tract elements
• Localized lung lesion, peripheral lesion
• Adenocarcinoma, metastatic lesion, lymphoma
• Benign tumor

Bronchial cytologyBronchial cytology
• Fiberoptic bronchoscopy• Bronchoscope positions at the area of
abnormality• Adequacy: large number of bronchial
epithelial cells and alveolar macrophages• Inadequate specimen: heavy oral
contamination, obscuring blood, inflammatory process, dried artefact
Bronchial cytology: Bronchial cytology: disadvantagesdisadvantages
• Limited area of the lung examined by bronchoscopy
• Invasive procedure: unpleasant for the patients
• Benign tumors, extremely peripheral lesions

Bronchoalveolar lavageBronchoalveolar lavage
• The most distal airspaces• Diffuse disease process• Pulmonary infection: opportunistic
infections• Interstitial lung disease• Lymphoproliferative disorders• Malignancy

BAL cytologyBAL cytology
• Adequacy: abundant alveolar macrophages
• Inadequacy: bronchial epithelial cells or squamous cells >75%


FNA cytologyFNA cytology
• Percutaneous transthoracic FNA– Direct lung tap– CT-guided FNAB
• Transbronchial (Wang’s needle) FNA– Bronchoscopy– Staging of lung tumors
• Hilar nodes• Mediastinal nodes• Subcarinal nodes

FNA lung lesionFNA lung lesion
• Sensitivity: 75-95%• Specificity: 95-100%• Classification of tumor: 70-85%• Complications: lesion depth/size, needle
– Pneumothorax: 5-10% need treatment– Hemoptysis– Air embolism

Normal Elements Normal Elements
• Upper respiratory tract– Nonkeratinizing stratified squamous cells
• Lower respiratory tract– Ciliated columnar bronchial epithelial cells– Goblet cells– Alveolar pneumocytes
• Reactive changes– Flat cohesive sheets – Multinucleated ciliated cells






Benign cellular Benign cellular proliferationsproliferations
• Creola body– Bronchial cell hyperplasia
• Goblet cell hyperplasia– Mucin vacuoles with small nuclei
• Reserved cell– Basal cells with molded nuclei






Noncellular Noncellular componentscomponents
• Corpora amylacea: noncalcified concretions
• Psammoma bodies• Ferruginous bodies• Charcot-Layden crystals• Curschmann spirals• Contaminants: pollen, food





Nonneoplastic lung Nonneoplastic lung diseasedisease
• Sarcoidosis– Granulomatous inflammation of lung
parenchyma with hilar/mediastinal node involement
– FNA diagnosis– Diagnosis includes typical features of
nonnecrotizing granuloma and exclusion of specific infectious etiology
– Culture and special stains needed

Noneoplastic lung Noneoplastic lung diseasedisease
• Pulmonary alveolar proteinosis– BAL diagnosis
• Gross: cloudy/milky white with graular debris
– Paucicellular sample of mononuclear inflammatory cells
– Amorphous basophilic granular debris– D/Dx: Pneumocystosis, Nocardia,
amyloidosis

Hemosiderin pigments in alveolar macrophages (PAP)


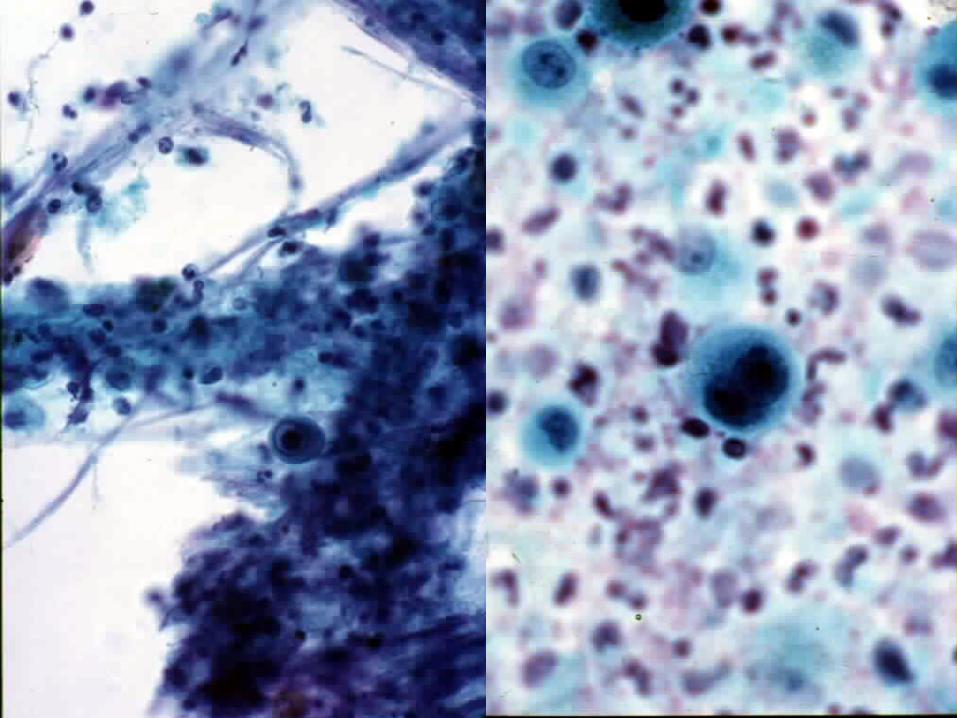
Pulmonary InfectionPulmonary Infection
• Viral infection– BAL diagnosis– Cilicytophthoria: detachment of cilia
• Adenovirus infection
– Reactive epithelial atypia– Specific viral inclusions