Bariatric Surgery in Pediatrics - Is it Time?
14
© Freund Publishing House Ltd., London Journal of Pediatric Endocrinology & Metabolism, 20, 751-761 (2007) Bariatric Surgery in Pediatrics - Is it Time? Manoel Carlos Prieto Velhote 1 , Durval Damiani 2 and Sergio Santoro 3 1 Pediatric Surgery and 2 Pediatric Endocrinology Unit, Instituto da Criança, Hospital das Clínicas, São Paulo University Medical School and 3 Hospital Israelita Albert Einstein, São Paulo, Brazil ABSTRACT In view of the increasing prevalence of obesity all over the world, we have seen morbid obesity occurring at earlier ages, and especially in adolescents. The first and main approach has been a conservative one, including change of lifestyle - implying better feeding habits and physical activity. However, our weapons to deal with this ‘pandemic of obesity’ have not solved a large number of cases, and we have to admit that bariatric surgery should be contemplated in special cases. Many different approaches have been devised by bariatric surgeons and although the complications over the short- and long-term are high and potentially severe, in some cases it is the only approach that has the potential to put the patient back to a more ‘normal’ metabolic situation with a significant weight loss. We discuss the main surgical approaches for morbid obesity and we comment on the pros and cons of each of them. KEY WORDS obesity, overweight, metabolic syndrome, bariatric surgery, leptin, hyperinsulinemia, GLP-1, adoles- cents INTRODUCTION The world is gaining weight, and very few countries have been spared from this ‘pandemic’ of obesity with all its implications. The efforts to curb this epidemic have not been very successful, and much is still unknown about the roots and the origins of the problem. Quoting Rosenbaum and Liebel 1 : “Obesity is a complex phenotype that resolves the influence of genes, development and environment”, and so it must be understood. Since genes in the population are stable to act in the remaining factors, a behavioral change is urgently needed, and educa- tion of our children and adolescents is essential to make a leaner world in the future. Although obesity has to be clinically treated and efforts for its prevention must be made, including feeding habits, physical activity and support 2 , in the present state of our knowledge extreme obesity is a condition in which only surgical approaches may have good results in the long run 3,4 . In the USA, the growing epidemic of obesity is a reality, it has been noticed for decades 5 , and has been growing even in children and adolescents, spreading out now to other developed and under- developed countries 6 . In the last decades, the lack of response to measures intending to avoid a world explosion of obesity is a strong sign of the failure of the proposed therapies to curb the problem. Among adults, a surgical approach is the first- choice therapy for the extremely obese 3 . Bariatric surgery has shown a huge growth in recent years (103,000 operations were performed in 2003 in the USA), and the number of associates of the Ameri- can Society for Bariatric Surgery (ASBS) has increased from 258 surgeons in 1998 to 1,070 in 2003 7 . In children, there has always been a resistance to accept this modality of treatment, mainly due to concerns about the risks of surgery 8 and about growth and psychological disturbances. Reprint address: Manoel Carlos Prieto Velhote Rua São Firmo 81 CEP-05454-060-SP Brazil e-mail: [email protected] VOLUME 20, NO. 7, 2007 751
description
Transcript of Bariatric Surgery in Pediatrics - Is it Time?

© Freund Publishing House Ltd., London Journal of Pediatric Endocrinology & Metabolism, 20, 751-761 (2007)
Bariatric Surgery in Pediatrics - Is it Time? Manoel Carlos Prieto Velhote1, Durval Damiani2 and Sergio Santoro3
1Pediatric Surgery and 2Pediatric Endocrinology Unit, Instituto da Criança, Hospital das Clínicas, São Paulo University Medical School and 3Hospital Israelita Albert Einstein, São Paulo, Brazil
ABSTRACT
In view of the increasing prevalence of obesity all over the world, we have seen morbid obesity occurring at earlier ages, and especially in adolescents. The first and main approach has been a conservative one, including change of lifestyle - implying better feeding habits and physical activity. However, our weapons to deal with this ‘pandemic of obesity’ have not solved a large number of cases, and we have to admit that bariatric surgery should be contemplated in special cases. Many different approaches have been devised by bariatric surgeons and although the complications over the short- and long-term are high and potentially severe, in some cases it is the only approach that has the potential to put the patient back to a more ‘normal’ metabolic situation with a significant weight loss. We discuss the main surgical approaches for morbid obesity and we comment on the pros and cons of each of them.
KEY WORDS
obesity, overweight, metabolic syndrome, bariatric surgery, leptin, hyperinsulinemia, GLP-1, adoles-cents
INTRODUCTION
The world is gaining weight, and very few countries have been spared from this ‘pandemic’ of obesity with all its implications. The efforts to curb this epidemic have not been very successful, and much is still unknown about the roots and the origins of the problem. Quoting Rosenbaum and Liebel1: “Obesity is a complex phenotype that resolves the influence of genes, development and environment”, and so it must be understood. Since genes in the population are stable to act in the remaining factors, a behavioral change is urgently needed, and educa-tion of our children and adolescents is essential to make a leaner world in the future. Although obesity has to be clinically treated and efforts for its prevention must be made, including feeding habits, physical activity and support2, in the present state of our knowledge extreme obesity is a condition in which only surgical approaches may have good results in the long run3,4. In the USA, the growing epidemic of obesity is a reality, it has been noticed for decades5, and has been growing even in children and adolescents, spreading out now to other developed and under-developed countries6. In the last decades, the lack of response to measures intending to avoid a world explosion of obesity is a strong sign of the failure of the proposed therapies to curb the problem. Among adults, a surgical approach is the first-choice therapy for the extremely obese3. Bariatric surgery has shown a huge growth in recent years (103,000 operations were performed in 2003 in the USA), and the number of associates of the Ameri-can Society for Bariatric Surgery (ASBS) has increased from 258 surgeons in 1998 to 1,070 in 20037. In children, there has always been a resistance to accept this modality of treatment, mainly due to concerns about the risks of surgery8 and about growth and psychological disturbances.
Reprint address: Manoel Carlos Prieto Velhote Rua São Firmo 81 CEP-05454-060-SP Brazil e-mail: [email protected]
VOLUME 20, NO. 7, 2007 751

752 M.C.P. VELHOTE ET AL.
As in adults, however, these children are prone to develop metabolic consequences, as well as physical and social constraints which imply a poor quality of life and low survival. Obese children, like adults, may have insulin resistance and type 2 diabetes mellitus, high blood pressure, dyslipidemia, orthopedic problems, sleep apnea, hepatic steatosis, cholecystopathy, poly-cystic ovary syndrome with hyperandrogenism, menstrual irregularities and even infertility, cere-bral pseudo-tumor, alveolar hypoventilation, skin problems, besides low self-esteem and social isolation9. Due to refractoriness to clinical treatment and the severity of the associated co-morbidities, the surgical approach in obese adolescents has gained more and more adepts10. This attitude makes sense in view of the poor results even in very well structured clinical groups in which patient compliance is high11 as opposed to the initial good results of bariatric surgery12.
EVALUATION OF THE DEGREE OF OBESITY WITH THE AIM OF SURGERY
Body mass index (BMI) calculated by the quotient of the weight by the height squared has been extensively used in adults to evaluate the degree of obesity. As shown in Table 1, it is possible to classify individuals according to BMI13.
TABLE 1
Classification of individuals based on body mass index (BMI)
BMI (kg/m2) Classification
18-25 Normal
25-30 Overweight
30 -35 Moderately obese
35-40 Intensely obese
40-50 Extremely obese
50-60 Super-obese
Above 60 Super-super-obese
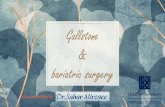
In children, due to the variability of BMI with regard to sex and age, we have to evaluate the degree of obesity by comparing the BMI using population charts14 (Fig. 1). The definition of over-weight is BMI between the 85th and 95th per-centiles, while obesity is defined as BMI above the 95th percentile. In these charts, there is no recog-nition of extreme obesity and super-obesity. From a practical point of view, we can say that for an adolescent who has completed at least 80% of his/her bone maturation, it is adequate to use the same parameters as in adults. However, when we pay attention to the distribution of the population BMI curves, we can see that in adolescents younger than 18 years of age the BMIs that define obesity and overweight are lower than in adults. Especially in 4-6 year-old children, a BMI of 18 is the limit for obesity and not a BMI of 30 as used for adults.
INDICATIONS FOR BARIATRIC SURGERY
In adults, there has been a consensus for more than 15 years that whenever BMI is greater than 35 with co-morbidities and above 40 even without co-morbidities this is an indication for surgery3. In children, cure of extreme exogenous obesity is extremely difficult, if not impossible, employing conventional clinical strategies. The best results with behavioral, dietetic, and clinical approaches in the long run (5-10 years) show that only 30% reach stability or some degree of improvement15. Those children who do not improve with clinical therapy may, with time, develop co-morbidities that shorten life expectancy and compromise physical and psychological status16, and will be obese adults. The American Pediatric Surgical Association (APSA) accepted the recommendation for surgery in girls older than 13 years and boys older than 15 years when BMI is greater than 40 with co-morbidities and above 50 as an isolated index17. Many authors state that, due to the failure of behavioral therapy in these highly obese patients, the benefit of surgery must be offered to children, using at least the same parameters as in adults12,18-24. Since good results have been obtained in adolescents submitted to bariatric surgery, there is no point in being more stringent in terms of indications for surgery or even postponing surgery
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM

BARIATRIC SURGERY IN PEDIATRICS 753
FIG 1
VOLUME 20, NO. 7, 2007

754 M.C.P. VELHOTE ET AL.
to an age greater than 18 years, since BMI will have increased even more. The risk of waiting for surgery till adult age is probably small, but the natural history of obesity indicates that it keeps on deteriorating9. This increases the surgical risks, and worsens self-esteem and social behavior, which may leave permanent psychological scars4. On the other hand, the sooner the orthopedic lesions, diabetes mellitus, and hypertension are stabilized or cured, the better the surgical results. Recent reports have been more liberal in the indications for surgery (younger patients, with smaller BMIs) using the same parameters as in adults (BMI >40 or BMI >35 with co-morbi-dities)18,20,25. Even in adults, there has been a tendency of being more flexible in individual cases, accepting for surgery patients with smaller BMIs26. This strategy takes into account the fact that higher risks of surgical complications are associated with late surgical indication, high BMI, and longer time suffering from diabetes mellitus or hypertension27. As new data in adolescents have demonstrated good results in the long run, low complication indices, and low morbidity and mortality, the acceptance of bariatric surgery has increased for extremely obese adolescents and even in the not-so-obese.
RATIONALE OF THE SURGICAL TECHNIQUES
The first trials to treat obesity with surgery date back to the 1950s. To create malabsorption, an internal jejuno-ileal bypass was performed by Kremen et al. in 195428. Although the weight loss was considerable, the maintenance of a normal gastric reservoir, profuse diarrhea with intense undernutrition, deficient calcium, vitamins B12, A, and D absorption, cholelithiasis and renal stones, precluded carrying on with this form of surgery. Observing the weight loss in patients submitted to gastrectomy, Mason and Ito in 1967 proposed gastric septation as a surgical procedure to treat obesity29. This pioneer technique branched into different approaches with the aim of creating a tiny gastric reservoir. The restrictive approach leads to difficulty in ingestion through the creation of a small gastric camera with a slow emptying outlet. The most used are adjustable gastric banding
(LAGB) and gastric bypass with Roux-en-Y reconstruction, devised by Fobi-Capella (RYGBP) In the USA, LAGB was only approved by the FDA in 2001, and this is the reason why the longer follow-up studies are European. It consists of laparoscopic placement of a silicon band, which is adjusted in the region of the cardia, keeping the gastric capacity above the band, at around 20 ml. The degree of compression of the band is adjusted in the post-operative period through the injection of saline into the subcutaneous reservoir, under radio-scopic control (Fig. 2B). This method has many advantages, being easily and quickly placed, keeps the patient in the hospital for a short time, has low indices of complications, and is totally reversible. The first reports used vertical-banded gastrec-tomy (VBG) (Fig. 2A), later replaced by the RYGBP, today the most often performed surgery for obesity all over the world, including the USA. From 1993, RYGBP began to be performed laparoscopically, with transection of the stomach close to the cardia, creating a gastric chamber with capacity around 25 ml. The remaining part of the stomach is left in the abdominal cavity. A Roux-en-Y loop in the jejunum is created, just after the Treitz angle, whose length goes from 100 to 150 cm, anastomosed to the gastric remnant (Fig. 2D). Disabsorptive techniques decrease the intestinal absorptive area, preventing the meal running through the whole digestive tract, since there is an internal bypass. The pattern of this surgery is the bilio-pancreatic bypass (BPD) by Scopinaro with or without duodenal switch. It consists of transverse gastrectomy with reconstruction in Roux-en-Y which keeps 50-100 cm of ileal loop with digestive enzymes (Fig. 2C). This technique has not usually been performed in children due to severe long-term complications (proteic-caloric malabsorption, bacterial overgrowth in the blind loop, the need to supplement vitamins, and the need for close medical follow-up for life)13. Recently, a new protocol has been proposed for modulated surgery which may also be used in pediatric patients. It is neither disabsorptive nor does it use obstructive devices, and aims at reactivating entero-hormones in the postprandial period, leading to early satiety. It has been named ‘digestive adaptation with intestinal reserve’
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM

BARIATRIC SURGERY IN PEDIATRICS 755
FIG 2 (DAIR), and consists of vertical gastrectomy, omentectomy and reduction of the small intestine to 3 meters (40 cm of jejunum and 260 cm of ileum). At its simplest it consists only of vertical gastrectomy (sleeve gastrectomy), a procedure suggested for super-obese or pre-adolescents. At the other extreme the reconstruction of the bowel is in Roux-en-Y gastroileal anastomosis, depicted in Figure 2E, keeping the pylorus and leaving the duodenum and 120 cm of small bowel in transit30,31. The modern diet, processed and easy to obtain, hypercaloric, and easy digestible in the proximal intestine, does not stimulate the terminal ileum to produce the entero-hormones (glucagon-like peptide 1 [GLP-1], PYY, and oxyntomodulin) implicated, among many different and interesting actions, in satiety and in the activation of an adequate insulin response to ingestion of food. In addition, the
satiety sensation is also obtained quickly after full
VOLUME 20, NO. 7, 2007

756 M.C.P. VELHOTE ET AL.
repletion of the stomach with small amounts of food. This technique takes into consideration all these factors. Vertical gastrectomy and entero-omentectomy are performed, and promising results have been shown, although the time of follow-up is up to 4 years in the oldest patient. The gastrectomy reduces the gastric capacity to around 200 ml, adapting the chamber size to the high caloric density of modern food, and diminishing ghrelin production, involved in the hunger sensation in fasting periods. The enterectomy allows the nutrients to reach the ileum, increasing the secretion of GLP-1 and PYY (leading to early satiety and higher and faster insulin secretion - the incretin effect). The removal of the epiplon reduces the dangerous visceral fat, an important factor in triggering metabolic syndrome, decreasing a source of IL-6, IL-8, TNF-α, and resistin, with reduction of insulin resistance in the liver32.
BARIATRIC SURGERY IN CHILDREN AND ADOLESCENTS
Bariatric surgery is far from being a cosmetic procedure. It is an extensive surgery, performed in patients with high surgical risk and with mortality7. The option of the surgical approach in adoles-cents has always faced strong opposition2,6 but the data are accumulating on the procedure and new techniques have been devised to try to solve or attenuate a very serious health problem with less risk to the patients. The first reports on adolescents submitted to bariatric surgery date back to 1985 by Silber, employing the gastric-ileal bypass technique. Although the weight loss is still significant after 10 years of follow-up, this technique has been abandoned due to high indices of severe complications (encephalo-pathy, nephrolithiasis, hypoproteinemia, cortical nephropathy, hepatopathy, etc.) and the need for frequent revisions. Since then, different modalities of surgery have revolutionized obesity surgery in adults due to much fewer complications and mortality. At the end of the 1990s, although recognizing the risks of infantile obesity, bariatric surgery for adolescents was not recommended, except in extreme cases, due to the risks of the procedure11,33. These restrictions have not been endorsed by other groups working with children who, although utilizing low number of patients, had low indices of complications and good results with regard to weight loss and patient satisfaction21-23,34,35. More recent data from adolescents confirm the good results with RYGBP18,25,37-39, placing this modality of surgery as an acceptable tool to deal with extreme obesity in adolescents. In 2005, a review of members of the ASBS revealed that 53% had already performed some surgical procedure in obese adolescents, 70% planned to start a regular program of surgery in adolescents, and 84% were interested in partici-pating in multicenter studies in this area. This demonstrates an increasing interest in bariatric surgery in pediatrics and forecasts its more disseminated utilization in the future40. Apovian et al. in 200541, in a study on evidence-based medicine, emphasizes the need for more research with regard to indications and long-term
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM

BARIATRIC SURGERY IN PEDIATRICS 757
results of bariatric surgery, and recognizes that the techniques applicable to adolescents are RYGBP and LAGB.
Laparoscopic adjustable gastric banding (Fig. 2B)
Adjustable silicon banding (LAGB), created in 1990, has been extensively used in Europe18-20,39. This procedure was only approved in the USA in 2001, which makes the European experience more extensive. In adults, the long-term European and Australian results have been very good: decrease in co-morbidities, absence of malabsorption, persis-tent weight loss, with decreased mortality and low complication indices. However, the weight loss is slower and less intense than with RYGBP13. Compared to RYGBP, LAGB has five-fold less mortality and much fewer complications, which make this procedure preferred over gastric bypass13. It has the advantage of being reversible and preserves the gastrointestinal physiology and anatomy39, and does not lead to malabsorption. The weight loss of 33% of the excess in the first 6 months, and 58% in the first year, caused BMI to fall from 44.7 kg/m2 in the pre-operative period to 30.2 kg/m2 in 2 years19. Therapeutic failures occurred in 2-3% of cases18,39. The indices of satisfaction and self-esteem in the post-operative period are improved, although the resolution of co-morbidities is lower than with RYGBP (67%)39. Surgical complications are few24,39, including gastric erosion with migration of the band18, wrong positioning of the band which requires re-operation18,20, no weight loss18 and secondary megaesophagus. It has been shown recently that gastric banding negatively interferes with esophagic motility42. The biggest criticism of this procedure is that the weight loss comes from an iatrogenic sub-esophagical gastric stenosis, caused by a foreign body. The patient may cheat weight loss by imbibing caloric fluids since the procedure does not lead to dumping.
Roux-en-Y gastric bypass (Fig. 2D)
Until 2004, there were 171 adolescent patients reported in the medical literature submitted to this modality of bariatric surgery12,21-25,34-38. The reports
emphasize the importance of referral centers that follow well-designed protocols to allow for com-parisons, since the total number of patients is small13. Analyzing the existing data, the initial results are uniformly good with 33% of weight loss up to the 6th month, 47% up to one year, and 53% up to 2 years of follow-up37. There was a good resolution of co-morbidities, such as diabetes mellitus, hypertension, and sleep apnea12,22,37, as well as improvement in self-esteem and social life36,38. On the other hand, some patients deve-loped cholelithiasis12,22,23,25 and needed surgery (laparoscopic in the majority of cases). This modality of surgery, to be effective in the long run, needs the maintenance of a small gastric chamber, with slow emptying (calibrated anastomosis). Vomiting is frequent when the ingested volume surpasses the gastric capacity, or when there is stenosis in the anastomosis. The com-plications directly related to the procedure are less than 5%, including deficiencies of vitamins D, BB1, B12 and A , as well as micronutrients, especially iron and calcium . Other complica-tions include dehiscent stitches in the remaining stomach , suppuration of the abdominal wall , incisional hernia , stenosis of the anastomosis, deep venous thrombosis , and occlusive scars . Four patients died some time after surgery and these deaths were not directly related to the surgical procedure . After 5 years, however, some patients started gaining weight , and some of them were submitted to another surgery to further reduce the gastric chamber .
22,25,43
22,36
37 38
22,38
37,38 22,38
23,38
38
25
Many patients got pregnant after the bariatric surgery and the pregnancy ran normally22. The main criticisms of the procedure are: it creates an intestinal bypass, leading to malabsorp-tion of nutrients that have exclusive proximal absorption. It does not allow gastric digestion, and potentially, changes the intestinal flora, due to the lack of gastric acid. The stomach itself stays isolated and is not accessible to endoscopic examination, in case this should be a necessary procedure. The ingestion of hyperosmolar meals leads to dumping.
VOLUME 20, NO. 7, 2007

758 M.C.P. VELHOTE ET AL.
Digestive adaptation with intestinal reserve (Fig. 2E)
This technique consists of vertical laparoscopic gastrectomy, preserving the antrum, followed by a small abdominal incision to complete the procedure with a resection of the greater epiplon and part of the small intestine, leaving 40 cm of jejunum and 260 cm of ileum30, as illustrated in Figure 2E. The advantages of this procedure are many: it does not use a prosthesis, and there are no areas excluded from the intestinal transit. The duodenum is kept on transit. There are no detectable signals of malabsorption, no diarrhea, no vomiting, and it allows the digestion of vitamins and oligonutrients. It gives early satiety and an outstanding improve-ment in insulin resistance, blood pressure and dyslipidimia31. Some bariatric surgeons criticize the enterec-tomy performed in this procedure but this is part of the adaptation of a long intestine to the kind of nutrients available in the modern diet, which seem to be insufficient for the proper stimulation of entero-hormones which produce a feeling of satiety. In a series of 12 adolescents, seven have been followed for 2 years. The mean BMI fell from 54 to 30, and there was a complete reversion of co-morbidities: five patients presented insulin resis-tance which normalized, four hypertensive patients normalized their blood pressure, and two dys-lipidemic patients normalized their serum lipids. One of our patients presented transitory peripheral polyneuropathy, which regressed with temporary vitamin B1 supplementation.
Laparoscopic sleeve gastrectomy (Fig. 2F)
In adult surgery, performing only a vertical gastrectomy (also known as laparoscopic sleeve gastrectomy [LSG]) in the super-super-obese patient is nowadays accepted as a first stage procedure to reduce weight with simpler laparo-scopic surgery44. It is not intended to completely correct the excess weight, but it has the advantage of producing a reduction of 45 kg after 6 months, with low surgical risk. This procedure improves health conditions in preparation for a second surgical stage45. Mognol et al.46 suggested that laparoscopic LSG can be used in bariatric surgery either as an isolated procedure, or as the first step
to a second procedure (DPB or RYGBP). We think that in children, LSG could have two indications: in prepubertal children with BMI >50 refractory to clinical therapy, and in Prader-Willi syndrome. Since it does not affect nutrition and meal absorption at all, it is presumed not to impair children’s growth, while it provokes consistent weight reduction. A 12 year-old child of 164 kg (BMI 58), obese from 3 years of age, with progressive increase in weight, underwent LSG. After 1.5 year, he lost 52 kg and had a BMI of 42. His growth during this year has been unimpaired and he is asymptomatic (personal communication). There are few reports on performing bariatric surgery with success in Prader-Willi syndrome. RYGBP and BPD have been used in children with Prader-Willi syndrome with variable results47-49. The rationale to use LSG in Prader-Willi syndrome rests on the knowledge that it is the only situation in obesity where basal blood levels of ghrelin are elevated. Gastrectomy, by reducing the bulk of the site of production, promotes a sustained reduction of ghrelin levels50 and could be useful as an endocrine-restrictive based surgery. It has already been performed in three patients (BMI 66, 65 and 50) with good control of feeding compulsion and initial weight loss (33, 80 and 21 kg 2 years, 1 year and 8 months after LSG, respectively). The blood ghrelin levels showed a significant reduction (per-sonal communication).
SELECTION OF PATIENTS
The following conditions must be taken into account for bariatric surgery in children and adolescents: • Exogenous obesity; • Multidisciplinary team evaluation of patients
who do not show satisfactory results after a 1-year period of treatment;
• Age >13 years in girls and >15 years in boys; • Patients who reached 80% of his/her adult
stature or the equivalent bone age; • BMI >40 or BMI >35 with co-morbidities; • Understanding and acceptance of the surgical
procedure and its consequences;
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM

BARIATRIC SURGERY IN PEDIATRICS 759
• Psychological evaluation attesting that the patient has emotional conditions to withstand the procedure;
• To agree in participating in follow-up visits as well as following nutritional orientation;
• The surgery has to be performed in a reference center, structured to provide a comprehensive approach to the patient, with well trained surgeons and a good system of data collection;
• The approach has to be individualized and has to take into account all the indications and limitations of the whole process13,18;
• Informed consent given by parents or guardians.
THE IMPROVEMENT OF CO-MORBIDITIES LINKED TO EXTREME OBESITY
The association of obesity with morbidities, such as metabolic syndrome, with dyslipidimia, hyperinsulinemia, and systemic hypertension, is well known51. Even before weight loss, some complications associated with obesity disappear or decrease in intensity. RYGBP and DAIR tend to correct the carbohydrate disturbances, and this improvement has been attributed to the increase in GLP-1, secreted by the L-cells of the terminal ileum once there are nutrients in the lumen of this portion of the intestine. Although this improvement also occurs, less intensely, with LAGB, besides weight loss the mechanisms involved are not yet clear. With weight loss, whatever the therapeutic modality employed, surgical or not, there is improvement of sleep apnea, hepatic steatosis, and joint problems, and in particular there is good improvement in social life and self esteem.
CONCLUSIONS
Clinical treatment of obesity, always the first step in the approach to this complex metabolic condition, has faced problems in solving the most severe cases, especially in the young. In this context, in selected cases, the possibility of submitting the patient to a surgical procedure has to be taken into account2, since it has been shown to
be an approach that effectively leads to maintained weight loss with acceptable surgical risk. All the modalities of bariatric surgery have shown much better results, in terms of weight loss, when compared to more conservative approaches. The procedures, although invasive, have demon-strated that they diminish co-morbidities, and carry a low risk and a low rate of complications. The best modality of surgery and the best time for it to be performed still depend on studies with a high number of pediatric patients and long-term follow-up. As the number of cases increases, there has been a tendency to indicate surgery at younger ages and with less severe degrees of obesity4,12,13,18,26,27. The initial criteria in the phase of acquisition of experience with this procedure have to be more rigid, but the number of patients operated upon until now allows us to see the procedure as a useful tool in extremely obese patients27, even at young age. Once the procedure has been proven to be safe and effective, we can have indications before the deleterious metabolic consequences of the obesity take place, since they increase surgical morbidity and mortality. The sustained improvement of conditions, such as insulin resistance, sleep apnea and hypertension, has to be taken into account in the indication of the procedure. The acknowledgment that obesity is more than an esthetic problem, but a disease with a very complex set of metabolic disturbances that poses serious risks to health and quality of life, induces us to regard surgical and more aggressive modalities of therapy as possible actions to be taken to circumvent the disturbances created by obesity. The procedure has a clear cost-benefit relationship, since reducing obesity dramatically decreases the later costs of complications in the medium- and long-term. However, in future generations, with new approaches to health care51, we hope that surgery for obese children, that today looks like being the future, will become outdated.
REFERENCES
1. Rosenbaum M, Leibel RL. The physiology of body weight regulation: the relevance to the etiology of
VOLUME 20, NO. 7, 2007

760 M.C.P. VELHOTE ET AL.
obesity in children. Pediatrics 1998; 101 (Suppl): 525-539.
2. Barlow SE, Dietz WH. Obesity evaluation and treat-ment. Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Adminstration and the Department of Health and Human Services. Pediatrics 1998; 102: e29.
3. National Institutes of Health Consensus Development Conference. Gastrointestinal surgery for severe obesity: Proceedings of a National Institutes of Health Consensus Development Conference, March 25-27, 1991, Bethesda, MD. Am J Clin Nutr 1992; 55 (Suppl): 487S-619S.
4. Garcia VF, deMaria EJ. Adolescent bariatric surgery: treatment delayed, treatment denied, a crisis invited. Obes Surg 2006; 16: 1-4.
5. Troiano RP, Flegal KM. Overweight children and adolescents: description, epidemiology and demo-graphics. Pediatrics 1998; 101 (Suppl): 497-504.
6. Dietz WH. Childhood obesity: susceptibility, cause and management. J Pediatrics 1983; 103: 676-686.
7. Steinbrooke R. Surgery for severe obesity. N Eng J Med 2004; 350: 1075-1079.
8. Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet 2002; 360: 473-482.
9. Must A, Strauss RS. Risk and consequences of child-hood and adolescent obesity. Int J Obes 1999; 23 (Suppl 2): S2-S11.
10. Kirk S, Scott BJ, Daniels SR. Pediatric obesity epidemic: treatment options. J Am Diet Assoc 2005; 105 (Suppl): S44-51.
11. Epstein LH, Myers MD, Raynor HA, Saelens BE. Treatment of pediatric obesity. Pediatrics 1998; 101 (Suppl): 554-569.
12. Capella JF, Capella RF. Bariatric surgery in adoles-cence. Is this the best age to operate? Obes Surg 2003; 13: 826-832.
13. Inge TH, Zeller MH, Lawson L, Daniels SR. A critical appraisal of evidence supporting a bariatric surgical approach to weight management for adolescents. J Pediatrics 2005; 147: 10-19.
14. Growth Charts developed by the National Center for Health Statistics in collaboration with the National Center for Chronic Disease Prevention and Health Promotion (2000). http://www.cdc.gov/growthcharts.
15. Epstein LH, Valoski A, Wing R, McCurley J. Ten-year follow-up of behavioral family-based treatment for obese children. JAMA 1990; 264: 2519-2523.
16. Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics 1998; 101 (Suppl): 518-525.
17. Rodgers BM. Bariatric surgery for adolescents: a view from the American Pediatric Surgical Association. Pediatrics 2004; 114: 255-256.
18. Angrisani L, Favretti F, Furbetta F, Paganelli M, Basso N, Doldi SB, Iuppa A, Lucchese M, Lattuada E, Lesti
G, Capizzi FD, Giardiello C, Di Lorenzo N, Veneziani A, Alkilani M, Puglisi F, Gardinazzi A, Cascardo A, Borrelli V, Lorenzo M. Obese teenagers treated by Lap-Band system: the Italian experience. Surgery 2005; 138: 877-881.
19. Dolan K, Creighton L, Hopkins G, Fielding G. Laparo-scopic gastric banding in morbidly obese adolescents. Obes Surg 2003; 13: 101-104.
20. Yitzhak A, Mizrahi S, Avinoach E. Laparoscopic gastric banding in adolescents. Obes Surg 2006; 16: 1318-1322.
21. Greenstein RJ, Rabner JG. Is adolescent gastric-restrictive antiobesity surgery warranted? Obes Surg. 1995; 5: 138-144.
22. Strauss RS, Bradley LJ, Brolin RE. Gastric bypass surgery in adolescents with morbid obesity. J Pediatr 2001; 138: 499-504.
23. Breaux CW. Obesity surgery in children. Obes Surg 1995; 5: 279-284.
24. Abu-Abeid S, Gavert N, Klausner JM, Szold A. Bariatric surgery in adolescence. J Pediatr Surg 2003; 38: 1379-1382.
25. Stanford A, Glascock JM, Eid GM, Kane T, Ford HR, Ikramuddin S, Schauer P. Laparoscopic Roux-en-Y gastric bypass in morbidly obese adolescents. J Pediatr Surg 2003; 38: 430-433.
26. Fobi M, Lee H, Igwe D, Felahy B, James E, Stanczyk M, Fobi N. Gastric bypass in patients with BMI < 40 but > 32 without life-threatening co-morbidities: pre-liminary report. Obes Surg 2002; 12: 52-56.
27. Garcia VF. Adolescent bariatric surgery: treatment delayed may be treatment denied [Letter]. Pediatrics 2005; 115: 822.
28. Kremen AJ, Linner JH, Nelson CH. An experimental evaluation of the nutritional importance of proximal and distal small intestine. Ann Surg 1954; 140: 439-448.
29. Mason EE, Ito C. Gastric bypass in obesity. Surg Clin North Am 1967; 47: 1345-1351.
30. Santoro S, Velhote MCP, Malzoni CE, et al. Prelimi-nary results of digestive adaptation: a new surgical proposal to treat obesity based on physiology and evolution. São Paulo Med J 2006; 124: 192-197.
31. Santoro S, Malzoni CE, Velhote MCP, Milleo FQ, Santo MA, Klajner S, Damiani D, Maksoud JG. Digestive adaptation with intestinal reserve: a neuro-endocrine-based operation for morbid obesity. Obes Surg 2006; 16: 1371-1379.
32. Drazen DL, Woods SC. Peripheral signals in the control of satiety and hunger. Curr Opin Clin Nutr Metab Care 2003; 6: 621-629.
33. Flodmark CE. Childhood obesity. Clin Child Psychol Psychiatry 1997; 2: 283-295.
34. Anderson AE, Soper RT, Scott DH. Gastric bypass for morbid obesity in children and adolescents. J Pediatr Surg 1980; 15: 876-881.
35. Soper RT, Mason EE, Printen KJ, Zellweger H. Gastric
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM

BARIATRIC SURGERY IN PEDIATRICS 761
45. Regan JP, Inabnet W, Gagner M, Pomp A. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg 2003; 13: 861-864.
bypass for morbid obesity in children and adolescents. J Pediatr Surg 1975; 10: 51-58.
36. Rand CS, Macgregor AM. Adolescents having obesity surgery: a 6-year follow-up. South Med J 1994; 87: 1208-1213. 46. Mognol P, Chosidow D, Marmuse JP. Laparoscopic
sleeve gastrectomy as an initial bariatric operation for high-risk patients: initial results in 10 patients. Obes Surg 2005; 15: 1030-1033.
37. Inge TH, Garcia VF, Daniels SR, Langford L, Kirk S, Roehrig H, Amin R, Zeller M, Higa K. A multi-disciplinary approach to the adolescent bariatric surgical patient. J Pediatr Surg 2004; 39: 442-447. 47. Papavramidis ST, Kotidis EV, Gamvros O. Prader-
Willi syndrome-associated obesity treated by bilio-pancreatic diversion with duodenal switch. Case report and literature review. J Pediatr Surg 2006; 41: 1153-1158.
38. Sugerman HJ, Sugerman EL, DeMaria EJ, Kellum JM, Kennedy C, Mowery Y, Wolfe LG. Bariatric surgery for severely obese adolescents. J Gastrointest Surg 2003; 7: 102-108.
48. Braghetto I, Rodriguez A, Debandi A, Brunet L, Papapietro K, Pineda P, Pacheco MI. Prader-Willi syndrome (PWS) associated to morbid obesity: surgical treatment [in Spanish]. Rev Med Chil 2003; 131: 427-431.
39. Silberhumer GR, Miller K, Kriwanek S, Widhalm K, Pump A, Prager G. Laparoscopic adjustable gastric banding in adolescents: the Austrian experience. Obes Surg 2006; 16: 1062-1067.
40. Allen SR, Lawson L, Garcia V, Inge TH. Attitudes of bariatric surgeons concerning adolescent surgery (ABS). Obes Surg 2005; 92-1195.
49. Dousei T, Miyata M, Izukura M, Harada T, Kitagawa T, Matsuda H. Long-term follow-up of gastroplasty in a patient with Prader-Willi syndrome. Obes Surg 1992; 2: 189-193.
41. Apovian CM, Baker C, Ludwig DS, Hoppin AG, Hsu G, Lenders C, Pratt IS, Forse RA, O’Brien A, Tarnoff M. Best practice guidelines in pediatric/adolescent weight loss surgery. Obes Res 2005; 13: 274-280.
50. Langer FB, Reza Hoda MA, Bohdjalian A, Felberbauer FX, Zacherl J, Wenzl E, Schindler K, Luger A, Ludvik B, Prager G. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg 2005; 15: 1024-1029.
42. Suter M, Dorta G, Giusti V, Calmes JM. Gastric band-ing interferes with esophageal motility and gastro-esophageal reflux. Arch Surg 2005; 140: 639-643.
43. Towbin A, Inge TH, Garcia VF, Roehrig HR, Clements RH, Harmon CM, Daniels SR. Beriberi after gastric bypass surgery in adolescence. J Pediatrics 2004; 145: 263-267.
51. Bitsori M, Kafatos A. Dysmetabolic syndrome in child-hood and adolescence. Acta Paediatr 2005; 94: 995-1005.
52. Barlow SE. Bariatric surgery in adolescents: for treat-ment failures or health care system failures? Pediatrics 2004; 114: 252-253.
44. Milone L, Strong V, Gagner M. Laparoscopic sleeve gastrectomy is superior to endoscopic intragastric balloon as a first stage procedure for super-obese patients (BMI >50). Obes Surg 2005; 15: 612-617.
VOLUME 20, NO. 7, 2007

762 M.C.P. VELHOTE ET AL.
Fig. 1: Body mass index (BMI) growth charts from 2 to 20 years of age, for males and females. National Center for Health Statistics14.
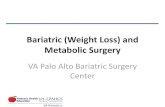
Fig. 2: Different modalities of bariatric surgery. VGB = vertical banded gastroplasty; LAGB = laparoscopic adjustable gastric banding; BPD = bilio-pancreatic diversion; RYGBP = Roux-en-Y gastric bypass; DAIR = digestive adaptation with intestinal reserve; LSG = laparoscopic sleeve gastrectomy.
Fig. 1: Body mass index (BMI) growth charts from 2 to 20 years of age, for males and females. National Center for Health Statistics14.
Fig. 2: Different modalities of bariatric surgery. VGB = vertical banded gastroplasty; LAGB = laparoscopic adjustable gastric banding; BPD = bilio-pancreatic diversion; RYGBP = Roux-en-Y gastric bypass; DAIR = digestive adaptation with intestinal reserve; LSG = laparoscopic sleeve gastrectomy.
JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM