Bariatric surgery as treatment of type 2 ... - DiVA portal
56
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2020 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1672 Bariatric surgery as treatment of type 2 diabetes – clinical and mechanistic aspects. PETROS KATSOGIANNOS ISSN 1651-6206 ISBN 978-91-513-0976-7 urn:nbn:se:uu:diva-416646
Transcript of Bariatric surgery as treatment of type 2 ... - DiVA portal

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1672
Bariatric surgery as treatmentof type 2 diabetes – clinical andmechanistic aspects.
PETROS KATSOGIANNOS
ISSN 1651-6206ISBN 978-91-513-0976-7urn:nbn:se:uu:diva-416646

Dissertation presented at Uppsala University to be publicly examined in Enghoffsalen, Ing.50, Akademiska Sjukhuset, Uppsala, Friday, 11 September 2020 at 13:00 for the degree ofDoctor of Philosophy (Faculty of Medicine). The examination will be conducted in English.Faculty examiner: PhD Daniel Andersson (Karolinska Institute Department of Medicine,Endocrinology and Diabetology.).
AbstractKatsogiannos, P. 2020. Bariatric surgery as treatment of type 2 diabetes – clinical andmechanistic aspects.. Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1672. 55 pp. Uppsala: Acta Universitatis Upsaliensis.ISBN 978-91-513-0976-7.
Bariatric surgery can rapidly improve glycemic control and cardiovascular risk factors inpatients with T2D and obesity. These improvements appear to be partly independent of weightloss, however, the underlying mechanisms remain incompletely understood. A randomizedcontrolled trial was designed where 19 patients with obesity and T2D were either operated witha Roux-en-Y gastric bypass (RYGB) operation or continued with standard-of-care treatmentand followed up for 2 years, providing the data for Paper I-III.
In paper I, we focused on changes in whole-body glucose metabolism in relation to changesin adipose tissue metabolism and morphology. We observed an early adipose tissue remodelingand a reduction in adipocyte size that however, did not correlate to the early improvements inmetabolic control.
In paper II, we analyzed the neuroendocrine changes after RYGB. We observed changeswithin 4 weeks with signs of enhanced parasympathetic outlow, reduced morning cortisol,and enhanced incretin and glucagon responses to glucose, suggesting that neurohormonalmechanisms can contribute to the rapid improvement of insulin resistance and glycemiafollowing RYGB in T2D.
In paper III the patients from the RYGB group were interviewed 2 years after surgery toexamine the effects of surgery on health-related quality of life (HRQoL). We found that theimproved HRQoL after RYGB was not explained specifically by the magnitude of weight loss,but rather by the participants achieving a state of union between body and consciousness.
In paper IV, we compared changes in circulating cytokine and adipokine levels in obesepatients with- and without T2D. We observed that the cytokine profile of these patients is alteredwhen compared to lean healthy control subjects and persist to a large extent after RYGB despitethe weight loss and improved metabolic status.
In conclusion, we observed that in the early post-operative period, neurohormonal changesappear to be more important than adipose tissue changes in improving insulin sensitivity andleading to diabetes remission.
In the qualitative part of our study, we observed that the improved HRQoL was not solelyexplained by weight loss
Keywords: Roux-en-y gastric bypass, Type 2 diabetes, incretins, cytokines, adipokines,adipose tissue, heart rate variability, quality of life.
Petros Katsogiannos, Department of Medical Sciences, Clinical diabetology and metabolism,Akademiska sjukhuset, Uppsala University, SE-75185 Uppsala, Sweden.
© Petros Katsogiannos 2020
ISSN 1651-6206ISBN 978-91-513-0976-7urn:nbn:se:uu:diva-416646 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-416646)

To Denia, Eleana and Dimitris

When you set out on your journey to Ithaca, pray that the road is long, full of adventure, full of knowledge. Konstantinos Kavafis

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I. Katsogiannos P, Kamble PG, Boersma GJ, Karlsson FA, Lundkvist P, Sundbom M, Pereira MJ, Eriksson JW. “Early changes in adipose tissue mor-phology, gene expression and metabolism after RYGB in patients with obesity and T2D.” J Clin Endocrinol Metab. 2019 Jul 1;104(7):2601-2613. II. Katsogiannos P*, Kamble PG*, Wiklund U, Sundbom M, Espes D, Ham-mar U, Karlsson FA, Pereira MJ, Eriksson JW. ”Rapid changes in neuroendo-crine regulation may contribute to reversal of type 2 diabetes after gastric by-pass surgery.” Endocrine. 2020 Feb;67(2):344-353. *These authors contributed equally III. Katsogiannnos P, Randell E., Sundbom M., Rosenblad A., Eriksson JW., Leksell J. “Quality of life after gastric bypass surgery in patients with type 2 diabetes: Patients’ experiences during 2 years of follow-up.” Submitted
IV. Katsogiannos P., Kamble PG., Pereira MJ.,Sundbom M., Carlsson PO., Erikson JW., Espes D. ” Changes in circulating cytokines and adipokines after gastric bypass surgery in patients with obesity with and without type 2 diabe-tes.” Submitted
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11 Obesity ...................................................................................................... 11 Type 2 Diabetes mellitus .......................................................................... 12 Adipose tissue ........................................................................................... 13
Background Bariatric Surgery ....................................................................... 14 Bariatric surgery as a treatment for obesity .............................................. 14 Mechanisms for T2D remission after RYGB ........................................... 15 Impact of bariatric surgery on quality of life ............................................ 17 Adverse effects of bariatric surgery .......................................................... 17
Aim ................................................................................................................ 18
Objectives ...................................................................................................... 19
Subjects and Study Design ............................................................................ 20
Methods ......................................................................................................... 22 Roux-En-Y Gastric Bypass surgery (Papers I-IV) ................................... 22 Biochemical Analyses (Papers I, II, IV) ................................................... 22 Heart rate variability analysis (Paper II) ................................................... 23 Intravenous Arginine Stimulation test (Paper II) ..................................... 23 Oral glucose tolerance test (OGTT) Paper I-II ......................................... 23 Adipose tissue biopsy (Paper I) ................................................................ 24 Glucose uptake in adipocytes (Paper I ) ................................................... 24 Lipolysis in adipocytes (Paper I ) ............................................................. 24 Adipocyte size (Paper I ) .......................................................................... 25 Gene expression analysis (paper I, II) ...................................................... 25 RAND SF-36 health questionnaire (Paper III) ......................................... 26 Qualitative interviews (Paper III) ............................................................. 26
Results ........................................................................................................... 27 Paper I ....................................................................................................... 27 Paper II ..................................................................................................... 29
Heart rate variability ............................................................................ 31 Paper III .................................................................................................... 32 Paper IV .................................................................................................... 32

Discussion ..................................................................................................... 34 Metabolic effects of RYGB: Tissue crosstalk and time course (paper I-II) .............................................................................................................. 34 Quality of Life (Paper III) ........................................................................ 37 Effects on inflammation: cytokines and adipokines (Paper IV) ............... 37
Conclusions ................................................................................................... 40
Svensk sammanfattning (Summary in Swedish) ........................................... 43
Acknowledgements ....................................................................................... 45
References ..................................................................................................... 48

Abbreviations
T2D, Type 2 diabetes RYGB, Roux-en-Y gastric bypass BMI, Body Mass Index LCD, Low-calorie diet SAT, Subcutaneous adipose tissue HRV, Heart Rate Variability measurements OGTT, Oral glucose tolerance test ANS, Autonomic Nervous System FFA, Free Fatty Acid GLP-1, Glucagon-like peptide-1 GIP, Glucose-dependent insulinotropic peptide/Gastric Inhibitory Peptide IGF-1, Insulin-like growth factor 1 GH, Growth hormone IGI, Insulinogenic Index HRQoL , Health-related Quality of Life HbA1c, Glycosylated haemoglobin HDL, High density lipoproteins LDL, Low density lipoproteins TNF-alpha, tumor-necrosis factor alpha IL-6, Interleukin 6 HGF, Hepatocyte growth factor Reg3A, islet-derived protein 3A BMP4, bone morphogenic protein-4


11
Introduction
Obesity The World Health Organization (WHO) has defined the term “obesity” as ex-cessive fat accumulation that is harmful to health. Considered the twenty-first-century epidemic, obesity is one of the leading health problems , reducing life expectancy, and presenting a challenge for the global economy. With more than 1.9 billion adults being overweight, and of these over 650 million being obese, this is a disease with exponential growth. Furthermore, the epidemic is affecting the younger population, with 38 million children under the age of 5 being overweight or obese in 2019. Obesity, defined as a Body mass index (BMI) higher than or equal to 30 kg/m2, is a chronic disease involving genetic, metabolic, psychological, and endocrinology-related factors, among others (1). The main cause of obesity is the long-term imbalance in energy consumption, excess calorie intake, and lower calorie expenditure. However, many other factors contribute to making this disease complex to understand and to treat (2). Ongoing research has im-proved our understanding of how the adipose tissue interplays with gut or liver hormones and how neural pathways in specific brain areas are also involved (4). Obesity-associated comorbidities are numerous and are also related to higher mortality. Obesity is recognized as a risk factor for various other chronic ill-nesses related to metabolic syndrome including type 2 diabetes mellitus (T2D), hypertension, dyslipidemia, cardiovascular diseases (CVD), respira-tory disorders, psychosocial problems, and even several types of cancer (in-cluding esophagus, colon, pancreas, prostate, and breast) (5). In the ongoing coronavirus pandemic, obesity has been recognized as a risk factor for greater COVID-19 severity (6).

12
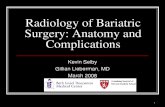
Type 2 Diabetes mellitus Type 2 diabetes mellitus (T2D) is characterized by hyperglycemia, insulin re-sistance, and relative impairment in insulin secretion. The pathophysiology of type 2 diabetes of diabetes is complex affecting multiple organs, as shown in figure 1 below (7).
Figure 1. Pathophysiology of type 2 diabetes (adapted from Pratley, American Jour-nal of Medicine 2013)
The pathogenesis of T2D is also influenced by genetic (8), intrauterine (9), or environmental factors (10), thus making it difficult to determine the exact cause in an individual patient. The incidence of T2D globally is growing parallel to obesity, urbanization, and a more pronounced sedentary lifestyle. It is widely recognized as one of the most challenging threats to public health (11). T2D and it´s chronic micro- and macrovascular complications have resulted in T2D being one of the lead-ing causes of premature morbidity and mortality (12). Lifestyle modification with diet and exercise is considered the first option for achieving weight control and is also the first option for better glycemic control (13). The reduction of microvascular and macrovascular complications of di-abetes has been a target of medical treatment (14). The latest pharmacological complements to the treatment of T2D namely in-cretin-based treatment and SGLT-2 inhibitors have also shown to affect

13
weight, while improving glycemic control and reducing complications of T2D (15-16) Despite improvements in pharmacotherapy, fewer than 50% of patients with moderate-to-severe type 2 diabetes achieve and maintain adequate thresholds for glycemic control (17).
Adipose tissue Adipose tissue was once considered as a storage organ for triacylglycerol; however, in the last decades, it's physiology, pathophysiology, it's role in the body, and it's interaction with other organs has been of considerable research interest. In mammals, there are two types of adipose tissue: white and brown and are comprised of adipocytes with different morphology and function. Brown adipose tissue is almost absent in adult humans but found at birth is involved in thermogenesis (18). Adipose tissue is no longer considered to be an inert tissue that just stores fat (19).
White adipose tissue is composed of adipocytes, and other cell types called the stroma-vascular fraction, comprising blood cells, endothelial cells, peri-cytes, and adipose precursor cells among others The multiple functions of white adipose tissue range from lipogenesis to lipolysis, involvement in glu-cose and metabolism, body weight homeostasis, appetite regulation, partici-pation as a secretory organ (20) with secreted adipokines such as leptin, adi-ponectin and also as a source of inflammatory cytokines, such as TNF-α and IL-6 (21). Research in this complex and extensive crosstalk involving adipokines, im-mune cells and cytokines has shown to be important in the obesity-associated inflammation and the development of insulin resistance (22). Furthermore, the sympathetic nervous system's involvement in obesity has given rise to this new field of neuroimmunometabolism (23).

14
Background Bariatric Surgery
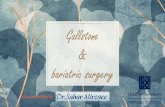
Bariatric surgery as a treatment for obesity Bariatric surgery is the most effective therapy with a long-lasting effect on severely obese patients. Weight loss and glycemic control are otherwise diffi-cult to maintain, despite intensive dietary and lifestyle modification as well as physical exercise and specialized psychological support, as demonstrated by studies such as the Look AHEAD (24). There are different effective surgical methods used for obesity treatment. The most commonly used bariatric procedures, such as Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy (SG), mini-gastric bypass, and biliopancreatic diversion (BPD) are considered safe procedures that are efficient regarding obesity-associated comorbidities and weight loss (25). In RYGB, the bypass-ing of the major part of the stomach and duodenum results in reduced food intake and various hormonal changes (Figure 2).
Figure 2. Roux-en-Y gastric bypass (RYGB)

15
Many observational studies, as well as clinical trials, have shown that bariatric surgery can rapidly improve glycemic control and decrease cardiovascular risk factors in severely obese patients with T2D (26-29). Hence the term “met-abolic surgery” is becoming increasingly popular in the past several years. These effects on glucose homeostasis appear to be partly independent of weight loss as they often occur earlier and without a clear correlation to the magnitude of weight loss (30). Despite the increasing use of bariatric surger-ies, the underlying mechanisms remain incompletely understood.
Mechanisms for T2D remission after RYGB Early and pronounced improvement in hepatic insulin sensitivity after RYGB, which could be related to caloric restriction in the short-term postoperative period and the reduction in intrahepatic fat, has been reported, as well as an improvement in peripheral insulin sensitivity, which occurs later. Its relation-ship with sustained weight loss has been previously described (31-32). Weight-independent glucose-lowering mechanisms of metabolic surgery have been studied thoroughly in animals and humans (33-34) and include 1) favor-able changes in gut hormones, 2) favorable changes in bile acid signaling, 3) increased glucose metabolism by the small intestine, 4) changes in intestinal nutrient sensing that improve insulin sensitivity, through both neural and hu-moral pathways, 5) reduced intestinal glucose transport via SGLT1, 6) de-creased circulating branched-chain amino acids and 7) possible alterations in gut microbiota (although evidence is more substantial for a role in weight loss than in improved glucose homeostasis) Neuroendocrine changes have also been suggested to be involved in the ben-eficial effects of metabolic surgery. Following RYGB, the most substantial change in gut hormones occurs post-prandially and includes glucagon-like peptide-1 (GLP-1) and peptide YY (PYY), which have been reported to in-crease by more than 10-fold (35-36). A modification of gastrointestinal hormone release has well-recognized ef-fects on food intake and energy equilibrium. Most of these hormones com-municate with the brain in an endocrine manner. They also act in a paracrine fashion by interacting with specific receptors located on vagal afferent nerve fibers that innervate the gastrointestinal tract and are close to gastrointestinal endocrine cells (37). Besides, vagal afferent endings also respond to mechan-ical stimuli such as distension (38). The nucleus tractus solitarius (NTS; vagal afferent nucleus) senses afferent inputs to regulate energy balance, including hunger and satiety feelings by the activation of brain regions involved in food intake regulation, as well as by vagal efferent inputs that regulate splanchnic

16
organs such as the liver and endocrine pancreas (39-40) . These pathways seem to be altered in obesity with vagal afferent over-activation, likely due to a decreased sensitivity to vagal afferents stimuli, which require higher stimuli to activate a proper response to feeding, leading to hyperphagia (39). Reversal of sympathetic activation by weight loss has been previously reported (41-43) The role of adipose tissue in the pathogenesis of type 2 diabetes has also been studied thoroughly (44). It is known from earlier studies that pronounced re-ductions in both visceral adipose tissue (VAT) and subcutaneous adipose tis-sue (45) occur within the first few months after surgery (46). One may thus hypothesize that the reduction in adipose tissue mass per se may contribute to the metabolic improvements following RYGB.
In contrast to this hypothesis, in a study performed by Klein et al. (47) a large amount of SAT removed by liposuction from obese patients did not result in metabolic improvement at short- or long-term follow-up. Furthermore, partial removal of VAT in connection with bariatric surgery did not induce additional metabolic improvements (48-50). This may suggest that the removal of adi-pose tissue alone is not sufficient to induce the metabolic improvement ob-served after RYGB. Andersson et al. (51) showed that marked weight reductions in patients post-RYGB were associated with a decrease in subcutaneous fat cell volume (but not a number), which was significantly associated with improvements in in-sulin sensitivity. Furthermore, this study confirmed earlier observations that decreased visceral, but not subcutaneous fat mass, correlated with improve-ments in metabolic risk factors, including insulin resistance and dyslipidemia. Thus it seems that the adipose tissue is involved in RYGB-induced improve-ments in metabolic function in patients with impaired glucose metabolism. However, it is not clear whether changes in adipose tissue occur before or after metabolic improvements. Most studies to date were performed on patients several months after they had undergone RYGB. Thus they cannot address the time course of RYGB-induced effects on whole-body insulin sensitivity and adipose tissue. Inflammation is a known complication of obesity that supports T2D develop-ment and differentiates metabolic healthy from metabolically unhealthy obe-sity (52). Previous studies have shown that various cytokines, adipokines, and chemokines are altered in obesity and T2D. However, the data on how these factors behave in non-diabetic patients with obesity compared to patients with T2D undergoing RYGB is poorly understood (53).

17
Impact of bariatric surgery on quality of life Besides having improvements in their metabolic status and weight, patients undergoing bariatric surgery have also been shown to have improvements in their quality of life. In the Swedish obese subjects (SOS) intervention study the patients that underwent surgery have shown a long-lasting weight reduc-tion as well as a general long-standing positive outcome on health-related quality of life (HRQoL) (54-55). There is evidence showing a relationship between HRQoL improvement and weight loss (56); however, this improvement cannot be explained by weight loss alone. Patients experience a marked improvement in HRQoL shortly after surgery before any significant weight loss can occur, suggesting that psycho-logical factors (57) contribute to improvement in HRQoL almost instantly. A recently published meta-analysis showed mixed results of HRQoL when comparing metabolic surgery with medical treatment among obese subjects with T2D. One shortcoming with the included studies is their heterogeneity when measuring HRQoL and treatment satisfaction (58). In general, metabolic surgery results in significant physical health improvements, while there are mixed results concerning mental health (59).
Adverse effects of bariatric surgery Although bariatric surgery has become a safe procedure (60), complications still exist. Leakage at one of the two anastomoses occurs in 1-2% (61) as well as thromboembolic complications (62). In the longer term, about 5% of all patients suffer from internal herniation, a type of small bowel obstruction due to entrapment behind the anastomoses (63). This condition requires prompt surgery.
Dumping syndrome, another common side effect after RYGB, is present in various degrees of severity in about 85% of RYGB patients (64). The patients are at risk of developing common vitamin and mineral deficiencies due to the mild fat and protein malabsorption which is present after the procedure (65). Furthermore, increased risk of alcohol abuse and chronic abdominal pain are reported (66).

18
Aim
The purpose of the present work is to explore the neurohormonal, adipose tis-sue, and inflammatory pathways and how the dynamics of these pathways change over time after RYGB. In addition, assessing the effect of RYGB on QoL and to examine how this correlates to the overall improvements in me-tabolism.

19
Objectives
Paper I To examine how early changes in adipose tissue morphology and metabolism after RYGB contribute to the rapid improvements in whole-body metabolism. Paper II To further explore if neurohormonal changes contribute to the rapid improvement and remission of diabetes after RYGB. Paper III To analyze and investigate the patients´ experiences of their life adjustments and HRQoL after RYGB. Paper IV To compare cytokine and adipokine levels in patients with obesity, with- and without T2D before and after RYGB and in comparison, to lean healthy controls.

20
Subjects and Study Design
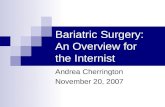
Paper I-III - Bariglykos Trial - Twenty-one patients with T2D; 14 women, mean age 55 years, mean preoperative BMI 36.8 kg/m2, were included and randomly assigned to either RYGB or standard-of-care medical treatment with an allocation ratio of 2:1 after completing the baseline examination shown below.
Figure 3. Consort Flow Diagram – Bariglykos trial

21
The surgery group was examined on the day of surgery after a 4-week LCD, at four weeks, 24 weeks and 104 weeks after surgery with lab tests, HRV measurements, subcutaneous adipose tissue (SAT) biopsy followed by an in-travenous arginine challenge and lastly an OGTT. The control group received routine lifestyle advice and continued or adjusted medications according to clinical guidelines, and the investigations were carried out at baseline and after 24 weeks. In Paper I and II the results up to 6 months follow-up were reported. For Paper III, HRQoL was evaluated using the RAND-36-item health survey before, at 24 weeks, and 104 weeks after RYGB. Furthermore, interviews for an in-depth analysis of HRQoL were performed 104 weeks after surgery. Paper IV Thirty-six patients (15 without T2D; 14 women, mean age 43 years, mean preoperative BMI 43.7 kg/m2 and 21 with T2D; 18 women, mean age 51 years, mean preoperative BMI 38.4 kg/m2) were compared before and six months after RYGB to 32 lean, healthy age- and sex-matched controls. Cyto-kines, adipokines, and peptides of relevance for inflammation and metabolism were analyzed in plasma.

22
Methods
Roux-En-Y Gastric Bypass surgery (Papers I-IV) Following a 4-week low-calorie diet (LCD) (800-1100 kcal/day), laparoscopic RYGB surgery was performed, where an approximately 100-cm Roux-limb is connected to a small proximal gastric pouch and an approximately 50-cm bili-opancreatic limb.
Biochemical Analyses (Papers I, II, IV) HbA1c, fasting glucose, C-peptide, cholesterol, HDL cholesterol, LDL cho-lesterol, and triglycerides, insulin, cortisol, and insulin-like growth factor -1 (IGF-1) were analyzed according to the clinical routine at the Department of Clinical Chemistry at the University Hospital of Uppsala. If not analyzed im-mediately, plasma samples were stored at -80°C. Hormone analysis was per-formed using commercially available kits, growth hormone (GH) (Immulite 2000XPi; Siemens Healthcare Global), and total adiponectin (RnD Systems, Minneapolis, MN, USA), total GLP-1 (Merck Millipore St Louise, MO, USA), total GIP (Merck Millipore, Darmstadt, Germany) and total Adiponec-tin (RnD Systems, Minneapolis, MN), glucagon (Mercodia, Uppsala, Swe-den), total GLP-1 (Merck Millipore St Louise, MO, USA), total GIP (Merck Millipore, Darmstadt, Germany) Leptin, Reg3A, TNF-alpha, IL-6, IL-33, visfatin, IFN-beta, IL-27, IFN-gamma, IL-1 alpha, IL-2, resistin, osteopontin, IL-15, IL-21, hepatocyte growth factor (HGF), bone morphogenic protein-4 (BMP-4) and IL-18 were analyzed using a magnetic bead-based Luminex as-say (RnD Systems).
Nonesterified fatty acids (NEFA) were measured using the Free Fatty Acid Fluorometric Assay Kit (Cayman Chemical, Ann Arbor, MI). Glycerol using Free Glycerol Reagent (Sigma-Aldrich, St. Louis, MO). The absorbance or fluorescence was read using a microplate reader (Infinite®200 PRO, Tecan, Männedorf, Switzerland).

23
Heart rate variability analysis (Paper II) A 5-minute resting HRV analysis, as previously described (67), was per-formed to study the efferent activity in the autonomic nervous system. R–R intervals were extracted from the recorded ECG:s and transformed into evenly sampled (2 Hz) heart rate time series by cubic spline interpolation. HRV was analyzed by power spectrum analysis of R-R intervals related to normal sinus rhythm using Welch’s periodogram method as previously described (68). The total spectral power, the power of the low-frequency (PLF,0.04-0.15 Hz), and high-frequency (PHF, 0.15-0.50 Hz), all log-transformed, were calculated over consecutive 5-minute periods from the complete recording. Since PHF mainly reflects the parasympathetic part while PLF reflects a combination of sympathetic and parasympathetic activity, the ratio PLF/PHF was used as a marker of the balance between sympathetic and parasympathetic activity (69). The HRV analysis was performed using Matlab software (MathWorks, Na-tick, MA).
Intravenous Arginine Stimulation test (Paper II) Insulin secretion was assessed after administrating a bolus dose of 5 g arginine iv, followed by measuring S-insulin at 0, 2, 3, 4, 5, 7, 10, 25, and 30 minutes (70). The acute insulin response to arginine (AIRarg) in paper II was calcu-lated using the mean of the three highest plasma insulin concentrations ob-tained within 5 minutes after the arginine bolus minus the prestimulus plasma insulin concentration.
Oral glucose tolerance test (OGTT) Paper I-II All subjects underwent a 3-h OGTT at all-time visits except at the post-LCD visit for the surgical group, to assess glucose tolerance and insulin secretion and sensitivity. Blood samples during the OGTT were obtained at baseline and 15, 30, 60, 90, 120, and 180 minutes after ingestion of a glucose solution to measure the levels of plasma glucose and insulin. Plasma FFA levels were measured using a commercially available FFA fluorometric assay kit (Cay-man Chemical, Ann Arbor USA). According to the manufacturer protocol, plasma glycerol levels were measured using Free Glycerol Reagent (Sigma-Aldrich, St. Louis, USA).
The OGTT data were used to assess glucose tolerance and to calculate dy-namic insulin sensitivity and secretion indices; the Matsuda index and the In-sulinogenic Index (IGI), respectively (71).

24
Adipose tissue biopsy (Paper I) The SAT samples were obtained via a needle biopsy following local anesthe-sia. However, at the post-LCD investigation, adipose tissue was obtained by surgical biopsy during the RYGB procedure. A part was immediately frozen in liquid nitrogen and stored at -80°C for gene expression analysis, whereas the other part was imminently used to perform ex vivo metabolic assays. Adi-pose tissue was digested with collagenase A (Roche, Indianapolis, IN, USA) for one hour at 37oC in a shaking water bath. After collagenase treatment, the cell suspension was filtered through a nylon mesh and washed, and isolated adipocytes were used for glucose uptake and lipolysis assays and adipocyte size measurements. Due to the limited amount of tissue obtained, parts of the experiments could not be performed in all subjects.
Glucose uptake in adipocytes (Paper I ) Glucose uptake rate was measured as previously described (72). Briefly, iso-lated adipocytes were diluted in Krebs-Ringer-Hepes (KRH) buffer supple-mented with 4% BSA, 150 nM adenosine (Sigma Chemical, St. Louise, MO, USA), and were incubated in triplicates at 37oC in a shaking water-bath for 15 minutes with or without 25 or 1000 µU/ml of insulin corresponding to physiological and supra-physiological concentrations respectively of insulin (Actrapid, Novo Nordisk, Bagsvaerd, Denmark). After that, cells were incu-bated with D-(U-14C) glucose (0.86 µM glucose, 0.26 mCi/mL, Perkin Elmer, Boston, USA) for 45 minutes. The reaction was stopped by transferring the cells suspension into pre-chilled tubes on ice, and cells were immediately sep-arated from media by centrifugation through silicon oil (SERVA Electropho-resis GmbH, Germany). Radioactivity associated with cells was then meas-ured with a scintillation counter (Radiomatic series 500TR, Perkin Elmer An-alytical Instruments). Glucose uptake was expressed as clearance of medium glucose per cell. Cell number was determined following measurements of tri-glyceride content (Doles extraction) (73) and cell size as described below.
Lipolysis in adipocytes (Paper I ) The lipolysis rate was measured in triplicate under basal conditions or during β-adrenergic-stimulation with isoproterenol (Sigma), or combined isopro-terenol+insulin exposure as previously described (74). To measure basal and stimulated lipolysis, the cell suspension was incubated without or with isopro-terenol (0.5 µM), respectively, in a shaking water bath at 37°C for 120 minutes. In addition, to measure the antilipolytic effect of insulin, the cells were treated with different concentrations of insulin (0.1-100 µU/ml) together

25
with isoproterenol (0.5 µM). The reaction was stopped by transferring the vi-als containing cell suspension to ice. Hereafter, to determine the lipolysis rate, glycerol released into the media was measured using Free Glycerol Reagent (Sigma). The glycerol released into the medium was normalized per 105 cells.
Adipocyte size (Paper I ) Adipocyte size was measured in isolated adipocytes suspension according to the method previously described by Smith et al. (75). Briefly, 200 µl of cell suspension was pipetted on a siliconized glass slide and covered with a co-verslip. For each sample, the diameter of 100 adipocytes was measured from different areas of the slide surface using a Zeiss microscope and Axiovision software (Axiovision, München, Germany). Adipocytes were identified by their spherical shape and light-refractile lipid droplet. Based on the cell diam-eters, an individual adipocyte volume was determined, and weight was com-puted using the density of triolein, 0.915 g/ml. The total number of adipocytes in the body was estimated, as described previously (76). Total body fat mass (BF%/100) × body weight) was divided by mean fat cell weight.
Gene expression analysis (paper I, II) Total RNA from adipose tissue was harvested using the RNeasy lipid tissue mini kit (Qiagen, Hilden, Germany). Total RNA concentration was measured with a Nanodrop system (Thermo Scientific) and then reverse-transcribed us-ing High Capacity cDNA Reverse Transcriptase Kits (Applied Biosystems, Foster City, CA, USA). All protocols were performed strictly by the manufac-turer’s instructions. The expression of genes was studied with TaqMan gene expression assays (Thermo Fisher) and detected using the QuantStudio 3 sequence detection sys-tem (Applied Biosystems). The data were calculated using a relative standard curve method or 2−delta Ct. The results are plotted as relative quantification using glucuronidase beta (GUSB) as an endogenous control. All samples were run in duplicates. The details of gene-specific TaqMan probes are given in the supplementary material in the paper I (ESM, table 3). We first studied the expression of selected genes in a subset of adipose tissue samples collected pre- and four weeks post-surgery (n=8). The genes of interest were further analyzed in a full set of samples, including adipose tissue collected at baseline, 4, 24 weeks post-surgery (n=11 to 12), and samples from the control group (n=6).

26
RAND SF-36 health questionnaire (Paper III) The RAND SF-36 health questionnaire was used to assess eight separate health concepts with multi-dimensional scales (77). These are physical func-tioning, role limitations due to physical health problems, pain, general health, energy/fatigue, social functioning, role limitations due to emotional health problems, and emotional well-being. An additional single item assesses change in perceived health during the last 12 months. Scoring the question-naire is a two-step procedure; first, for each item, the response category is recoded to a numeric value according to a scoring key, and second, all specific items in the same subscale are averaged to create the eight subscale scores. The scores may be treated as an ordinal scale or as an approximation of an interval or ratio level scale. Scores in subscales range from 0 to 100, with 100 representing the best level of health status (78). A difference of 3–5 points in the RAND-36 subscales is considered clinically significant (79,80).
Qualitative interviews (Paper III) Two years after the RYGB surgery, the interviews were conducted by a social worker using the same interview guide.
The duration of each interview varied between 0.5 and 1.5 hours, and all par-ticipants were given enough opportunity to share their views. A semi-struc-tured interview guide was developed according to the aim of the study.

27
Results
Paper I As expected, all 13 patients who underwent RYGB had a significant reduction in weight, waist-hip ratio, BMI, and body fat percent between the baseline visit and the four weeks visit and between the 4 and 24 weeks visit. HbA1c and fasting plasma glucose were also significantly decreased. All patients ex-cept one discontinued their oral antidiabetic treatment before the 4-week post-surgery visit and the patient that continued metformin treatment received a lower dose. The patients had significantly lower fasting insulin levels and glucose and in-sulin at 120 minutes of OGTT. Insulin sensitivity assessed with the Matsuda index was increased at 4 and 24 weeks post-surgery.

28
Adipocyte diameter was compared between visits (Figure 4 a-c). No signifi-cant difference was seen between baseline and post-LCD visits.
Figure 4. Effect of bariatric surgery on adipocyte size and metabolism ex vivo. (a) average adipocyte diameter (b) distribution of adipocyte diameter (n=12, 12, 10 and 12 for baseline, post-LCD, 4 wks post-surgery and 24 wks-post surgery, respec-tively) (c) the representative image of adipocyte size. The images were captured us-ing a light microscope with a magnification of 100X.
At four weeks after surgery, the adipocyte size significantly decreased by 13% to baseline and post LCD. At 24 weeks, the adipocyte size was smaller by 10% compared to the size of adipocytes at baseline and post-LCD visit (Figure 3a). At 4 and 24 weeks, the adipocyte volume was decreased vs. baseline and post-LCD. The total number of adipocytes in the body, based on total body fat and aver-age fat cell size, showed that there was no reduction but a tendency to increase (NS), in the adipocyte number 4 weeks, after surgery.
At 24 weeks, however, the number was lower compared to baseline and four weeks. Adipocyte glucose uptake rate was measured at basal, submaximal, and maximal insulin-stimulated glucose uptake, and no difference was seen be-

29
tween the baseline and post-LCD investigations. At four weeks, the submaxi-mal and maximal insulin-stimulated glucose uptake was decreased by about 35%. At 24 weeks, adipocyte glucose uptake tended to increase without reach-ing significance.
Adipocyte lipolysis rate was also studied between visits, and the basal lipol-ysis rate did not change significantly. However, at four weeks, isoproterenol-stimulated lipolysis tended to be higher, whereas, at 24 weeks, it dropped to that of baseline visit and was significantly lower than four weeks. Expression of genes involved in adipose tissue function showed a signifi-cant increase after four weeks in genes involved in fatty acid oxida-tion,e.g., CPT1B and ADIPOQ,whereas Leptin and E2F1 (involved in cell proliferation) were reduced (p<0.05 for all) No changes were seen between visits in the control group.
Paper II We observed changes in incretin hormone levels, which were most apparent at the OGTT (Figure 5a-f). Fasting GLP-1 levels decreased at four weeks and 24 weeks compared to baseline; however, the GLP-1 response during OGTT was higher at both 4 and 24 weeks post-surgery. Fasting GIP levels did not differ between visits; however, the peak GIP levels during OGTT (30 min) were higher at 4 and 24 weeks for both visits), and instead, a steep decline was observed after 30 minutes. Fasting glucagon levels did not differ between visits than baseline, which then dropped to their starting levels at 180 min, but remained numerically higher than the baseline visit. Peak glucagon levels at four weeks during OGTT were higher than at 24 weeks. The total AUC for glucagon during OGTT was higher at 4 and 24 weeks compared to baseline.

30
Figure 5. Plasma incretins and glucagon in response to OGTT in surgery and control groups. a GLP-1 in surgery group; b GLP-1 in control group; c GIP in surgery group; d GIP in control group; e glucagon in surgery group; f glucagon in control group. Data are shown as mean ± 95% CI. a,ABaseline vs post surgery at 4 weeks. b,BBaseline vs post surgery at 24 weeks. c,C4 weeks vs post surgery at 24 weeks. Lower case letters; p < 0.05, upper case letters; p < 0.01

31
Insulin secretion during arginine challenge decreased at 4 and 24 weeks compared to baseline (Figure 6 a,b). The acute insulin response to arginine at the three peak time points (2, 3 and 4 min) was lower by 45% and 48% at 4 and 24 weeks, respectively, compared to baseline. However, the relative in-crease in peak insulin levels after arginine did not change at 4 weeks but was higher by 85% at 24 weeks compared to baseline.
Figure 6. Arginine-stimulated insulin secretion in surgery and control groups. a In-sulin levels during arginine challenge in surgery group, b insulin levels during argi-nine challenge in control group. Data are shown as mean ± 95% CI. ABaseline vs post surgery at 4 weeks. Bbaseline vs post surgery at 24 weeks. C4 weeks vs post sur-gery at 24 weeks. Lower case letters; p < 0.05, upper case letters; p < 0.01
We measured circulating levels of adipokines and found higher levels of adi-ponectin at 4 and 24 weeks. Leptin levels reduced at 4 and 24 weeks after surgery. At 24 weeks, visfatin levels were higher than baseline and 4 weeks. Likewise, plasma resistin was higher at 24 weeks than baseline. At 24 weeks, bone morphogenic protein-4 (BMP4) levels were higher than baseline and 4 weeks.
Heart rate variability The changes in heart rate variability are summarized in Table 1. When com-paring to baseline, HRV at 4 and 24 weeks post-surgery were significantly increased. The RR interval was longer, corresponding to decreased heart rate. The significant rises in Ptot (total variability measurement) and spectral com-ponents such as PVLF depict enhanced parasympathetic nerve activity.

32
Table 1. Data are means (SD) of baseline values and of changes between follow-ups and baseline. Spectral Indices are log-transformed. RR= mean RR interval, Ptot=total power, PVLF=power of very low-frequency component, PLF=power of low-frequency component, PHF= power of high-frequency component. Lower case letters; p<0.05, Upper case letters; p<0.01 (paired t-tests). a,A Change at 4 weeks from baseline. b,B Change at 24 weeks from baseline.
The change in the Matsuda index from baseline to 4 weeks after surgery was positively associated with the change in Ptot (rho=0.762, p<0.05) and PLF
(rho=0.893, p<0.01) at 4 weeks after surgery. There were no associations be-tween change in the Matsuda index at 24 weeks and a change in HRV measures at 4 or 24 weeks. In the control group, no significant changes were observed in any of the above measures.
Paper III In this mixed-methods study, we observed a significant improvement from baseline to 6 months for two of the eight health concepts, general health, and emotional well-being. At two years, improvements were also seen in physical functioning, role limitations due to physical health problems, energy/fatigue, and social functioning. We performed multiple regression analyses between the magnitude of decrease in weight, BMI, and HbA1c during follow-up and improvement in HRQoL and found mostly non-significant associations. The analyses from qualitative interviews supported that the patients’ improvement in the quality of life was associated with achieving a balance between the ex-perience of the new bodyweight and self-confidence.
Paper IV In this exploratory study, the plasma levels of cytokines, adipokines, and other peptides relevant to inflammation and metabolism were measured in patients

33
with and without T2D before and six months after RYGB. They were com-pared to the levels of lean, healthy controls. At baseline, TNF-alpha, IL-6, IL-18, leptin, and hepatocyte growth factor (HGF) were higher in all patients, whereas islet-derived protein 3A (Reg3A) and bone morphogenic protein-4 (BMP4) were lower. In patients without T2D, IL-1alpha, IL-2, IL-15, and visfatin were increased, while IL-2, IL-18, and osteopontin were decreased. After surgery, IL-6 and HGF were still increased compared to controls. Reg3A, IL-27, and osteopontin increased in both RYGB groups. TNF-alpha, IL-18, and leptin remained elevated in patients without T2D. IL-1alpha, IL-2, IL-15, and visfatin increased in T2D patients and surpassed controls. Patients with T2D had higher growth hormone but lower leptin and TNF-alpha than those without.

34
Discussion
Metabolic effects of RYGB: Tissue crosstalk and time course (paper I-II) In paper I we observed that glycemic control and insulin sensitivity were markedly improved already four weeks after RYGB, and this was maintained at 24 weeks. In contrast, these rapid improvements in whole-body glucose ho-meostasis were not accompanied by consistent changes in insulin action on glucose uptake and lipolysis rates in isolated adipocytes studied ex vivo. There were, however, striking reductions in mean adipocyte size after four weeks. Notably, the patients followed a 4-week LCD regimen before surgery, and this contributes to the improvement in glucose homeostasis, as shown previously in the DiRECT trial (45). The discrepancy in insulin sensitization in vitro and in vivo may be due to mechanisms occurring mainly in tissues other than adipose, such as liver, mus-cle, or brain. It was previously reported that alterations in glycemic control occurred without changes in adipose function within the first weeks after RYGB (30,31) . Most studies indicate an increased peripheral and hepatic insulin sensitivity following RYGB (30,32,81), but there are also some reports suggesting that insulin sensitivity assessed with a hyperinsulinemic-euglycemic clamp may not be changed after up to one year even though circulating glucose and insu-lin levels are markedly reduced (82). This, in turn, may be compatible with early alterations in the oral glucose tolerance occurring as a consequence of rapid glucose absorption in the gut or gut hormone signaling. We found no consistent differences in glucose uptake and lipolysis in adipo-cytes, however, the observed changes in adipocyte morphology and expres-sion of adipokines such as an increase in adiponectin and decrease in leptin, respectively may, indicate that adipose tissue effects could be important via communication with other tissues, e.g., muscle, liver, and brain at this early time point. It is known from previous studies that secreted biomolecules from SAT and VAT influence glucose uptake in muscle cells (83).

35
In this study, we observed a striking decrease in adipocyte size, which was not accompanied by a similar degree of decrease in percent (or absolute amount) body fat. Furthermore, the absence of alterations in adipocyte size after the low-calorie diet, which induced a similar reduction of body weight, suggests that this decrease in cell size is specific to the RYGB. The size of the adipo-cytes observed four weeks post-surgery resemble that generally found in lean (84) individuals, whereas the bodyweight of the patients remained in the obe-sity range. In apparent contrast to our findings, it was previously shown by Andersson et al. (51) that a reduction in subcutaneous fat cell size two years after RYGB in obese women was more strongly associated with the improve-ment of insulin sensitivity than fat mass reduction per se. This is in harmony with other work showing an independent inverse association between fat cell size and insulin sensitivity (85). The explanation for the lack of such an asso-ciation in our present results may be the assessments' timing, as ours were done much earlier, at 4 weeks post-surgery. This may suggest that local AT factors such as size or insulin sensitivity of adipocytes are important at a later stage.
In contrast, other tissues or pathways are more important to mediate improved glucose homeostasis within the first 6 months after RYGB. This could be fur-ther supported by an observed significant association between adipocyte size at 24 weeks and basal, submaximal and maximal insulin-stimulated in vitro glucose uptake. In contrast, we did not find any association between the re-duced adipocyte size at four weeks, and insulin sensitivity index, Matsuda, or insulin-mediated adipocyte glucose uptake in vitro.
Interestingly, we found a partial regain of adipocyte size at 24 weeks, and additional assessments at two years of follow-up are ongoing. It was recently shown that independent of BMI, patients with higher body fat % displayed lower insulin sensitivity, and larger subcutaneous adipocytes 2 years after RYGB(86) . Thus, body fat % should also be taken into consider-ation when following-up patients after RYGB as it may provide additional information about the patients metabolic status. The expression of genes involved in cell proliferation was considerably de-creased. In contrast, the adipogenic genes increased after surgery, suggesting that RYGB surgery may have a stimulating effect on adipogenesis, leading to the formation of new, smaller adipocytes. However, due to the very slow turn-over rate of human adipocytes (87), it is unlikely that this would lead to a substantial increase in the total adipocyte number during the 4-24-week post-RYGB period.

36
Of note, an average shrinkage of each adipocyte may be linked to a temporary redistribution of lipid stores towards ectopic deposition, eg. in the liver, mus-cle and pancreas. This could probably explain the observed discrepancy at 4 weeks post-surgery between the relative reductions in body fat content (ap-prox. 7 %) and of adipocyte volume (approx. 35%). Thus, a relative redistri-bution of fat stores via flux from adipocytes to other sites, rather than an in-creased number of adipocytes is likely to occur. This is also supported by the elevated fasting FFA levels at 4 weeks and by somewhat increased adipocyte lipolysis rates. A temporary redistribution of lipids from visceral and subcu-taneous adipose depots to the liver has been reported previously following RYGB (88) , but it is not clear if it affects insulin sensitivity or glucose home-ostasis.Of note, the expression of CPT1b gene increased after surgery suggest-ing that adipocyte fatty acid oxidation may have increased, contributing to reduction of adipocyte triglyceride content and cell size. In paper II we showed an elevated response of incretin hormones and glucagon during OGTT after surgery. The fasting plasma levels of adiponectin were increased while leptin was reduced after RYGB. The heart rate variability and in particular, the HF component was increased after RYGB suggesting an el-evated parasympathetic outflow after surgery. Our results are in agreement with the previous studies in obese type 2 diabetes patients that reported increased GLP-1 levels during OGTT one month after surgery (89,90). Previous studies about GIP levels are less consistent, some showing increased levels after surgery (89), some decreased (91,92) and some showing no changes (93).
The mechanisms for the increase in incretin levels after bariatric surgery are not completely understood; however, the exposure of nutrients to the lower gut soon after ingestion may potentially change the duration of physiological release of incretin hormones. (94).
We further observed a paradoxical increase in glucagon during OGTT despite the marked increase in GLP-1, which inhibits glucagon release (95). This is in agreement with previous studies (96), and the mechanism for this remains to be elucidated (97). Increased plasma levels of leptin have been shown to significantly inhibit glu-cose-stimulated insulin secretion in vivo and determine insulin resistance (98). The reduction in leptin levels after surgery may play a direct or indirect role in bodyweight reduction and the control of type 2 diabetes after surgery. Sim-ilarly, the significant increase in the fasting adiponectin levels 24 weeks after RYGB, which is known to improve insulin sensitivity and inflammation

37
(99,100), suggests that this protein's role in mediating insulin sensitization comes at a later stage but not earlier after RYGB.
The ANS changes seen in our study with increased heart rate variability and in particular the elevated parasympathetic outflow after surgery is in accord-ance with what has previously been shown (101) and supports the theory that afferent vagal pathways are probably the most important link between the gut and the brain and interact in a complicated way with gut hormones.
Quality of Life (Paper III) In this study, we observed a significant improvement in general health and emotional wellbeing already at six months after surgery. Besides, after two years, improvement in six of the eight HRQoL domains was found (physical functioning, role functioning/physical, general health, energy/fatigue, social functioning, and emotional wellbeing). We could not, however, observe significant associations between the decrease in weight, BMI, and HbA1c and the improvement in the RAND-36 domains at the 6 and 12 months' follow-up. Earlier studies demonstrated mixed results concerning HRQoL postopera-tively (102-104). In the present study, the patients scored higher in six of the eight domains of the RAND-36 instruments compared at two years. All im-provements were well above 3-5 points, i.e., of significant clinical importance. The lack of consistently demonstrated significant associations between the magnitude of weight loss, HbA1c decrease, and BMI decrease and improved HRQoL might be because our study was underpowered to detect differences in HRQoL. When analyzing the qualitative interviews, we confirmed the results from the RAND-36. We could conclude that it was not necessarily the weight loss that contributed to the improvement in the HRQoL but that the patients managed to find a balance between the reduced body weight and increased self-confi-dence.
Effects on inflammation: cytokines and adipokines (Paper IV) In this study, we found that several inflammatory cytokines (TNF-alpha, IL-6, and IL-18) were elevated in patients with and without T2D compared to lean controls.

38
We observed a positive correlation between pre-operative BMI and TNF-al-pha levels, which supports the contribution of adipose tissue and stromovas-cular fraction to TNF-alpha's systemic levels (105).
Despite that, the TNF-alpha levels remained relatively unchanged in both groups following RYGB, which indicates that it is not only the sheer volume but perhaps also the adipocyte phenotype in obesity, which impacts the TNF-alpha production. Similar to our findings, previous studies have found that the levels of IL-6 remain increased after RYGB (106). We also observed a positive correlation of IL-6 to BMI. The gene expression of IL-6 in adipocytes was lower post-surgery, implying that the levels are maintained through its secretion from im-mune cells. Two cytokines, IL-2 and IL-18, varied between T2D and non-diabetic patients at baseline. Regarding IL-2, it has previously been shown that peripheral blood mononuclear cells (PBMCs) from subjects with T2D produce signifi-cantly less IL-2, a surrogate marker of proliferation when stimulated with the T-cell mitogen PHA. The lower production of IL-2 after PHA stimulation ob-served in individuals with obesity and T2D suggests that diabetes further im-pairs T-cells' ability to respond and proliferate (107). Circulating levels of IL-2 have previously been found to be reduced by calorie restriction but unaf-fected by RYGB (108). In contrast, we observed an increase of IL-2 in T2D patients after RYGB despite its positive correlation to BMI. This could indi-cate that the normalization of metabolic control following RYGB also affects the PBMCs capacity to produce IL-2. IL-18, on the other hand, is produced by a large number of tissues, including adipose tissue, skeletal muscle, pancreas, brain, and endothelium and is found to be increased in T2D patients (109) and correlates with insulin resistance and metabolic syndrome in patients with obesity (110). We observed a de-crease after RYGB as previously shown (111), We also found that gene ex-pression of IL18 in adipose tissue was reduced following RYGB, which fur-ther supports that the reduced circulating levels of IL-18 are related to weight loss. Interestingly, an experimental study has recently shown that the gene expression of IL-18 from the intestinal mucosa is reduced following RYGB (112). IL-27 was also measured in this study. At baseline, the IL-27 levels were com-parable between patients with obesity and lean patients, but the levels in-creased in both non-diabetic and T2D patients after RYGB. To the best of our knowledge, there are no previous reports on how the circulating levels of IL-

39
27 are affected in obesity or T2D following RYGB. Given the pleiotropic ef-fects of IL-27 (113,114) and counteracting the balance between pro- and anti-inflammatory effects, it isn't easy to interpret the clinical impact of this in-crease. We also measured several adipokines and other peptides of importance to obe-sity and T2D. We found increased adiponectin levels after RYGB in patients with T2D and without T2D, contributing to improved insulin sensitivity. Lep-tin levels decreased, as described in paper II. We measured the levels of islet-derived protein 3A (Reg3A), which, to the best of our knowledge, has not previously been studied in patients with obesity undergoing RYGB. We found that the levels of Reg3A were lower at baseline in both groups but increased following RYGB and were found to be elevated compared to lean controls. These changes could reflect gut microbiota altera-tions, which are known to be permanently altered following RYGB (115). The increased levels of Reg3A could, as IL-27, reflect an attempt to counteract the increase of other pro-inflammatory cytokines such as IL1-alpha and IL-15. Visfatin, which has previously been linked to obesity and T2D (116) and it's levels have been found to correlate with BMI. We found that visfatin was in-creased in the present non-diabetic patients, but unchanged following RYGB, and increased in T2D patients. However, the gene expression in adipose tissue was unaltered, suggesting increased secretion from leukocytes. Apart from its relation to body weight and metabolic markers, previous reports have also de-scribed a strong correlation between visfatin levels and inflammatory cyto-kines, such as IL-6, which could explain our observed increase in visfatin lev-els following RYGB. When computing correlations for post-surgery visfatin levels, we found a positive correlation with TNF-alpha, IL-1, IL-2, IL-6, and IL-2.

40
Conclusions
Our findings support that neurohormonal mechanisms are involved in the rapid improvement of glucose metabolism after RYGB. We hypothesize that shortly after surgery, the elevated parasympathetic outflow and the increase in incretin hormones contribute to the increase in insulin secretion and an in-crease in insulin sensitivity leading to diabetes remission. In our ongoing analyses for the two-year follow-up, we observed that the pa-tients maintained a stable BMI having a discrete increase in total body fat. Insulin resistance and insulin sensitivity remain relatively unchanged after two years. Heart rate variability parameters at two years however, return towards baseline values. Still, a significant reduction of heart rate could indicate a per-sisting change in the balance between the sympathetic and parasympathetic activity. Adipocytes remained smaller throughout the two years and compared to baseline the adipocyte basal and insulin-stimulated glucose uptake did not change at four weeks, but gradually increased at 24 weeks and reached signif-icance at 104 weeks suggesting that improvements in adipose tissue factors or adipocyte insulin sensitivity might develop at a later stage, as a secondary phenomenon. The significant early decrease in morning cortisol seen at four weeks is not present at two years; however, ACTH shows a trend towards lower values that seems to be present at two years. The corticotropic axis in RYGB has not been studied extensively before, and existing studies have inconclusive results, larger studies will be needed to explore this. The improved HRQoL after gastric bypass surgery in obese patients with type 2 diabetes, was not explicitly explained by the magnitude of weight loss. In-stead, the participants achieved a state of union between body and conscious-ness.

41
The patients with and without T2D after RYGB, retained, or even further in-creased a pro-inflammatory cytokine profile at six months, despite the dra-matic weight loss and improvement in metabolic measures compared to lean healthy controls.
The persisting differences in the inflammatory and adipokine profiles between patients having had gastric bypass surgery and lean controls need to be ad-dressed clinically to further reduce the risk of long-term complications. In summary, our studies provided an integrated and repeated assessment of neural, hormonal, and metabolic pathways, potentially contributing to the rapid glycemic improvement following RYGB in patients with T2D (figure 7).
Figure 7. Schematic time course of RYGB effects. (red arrows- clinical outcomes, yellow arrows - hypothetical mechanisms.)
We hypothesize that shortly after surgery, an elevated parasympathetic out-flow and reduced cortisol axis activity may improve insulin sensitivity and act together with the increased incretin hormones to promote diabetes remission. Adipose tissue morphological and functional changes also occur within a few weeks after RYGB in T2D patients. Still, these changes do not seem to have a direct effect on the improvements in metabolism. The inflammatory and ad-ipokine profile of patients with obesity appears to persist after RYGB. The in-depth interviews of patients after RYGB contributed with useful infor-mation as to what the patients experience after RYGB and how this improves their quality of life. This information can improve patient care and shed some more light on the burden of metabolic syndrome.

42
Overall, our findings should mainly be considered as hypothesis-generating, and larger studies are needed for confirmation and detailed characterization of the metabolic and neuroendocrine effects of bariatric surgery.

43
Svensk sammanfattning (Summary in Swedish)
Övervikt och fetma är ett av våra allvarligaste folkhälsoproblem. Mer än 1,9 miljarder människor i världen är överviktiga och 650 miljoner har fetma. Övervikt definieras enligt Världshälsoorganisationen (WHO) att ha ett BMI mellan 25–30 kg/m2 och fetma definieras som ett BMI över 30 kg/m2. Denna epidemi drabbar även den yngre befolkningen där man ser ca 38 miljoner barn under 5 år med övervikt.
Att ha övervikt eller fetma innebär en ökad risk för att drabbas av andra sjuk-domar, exempelvis högt blodtryck, höga blodfetter, typ 2 diabetes (T2D) samt hjärtkärlsjukdomar. Fetma ökar även risken för vissa cancerformer, till exem-pel bröstcancer och pankreascancer. Grav fetma (definieras med ett BMI över 40 kg/m2) innebär en mer än 10 gånger så hög risk att dö i förtid jämfört med normalvikt. För att förebygga övervikt behövs många olika typer av åtgärder där diet är en viktig del. Det saknas dock riktigt effektiva dieter eller medi-cinska behandlingar som kan ge en bestående viktminskning. Typ 2 diabetes är en av de vanligaste sjukdomar som drabbar överviktiga pa-tienter och karakteriseras av högt blodsocker och en ökad insulinresistens. Ef-ter några års sjukdomsduration tillkommer ofta dessutom en nedsatt insulin-produktion från bukspottskörteln. T2D ingår i det metabola syndromet med högt blodtryck, höga blodfetter, övervikt och bukfetma.
T2D är en ökande folksjukdom där prevalensen i Sverige idag är cirka 4–5 % och i världen i genomsnitt cirka 8,5%. Behandlingen eftersträvar att reducera patientens samlade riskfaktorer för hjärtkärlsjukdom, och viktminskning är en åtgärd som kan förbättra glukoskontrollen.
Trots nya och bättre läkemedelsbehandlingar för T2D finns det fortsatt många patienter som inte uppnår och behåller en god metabol kontroll. Överviktskirurgi har de senaste åren blivit ett effektivt behandlingsalternativ mot övervikt och fetma, man har även sett långvariga positiva effekter även mot T2D. Olika typer av överviktskirurgi används men den vanligaste operat-ionen som används i Sverige och internationellt är den så kallade Roux-en-Y

44
Gastric Bypass (RYGB). Vid RYGB skapas en ny magsäcksficka av den övre delen av magsäcken (ca 15–30 ml stor) och resterande magsäcken och början av tunntarmen kopplas bort. Efter RYGB minskar matintaget, nervsystemet i tarmen påverkas och hormonella förändringar uppträder, gallsyraomsätt-ningen förändras och vi får även en effekt på sammansättningen av bakterie-floran i tarmen. Allt detta sammantaget bidrar till en bestående viktnedgång, en förbättrad glukoskontroll och i många fall även en remission av T2D. Detta arbete fokuserade på hur neurohormonella, fettvävs- och inflammato-riska mekanismer bidrar till förbättringen av den metabola kontrollen efter RYGB och hur dessa förändringar utvecklas över tid efter RYGB. Dessutom undersöktes hur livskvaliteten utvecklas efter RYGB och hur detta korreleras till förbättringar i metabolismen. Artikel I, fokuserade på metabola förändringar i hela kroppen i relation till förändringar i underhudsfettet. Fettvävens utseende och funktion undersöktes för att se hur detta förändras efter RYGB. Vi observerade en tidig minskning i fettcellernas storlek redan 4 veckor efter RYGB men trots detta ses inga po-sitiva effekter vad gäller fettcellernas insulinkänslighet Inget samband kunde heller fastställas mellan den förbättrade allmänna metabola kontrollen och de tidiga förändringarna i fettväven efter RYGB. Artikel II, fokuserade på förändringarna i det autonoma nervsystemet och hor-monerna efter RYGB. Vi observerade förändringar i det autonoma nervsyste-met redan 4 veckor efter RYGB. Hormonellt påvisas både lägre nivåer av kor-tisol på morgonen och en förstärkt utsöndring av tarmhormoner efter intag av sockerlösning. Dessa effekter verkar ha en central roll när det gäller tidig po-sitiv påverkan på insulinresistens och diabetes postoperativt. Artikel III - I denna studien intervjuades patienterna med T2D 2 år efter RYGB för att undersöka hur operationen påverkade deras livskvalité. Vi ob-serverade att förbättringarna vad gäller livskvalitet efter RYGB inte korrele-rade till graden av viktreduktion utan mer att personerna upplevde en ökad balans mellan kropp och själ efteråt.
Artikel IV – I denna studie undersöktes olika inflammatoriska ämnen (cytoki-ner, adipokiner) som har visat sig vara viktiga vad gäller kroppens metabola kontroll. Vi undersökte hur nivåerna av dessa ämnen skiljer sig åt mellan överviktiga patienter med och utan T2D, hur det ser ut hos normalviktiga kon-troller och hur nivåerna av dessa olika ämnen förändras efter RYGB. Vi ob-serverade att den inflammatoriska profilen hos de överviktiga patienterna till viss del kvarstår efter RYGB, detta trots en påtaglig viktreduktion och en för-bättrad metabol kontroll.

45
Acknowledgements
This thesis has been made possible thanks to the help and support of many people, to whom I express my sincere appreciation. A thank you to the Faculty of Medicine at the University of Uppsala for giving me the opportunity to carry out my Ph.D. studies. Many thanks to all the patients that agreed to participate in our trial and re-mained positive throughout the two years of follow-up, always willing to come to the study visits. Without them, this work would not be possible. Professor Jan Eriksson, my main supervisor. I would like to express my sin-cere gratitude for your continuous support during these years and for your pa-tience, motivation, and immense knowledge. Your guidance helped me in all the aspects of my studies. I could not have imagined having a better advisor and mentor for my Ph.D studies. Professor Magnus Sundbom, co-supervisor. Besides being instrumental with the main intervention in our trial, the combination of your surgical skills and in-depth theoretical knowledge in the field of bariatric surgery have been invaluable. Professor Per-Ola Carlsson, co-supervisor. Thank you for your inspiring en-thusiasm in the field of research and your support during my studies. Professor Emeritus Anders Karlsson – The year I started as a resident doc-tor in the Department of Endocrinology, you retired. I initially felt disap-pointed to have missed the opportunity to work and learn from you. You have, however, continued to work and inspire the whole team with your enthusiasm and knowledge. It is an honor for me to have worked with you both in the clinic and research. Associate Professor Janeth Leksell – Thank you for sharing your invaluable knowledge and experience in the field of qualitative research. Paper III would not have been possible without you.

46
Associate Professor Daniel Espes – Your driving-force is fantastic! It has been great working with you both clinically and in research. Prasad Kamble – This thesis would not have been possible without your help with the lab experiments and with the manuscripts . You really made it a smoother roller-coaster ride! Thank you for everything. Maria Pereira – You have been a reliable and stable help throughout all these years. From our short morning meetings at Liten Lär to the more extended discussions and phone calls, you have helped me in every problem that can come up during a Ph.D. student´s bumpy ride. My fellow co-authors- Eva Randell, thank you for your fantastic work with the patients’ interviews and your input in the qualitative paper. A big thank you to Andreas Rosenblad and Ulf Hammar for helping with our statistical endeavors. Gretha Boersma for kick-starting the lab analyses and providing the starting data for our projects, Urban Wiklund, for your help analyzing the heart rate variability data. Per Lundkvist – It has been a pleasure working with you both at the department and in the research group. The fantastic research team for all the meetings, work and time, spent together. The best research nurses Carola Almström, Caroline Woxberg, Anna Åh-lander, Sofia Löfving, Monika Gelotte, and Jan Hall for all your support, hard work and the laughs over these past years. Thank you to Karin Kjell-ström and Rebecka Hilmius for all the help with collecting the data for paper IV. Lastly all the present and past members of the clinical diabetes group: As-sel Sarsenbayeva, Milica Vranic, Robin Kristofi, Kristina Almby, Su-sanne Hetty, Cherno Sidibeh, Joey Lau Börjesson. All my wonderful present and past colleagues at the Endocrinology & Dia-betology Department; Östen, Britt, Karin, Andreas, Niclas, Magnus, Jarl, Selwan, Steinunn, Katarina, Eleni, Arvo, Erika, Georgios, Duska, Be-atrice. I am not exaggerating when I say that we have the best Endocrinology clinic! All the nurses and administrative personal at the Endocrinology & Diabetol-ogy Department for being always available and willing to help make work a daily pleasure. My friends in Uppsala and around the world for being there throughout the years despite the distances separating us. To my best friends in our “Challenge group” that pushed me to do things, I would never have thought of doing alone!

47
My father, mother and my sisters, for their love and support. No words can describe my gratitude. My extended family (Panagos, Lena, Melina, and Makis, Florian, Michalis) for also being so loving and helpful. Σας ευχαριστώ για όλα! Finally, thanks to my beloved family, my dear children Eleana, Dimitris, and my amazing wife Denia, for all support and love, thank you for everything! This work was supported by grants from; the Swedish Diabetes supported by researchgrants from the Swedish Diabetes Foundation, Excellence Of Diabe-tes Research in Sweden (EXODIAB), the Ernfors foundation, and by ALF funding from Uppsala County Council and Uppsala University Hospital.

48
References
1. Grundy SM. Multifactorial causation of obesity: implications for prevention. Am J Clin Nutr. 1998;67(3 Suppl):563S-72S.
2. Bluher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288-98.
3. Heymsfield SB, Wadden TA. Mechanisms, Pathophysiology, and Management of Obesity. New England Journal of Medicine. 2017;376(3):254-66.
4. Murray S, Tulloch A, Gold MS, Avena NM. Hormonal and neural mechanisms of food reward, eating behaviour and obesity. Nat Rev Endocrinol. 2014;10(9):540-52.
5. Field AE, Coakley EH, Must A, Spadano JL, Laird N, Dietz WH, et al. Impact of Overweight on the Risk of Developing Common Chronic Diseases During a 10-Year Period. Archives of Internal Medicine. 2001;161(13):1581-6.
6. Gao F, Zheng KI, Wang X-B, Sun Q-F, Pan K-H, Wang T-Y, et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care. 2020;43(7):e72-e4.
7. Pratley RE. The early treatment of type 2 diabetes. Am J Med. 2013;126(9 Suppl 1):S2-9.
8. Merino J, Udler MS, Leong A, Meigs JB. A Decade of Genetic and Metabolomic Contributions to Type 2 Diabetes Risk Prediction. Curr Diab Rep. 2017;17(12):135.
9. Portha B, Chavey A, Movassat J. Early-life origins of type 2 diabetes: fetal programming of the beta-cell mass. Exp Diabetes Res. 2011;2011:105076.
10. Dendup T, Feng X, Clingan S, Astell-Burt T. Environmental Risk Factors for Developing Type 2 Diabetes Mellitus: A Systematic Review. Int J Environ Res Public Health. 2018;15(1).
11. Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378(9785):31-40.
12. Federation ID. IDF diabetes atlas: International Diabetes Federation, Executive Office; 2011.
13. Wadden TA, Webb VL, Moran CH, Bailer BA. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012;125(9):1157-70.
14. Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193-203.

49
15. Drucker DJ, Sherman SI, Gorelick FS, Bergenstal RM, Sherwin RS, Buse JB. Incretin-based therapies for the treatment of type 2 diabetes: evaluation of the risks and benefits. Diabetes care. 2010;33(2):428-33.
16. Verma S, McMurray JJV. SGLT2 inhibitors and mechanisms of cardiovascular benefit: a state-of-the-art review. Diabetologia. 2018;61(10):2108-17.
17. Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA. 2004;291(3):335-42.
18. Saely CH, Geiger K, Drexel H. Brown versus white adipose tissue: a mini-review. Gerontology. 2012;58(1):15-23.
19. Ottaviani E, Malagoli D, Franceschi C. The evolution of the adipose tissue: a neglected enigma. Gen Comp Endocrinol. 2011;174(1):1-4.
20. Ahima RS, Flier JS. Adipose tissue as an endocrine organ. Trends Endocrinol Metab. 2000;11(8):327-32.
21. Coelho M, Oliveira T, Fernandes R. Biochemistry of adipose tissue: an endocrine organ. Arch Med Sci. 2013;9(2):191-200.
22. Reilly SM, Saltiel AR. Adapting to obesity with adipose tissue inflammation. Nat Rev Endocrinol. 2017;13(11):633-43.
23. Larabee CM, Neely OC, Domingos AI. Obesity: a neuroimmunometabolic perspective. Nat Rev Endocrinol. 2020;16(1):30-43.
24. Cardiovascular Effects of Intensive Lifestyle Intervention in Type 2 Diabetes. New England Journal of Medicine. 2013;369(2):145-54.
25. Daigle CR, Brethauer SA, Tu C, Petrick AT, Morton JM, Schauer PR, et al. Which postoperative complications matter most after bariatric surgery? Prioritizing quality improvement efforts to improve national outcomes. Surg Obes Relat Dis. 2018;14(5):652-7.
26. Buchwald H, Estok R, Fahrbach K, Banel D, Jensen MD, Pories WJ, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248-56 e5.
27. Schauer PR, Burguera B, Ikramuddin S, Cottam D, Gourash W, Hamad G, et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003;238(4):467-84; discussion 84-5.
28. Sjöström L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683-93.
29. Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM, et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995;222(3):339-50; discussion 50-2.
30. Mingrone G, Cummings DE. Changes of insulin sensitivity and secretion after bariatric/metabolic surgery. Surg Obes Relat Dis. 2016;12(6):1199-205.
31. Bojsen-Møller KN, Dirksen C, Jørgensen NB, Jacobsen SH, Serup AK, Albers PH, et al. Early enhancements of hepatic and later of peripheral insulin sensitivity combined with increased postprandial insulin secretion contribute to improved glycemic control after Roux-en-Y gastric bypass. Diabetes. 2014;63(5):1725-37.
32. Camastra S, Gastaldelli A, Mari A, Bonuccelli S, Scartabelli G, Frascerra S, et al. Early and longer term effects of gastric bypass surgery on tissue-specific insulin sensitivity and beta cell function in morbidly obese patients with and without type 2 diabetes. Diabetologia. 2011;54(8):2093-102.
33. Batterham RL, Cummings DE. Mechanisms of Diabetes Improvement Following Bariatric/Metabolic Surgery. Diabetes Care. 2016;39(6):893-901.

50
34. Cummings DE, Rubino F. Metabolic surgery for the treatment of type 2 diabetes in obese individuals. Diabetologia. 2018;61(2):257-64.
35. Falken Y, Hellstrom PM, Holst JJ, Naslund E. Changes in glucose homeostasis after Roux-en-Y gastric bypass surgery for obesity at day three, two months, and one year after surgery: role of gut peptides. J Clin Endocrinol Metab. 2011;96(7):2227-35.
36. Jørgensen NB, Jacobsen SH, Dirksen C, Bojsen-Møller KN, Naver L, Hvolris L, et al. Acute and long-term effects of Roux-en-Y gastric bypass on glucose metabolism in subjects with Type 2 diabetes and normal glucose tolerance. Am J Physiol Endocrinol Metab. 2012;303(1):E122-31.
37. Shin AC, Zheng H, Berthoud HR. Vagal innervation of the hepatic portal vein and liver is not necessary for Roux-en-Y gastric bypass surgery-induced hypophagia, weight loss, and hypermetabolism. Ann Surg. 2012;255(2):294-301.
38. Kentish SJ, Page AJ. The role of gastrointestinal vagal afferent fibres in obesity. J Physiol. 2015;593(4):775-86.
39. Blasi C. The Role of the Vagal Nucleus Tractus Solitarius in the Therapeutic Effects of Obesity Surgery and Other Interventional Therapies on Type 2 Diabetes. Obesity Surgery. 2016;26(12):3045-57.
40. Murphy KG, Bloom SR. Gut hormones and the regulation of energy homeostasis. Nature. 2006;444(7121):854-9.
41. Muscelli E, Emdin M, Natali A, Pratali L, Camastra S, Gastaldelli A, et al. Autonomic and Hemodynamic Responses to Insulin in Lean and Obese Humans1. The Journal of Clinical Endocrinology & Metabolism. 1998;83(6):2084-90.
42. Nault I, Nadreau E, Paquet C, Brassard P, Marceau P, Marceau S, et al. Impact of bariatric surgery--induced weight loss on heart rate variability. Metabolism: clinical and experimental. 2007;56(10):1425-30.
43. Perugini RA, Li Y, Rosenthal L, Gallagher-Dorval K, Kelly JJ, Czerniach DR. Reduced heart rate variability correlates with insulin resistance but not with measures of obesity in population undergoing laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2010;6(3):237-41.
44. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860-7.
45. Lean ME, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet. 2018;391(10120):541-51.
46. Frikke-Schmidt H, O'Rourke RW, Lumeng CN, Sandoval DA, Seeley RJ. Does bariatric surgery improve adipose tissue function? Obes Rev. 2016;17(9):795-809.
47. Klein S, Fontana L, Young VL, Coggan AR, Kilo C, Patterson BW, et al. Absence of an effect of liposuction on insulin action and risk factors for coronary heart disease. N Engl J Med. 2004;350(25):2549-57.
48. Dillard TH, Purnell JQ, Smith MD, Raum W, Hong D, Laut J, et al. Omentectomy added to Roux-en-Y gastric bypass surgery: a randomized, controlled trial. Surg Obes Relat Dis. 2013;9(2):269-75.
49. Fabbrini E, Tamboli RA, Magkos F, Marks-Shulman PA, Eckhauser AW, Richards WO, et al. Surgical removal of omental fat does not improve insulin sensitivity and cardiovascular risk factors in obese adults. Gastroenterology. 2010;139(2):448-55.

51
50. Herrera MF, Pantoja JP, Velázquez-Fernández D, Cabiedes J, Aguilar-Salinas C, García-García E, et al. Potential additional effect of omentectomy on metabolic syndrome, acute-phase reactants, and inflammatory mediators in grade III obese patients undergoing laparoscopic Roux-en-Y gastric bypass: a randomized trial. Diabetes Care. 2010;33(7):1413-8.
51. Andersson DP, Eriksson Hogling D, Thorell A, Toft E, Qvisth V, Näslund E, et al. Changes in subcutaneous fat cell volume and insulin sensitivity after weight loss. Diabetes Care. 2014;37(7):1831-6.
52. Denis GV, Obin MS. 'Metabolically healthy obesity': origins and implications. Mol Aspects Med. 2013;34(1):59-70.
53. Wolf RM, Jaffe AE, Steele KE, Schweitzer MA, Magnuson TH, Wolfe A, et al. Cytokine, Chemokine, and Cytokine Receptor Changes Are Associated With Metabolic Improvements After Bariatric Surgery. J Clin Endocrinol Metab. 2019;104(3):947-56.
54. Karlsson J, Taft C, Rydén A, Sjöström L, Sullivan M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes (Lond). 2007;31(8):1248-61.
55. Karlsson J, Sjöström L, Sullivan M. Swedish obese subjects (SOS)--an intervention study of obesity. Two-year follow-up of health-related quality of life (HRQL) and eating behavior after gastric surgery for severe obesity. Int J Obes Relat Metab Disord. 1998;22(2):113-26.
56. Robert M, Denis A, Badol-Van Straaten P, Jaisson-Hot I, Gouillat C. Prospective longitudinal assessment of change in health-related quality of life after adjustable gastric banding. Obes Surg. 2013;23(10):1564-70.
57. Long-Term Quality of Life Following Bariatric Surgery: A Descriptive Study. Bariatric Surgical Practice and Patient Care. 2013;8(1):29-38.
58. Cresci B, Cosentino C, Monami M, Mannucci E. Metabolic Surgery for the Treatment of Type 2 Diabetes: A Network Metanalysis of Randomized Controlled Trials. Diabetes Obes Metab. 2020.
59. Szmulewicz A, Wanis KN, Gripper A, Angriman F, Hawel J, Elnahas A, et al. Mental health quality of life after bariatric surgery: A systematic review and meta-analysis of randomized clinical trials. Clin Obes. 2019;9(1):e12290.
60. Sundbom M, Näslund E, Vidarsson B, Thorell A, Ottoson J. Low overall mortality during 10 years of bariatric surgery: nationwide study on 63,469 procedures from the Scandinavian Obesity Registry. Surg Obes Relat Dis. 2020;16(1):65-70.
61. Vidarsson B, Sundbom M, Edholm D. Incidence and treatment of small bowel leak after Roux-en-Y gastric bypass: a cohort study from the Scandinavian Obesity Surgery Registry. Surg Obes Relat Dis. 2020.
62. Froehling DA, Daniels PR, Mauck KF, Collazo-Clavell ML, Ashrani AA, Sarr MG, et al. Incidence of venous thromboembolism after bariatric surgery: a population-based cohort study. Obes Surg. 2013;23(11):1874-9.
63. Geubbels N, Lijftogt N, Fiocco M, van Leersum NJ, Wouters MW, de Brauw LM. Meta-analysis of internal herniation after gastric bypass surgery. Br J Surg. 2015;102(5):451-60.
64. Emous M, Wolffenbuttel BHR, Totté E, van Beek AP. The short- to mid-term symptom prevalence of dumping syndrome after primary gastric-bypass surgery and its impact on health-related quality of life. Surg Obes Relat Dis. 2017;13(9):1489-500.
65. Fujioka K. Follow-up of nutritional and metabolic problems after bariatric surgery. Diabetes Care. 2005;28(2):481-4.

52
66. King WC, Chen JY, Courcoulas AP, Dakin GF, Engel SG, Flum DR, et al. Alcohol and other substance use after bariatric surgery: prospective evidence from a U.S. multicenter cohort study. Surg Obes Relat Dis. 2017;13(8):1392-402.
67. Svensson MK, Lindmark S, Wiklund U, Rask P, Karlsson M, Myrin J, et al. Alterations in heart rate variability during everyday life are linked to insulin resistance. A role of dominating sympathetic over parasympathetic nerve activity? Cardiovasc Diabetol. 2016;15:91.
68. Wiklund U, Hornsten R, Karlsson M, Suhr OB, Jensen SM. Abnormal heart rate variability and subtle atrial arrhythmia in patients with familial amyloidotic polyneuropathy. Ann Noninvasive Electrocardiol. 2008;13(3):249-56.
69. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 1996;17(3):354-81.
70. Sjostrand M, Carlson K, Arnqvist HJ, Gudbjornsdottir S, Landin-Olsson M, Lindmark S, et al. Assessment of beta-cell function in young patients with type 2 diabetes: arginine-stimulated insulin secretion may reflect beta-cell reserve. J Intern Med. 2014;275(1):39-48.
71. Perseghin G, Caumo A, Caloni M, Testolin G, Luzi L. Incorporation of the fasting plasma FFA concentration into QUICKI improves its association with insulin sensitivity in nonobese individuals. J Clin Endocrinol Metab. 2001;86(10):4776-81.
72. Pereira MJ, Palming J, Rizell M, Aureliano M, Carvalho E, Svensson MK, et al. mTOR inhibition with rapamycin causes impaired insulin signalling and glucose uptake in human subcutaneous and omental adipocytes. Mol Cell Endocrinol. 2012;355(1):96-105.
73. Di Girolamo M, Mendlinger S, Fertig JW. A simple method to determine fat cell size and number in four mammalian species. The American journal of physiology. 1971;221(3):850-8.
74. Pereira MJ, Palming J, Rizell M, Aureliano M, Carvalho E, Svensson MK, et al. The immunosuppressive agents rapamycin, cyclosporin A and tacrolimus increase lipolysis, inhibit lipid storage and alter expression of genes involved in lipid metabolism in human adipose tissue. Mol Cell Endocrinol. 2013;365(2):260-9.
75. Smith U, Sjostrom L, Bjornstorp P. Comparison of two methods for determining human adipose cell size. Journal of lipid research. 1972;13(6):822-4.
76. Spalding KL, Arner E, Westermark PO, Bernard S, Buchholz BA, Bergmann O, et al. Dynamics of fat cell turnover in humans. Nature. 2008;453(7196):783-7.
77. Hays RD, Sherbourne CD, Mazel RM. The RAND 36-Item Health Survey 1.0. Health Econ. 1993;2(3):217-27.
78. Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med. 2001;33(5):350-7.
79. Hopman WM, Berger C, Joseph L, Towheed T, VandenKerkhof E, Anastassiades T, et al. The natural progression of health-related quality of life: results of a five-year prospective study of SF-36 scores in a normative population. Qual Life Res. 2006;15(3):527-36.

53
80. Wang HM, Beyer M, Gensichen J, Gerlach FM. Health-related quality of life among general practice patients with differing chronic diseases in Germany: cross sectional survey. BMC Public Health. 2008;8:246.
81. Pournaras DJ, Nygren J, Hagström-Toft E, Arner P, le Roux CW, Thorell A. Improved glucose metabolism after gastric bypass: evolution of the paradigm. Surg Obes Relat Dis. 2016;12(8):1457-65.
82. Campos GM, Rabl C, Peeva S, Ciovica R, Rao M, Schwarz JM, et al. Improvement in peripheral glucose uptake after gastric bypass surgery is observed only after substantial weight loss has occurred and correlates with the magnitude of weight lost. J Gastrointest Surg. 2010;14(1):15-23.
83. Sarr O, Strohm RJ, MacDonald TL, Gaudio N, Reed JK, Foute-Nelong J, et al. Subcutaneous and Visceral Adipose Tissue Secretions from Extremely Obese Men and Women both Acutely Suppress Muscle Insulin Signaling. Int J Mol Sci. 2017;18(5).
84. Cancello R, Zulian A, Gentilini D, Mencarelli M, Della Barba A, Maffei M, et al. Permanence of molecular features of obesity in subcutaneous adipose tissue of ex-obese subjects. Int J Obes (Lond). 2013;37(6):867-73.
85. Lundgren M, Svensson M, Lindmark S, Renstrom F, Ruge T, Eriksson JW. Fat cell enlargement is an independent marker of insulin resistance and 'hyperleptinaemia'. Diabetologia. 2007;50(3):625-33.
86. Eriksson Hogling D, Bäckdahl J, Thorell A, Rydén M, Andersson DP. Meta-bolic Impact of Body Fat Percentage Independent of Body Mass Index in Women with Obesity Remission After Gastric Bypass. Obes Surg. 2020;30(3):1086-1092.
87. Arner P, Bernard S, Salehpour M, Possnert G, Liebl J, Steier P, et al. Dynamics of human adipose lipid turnover in health and metabolic disease. Nature. 2011;478(7367):110-3.
88. Johansson L, Roos M, Kullberg J, Weis J, Ahlstrom H, Sundbom M, et al. Lipid mobilization following Roux-en-Y gastric bypass examined by magnetic resonance imaging and spectroscopy. Obes Surg. 2008;18(10):1297-304.
89. Laferrere B, Heshka S, Wang K, Khan Y, McGinty J, Teixeira J, et al. Incretin levels and effect are markedly enhanced 1 month after Roux-en-Y gastric bypass surgery in obese patients with type 2 diabetes. Diabetes Care. 2007;30(7):1709-16.
90. Van der Schueren BJ, Homel P, Alam M, Agenor K, Wang G, Reilly D, et al. Magnitude and variability of the glucagon-like peptide-1 response in patients with type 2 diabetes up to 2 years following gastric bypass surgery. Diabetes care. 2012;35(1):42-6.
91. Wu Q, Xiao Z, Cheng Z, Tian H. Changes of blood glucose and gastrointestinal hormones 4 months after Roux-en-Y gastric bypass surgery in Chinese obese type 2 diabetes patients with lower body mass index. Journal of Diabetes Investigation. 2013;4(2):214-21.
92. Kim MJ, Park HK, Byun DW, Suh KI, Hur KY. Incretin levels 1 month after laparoscopic single anastomosis gastric bypass surgery in non-morbid obese type 2 diabetes patients. Asian J Surg. 2014;37(3):130-7.
93. Korner J, Bessler M, Inabnet W, Taveras C, Holst JJ. Exaggerated glucagon-like peptide-1 and blunted glucose-dependent insulinotropic peptide secretion are associated with Roux-en-Y gastric bypass but not adjustable gastric banding. Surg Obes Relat Dis. 2007;3(6):597-601.
94. Jirapinyo P, Jin DX, Qazi T, Mishra N, Thompson CC. A Meta-Analysis of GLP-1 After Roux-En-Y Gastric Bypass: Impact of Surgical Technique and Measurement Strategy. Obes Surg. 2018;28(3):615-26.

54
95. Drucker DJ. Biological actions and therapeutic potential of the glucagon-like peptides. Gastroenterology. 2002;122(2):531-44.
96. Laferrere B, Teixeira J, McGinty J, Tran H, Egger JR, Colarusso A, et al. Effect of weight loss by gastric bypass surgery versus hypocaloric diet on glucose and incretin levels in patients with type 2 diabetes. J Clin Endocrinol Metab. 2008;93(7):2479-85.
97. Jorgensen NB, Dirksen C, Bojsen-Moller KN, Jacobsen SH, Worm D, Hansen DL, et al. Exaggerated glucagon-like peptide 1 response is important for improved beta-cell function and glucose tolerance after Roux-en-Y gastric bypass in patients with type 2 diabetes. Diabetes. 2013;62(9):3044-52.
98. Cases JA, Gabriely I, Ma XH, Yang XM, Michaeli T, Fleischer N, et al. Physiological increase in plasma leptin markedly inhibits insulin secretion in vivo. Diabetes. 2001;50(2):348-52.
99. Kadowaki T, Yamauchi T, Kubota N, Hara K, Ueki K, Tobe K. Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J Clin Invest. 2006;116(7):1784-92.
100. Ouchi N, Kihara S, Funahashi T, Matsuzawa Y, Walsh K. Obesity, adiponectin and vascular inflammatory disease. Curr Opin Lipidol. 2003;14(6):561-6.
101. Casellini CM, Parson HK, Hodges K, Edwards JF, Lieb DC, Wohlgemuth SD, et al. Bariatric Surgery Restores Cardiac and Sudomotor Autonomic C-Fiber Dysfunction towards Normal in Obese Subjects with Type 2 Diabetes. PLoS One. 2016;11(5):e0154211.
102. Colquitt JL, Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014(8):CD003641.
103. Fisher L, Tang T, Polonsky W. Assessing quality of life in diabetes: I. A practical guide to selecting the best instruments and using them wisely. Diabetes Res Clin Pract. 2017;126:278-85.
104. Norris SL. Health-related quality of life among adults with diabetes. Curr Diab Rep. 2005;5(2):124-30.
105. Fain JN, Bahouth SW, Madan AK. TNFalpha release by the nonfat cells of human adipose tissue. Int J Obes Relat Metab Disord. 2004;28(4):616-22.
106. Miller GD, Nicklas BJ, Fernandez A. Serial changes in inflammatory biomarkers after Roux-en-Y gastric bypass surgery. Surg Obes Relat Dis. 2011;7(5):618-24.
107. Richard C, Wadowski M, Goruk S, Cameron L, Sharma AM, Field CJ. Individuals with obesity and type 2 diabetes have additional immune dysfunction compared with obese individuals who are metabolically healthy. BMJ Open Diabetes Res Care. 2017;5(1):e000379.
108. Lips MA, van Klinken JB, Pijl H, Janssen I, Willems van Dijk K, Koning F, et al. Weight loss induced by very low calorie diet is associated with a more beneficial systemic inflammatory profile than by Roux-en-Y gastric bypass. Metabolism. 2016;65(11):1614-20.
109. Zhuang H, Han J, Cheng L, Liu SL. A Positive Causal Influence of IL-18 Levels on the Risk of T2DM: A Mendelian Randomization Study. Front Genet. 2019;10:295.
110. Hung J, McQuillan BM, Chapman CM, Thompson PL, Beilby JP. Elevated interleukin-18 levels are associated with the metabolic syndrome independent of obesity and insulin resistance. Arterioscler Thromb Vasc Biol. 2005;25(6):1268-73.

55
111. Schernthaner GH, Kopp HP, Kriwanek S, Krzyzanowska K, Satler M, Koppensteiner R, et al. Effect of massive weight loss induced by bariatric surgery on serum levels of interleukin-18 and monocyte-chemoattractant-protein-1 in morbid obesity. Obes Surg. 2006;16(6):709-15.
112. Subramaniam R, Aliakbarian H, Bhutta HY, Harris DA, Tavakkoli A, Sheu EG. Sleeve Gastrectomy and Roux-en-Y Gastric Bypass Attenuate Pro-inflammatory Small Intestinal Cytokine Signatures. Obes Surg. 2019;29(12):3824-32.
113. Shahi A, Afzali S, Salehi S, Aslani S, Mahmoudi M, Jamshidi A, et al. IL-27 and autoimmune rheumatologic diseases: The good, the bad, and the ugly. Int Immunopharmacol. 2020;84:106538.
114. Nam H, Ferguson BS, Stephens JM, Morrison RF. Modulation of IL-27 in adipocytes during inflammatory stress. Obesity (Silver Spring). 2016;24(1):157-66.
115. Paganelli FL, Luyer M, Hazelbag CM, Uh HW, Rogers MRC, Adriaans D, et al. Roux-Y Gastric Bypass and Sleeve Gastrectomy directly change gut microbiota composition independent of surgery type. Sci Rep. 2019;9(1):10979.
116. Carbone F, Liberale L, Bonaventura A, Vecchie A, Casula M, Cea M, et al. Regulation and Function of Extracellular Nicotinamide Phosphoribosyltransferase/Visfatin. Compr Physiol. 2017;7(2):603-21.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1672
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-416646
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020