Banks_Honors Thesis 2016
50
Running head: PREDICTIVE VALIDITY OF THE HCR-20 V3 1 Assessing the Predictive Validity of the HCR-20 V3 in Predicting Civil Psychiatric Patients’ Short-term Violence Risk Meghan Banks Fordham University
-
Upload
meghan-banks -
Category
Documents
-
view
14 -
download
2
Transcript of Banks_Honors Thesis 2016

Running head: PREDICTIVE VALIDITY OF THE HCR-20V3 1
Assessing the Predictive Validity of the HCR-20V3 in Predicting Civil Psychiatric
Patients’ Short-term Violence Risk
Meghan Banks
Fordham University

PREDICTIVE VALIDITY OF THE HCR-20V3
Abstract
Assessment and prevention of violence are critical in psychiatric settings. Clinicians have
to make decisions about their patients’ violence risk; however, their unaided clinical
judgment often results in a number of false positives. As a result, there is a considerable
need for an accurate violence screening measure. The present study assessed the
predictive accuracy of the HCR-20 Version 3 (HCR-20V3) Summary Risk ratings (SSRs)
in gauging civil psychiatric patients’ violence risk. The sample consisted of 63 civil
psychiatric patients that were admitted to an urban public psychiatric hospital. Four raters
completed the HCR-20V3 ratings within 3 weeks after the patients’ hospital admission.
Within the study period, 59 percent of civil psychiatric patients were involved in at least
one aggressive incident. There was not a significant difference in aggression occurrence,
frequency and severity between low, moderate, and high risk patients on Case
Prioritization. There was not a significant difference in aggression severity between low,
moderate, and high risk patients who engaged in severe physical harm. Although there
was not a significant difference in aggression frequency, there was a significant different
difference in aggression severity between low, moderate, and high risk patients who
engaged in imminent violence. Case Prioritization and Severe Physical Harm ratings had
weak and non-significant predictive validity. However, Imminent Violence ratings had
moderate predictive validity that approached significance. The results suggest that the
HCR-20V3 has limited predictive accuracy in identifying civil psychiatric patients’
violence risk. The implications of these results for clinical practice are discussed.
2

PREDICTIVE VALIDITY OF THE HCR-20V3
Assessment and prevention of violence are critical in psychiatric care,
management, and treatment (Chu, Daffern, & Ogloff, 2013). Clinicians often have to
make decisions about their patients’ violence risk, especially when presented with
behavioral emergencies that require psychiatric hospitalization (McNiel, Gregory, Lam,
& Binder, 2003). As a result, clinicians need to accurately gauge patients’ violence risk at
the time of psychiatric hospital admission. Although violence-screening measures are
frequent in psychiatric settings, there are well-known limitations of clinicians’ unaided
clinical judgment in assessing violence risk (McNiel, Lam, & Binder, 2000; McNiel et
al., 2003). Clinicians have modest predictive validity in assessing psychiatric patients’
violence risk; however, their assessments result in a greater likelihood of false positives
than any other type of error (Borum, 1996; Otto, 1992). A major reason for clinicians’
inability to accurately gauge psychiatric patients’ violence risk is because there is no
explicit professional standard for violence risk assessment. Consequently, there is a
considerable need for an accurate measure of violence risk, especially at the time of
hospital admission.
There are several reasons why an accurate violence-screening measure is critical
in psychiatric settings. First, psychosis is a significant factor for the occurrence of
violence within psychiatric settings (Douglas, Guy, & Hart, 2013). Psychiatric patients
are more psychotic at the time of hospitalization, and in turn have a higher propensity
towards violent behavior. Second, violence within the first few days of a psychiatric
hospitalization is a salient predictor of the length of that hospitalization (McNiel &
Binder, 1991). In relation to length of hospitalization, hospital staff often expects
violence from newly admitted patients and is less prepared for violent attacks from
3

PREDICTIVE VALIDITY OF THE HCR-20V3
patients whose stays are longer (Cooper & Mendonca, 1989; Davis, 1991). Third,
psychiatric patient violence is one of the most frequent causes of staff injuries (Carmel &
Hunter, 1989; McNiel et al., 2003). Among staff working in psychiatric settings, 44
percent of clinical staff and 72 percent of nursing staff have been subjected to psychiatric
patient violence (Bowers et al., 2011). As a result, violence inflicted onto staff members
can result in staff absence and hinder the efficiency of the psychiatric services provided
to patients. Fourth, the base rate for physical violence within psychiatric settings is
roughly 50 percent, indicating that about half of all psychiatric patients commit a
physically violent attack during hospitalization (Bowers et al., 2011). Finally, among the
psychiatric patients who engage in violence, 45 percent are involved in repeated violent
attacks with a mean rate of 5.6 attacks (Bowers et al., 2011). Thus, clinicians need to
quickly assess psychiatric patients’ violence risk in order to make decisions regarding the
level of security that is needed during hospitalization, whether to initiate civil
commitment proceedings, and whether to warn or protect third parties from any
threatened violent behavior (McNiel et al., 2003).
In view of these potential obstacles, researchers have developed several violence-
screening measures that differ in terms of content, focus, and length. Four measures have
been most commonly used and studied with regard to improving clinicians’ decision
making about psychiatric patients’ violence risk: the Violence-Screening Checklist (VSC;
McNiel & Binder, 1994), the Brøset Violence Checklist (BVC; Almvik, Woods, &
Rasmussen, 2000), The Dynamic Appraisal of Situational Aggression (DASA; Ogloff &
Daffern, 2006), and the Historical-Clinical Risk Management Version 3 (HCR-20V3;
Douglas, Hart, Webster, & Belfrage, 2014).
4

PREDICTIVE VALIDITY OF THE HCR-20V3
Violence-Screening Checklist (VSC)
McNiel and Binder (1994) developed the Violence-Screening Checklist (VSC) to
aid in the assessment of violence risk in newly admitted psychiatric patients. The VSC
contains five items that are each assigned to a one-point value: (a) history of physical
attacks or fear-inducing behavior in the two weeks prior to hospital admission; (b)
absence of suicidal behavior (e.g., attempts or gestures within two weeks before
admission); (c) schizophrenia or mania diagnosis; (d) male gender; (e) currently married
or cohabitating (McNiel & Binder, 1994). Scores of 3 or higher indicate that the patient is
at high risk for future violent behavior.
McNiel and Binder (1994) applied the VSC to sample of 338 patients admitted to
a short-term psychiatric until of a university-based hospital between 1989 and 1990. The
sample consisted of 156 females (46%) and 182 males (54%) who primarily identified as
White (71%). Most participants were diagnosed with schizophrenia (27%) and other
forms of psychosis (55%). Among the participants, 92 percent were involuntarily
committed. Patients rated as high risk on the VSC were significantly more likely to
exhibit physical attacks and aggressive behavior in the hospital than their low risk
counterparts, X2 (2, N = 338) = 27.43, p < .0001. When the outcome was violent physical
attacks, the VSC had a sensitivity of 55 percent, a specificity of 64 percent, and a total
predictive accuracy of 62 percent. Although the results were modest, the VSC performed
better than most studies of clinical judgment in assessing violence risk (McNiel &
Binder, 1994).
McNiel, Gregory, Lam, and Binder (2003) evaluate the predictive validity of the
VSC using a sample of 100 patients admitted to a short-term psychiatric unit. The sample
5

PREDICTIVE VALIDITY OF THE HCR-20V3
consisted of 53 females and 47 males with a mean age of 45.7 years (SD = 17.2). Among
the patients, 22 percent were married or cohabiting and 78 percent were single, divorced,
or widowed. The patients were identified as Caucasian (54%), Asian (19%), African
American (18%), and other ethnic backgrounds (9%). Most patients were diagnosed with
mood disorders (29%), schizophrenia (26%), substance-related disorders (27%), and
other forms of psychosis (20%). Patients were involuntarily civilly committed due to
dangerousness to others (22%), involuntarily civilly committed due to dangerousness to
self and/or grave disability (66%), or hospitalized voluntarily (11%). The VSC overall
had a significant and moderate association with the likelihood of later violence (r = .38, p
= .01). The study further assessed correlations between the items of the VSC and future
violence: history of physical attacks and/or fear-inducing behavior within 2 weeks before
hospital admission (r = .26, p < .001), absence of suicidal behavior (r = .40, p < .001),
schizophrenia or mania diagnosis (r = .39, p < .001), male gender (r = .18, p = .67), and
currently married or cohabitating (r = -.15, p = .14). At a cut-off score of 3, the VSC had
a sensitivity of 64 percent, a specificity of 80 percent, and a positive predictive value of
76 percent. The overall predictive accuracy (based on the Area Under the Curve or the
AUC statistic) was .74. Consistent with previous research, the VSC was moderately
effective in identifying patients who would and would not become violent when a score
of 2 or less was considered low risk and 3 or more was considered high risk (McNiel &
Binder, 1994; McNiel et al., 2003).
Nicholls, Ogloff, and Douglas (2004) evaluated whether there were sex
differences in the predictive accuracy of the VSC using a retrospective follow-up study.
The sample consisted of 268 involuntary psychiatric patients with 106 females and 162
6

PREDICTIVE VALIDITY OF THE HCR-20V3
males who were primarily diagnosed with schizophrenia and affective disorders.
Psychiatric patients’ psychosocial histories, institutional behavior, release plan, and
intake were used to complete their VSC scores. At a cut-off score of 3, 117 males and 25
females were considered “high risk” on the VSC. The VSC had a sensitivity of 87
percent, a specificity of 22 percent, and a positive predictive value of 47 percent for male
psychiatric patients. The VSC had a sensitivity of 29 percent, a specificity of 49 percent,
and a positive predictive value of 47 percent for female psychiatric patients. Although the
VSC had excellent sensitivity in predicting male psychiatric violence, it had relatively
poor specificity. Furthermore, the VSC had a small and non-significant predictive
accuracy in gauging female psychiatric patient violence risk (Nicholls, Ogloff, &
Douglas, 2004).
Brøset Violence Checklist (BVC)
The Brøset Violence Checklist (BVC; Almvik et al., 2000) is a six-item violence
risk measure intended to identify patients at high risk for physical violence. The BVC
measures 6 behaviors and mental states: confusion, irritability, boisterous behavior,
verbal threatening, physical threatening, and attacking objects (Almvik et al., 2000).
Scores of 1 and 2 suggest that psychiatric patient violence risk is moderate and
preventative measures should be taken. Scores of 3 or higher suggest that psychiatric
patient violence risk is very high, immediate preventative measures are required, and
plans for handling an attack should be initiated (Almvik et al., 2000).
Almvik, Woods, and Rasmussen (2000) assessed the predictive validity of the
BVC in four psychiatric hospitals in Norway. A sample of 109 patients was admitted
during a 2-month period in 1997. The sample consisted of 52 male and 57 female
7

PREDICTIVE VALIDITY OF THE HCR-20V3
psychiatric patients that were mostly involuntarily admitted (60%). Within the study
period, four male and eight female psychiatric patients were involved in a total of 33
violent incidents. When examining the distribution of BVC scores between violent and
non-violent patients, violent patients had a mean score of 2.5 (SD = 1.95) and non-violent
patients had a mean score of 0.32 (SD = 0.74). Further, there was a significant difference
between the means, indicating that violent patients scored significantly higher on the
BVC than their non-violent counterparts, t = 8.88, df = 64.39, p < .001. The study further
assessed the significance of differences in the six BVC items between violent and non-
violent patients by chi-square analysis: confusion (X2 = 43.47, p < .001), irritability (X2 =
151.40, p < .001), boisterousness (X2 = 163.54, p < .001), verbal threats (X2 = 147.17, p <
.001), physical threats (X2 = 111.93, p < .001), and attacks on objects (X2 = 176.32, p
< .001). At a cut-off score of 2, the BVC had a sensitivity of 63 percent and a specificity
of 92 percent. The BVC had an AUC of .82, indicating that the BVC had an excellent
predictive validity in gauging future psychiatric patient violence (Almvik et al., 2000).
Abderhalden, Needham, Miserez, Almvik, Dassen, and Fischer (2004) conducted
a multicenter prospective study to assess the predictive validity of the BVC in three Swiss
psychiatric hospitals. A sample of 219 patients was admitted into six acute psychiatric
wards. The sample consisted of 133 male patients (61%) and 86 female patients (39%)
who were primarily diagnosed with substance use and schizophrenic disorders. Nurses in
charge of each patient completed the BVC at the end of every shift, following a 2-week
run-in period. Within the study period, psychiatric patients committed 28 physical violent
attacks against persons. Of the 28 attacks, 4 were committed before the first rating, 14
during the prediction period, and 10 after the prediction period. The BVC had a
8

PREDICTIVE VALIDITY OF THE HCR-20V3
sensitivity of 64 percent, a specificity of 94 percent, and a positive predictive value of 11
percent. The BVC had an AUC of .88, indicating an excellent predictive validity
(Abderhalden, Needham, Miserez, Almvik, Dassen, & Fisher, 2004). Further, the results
demonstrated the general applicability of the BVC in psychiatric settings. Under periods
of extreme workload, nurses were able to complete 93 percent of the BVC forms within
less than 3 minutes (Abderhalden et al., 2004). Thus, the BVC is an effective and
efficient measure in predicting short-term psychiatric patient violence in routine care.
Abderhalden, Needham, Dassen, Halfens, Haug, and Fischer (2006) conducted a
prospective study in order to assess the predictive validity of the BVC in two Swiss
psychiatric hospitals. In order to further improve the accuracy of the BVC, the study
combined the measure with a Visual Analogue Scale (VAS). The sample consisted of 300
patients admitted during a six-month period. For three days, psychiatric nursing staff
provided assessments twice daily at 10 a.m. and 6 p.m. At the end of the study period, the
nurses combined patients’ BVC scores with the maximum value of the 12-point VAS
scale. Psychiatric patients committed 37 physical attacks within the study period. Of the
37 attacks, 27 were directed at patients. The BVC had an AUC of .90, indicating an
excellent predictive accuracy. However, when the BVC was combined with the VAS, the
predictive dropped to an AUC of .83. Thus, the BVC overall is an effective measure in
gauging short-term psychiatric patient violence, but the inclusion of the VAS appears to
hinder its predictive accuracy.
Hvidhjelm, Sestoft, Skovgaard, and Bjorner (2014) assessed the predictive
validity of the BVC in a sample of 156 Danish forensic psychiatric patients. The sample
consisted of 150 male patients (96%) and 6 female patients (4%) that were primarily
9

PREDICTIVE VALIDITY OF THE HCR-20V3
diagnosed with schizophrenic (83%) and behavioral disorders (5%). The patients’ mean
age was 38.4 years (SD = 11.1). Patients were assessed three times daily with the BVC
for 24 months. All violent incidents were recorded using the Staff Observation
Aggression Scale-Revised (SOAS-R; Nijman et al., 1999), with scores of 9 or more
indicating a violent attack. Within the study period, 419 physically violent incidents
occurred. Most violent incidents were provoked by the denial of something requested by
a patient (54.4%) and staff members were the most frequent targets of violence (78.8%).
In total, 76 patients (51%) had one or more violent incident. At a cut-off score of 2, the
BVC had a sensitivity of 80 percent, a specificity of 99 percent, and a positive predictive
value of 23 percent. At a cut-off score of 3, the BVC had a sensitivity of 95 percent, a
specificity of 99 percent, and a positive predictive value of 37 percent. The BVC across
all cut-off scores had an AUC of .92, indicating an excellent predictive validity in
gauging psychiatric patient violence risk. Thus, the BVC had a good sensitivity and
specificity in discriminating the potential for violent and non-violent acts in psychiatric
patients (Hvidhjelm, Sestoft, Skovgaard, & Bjorner, 2014).
Rechenmacher, Müller, Abderhalden, and Schulc (2014) also conducted a
prospective cohort study to assess the predictive validity of the BVC combined with the
VAS in four adult psychiatric hospitals in Austria. The sample consisted of 155 male
patients (49.6%) and 117 female patients (50.4%) that were primarily diagnosed with
mood (34.9%) and schizophrenic (20.7%) disorders. Psychiatric nursing staff rated
patients using the BVC-VAS between 10 a.m. and 11 a.m. and 6 p.m. and 7 p.m. At a
cut-off score of 7, the BVC-VAS had a sensitivity of 59 percent, a specificity of 97
percent, and a positive predictive value of 19 percent. The BVC-VAS had an AUC of .93,
10

PREDICTIVE VALIDITY OF THE HCR-20V3
indicating an excellent predictive validity in differentiating high-risk from low-risk
psychiatric patients. However, there were 7 false negative and 44 false positive cases,
resulting in the BVC-VAS having a lower sensitivity than anticipated.
Dynamic Appraisal of Situational Aggression (DASA)
The Dynamic Appraisal of Situational Aggression (DASA; Ogloff & Daffern,
2006) is a brief structured violence risk instrument developed to assess violence risk in
psychiatric patients. The DASA takes less than five minutes to be complete in psychiatric
settings (Vojt, Marshall, & Thompson, 2010). The DASA, like the BVC, assumes that
physical violence is likely to occur in the presence of aggressive behaviors (Daffern &
Howells, 2007). The seven item instrument is composed of strictly dynamic violence risk
factors: negative attitudes, impulsivity, irritability, verbal threats, sensitive to perceived
provocation, easily angered when requests are denied, and unwillingness to follow
directions (Ogloff & Daffern, 2006). Each of the seven items is scored for its presence or
absence, with scores of 6 or 7 indicating that a patient likely presents an imminent risk
for physical violence and preventative measures need to be implemented. However,
scores of 4 or more should also be considered high risk in order to initiate immediate
intervention, and in turn, reduce the likelihood of the patient engaging in physical violent
behavior (Ogloff & Daffern, 2006).
Ogloff and Daffern (2006) assessed the predictive validity of the DASA in a
sample of 100 psychiatric patients during a 6-month study period. The sample consisted
of 78 male patients and 22 female patients admitted to the Thomas Embling Hospital who
were primarily diagnosed with schizophrenic or other psychotic disorders (77%). Nursing
staff rated patients using the DASA three times daily at 7 a.m., 1 p.m., and 9 p.m. Within
11

PREDICTIVE VALIDITY OF THE HCR-20V3
the study period, psychiatric patients committed 111 physically violent incidents.
Specifically, 35 male patients (44.9%) and 15 female patients (68.2%) committed
physical violent acts. Among the violent patients, 18 percent had a DASA score of 1-3,
15 percent had a DASA score of 4-5, 55 percent had a DASA score of 6-7. And 11
percent had a DASA score of 0. When comparing nursing staff’s risk ratings with and
without the aid of the DASA, their accuracy increased when using the DASA. Further
differences in risk ratings with and without the aid of the DASA were significant X2 (2) =
33.76, p < .0001, indicating that risk ratings with the DASA were significantly more
accurate. The DASA had an AUC of .82, indicating that the measure had an good
predictive validity in differentiating violence risk between violent and non-violent
patients.
Daffern and Howells (2007) assessed the predictive validity of the DASA in
gauging imminent violence risk in patients admitted to a highly secure psychiatric
hospital. The sample consisted of 40 patients from the high secure Dangerous and Severe
Personality Disorder (DSPD) unit of the Rampton Hospital. Nursing staff rated patients’
violence risk at approximately 1 p.m. daily using the DASA during a four-month study
period. Within the study period, there were 85 incidents of physical violence. Violent
patients that had a DASA score of 0 committed 49 (57.6%) of the physically violent
incidents. At a cut-off score of 4.5, the DASA had a sensitivity of 13 percent and a
specificity of 98 percent. At a cut-off score of 6.5, the DASA had a sensitivity of 4.7
percent and a specificity of 99.6 percent. The DASA across all cut-off score had an AUC
of .65, indicating a modest, but lower than expected, predictive accuracy for violence risk
(Daffern & Howells, 2007). Overall, the DASA was a weak measure of violence risk in
12

PREDICTIVE VALIDITY OF THE HCR-20V3
this study. The authors suggested that patients with a personality disorder are more likely
to engage in instrumental violence than reactive violence when compared with mentally
ill patients (Daffern & Howells, 2007). Thus, the DASA may be an effective measure in
predicting reactive violence but less effective in predicting instrumental violence.
Vojt et al. (2010) conducted a prospective cohort study to assess the predictive
validity of the DASA in a sample of psychiatric patients. The sample consisted of 20
patients admitted to a secure hospital in Northern Ireland. All of the patients were males
primarily diagnosed with a psychotic disorder (77%). The majority of the patients were
admitted due to a violent index offense (69%), while some patients were admitted due to
an elevated risk of violence (7.7%). Within the study period, 14 incidents of physical
violence occurred with an average SOAS-R score of 9, indicating that the patients’
physically violent attacks were in general severe. In terms of physical violence, the
DASA had an AUC of .65, indicating a moderate predictive accuracy in differentiating
high risk from low risk psychiatric patients. However, the DASA showed poor predictive
validity when capturing specific victim categories of psychiatric patient violence. The
DASA had an AUC of .48 and .55 for physical violence against staff members and
patients respectively. While the DASA may be moderately effective in predictive violent
incidents in general, it does not appear to be reliable in predicting the recipient patients’
violent behavior.
Chu, Daffern, and Ogloff (2013) compared the predictive validity of the BVC and
the DASA in assessing violence risk of 70 psychiatric patients. The sample consisted of
55 male and 15 female patients that had a mean age of 30.47 years (SD = 12.42). Patients
were primarily diagnosed with psychosis (80%), substance use (74.3%), and personality
13

PREDICTIVE VALIDITY OF THE HCR-20V3
disorders (20%). When the outcome variable was limited to interpersonal violence, the
BVC had an AUC of .66, indicating a moderate to large effect size. At a cut-off score of
3, the BVC had a sensitivity of 52 percent, a specificity of 95 percent, and a positive
predictive value of 1 percent. At a cut-off score of 4, the DASA had a sensitivity of 81
percent, a specificity of 76 percent, and a positive predictive value of 4 percent. At a cut-
off score of 6, the DASA had a sensitivity of 57 percent, a specificity of 91 percent, and a
positive predictive value of 7 percent. The DASA had an AUC of .75, indicating a
comparable predictive validity to the BVC (Chu et al., 2013). Although both measures
demonstrated strong predictive validity for psychiatric patient violence, they both had
low positive predictive accuracy. Further research is needed to reduce the rate of false
positives using these measures (Chu et al., 2013).
Historical-Clinical-Risk Management-20 Version 3 (HCR-20V3)
The HCR-20 Version 3 (HCR-20V3; Douglas & Belfrage, 2014) is a structured
professional judgment (SPJ) tool designed to aid clinicians in assessing the likelihood of
violence in criminal offenders and psychiatric patients. The 20-item instrument includes
three subscales composed of violence risk factors: Historical (H), Clinical (C), and Risk
Management (R). The H subscale includes ten static violence risk factor items (e.g.,
Previous Violence, Substance Use), the C subscale includes five dynamic risk factor
items (e.g., Symptoms of Major Mental Disorder, Violent Ideation or Intent), and the R
subscale includes five risk factor items pertaining to future situational circumstances that
increase violence risk (e.g., Personal Support, Stress or Coping (Douglas & Belfrage,
2014; Douglas, Hart, Webster, & Belfrage, 2014).
14

PREDICTIVE VALIDITY OF THE HCR-20V3
Rather than using cut-off scores, clinicians arrive at categorical estimations for the
presence and relevance of each risk factor. Presence of each risk factor is rated as not
present (N), possibly or partially present (P), or definitely present (Y). Relevance
estimates the extent to which each risk factor, if present, is pertinent to the specific
patient’s violence risk. Relevance of each risk factor is rate as low, moderate, or high.
Finally, clinicians formulate summary risk ratings (SRRs) to rate case prioritization,
severe physical harm, and imminent violence as low, medium, or high risk.
Hogan and Olver (2016) assessed the predictive validity of the HCR-20V3 in
identifying violent forensic psychiatric patients. The sample consisted of 99 forensic
psychiatric patients admitted into a psychiatric hospital in western Canada from January
2005 to July 2008. The sample was predominantly male (86%) with a mean age of 36.7
years (SD = 12.8). Patients were primarily diagnosed with schizophrenia and psychotic
disorders (61%) and substance/alcohol disorders (70%). Patients were either not
criminally responsible (NCR; 52%), convicted offenders admitted for psychiatric
treatment (24%), or admitted for other services (24%). Most patients had a previous
criminal charge (70%), documented history of institutional aggression (54%), and had
committed violent index offenses (71%). The HCR-20V3 Presence and Relevance ratings
had AUC values of .76 (p < .001) and .70 (p < .001) respectively, indicating moderate to
large and significant predictive validity. Case Prioritization and Imminent Violence risk
ratings had an AUC of .68 (p < .01) and .75 (p < .001) respectively, indicating a moderate
to large and significant predictive validity. However, the Severe Physical Harm risk
rating had an AUC of .44, indicating a weak and not significant predictive validity. Thus,
the HCR-20V3 demonstrated moderate predictive accuracy; however, there is limited
15

PREDICTIVE VALIDITY OF THE HCR-20V3
research on the measure’s predictive validity for identifying violence in civil psychiatric
patients.
Despite differences among these validated violence screening measures, there is
little evidence that suggests one predicts violence risk better than the other. Because the
HCR-20V3 is widely used in assessing community violence and is often completed in
hospital settings prior to discharge, the present study assessed whether it would be useful
in also gauging short-term violence risk in civil psychiatric patients (Singh, Grann, &
Fazel, 2011).
The present study addressed four research questions. The first research question
addressed whether the HCR-20V3 Case Prioritization, Severe Physical Harm, and
Imminent Violence risk ratings would each be associated with aggression frequency and
severity among civil psychiatric patients during a 3 month follow-up period. The second
research question addressed whether the Case Prioritization rating would predict
aggression occurrence, frequency, and severity. The third research question addressed
whether the Severe Physical Harm risk rating would predict aggression severity. The
final research question addressed whether the Imminent Violence risk rating would
predict aggression frequency and severity.
Method
Participants
The sample was comprised of 63 civil psychiatric patients that were admitted to
an urban public psychiatric hospital between February and December of 2013 (described
in Howe et al., 2015). The sample consisted of 47 male (73%) and 17 female (27%)
patients ranging in age from 18 to 70 years old with a mean age of 37.97 years (SD =
16

PREDICTIVE VALIDITY OF THE HCR-20V3
13.15). Patients identified as White (14%, n = 9), Black (69% n = 44), Asian (2%, n = 1),
and mixed race/ethnicity (5%, n = 3), but some did not have race/ethnicity coded in their
charts (11%, n = 7). All patients were diagnosed with schizophrenia or schizoaffective
disorder (86%, n = 55) or a mood disorder (14%, n = 9). Patients were transferred from
acute hospitals (75%, n = 48), prison (22%, n = 14), or admitted from another location
(3%, n = 2).
Measures
The HCR-20V3 is the third edition of the HCR-20 (Douglas, Hart, Webster, &
Belfrage, 2013). The HCR-20V3 resembles the HCR-20 Version 2 in format and structure,
but differs in several specific risk factors and final SRRs. Along with presence ratings,
clinicians are also required to rate the relevance of each risk factor as low, moderate, or
high, which was not included in the preceding version. For statistical analysis purposes,
the presence and relevance ratings are converted into numerical ratings: 0 = not
present/low relevance, 1 = possibly or partially present/moderate relevance, and 2 =
present/high relevance. If a presence rating item is omitted or the item is rated as not
present, the relevance rating for the item is omitted as well. Presence and relevance
ratings are used to inform three SRRs: case prioritization, severe physical harm, and
imminent violence that are all rated as low, moderate, or high risk. Final qualitative
ratings can be converted into numerical ratings, with 1 = low risk, 2 = moderate risk, and
3 = high risk.
Procedure
Violence risk ratings for the HCR-20V3 were completed within 2 to 3 weeks after
hospital admission. The rating period for the clinical subscales was the preceding three
17

PREDICTIVE VALIDITY OF THE HCR-20V3
months. If the patient was discharged at the time the instrument was coded, the rating
period started three months before the date of discharge. Research staff coded risk
management rating based on the discharge or release plans if the patient had existing
plans to be released into the community at the time of evaluation. Data regarding
aggressive incidents was extracted from the hospital’s database. Target of aggression was
coded as 1 = patient, 2 = ward staff (e.g., TA), 3 = professional staff (e.g., clinician), 4 =
visitor, 5 = multiple targets, and 6 = other. Setting of aggression was coded as 1 = ward,
2 = treatment program, and 3 = on grounds. Aggression was coded as 1 = present and 0
= not present. Aggression frequency was coded based on the number of aggressive acts
committed by each patient. Aggression severity was coded as 1 = minimal (e.g., verbal
aggression only). 2 = moderate (e.g., physical attack without injury; threat with a
weapon), and 3 = severe (e.g., life threatening or resulting in serious injury). Aggression
occurrence, frequency, and severity were assessed during a 3-month follow-up period.
Research staff included four raters: one forensic psychologist who routinely used
the HCR-20V3 in clinical practice and three MA-level clinical psychology doctoral
students who received both didactic and supervised training in the administration and
scoring of the instrument. Raters made independent ratings for each scale and scored
instrument based on the patient’s medical record information, chart reviews, and brief
interviews with the patient’s treatment team. Out of the 64 psychiatric patients, two raters
independently rated 35 patients, finding good inter-rater reliability (Howe et al., 2015).
The Spearman correlation test was conducted to determine whether the SRRs
were significantly associated with civil psychiatric patient aggression frequency and
severity. The Chi-Square test of independence was conducted to determine whether the
18

PREDICTIVE VALIDITY OF THE HCR-20V3
Case Prioritization rating would significantly predict the occurrence of aggression during
a 3-month follow-up period. One-way ANOVA test was conducted to determine whether
the Case Prioritization and Imminence Violence risk ratings would significantly predict a
difference in aggression frequency and severity between the means of low, moderate, and
high risk patients. Another one-way ANOVA test was conducted to determine whether
the Severe Physical Harm risk ratings would significantly predict a difference in
aggression severity between the means of low, moderate, and high risk patients.
Results
During the study period, 38 of the 64 patients (59.38%) were involved in at least
one aggressive incident. Among the patients who were involved in an aggressive
incident, 6 had been rated as low risk on the HCR-20V3 Case Prioritization risk rating, 20
had been rated as moderate risk, and 12 had been rated as high risk on Case Prioritization
risk ratings. There was a weak, positive, and non-significant correlation between
aggression and Case Prioritization risk ratings, rs (61) = .10, p = .46. The occurrence of
aggression did not significantly differ by low, moderate, and high risk patients during the
3-month follow-up period, X2 (2, N = 63) = 1.14, p = .56 (Table 1).
Table 1
Cross-Tabulation of Aggression by Case Prioritization
Case Prioritization Yes No X2
Low 6 4 1.14
Moderate 20 10
High 12 11
19

PREDICTIVE VALIDITY OF THE HCR-20V3
Total 38 25
There were also no significant differences in aggression frequency between low,
moderate, and high risk patients, F (2, 62) = 0.57, p = .57. On average, patients rated as
low risk on Case Prioritization committed the least number of aggressive incidents (M =
0.40, SD = .52), ranging from 0 to 1.Patients rated as moderate risk on Case Prioritization
committed the greatest number of aggressive incidents (M = 1.27, SD = 2.96), ranging
from 0 to 12. Patients rated as high risk on Case Prioritization committed less aggressive
incidents than their moderate risk counterparts (M = 1.00, SD = 1.41), with the number of
incidents ranging from 0 to 5 (Table 2). Similarly, there were no significant differences in
aggression severity between low, moderate, and high risk patients on Case Prioritization,
F (2, 62) = .71, p = .49. Patients rated as high risk on Case Prioritization, on average, had
the highest level of aggression severity within the follow-up period (M = .96, SD = .79);
however, patients rated as low risk almost had a comparable aggression severity level as
their high risk counterparts (M = 0.90, SD = 1.20) (Table 3).
Table 2
Means and Standard Deviations of Aggression Frequency by Case Prioritization
Case Prioritization n M SD
Low 10 0.40 0.52
Moderate 30 1.27 1.05
High 23 1.00 1.41
Total 63 1.03 2.22
20

PREDICTIVE VALIDITY OF THE HCR-20V3
Table 3
Means and Standard Deviations of Aggression Severity by Case Prioritization
Case Prioritization n M SD
Low 10 0.90 1.20
Moderate 30 0.63 0.93
High 23 0.96 1.07
Total 63 0.76 1.02
There was not a significant difference in aggression severity between low,
moderate, and high risk patients with regard to engaging in severe physical harm, F (2,
62) = 1.18, p = .32. However, patients rated as high risk for engaging in severe physical
harm had the highest level of aggression severity (M = 1.40, SD = 0.89) and patients rated
as low risk had the lowest overall mean aggression severity (M = 0.67, SD = 0.99) (Table
4).
Table 4
Means and Standard Deviations of Aggression Severity by Severe Physical Harm
Severe Physical Harm n M SD
Low 33 0.67 0.99
Moderate 25 0.84 1.07
High 5 1.40 0.89
Total 63 0.79 1.02
There was not a significant difference in aggression frequency between low,
moderate, and high risk patients in engaging in imminent violence, F (2, 62) = 0.47, p
= .63. Patients rated as high risk of engaging in imminent violence committed the greatest
21

PREDICTIVE VALIDITY OF THE HCR-20V3
number of aggressive acts (M = 1.75, SD = 1.83); but there was no difference in the
frequency of aggressive acts between patients rated low and moderate risk of engaging in
imminent violence (Low: M = 0.93, SD = 2.41; Moderate: M = 0.93, SD = 2.16) (Table
5). There was a significant difference in aggression severity between low, moderate, and
high risk patients of engaging in imminent violence, F (2, 62) = 3.47, p = .03 (Table 6).
Patients rated as low risk in engaging in imminent violence had the lowest level of
aggression severity (M = 0.59, SD = .93). Patients rated as moderate risk in engaging in
imminent violence fell in between the patients rated as low and high risk in terms of
aggression severity ratings (M = 0.75; SD = 1.00). Patients rated as high risk in engaging
in imminent violence had the highest level of aggression severity (M = 1.63; SD = 1.06)
(Table 7).
Table 5
Means and Standard Deviations of Aggression Frequency by Imminent Violence
Imminent Violence n M SD
Low 27 0.93 2.42
Moderate 28 0.93 2.16
High 8 1.75 1.83
Total 63 1.03 2.22
Table 6
One-Way Analysis of Variance of Aggression Severity by Imminent Violence
Source df SS MS F p
Between groups 2 6.67 3.34 3.47 .04*
Within groups 60 57.64 0.961
22

PREDICTIVE VALIDITY OF THE HCR-20V3
Total 62 64.32
Note. *p < .05, two-tailed.
Table 7
Means and Standard Deviations of Aggression Severity by Imminent Violence
Imminent Violence n M SD
Low 27 0.59 0.93
Moderate 28 0.75 1.05
High 8 1.63 1.06
Total 63 0.79 1.02
There was a weak, positive, and non-significant association between aggression
frequency and severity and Case Prioritization ratings, rs = .13, p = .32 and rs = .08, p
= .53, respectively. Similarly, there was a weak, positive, and non-significant association
between aggression frequency and severity and risk of engaging in serious physical harm
ratings, rs = .19, p = .19 and rs = .17, p = .19, respectively. There was a weak positive
association between aggression frequency and risk of engaging in imminent violence, rs =
.22, p = .08, that approached significance. However, there was a positive significant
association between aggression severity and risk of engaging in imminent violence, rs
= .25, p = .03 (Table 8).
Table 8
Spearman Correlations between SRRs and Aggression Frequency and Severity
SRRs Frequency Severity
Case Prioritization .13 .08
Severe Physical Harm .19 .17
23

PREDICTIVE VALIDITY OF THE HCR-20V3
Imminent Violence .22 .25*
Note. *p < .05, two-tailed.
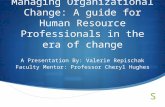
When predictive accuracy was gauged using Receiver Operating Characteristic
(ROC) curve analysis, Case Prioritization and Severe Physical Harm ratings had a weak
and non-significant predictive validity, AUC = .55, p = .49 and AUC = .60, p = .49,
respectively. However, Imminent Violence risk ratings had a moderate predictive validity
that approached significance, AUC = .63, p = .08 (Figure 1).
Discussion
The aim of the current study was to assess the predictive validity of the
HCR-20V3 Summary Risk Ratings (SRRs) in gauging violence risk in civil psychiatric
patients. As evident from previous research, there is a high base rate for patient
aggression within psychiatric settings (Bowers et al., 2011). In this study, more than half
of the sample committed at least one aggressive incident, however, severe aggression was
not very common. Thus, there were only a handful of moderately severe aggressive acts,
which were not life threatening.
However, contrary to expectations, the HCR-20V3 was not an effective measure at
predicting aggression within this civil psychiatric setting. The Case Prioritization SRR
demonstrated particularly weak predictive validity in gauging violence risk. Likewise, the
Severe Physical Harm SRR also demonstrated weak predictive validity in gauging
violence risk, and was not a significant predictor of severity of violence. However, the
pattern of findings indicated greater violence severity among those patients thought to be
at high risk for severe violence and lower levels of violence severity among those deemed
to be at low risk. The Imminent Violence SRR also demonstrated moderate predictive
24

PREDICTIVE VALIDITY OF THE HCR-20V3
validity with regard to severity of violence, though it was still weakly associated with
aggression in this sample of civil psychiatric patients.
Although the HCR-20V3 SRRs’ showed limited predictive validity, the study had
several limitations. While the HCR-20V3 seems to have excellent predictive accuracy in
community and forensic settings, it demonstrated poor predictive accuracy within the
sample of civil psychiatric patients. Perhaps the HCR-20V3 risk factors were not relevant
to this sample of civil psychiatric patients. As well, the study’s definition of violence
encompassed both verbal and life threatening physical aggression, which may have been
too broad to be captured adequately by the HCR-20V3. Although the sample had a high
rate of aggression, its low aggression severity may have impacted the predictive validity
of the SRRs. This could also be due the study’s low threshold for identifying aggressive
behavior or that the facility primarily focused on highly aggressive patients that could not
be managed elsewhere. Finally, the study did not compare the predictive validity of the
BVC, DASA, VSC, and HCR-20V3 in gauging violence risk within the sample. As a
result, the poor predictive accuracy demonstrated could be due to the HCR-20V3,
inaccuracy in the ratings of the research team, or the civil psychiatric setting itself.
The sample size also limited the study’s statistical power. Although 38 out of 63
patients engaged in some type of aggressive behavior, the overall sample size of 63 was
still modest. As a result, the study was unable to look at potentially important variables,
such as the differential risk for violence between diagnostic categories or gender. As
well, the sample size was too small to analyze victim characteristics (e.g., patient versus
staff) or the setting of civil psychiatric patient violence (e.g., hospital, grounds,
community).
25

PREDICTIVE VALIDITY OF THE HCR-20V3
The sample’s characteristics were an additional limitation. Patients were
hospitalized in a public psychiatric facility that provided long-term care. Although the
sample was representative of chronic psychiatric patients in most urban psychiatric
settings, there was little to no variability in diagnosis (e.g., all patients suffered from and
had active symptoms of a major mental disorder). This lack of variability could have
prevented an analysis of some items related to the SRRs (e.g., presence of a mental
disorder; Howe et al., 2015). Finally, the HCR-20V3 ratings were based on chart reviews
and interviews with the treatment teams, not clinical interviews with the patients
themselves. A reliance on charts to assess the final SRRs may have had an adverse
impact on information about patients’ future plans and propensity to commit an
aggressive act.
The study’s findings, while in general not significant, revealed some
counterintuitive trends of civil psychiatric patient violence. For example, low and
moderate risk patients were the most likely to engage in any aggression and accounted
for more aggressive incidents than high risk patients. This could be due to the facility’s
allocation of primary and aggressive treatment. High risk patients more likely to receive
the most aggressive interventions, which in turn, could have impacted the subsequent
severity of aggression and predictive accuracy of the HCR-20V3 within the sample.
Although the results suggest that the HCR-20V3 is not an accurate measure in
identifying high risk patient aggression, the current study underscores the aggressive
behavior of chronically ill patients in civil psychiatric settings. Future research should
compare the predictive accuracy of several violence screening measures in order to
determine which measure is the most effective in gauging short-term psychiatric patient
26

PREDICTIVE VALIDITY OF THE HCR-20V3
violence risk. By determining which measures provide the strongest predictive accuracy,
the number and severity of violent attacks committed by chronically ill patients can be
decreased. Future research should explore the predictive accuracy of the HCR-20V3 SRRs
in capturing violence risk across gender, diagnostic, victim, and setting categories. As
well, future research should explore the predictive accuracy in capturing civil psychiatric
patients’ unprovoked and retaliated forms of violence. Finally, clinicians need to focus on
the behavioral interventions provided to psychiatric patients rated as moderate risk.
Moderate risk psychiatric patients are still at a high risk for inpatient aggression, perhaps
because more aggressive interventions are prioritized to high risk patients. Thus, the
current study revealed the poor predictive accuracy of the HCR-20V3, but provides
clinical implications for future practice within psychiatric settings.
27

PREDICTIVE VALIDITY OF THE HCR-20V3
References
Abderhalden, C., Needham, I., Miserez, B., Almvik, R., Dassen, T., Haug, H. J., &
Fischer, J. E. (2004). Predicting inpatient violence in acute psychiatric wards
using the Brøset‐Violence‐Checklist: a multicentre prospective cohort study.
Journal of Psychiatric and Mental Health Nursing, 11(4), 422-427.
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Haug, H. J., & Fischer, J. (2006).
Predicting inpatient violence using an extended version of the Brøset-Violence-
Checklist: instrument development and clinical application. BMC psychiatry,
6(1), 17.
Borum, R. (1996). Improving the clinical practice of violence risk assessment:
Technology, guidelines, and training. American Psychologist, 51(9), 945.
Bowers, L., Stewart, D., Papadopoulos, C., Dack, C., Ross, J., Khanom, H., & Jeffery, D.
(2011). Inpatient violence and aggression: a literature review. Report from the
conflict and containment reduction research programme. Institute of Psychiatry,
Kings College London doi: http://www. kcl. ac.
uk/iop/depts/hspr/research/ciemh/mhn/projects/litreview/LitRevAg g. pdf.
Chu, C. M., Daffern, M., & Ogloff, J. R. (2013). Predicting aggression in acute
inpatient psychiatric setting using BVC, DASA, and HCR-20 Clinical scale. The
Journal of Forensic Psychiatry & Psychology, 24(2), 269- 285.
Cooper, A. J., & Mendonca, J. D. (1989). A prospective study of patient assaults on
nursing staff in a psychogeriatric unit. The Canadian Journal of Psychiatry/La
Revue canadienne de psychiatrie.
28

PREDICTIVE VALIDITY OF THE HCR-20V3
Daffern, M., & Howells, K. (2007). The prediction of imminent aggression and self-harm
in personality disordered patients of a high security hospital using the HCR-20
clinical scale and the dynamic appraisal of situational aggression. International
Journal of Forensic Mental Health, 6(2), 137-143.
Davis, S. (1991). Violence by psychiatric inpatients: a review. Psychiatric Services,
42(6), 585-590.
Douglas, K. S., & Belfrage, H. (2014). Inter-rater reliability and concurrent validity of the
HCR-20 Version 3. International Journal of Forensic Mental Health, 13(2), 130-
139.
Douglas, K. S., Hart, S. D., Webster, C. D., & Belfrage, H. (2013). HCR-20 V3
Historical, Clinical, Risk Management (Version 3): Professional guidelines for
evaluating risk of violence.
Douglas, K. S., Hart, S. D., Webster, C. D., Belfrage, H., Guy, L. S., & Wilson, C. M.
(2014). Historical-Clinical-Risk Management-20, Version 3 (HCR-20V3):
Development and Overview. International Journal of Forensic Mental Health,
13(2), 93-108.
Guy, L. S., Wilson, C. M., Douglas, K. S., Hart, S. D., Webster, C. D., & Belfrage, H.
(2013). HCR-20 Version 3: Item-by-item summary of violence literature. HCR-20
Violence Risk Assessment White Paper Series,# 3. Burnaby, Canada: Mental
Health. Law, and Policy Institute, Simon Fraser University.
Howe, J., Rosenfeld, B., Foellmi, M., Stern, S., & Rotter, M. (2016). Application of the
HCR-20 version 3 in civil psychiatric patients. Criminal Justice and Behavior,
43(3), 398-412.
29

PREDICTIVE VALIDITY OF THE HCR-20V3
Hvidhjelm, J., Sestoft, D., Skovgaard, L. T., & Bjorner, J. B. (2014). Sensitivity and
specificity of the Brøset Violence Checklist as predictor of violence in forensic
psychiatry. Nordic Journal Of Psychiatry, 68(8), 536-542.
doi:10.3109/08039488.2014.880942
McNiel, D. E., & Binder, R. L. (1994). Screening for risk of inpatient violence. Law and
Human Behavior, 18(5), 579-586.
McNiel, D. E., Gregory, A. L., Lam, J. N., Binder, R. L., & Sullivan, G. R. (2003).
Utility of decision support tools for assessing acute risk of violence. Journal of
consulting and clinical psychology, 71(5), 945.
Nicholls, T. L., Ogloff, J. R., & Douglas, K. S. (2004). Assessing risk for violence among
male and female civil psychiatric patients: the HCR‐20, PCL: SV, and VSC.
Behavioral sciences & the law, 22(1), 127-158.
Ogloff, J. R., & Daffern, M. (2006). The dynamic appraisal of situational aggression: An
instrument to assess risk for imminent aggression in psychiatric inpatients.
Behavioral sciences & the law, 24(6), 799-813.
Rechenmacher, J., Müller, G., Abderhalden, C., & Schulc, E. (2014). The diagnostic
efficiency of the extended German Brøset Violence Checklist to assess the risk of
violence. Journal Of Nursing Measurement, 22(2), 201-212. doi:10.1891/1061-
3749.22.2.201
Singh, J. P., Grann, M., & Fazel, S. (2011). A comparative study of violence risk
assessment tools: A systematic review and metaregression analysis of 68 studies
involving 25,980 participants. Clinical psychology review, 31(3), 499-513.
30

PREDICTIVE VALIDITY OF THE HCR-20V3
Appendix
Figure 1. ROC curves of Summary Risk Ratings.
31