bahan p. samsirun.pptx
39
Dr Samsirun Halim SpPD KIC
-
Upload
fitria-shizuoka-jiyeon -
Category
Documents
-
view
9 -
download
0
Transcript of bahan p. samsirun.pptx
Dr Samsirun Halim SpPD KIC1Primary hypertension accounts for approximately 90-95% of patients diagnosed with hypertension. Unlike secondary hypertension, there is no known cause of primary hypertension. Despite many years of active research, there is no unifying hypothesis to account for the pathogenesis of primary hypertension. There is a natural progression of this disease that suggests early elevations in blood volume and cardiac output might initiate subsequent changes in the systemic vasculature (increased resistance). This has suggested to some researchers that a basic underlying defect in many hypertensive patients is an inability of the kidneys to adequately handle sodium. Increased sodium retention could then account for the increase in blood volume. In chronic, long-standing hypertension, blood volume and cardiac output are often normal, therefore the hypertension is sustained by an elevation in systemic vascular resistance rather than by an increase in cardiac output. This increased resistance is caused by a thickening of the walls of resistance vessels and by a reduction in lumen diameters. There is also evidence for increased vascular tone. This could be mediated by enhanced sympathetic activity or by increased circulating levels of angiotensin II. In recent years, considerable evidence has suggested that changes in vascular endothelial function may cause the increase in vascular tone outlineSelayang pandang hipertensiDefinisiPatofisiologi etiologiCara pengukuran tensiDerajat hipertensiKomplikasipengobatan
Global Leading Risks for Death, 2010Systolic blood pressure > 115 mmHgGlobal Burden of Disease Study 2010 , Lancet 2012; 380: 222460Increased blood pressure is the leading risk for death and disability globally according to the Global Burden of Disease Study published in 2012 3Prevalensi hipertensi sesuai umurumur18-2930-3940-4950-5960-6970-7980+% Hypertensi41121445464654Can you see that age is a risk factor?Hypertension Prevalence in Canada Source: Public Health Agency of Canada using CCDSS Data Report from the Canadian Chronic Disease Surveillance System (CCDSS) reveals that 22.7% of adults aged over 20 years has hypertension and that the prevalence increases with age. Hypertension affects over 1 in 5 adult Canadians (an estimated 7.4 million people in 2012/13) and another 1 in 5 have high normal blood pressureIt is estimated that over 90% of people will develop hypertension if they live an average lifespan (based on data from Framingham Heart Study)
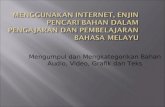
5Blood Pressure & CVD Risk Lewington et al. Prospective Studies Collaboration. Lancet. 2002;360:1903-13.
Data from study by Lewington et al. (2002) which examined effects of blood pressure and mortality in 1 million adults Shows the relationship between increasing blood pressure and stroke death. It shows that there is a log-linear relationship between systolic blood pressure and stroke death in different age groups. The data for cardiac mortality is very similar and is also presented in the same manuscript.6Blood Pressure as a Cardiovascular RiskAttributable Risk Overall of heart and stroke*Stroke 60-70%*Heart failure 50%Heart attack 25%Kidney failure 20%DementiaSexual dysfunction7* Systolic blood pressure greater than 115 mmHgThis slide shows the proportion of different vascular diseases that are related to high blood pressure. Note that for some of them the risk is indicated for systolic blood pressure above 115 mm Hg, while for heart failure, heart attack and kidney failure the risk indicated on this slide is for the current definition of hypertension ( >140/90 mm Hg).* Defined as death due to CV disease; recognized myocardial infarction (MI), stroke, or congestive heart failure (CHF). Adapted from Vasan RS. N Engl J Med. 2001;345:1291-1297.Cumulative Incidence (%)of Major CV Events1612108642014024681012Time (y)Optimal BP( 160or > 1002007 European Societies of HTN and Cardiology: Classification of HTNBP ClassificationSBP mmHgDBP mmHgOptimal BP< 120 < 80Normal120 - 129and /or 80 - 84High Normal130 - 139and /or 85 - 89Grade 1140 - 159and / or 90 - 99Grade 2160 - 179and / or 100 - 109Grade 3> 180 and / or > 110Isolated Systolic HTN140< 90Mancia, G. et al. 2007 Guidelines for the Management of Arterial HTN: The Task Force for the Management of Arterial HTN of the Euro Soc of HTN (ESH) and of the Euro Soc of Card (ESC). J HTN 2007; 25: 1105.
Tensi yang tak terkontrol akan menyebabkan:Arteriosklerosis--kerusakan ginjalSerangan jantung--StrokePembesaran jantung--Kebutaan
Kerusakan organ target Jantung pembesaran ventrikel kiri Angina / prior MI perlu revascularisasi awal gagal jantung otak Stroke or transient ischemic attack Dementia gagal ginjal kronik penyakit pembuluh darah perifer Retinopathy
The physical examination should include: an appropriate measurement of BP, with verification in the contralateral arm; an examination of the optic fundi; a calculation of body mass index (BMI) (measurement of waist circumference is also very useful); an auscultation for carotid, abdominal, and femoral bruits; a palpation of the thyroid gland; a thorough examination of the heart and lungs; an examination of the abdomen for enlarged kidneys, masses, distended urinary bladder, and abnormal aortic pulsation; a palpation of the lower extremities for edema and pulses; andneurological assessment. NICE:For people aged under 40 years with stage 1 hypertension and noevidence of target organ damage, cardiovascular disease, renal disease ordiabetes, consider seeking specialist evaluation of secondary causes ofhypertension and a more detailed assessment of potential target organdamage. This is because 10-year cardiovascular risk assessments canunderestimate the lifetime risk of cardiovascular events in these people.[new 2011]17Bagaimana gejala darah tinggi?Tanpa gejalaKeluhan : sakit kepala, pusing, mimisen,cepat marah telinga berdenging, sukar tidur, sesak nafas rasa berat di tengkuk komplikasi : gangguan penglihatan gangguan fungsi ginjal gangguan fungsi jantung gangguan fungsi saraf
Apa yang harus kita lakukan kalau sudah diberi tahu darah tinggi Periksa ke dokter Untuk mengetahui apakah sudah ada kerusakan pada :Otak dan sarafMataJantung dan pembuluh darahGinjal
Identify CVD Risk Factors Age Hypertension Diabetes mellitus Elevated LDL or low HDL Estimated GFR < 60 mL / min Family history of premature CVD Microalbuminuria Obesity Physical inactivity Tobacco usage, particularly cigarettes
JNC VII: age 55 in male age 65 in female; ATP III age >45 male; female >55.21Stratification of total CV riskFour categories :
- Low- Moderate- High- Very high refer to 10 year risk of fatal or non-fatal CV event
Treatment Both GuidelinesModificationRecommendation~BP ReductionWeight Reduction
Maintain Normal Wgt5 - 20 mmHg / 10 kg weight lossDietary Approaches to Stop HTN ( DASH )Diet rich in fruits, vegs, low fat dairy, & dec fat8 - 14 mmHgDietary Na+ Reduction2.4g Na+ or 6g NaCl **1.5g Na+ / day 2 - 8 mmHgPhysical ActivityAerobic exercise 30 mins almost daily4 - 9 mmHgETOH Consumption2 drinks / day Men1 drink / day Women2 - 4 mmHgOFFER TO ALL STAGES: MAY BE ONLY TREATMENT RENDERED FOR STAGE 1 FOR A YEAR PER NICE GUIDELINESDont use K+, Magnesium, K+ supplements to decrease. Moderate caffeine intake to less than 5 cups per day. Can try lifestyle modifications for a year at a time if you lact: Target Organ Damage,