Avitene granulomas of colonic serosa - Annals of Clinical ... · PDF fileAvitene Granulomas of...
7
ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 16, No. 4 Copyright © 1986, Institute for Clinical Science, Inc. Avitene Granulomas ofColonic Serosa* DOUGLAS H. McGREGOR, MD.t RICHARD I. MacARTHUR, M D,t and TONY CARTER, MD§ Laboratoryf and Surgicalt§ Services, Veterans Administration Medical Center, Kansas City, MO 64128 and Department of Pathology and Oncologyt and Department of Surgery,$ University of Kansas Medical Center, Kansas City, KS 66103 ABSTRACT Avitene, microfibrillar collagen hemostat, is an absorbable topical hemostatic agent prepared from purified bovine corium collagen. A case is reported of a 58-year-old man who, one month after sigmoid colectomy for volvulus in which Avitene was used to control bleeding from a splenic capsular tear, developed symptoms of intestinal obstruction. On explor- atory laparotomy, the transverse and descending colon had numerous 0.1 to 2.0 cm nodules, adherent to the serosa of the bowel and mesentery, with kinking and partial obstruction of the splenic flexure. Light micro- scopically, the nodules were found to be composed of chronic inflamma- tory and granulomatous reaction with numerous deposits of eosinophilic fibrillar material consistent with Avitene. Electron microscopic examina- tion of the lesions and of Avitene confirmed the nature of this material. The practical and pathobiological implications of utilization of Avitene as a hemostatic agent are discussed. Introduction Avitene, microfibrillar collagen hemostat, is an absorbable topical hemostatic agent prepared as a dry, ster- ile, fibrous, water insoluble partial hydrochloric acid salt of purified bovine corium collagen.2,5,12 This substance, when in contact with a bleeding surface, attracts platelets which adhere to the * Address for correspondence: Dr. D. H. McGre- gor, Laboratory Service, Veterans Administration Medical Center, 4801 Linwood Boulevard, Kansas City, MO 64128. fibrils and undergo the release phenom- enon to trigger aggregation of platelets into thrombi in the interstices of the col- lagenous mass.7 Avitene is indicated for use in surgical procedures as an adjunct to hemostasis when control of bleeding by ligature or conventional procedures is ineffective or impractical.6,12,14 It has been found especially useful in control- ling generalized bleeding from raw or friable tissues, bleeding from highly vas- cularized organs, bleeding from cancel- lous bone, and bleeding around vascular anastomoses. 296 0091-7370/86/0700-0296 $01.20 © Institute for Clinical Science, Inc.
-
Upload
truongtram -
Category
Documents
-
view
217 -
download
1
Transcript of Avitene granulomas of colonic serosa - Annals of Clinical ... · PDF fileAvitene Granulomas of...

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 16, No. 4 Copyright © 1986, Institu te for Clinical Science, Inc.
Avitene Granulomas of Colonic Serosa*DOUGLAS H. McGREGOR, M D .t RICHARD I. MacARTHUR, M D ,t and TONY CARTER, MD§
Laboratoryf and Surgicalt§ Services, Veterans Administration Medical Center,
Kansas City, MO 64128 and Department of Pathology and Oncologyt
and Department of Surgery,$ University of Kansas Medical Center,
Kansas City, KS 66103
ABSTRACTA vitene, m icrofibrillar collagen hem ostat, is an absorbable topical
hem ostatic agent prepared from purified bovine corium collagen. A case is reported of a 58-year-old man who, one m onth after sigmoid colectomy for volvulus in which Avitene was used to control bleeding from a splenic capsular tear, developed symptoms of intestinal obstruction. On exploratory laparotomy, the transverse and descending colon had num erous 0.1 to 2.0 cm nodules, adherent to the serosa of the bowel and mesentery, with kinking and partial obstruction of the splenic flexure. Light microscopically, the nodules w ere found to be composed of chronic inflammatory and granulom atous reaction with num erous deposits of eosinophilic fibrillar m aterial consistent with Avitene. Electron microscopic examination of the lesions and of Avitene confirmed the nature of this material. The practical and pathobiological implications of utilization of Avitene as a hem ostatic agent are discussed.
IntroductionA v ite n e , m ic ro f ib r i l la r c o lla g e n
h e m o s ta t, is an a b so rb a b le to p ica l hemostatic agent p repared as a dry, sterile , f ib ro u s, w a te r in so lu b le p a rtia l hydrochloric acid salt of purified bovine corium co llagen .2,5,12 This substance, when in contact with a bleeding surface, attracts p la te le ts w hich ad h ere to the
* Address for correspondence: Dr. D. H. McGregor, Laboratory Service, Veterans Administration Medical Center, 4801 Linwood Boulevard, Kansas City, MO 64128.
fibrils and undergo the release phenom enon to trigger aggregation of platelets into throm bi in the interstices of the collagenous m ass.7 Avitene is indicated for use in surgical procedures as an adjunct to hemostasis w hen control of bleeding by ligature or conventional procedures is ineffective or im practica l.6,12,14 It has been found especially useful in controlling generalized b leeding from raw or friable tissues, bleeding from highly vascularized organs, b leeding from cancellous bone, and bleeding around vascular anastomoses.
2960091-7370/86/0700-0296 $01.20 © Institute for Clinical Science, Inc.

A V IT E N E G R A N U L O M A S O F C O L O N 2 9 7
The case reported here is an unusual example of intestinal obstruction caused in p a rt by reac tio n to A vitene. This m icrofib rilla r co llagen h em o sta t had been used one m onth previously during surgery on this patien t to control b leeding from a small splenic capsular tear. Pathologically, the cause of the marked foreign body granulom atous reaction, chronic inflam m ation and fibrosis in the colonic serosa was determ ined by light and electron m icroscopic study of the colonic serosal lesions, in com parison w ith lig h t an d e le c tro n m icroscop ic study of commercially available Avitene.
Case HistoryThe patient was a 58-year-old black male. One
month prior to admission, he had a reduction of sigmoid volvulus and a sigmoid colectomy with end-to- end colocolostomy. During this procedure, a small splenic capsular tear had been noted, and bleeding from this tear had been successfully controlled with Avitene and pressure. The Avitene had been applied with forceps and packed with a sponge. On the day of admission the p a tien t developed acute onset of abdominal pain and vomiting. Physical examination demonstrated moderate abdominal distention with tenderness on p ressu re and hyperactive bowel sounds. Upright abdominal x-ray showed distention of small bowel loops.
Exploratory laparotomy was performed, and two problems were identified. Firstly, the ascending colon was attached by adhesions to the sigmoid colon anastomatic region resulting in an internal hernia and consequent small bowel obstruction; these adhesions were taken down, and one was biopsied. Secondly, the mid-transverse to m id-descending colon had numerous 0.1 to 2.0 cm nodules, adherent to the serosa of the bowel and mesentery, with kinking and partial obstruction of the splenic flexure. Three of these nodules were biopsied. The splenic capsular tear was noted to be well healed. Postoperative course was uneventfu l and th e pa tien t was discharged three weeks after surgery free of abdominal or gastrointestinal symptoms. There has been no further evidence of intestinal obstruction during the subsequent four years.
Materials and MethodsSpecimens for light microscopic study,
in c lu d in g p o rtio n s of one ascen d in g colonic adhesion, th ree splenic flexure nodu les, and com m ercia lly o b ta ined A vitene, w ere fixed in form alin, ro u
tinely processed for histologic sectioning and s ta in ed w ith hem atoxy lin -eosin , M asson’s trich ro m e, phospho tungstic ac id -h em a to x y lin , an d p e rio d ic acid Sell ill {PAS).
Specim ens for e lec tron m icroscopic study, including portions of ascending colonic adhesion, splenic flexure nodules, and com m ercially ob ta ined Avitene, w ere fixed in four percent glutaral- dehyde in 0.1 M phosphate buffer at pH 7.4. These w ere postfixed in one percent osmium tetroxide in 0.1 M phosphate buffer, routinely processed, and em bedded in epoxy resin. U ltrathin sections were stained with a saturated solution of uranyl acetate and lead citrate and examined in an electron microscope.
ResultsG r o s s Pa t h o l o g y
The specim en consisted of th ree ovoid nodules of soft tissue and one irregular elongated piece of soft tissue (figure 1). The th ree ovoid nodules (obtained from transverse colonic serosa) m easured 2 X l x l cm ., 1.5 X 1 x 1 cm. and 0.9 X 0.6 x 0.5 cm in greatest dim ensions. They had an irregular m ottled pale red dish brown and yellow external surface, and a rubbery hom ogeneous pale tan cut su rface . T h e o n e e lo n g a te d n o d u le (obtained from the sigmoid colon anastomotic region) m easured 1.3 X 0.5 X 0.4 cm and was similar in color.
L ig h t M ic r o s c o p y
Hematoxylin-eosin stained sections of the th ree transverse colonic specimens (figures 2, 3, and 4) showed serosal adipose tissue extensively involved by large and sm all n o d u la r p ro life ra tio n s of fibrous tissue with m oderate to marked chronic inflam m atory cell infiltrate and num erous sm all and large deposits of eosinophilic m ateria l frequen tly asso-

2 9 8 M cG R E G O R , M acA R T H U R , A N D C A R T E R
^ , '. ?
J, y *
I B
« tu
w a tò r È n;p|ll|[!tljH|H,li|ll liil Iff

A V IT E N E G R A N U L O M A S O F C O L O N 2 9 9
ciated with foreign body giant cells. The inflam m atory cell infiltrate was mainly com posed of eosinoph ils w ith in te r spersed plasm a cells, lym phocytes and histiocytes. The eosinophilic m aterial was variably am orphous and coarsely fibrillar and occurred as m inute to large irregular accumulations. The color of this m aterial varied from in tensely eosinophilic (similar to normal collagen) to less eosinophilic to somewhat pale gray and faintly basophilic. The m ore intensely eosinophilic areas tended to appear blue on trichrom e stain and under polarized light to have a pink birefrigence similar to normal collagen, while the less eosinophilic areas tended to lack these collagenous ch arac teris tics . No fib rin was identified in PTAH-stained sections.
Hematoxylin-eosin stained sections of the sigmoid colon anastomotic specimen show ed serosal ad ipose tissu e e x ten sively involved by fibrosis with scattered capillaries, patchy recen t hem orrhage, minimal focal lymphocytic infiltrate and one suture granuloma. The intercellular m aterial in this specim en consistently dem onstrated a blue color on trichrom e s ta in and p in k b ire fr in g e n c e u n d e r polarized light, typical of normal collagen.
Hematoxylin-eosin stained sections of commercially available Avitene (figure 5) showed material similar to that seen in the transverse colonic specimens, except that it was less am orphous and m ore consistently composed of thick strands of intensely eosinophilic m aterial and narrow coarse fibers of less intensely eosinophilic material with a faintly basophilic hue. This m aterial foeally stained blue w ith tr ic h ro m e s ta in an d th e th ick
intensely eosinophilic m aterial showed a pink birefringence under polarized light.
E l e c t r o n M ic r o s c o p y
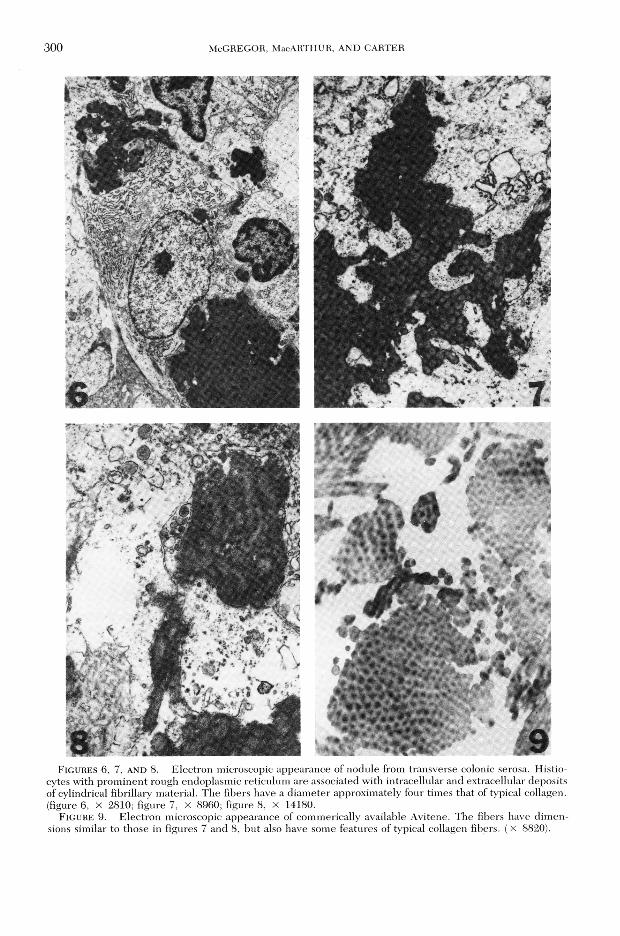
On electron microscopic study (figures 6, 7, and 8), the transverse colonic granu lom atous le s io n s w ere fo und to be m ainly com posed of h istiocy tes w ith sc a tte red eosinoph ils and occasional lymphocytes. The histiocytes generally had a m oderate to m arked increase in rough endoplasmic reticulum . The most notable feature of the lesions, however, was the num erous small and large irregularly shaped accumulations of electron dense material, which was adjacent to, partially engulfed by and occasionally phagocytized by the histiocytes. This material was composed of regular cylindrical, m oderately electron dense fibers, approximately four times the d iam eter of typical collagen, within a small am ount of highly electron dense matrix.
U ltrastructural study of commercially o b ta in e d A v iten e (figure 9) d e m o n strated it to be com posed of two main forms of fibrillary material: (1) discrete b und les of cy lind rica l p a ra lle l fibers about four times the d iam eter of normal collagen, on cross section having a dark central core and pale outer layer and on longitudinal section having a periodicity much finer than that of normal collagen; and (2) loosely a rra n g e d cy lin d rica l fibers, sim ilar to those com posing the above discrete bundles except for being more electron-dense and less parallel in arrangem ent. There was focal transition betw een the d iscrete bundles of fibers and th e loosely a rran g ed fibers. T he fibrillary material which had been seen
F i g u r e 1. External (a) and cut (b) surfaces of three nodules removed from transverse colonic serosa. The fourth tissue (lower right) is fibrous tissue removed from sigmoid colon anastomotic region.
F i g u r e s 2 , 3 AND 4 . Medium, low, and high power views of nodule from transverse colonic serosa. Multiple irregular deposits of amorphous and coarsely fibrillar material are dispersed about fibrous tissue with granulomatous reaction and chronic inflammation.
F i g u r e 5 . H i g h p o w e r v i e w o f s e c t i o n o f c o m m e r c i a l l y a v a i l a b l e A v i t e n e , s i m i l a r in a p p e a r a n c e t o t h e m a t e r i a l i n f ig u r e 4 .
300 M cG R E G O R , M acA R T H U R , A N D C A R T E R
FIG U R ES 6, 7, AND 8. Electron microscopic appearance of nodule from transverse colonic serosa. Histiocytes with prom inent rough endoplasmic reticulum are associated with intracellular and extracellular deposits of cylindrical fibrillary material. The fibers have a diam eter approximately four times that of typical collagen, (figure 6, x 2810; figure 7, x 8960; figure 8, x 14180.
Figure 9. E lectron microscopic appearance of commerically available Avitene. The fibers have dim ensions similar to those in figures 7 and 8, but also have some features of typical collagen fibers. (X 8820).

A V IT E N E G R A N U L O M A S O F C O L O N 30 1
in the pericolonic granulomas was similar to the loosely arranged fibers of Avi- tene, except for the former fibers being em bedded in a small am ount of highly e le c tro n -d e n se m atrix and h av ing a finely m icrofibrillary tex ture w ith very little evidence of periodicity on longitud inal section . T he p rev ious findings w ere felt to be consistent with the conclusion that the pericolonic granulomas rep resen ted a foreign body reaction to Avitene.
Electron microscopic study of the sigmoid colonic anastomotic specimen (pericolonic fibrotic area separate from the transverse colonic granulomas) dem onstra ted reactive fibrocyte proliferation and collagen deposition. The collagen fibers w ere typical in diam eter and periodicity and had a d iam eter about four times less than Avitene and the material in the granulomas. This was felt to indicate that the nature of the collagenous m aterial com posing A vitene (and the material in the transverse colonic granulomas) was different from normal collagen present in the patien t’s sigmoid p ericolonic fibrosis.
DiscussionIn a d v e rta n t sp len ic laceratio n is a
com m on co m p lica tio n of le ft u p p e r quadrant surgery, and this has frequently been successfully treated by the topical application of Avitene9,10, as in the case reported here. Adverse reactions to Avitene have been reported, and the most serious of these appear to be potentiation of infection (abscesses, etc.), hem atom a and wound dehiscence. O ther reported a d v e rs e re a c t io n s in c lu d e a lle rg ic responses, adhesions and foreign body reactions.3,11,13,14 These last three, particularly foreign body reaction, appear to have b e e n in v o lv e d in th e p re s e n t reported case. In one reported series of 811 patients treated with Avitene, there w ere 103 instances of adverse responses,
including two w ith foreign body reactions and three with adhesions.14 Thus it can be seen that such complications are relatively infrequent.
The cause of the unexpected adverse response to Avitene which occurred in this case is difficult to ascertain exactly b u t is likely re la ted to severa l factors such as immunologic reactivity and in trao p e ra tiv e te c h n iq u e . Im m u n o lo g ic h y p e rre a c tiv ity is su g g e s te d by th e marked infiltration of eosinophilic leukocytes involving all of the biopsied Avitene granulomas. Such an eosinophilic infiltrate has not been rep o rted to be characteristic of th e usual local tissue response to A vitene,15 or, for that m atter, to o ther injectable bovine collagen preparations.1 This peculiar response in the present case appears to represen t a local manifestation of a systemic im m unologic resp o n se since rev iew of th e patien t’s laboratory data revealed that h is p e r i p h e r a l b lo o d e o s in o p h i l s increased from zero to one percent at the tim e of th e first surgery and A vitene tre a tm e n t to five to 15 p e rc e n t one month later. The few apparent allergic reactions to Avitene reported in patients have sim ply consisted of e ry th em a or p r u r i t i s .14 F u r th e rm o re , e x te n s iv e immunologic studies in animals (guinea pigs, rabbits and dogs) and hum ans have indicated that allergic reactions to Avitene should be rare and of little significance. It is unknow n why th e patien t reported here had developed an im m unologic re a c tiv ity w h ich a p p a re n tly resulted in the local and systemic eosin- ophilia.
A n o th er cause of th e u n e x p e c te d a d v e rse re a c tio n to A v ite n e w h ich occurred in this case was likely related to the technique involved in Avitene application. The num erous nodu les no ted during the second operation w ere adheren t to the serosa and m esentery from m id-transverse to m id-descending colon. This w ould indicate a m ore extensive
3 0 2 M c G R E G O R , M acA R T H U R , A N D C A R T E R
application of Avitene than was required to trea t the splenic capsular tear, p e rhaps in part due to colonic serosa and m esentery inadvertently coming in contact with the site of splenic application. The prevention or lessening of the occurrence of this problem appears to now be available, w ith th e d ev elopm en t of a m ethod of preparing Avitene into a discrete firm pledget using a syringe.4
O ne im p o rtan t aspect of th is case involves the identification of a material which appears to be eliciting a foreign body g ranu lom atous reac tio n . R eferences such as th e ex ce llen t Particle Atlas8 are one available approach bu t in the p resen t case w ere of little help in solving this problem . In this case the steps which yielded the identification of the material included: (1) review of the o p era tiv e re p o rt and com m unication betw een the pathologist and surgeon, resulting in inform ation which circum stantially incrim inated Avitene; (2) light m icroscopic exam ination w ith rou tine a n d sp e c ia l s ta in s , c o m p a r in g th e patient’s biopsy m aterial with com m ercially available Avitene; and (3) electron microscopic examination, comparing the patient’s biopsy m aterial and Avitene.
In sum m ary, A vitene (m icrofibrillar collagen hemostat) can be a highly b eneficial agent as an adjunct to hemostasis when control of bleeding by ligature or conventional procedures is ineffective or impractical. Surgeons, however, should be aw are of p o ten tia l com plications, which in the present case w ere probably re la ted to im m unologic reactiv ity and o p e ra tiv e te c h n iq u e . F u r th e rm o re , pathologists should be aware of the histo- morphologic appearance of this material which may resu lt in bowel obstruction and other complications.Acknowledgments
Thanks are extended to William J. Bopp for assistance in electron microscopic processing, the Histology Section of the Laboratory Service for assistance in histologic processing, and Brenda Adams, Irene Gray and Angie Allen for secretarial assistance.
American Critical Care provided the Proceedings ofa Symposium on Avitene. Ultrastructural studieswere performed using the facilities of the ElectronM icroscopy Unit, L aboratory Service, VeteransAdministration Medical Center, Kansas City, MO.
References1. B a r r , R. J ., K i n g , D . E , M c D o n a l d , R. M .,
and B a r t l o w , G. A.: Necrobiotic granulomas associated with bovine collagen test site injections. Am. J. Acad. Dermatol. 6:867-869, 1982.
2. B a t t is t a , O. A.: The chemistry and preparation microfibrillar collagen hemostat. Proceedings o f Symposium on Avitene Microfibrillar Collagen Hemostat. San Francisco, Am erican Critical Care, 1975, pp. 38-40.
3. C h u n g , A. F., M e n o n , J., and D i l l o n , T. F.: Acute postoperative retroperitoneal fibrosis and ureteral obstruction secondary to the use of Avitene. Am. J. Obstet. Gynecol. i32:908-909, 1978.
4 . G o r d o n , L . A., S h a p i r o , S . J . , and F e i n b e r g , S. E.: Microfibrillar collagen hemostatic pledgets. Arch. Surg. 116:359-360, 1981.
5. H a it , M. R.: Microcrystalline collagen: A new hemostatic agent. Am. J. Surg. 120:330, 1970.
6. JO H N SO N , L. P.: A review of the use of Avitene in otolaryngologic surgery. Otolaryngol. Head Neck Surg. 88:8-9, 1980.
7. M a s o n , R .: Hemostatic mechanisms of microfibrillar collagen. Proceedings of Symposium on Avitene Microfibrillar Collagen Hemostat. San Francisco, American Critical Care, 1975, pp. 32-35.
8 . M c C r o n e , W . C . and D e l l y , J. C .: The Particle Atlas: Encyclopedia of Techniques for Small Particle Identification, 2nd ed. Ann Arbor, Ann Arbor Science Publishers, 1973.
9. M O R G EN STERN , L .: Splenic and general surgery. Proceedings of Symposium on Avitene Microfib rilla r C ollagen H em osta t. San Francisco, American Critical Care, 1975, pp. 8—10.
10. M ORGEN STERN , L .: The avoidable complications o f sp len e c to m y . S urg . G y n eco l. O b s te t. 145:515-528, 1977.
11. P a r k , S. A., G i a n n a t t a s i o , C. and T a n c e r , M. L.: Foreign body reaction to the intraperi- toneal use of Avitene. Obstet. Gynecol. 58:664— 667, 1981.
12. Physicians Desk Reference, 37th ed.: Medical Economics Company, Oradell, NJ, 1983, p. 578.
13. R a o , P. S., C a v e n a u g h , D., R i c h m a n , A. V., and F r e n c h m a n , S. M.: An evaluation of the tendency of Avitene to produce periureteral fibrosis in the dog. Am. J. Obstet. Gynecol. 745:87-91, 1983.
14. T e n e r y , J. H.: A summary. Proceedings of Symposium on A vitene M icro fib rillar C ollagen Hemostat. San Francisco, American Critical Care, 1975, pp. 46-47.
15. Z e l e z n i c k , L. D.: Toxicity and antigenicity of microfibrillar collagen hemostat. Proceedings of Symposium on Avitene Microfibrillar Collagen Hemostat. San Francisco, American Critical Care, 1975, pp. 41—44.