Av malformation
30
DR. SHAHZAD HUSSAIN BDS, FCPS(Resident) Nishtar institute of Dentistry, Multan SNDENTALCARE.CO
-
Upload
dr-shahzad-hussain -
Category
Health & Medicine
-
view
24 -
download
1
Transcript of Av malformation
DR. SHAHZAD HUSSAIN
BDS, FCPS(Resident)
Nishtar institute of Dentistry, Multan
SNDENTALCARE.CO
Case PresentationPatient Name: Asia
Age/Gender: 30 year/Female
Presenting Complaint
History Of Presenting Complaint
Past Medical & Dental History
Family History & Personal History
General Physical Examination
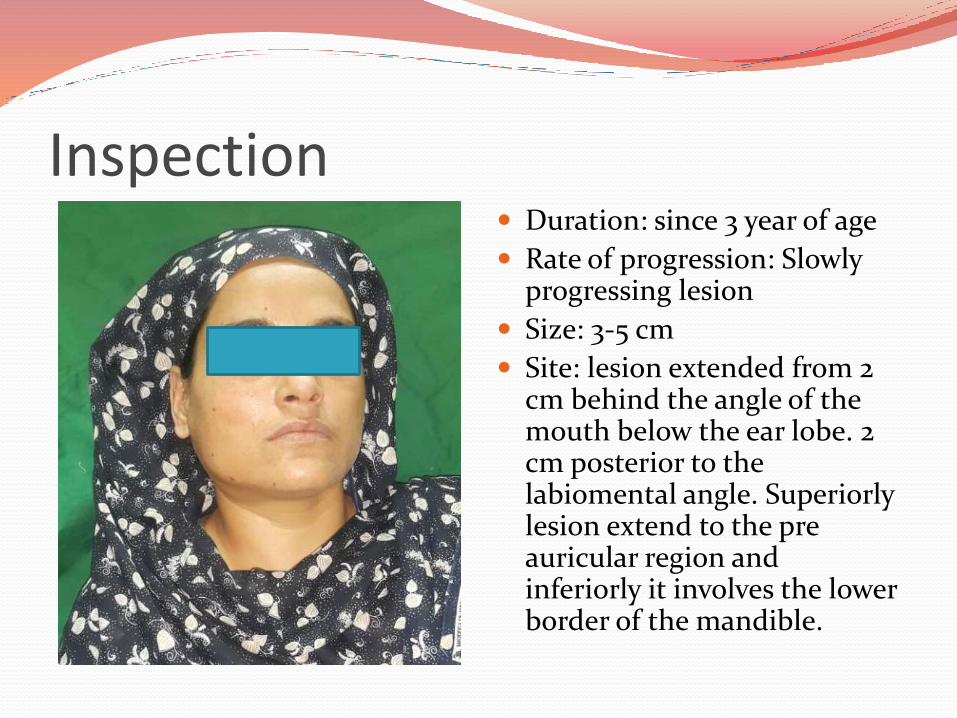
Inspection Duration: since 3 year of age
Rate of progression: Slowly progressing lesion
Size: 3-5 cm
Site: lesion extended from 2 cm behind the angle of the mouth below the ear lobe. 2 cm posterior to the labiomental angle. Superiorly lesion extend to the pre auricular region and inferiorly it involves the lower border of the mandible.
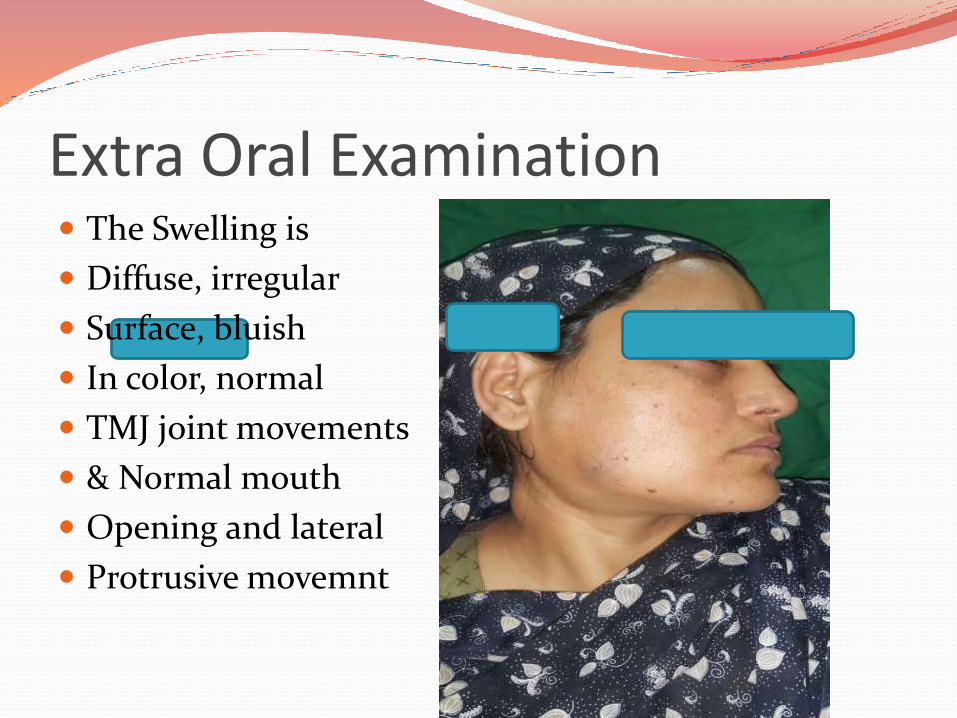
Extra Oral Examination The Swelling is
Diffuse, irregular
Surface, bluish
In color, normal
TMJ joint movements
& Normal mouth
Opening and lateral
Protrusive movemnt
Palpation Firm, tender & warm swelling.

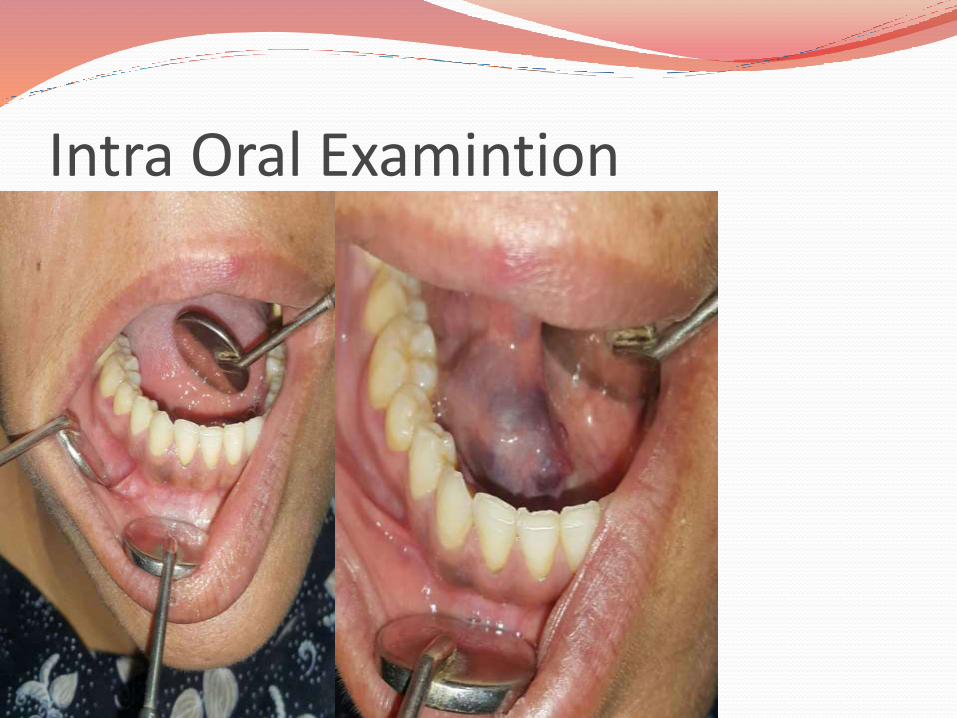
Intra Oral Examination The lesion extended
from floor of the mouth to the retromolar pad area sparing the lingual side. It also involves the right lower buccalvestibule, soft & hard palate & fauces.
Intra Oral Examintion
Diffrential Diagnosis
Vascular Tumors:1:Benign:I. Infantile HemangiomaII. Congenital Hemangioma: a. Rapid involuting Congenital Hemangioma, (RICH)b. Non involuting Congenital Hemangioma(NICH)c. Partially involuting Congenital Hemangioma(PICH)
2:Locally Aggressive Vascular Tumors3:Malignant Vascular Tumors
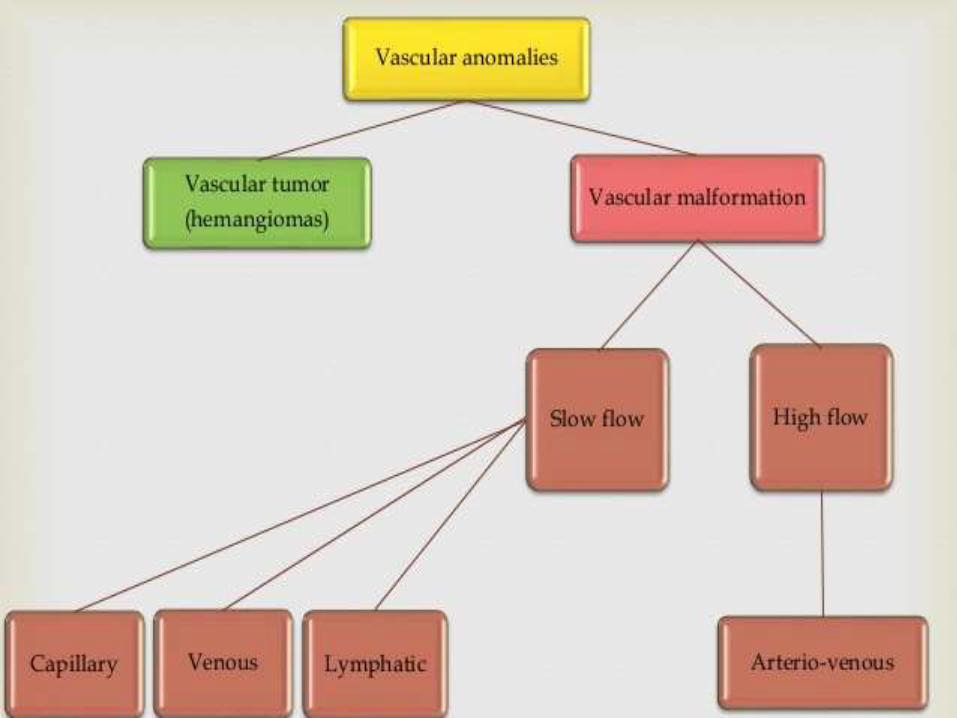
Basic Cell biology On basis of cell kinetics, there are two major types
of vascular anomalies:
Hemangiomas: lesions demonstrating endothelialhyperplasia.
Vascular Malformations : lesions with normalendothelial turnover.
Diffrential Diagnosis
Vascular Malformation:1. Capillary Malformation
a. Port Wine stains(Strug weber Syndrome)
1. Venous Malformation
2. Lymphatic Malformation
3. Arterio-Venous malformation
4. Arterior-Venous Fistula
5. HEREDITARY HEMORRHAGIC TELANGIECTASIA(Rendu Osler Weber disease)
Diagnostic Tests
1. History & clinical examination2. Complete Blood Count3. CT Angiography4. Ultrasonography5. CT scan6. MRI7. Plain X-ray OPG (Shows soap bubble & honey comb
appearance) Other Investigations that are required:1. GLUT +ve for Hemangioma2. GLUT –ve for Vascular malformation
CT Scan(Axial View)
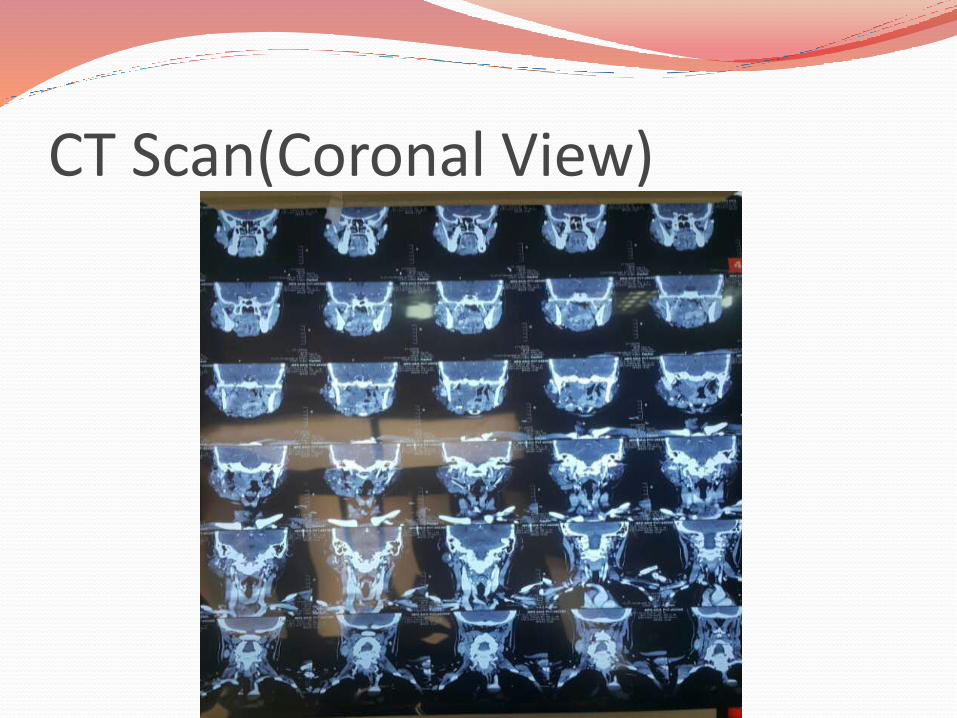
CT Scan(Coronal View)

CT Scan(Saggital View)
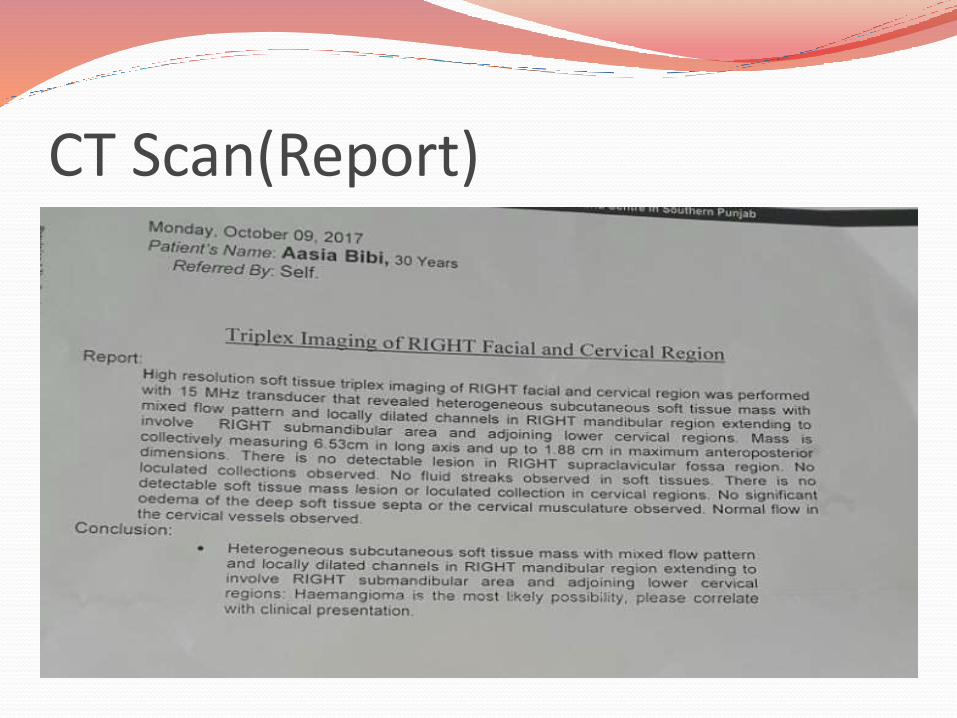
CT Scan(Report)
Diagnosis Vascular malformation (AV)
Hemangioma can’t be ruled out.
Treatment Options1. Non Surgical (Conservative)
2. Surgical (Non (Conservative)

Non SurgicalI. Medications
A. Intra Lesional Cortecosteroids
B. Interferon Therapy
C. Cytostatic Therapy
D. Propanol Therapy
2: Sclerotherapy
3: Laser Therapy
Surgical Resection Of the Lesion
Embulization
Compartmentalization
Intralesional CortecosteroidsMechanism: Lead to increase in the level of cytochrome b
and induces apoptosis in hemangioma.
Benefits:
1. First line therapy
2. Conservative
3. Inexpensive
Disadvantages:
1. Sleep disorder
2. Irritability
3. GERD
4. Osteoprosis
InterFeron Therapy Mechanism: Interferon alpha 2a and Alpha 2b based
on down regulation of fibroblasts growth factors.
Disadvantages: Due to neurotoxic side effects it is no longer recommended.
CytotoxiC therapy Dosage: I/V weekly dosage of 1 mg/m3 over a period of
one to 8 months responds well in all patients
Disadvantages:
1. Loss of hear
2. Abdominal discomfort
Proponol Therapy Mechanism: Exact mechanism not clearly understood.
The pro- angiogenic pathway could be suppressed by proponol therapy. Propnol therapy effect can be explained by premature apoptosis of Endothelial cells. It causes vasoconstriction of micro vessels.
It is the first line therapy for RICH. Within 24 hours after the first application , size reduction of upto 90 percent can be achieved within one two weeks.
Usual dose of 1-3 mg /kg daily
Laser Therapy Controversial
It is believed that laser/phototherapy will not cure the pathology as it has a penetration depth of 0.75 mm to a maximum of 2mm.
Only indicated for the superfacial parts of infantile hemangioma.
Sclerotherapy It is the most wide spread method.
In 1903, wyeth used boiling water as the sclerosing agent.
There are many sclerosing agents which are divided into following catogaries
1. Osmotic substances: Hypertonic saline, salicylate
2. Chemical Substances: Ethanol & iodine
3. Anticancer Substances: Bleomyocin
4. Detergents: Sodium tetradecylsulphate
Resection with immediate replantation.
Goal of the surgery is to remove the lesionControl of hemorhageReconstruct the defectIncision: Extraoral incision is preferable when the lesion
extends proximally to the angle and ramus. Tran oral approach doesn’t allow good visibility & hemorrhage control
Procedure: An osteotomy can be made, distal to the lesion & involved segment can be rotated laterally to visulaize the lingual surface of the mandible. The resected mandible is replaced with the autologus bone grapt which is stabilized with bone plates.
IMF is done to maintain proper jaw position.
Compartmentalization Jackson & colleagues treated 18 patients by this
technique in 1993.
They placed non resorbable sutures deep subcutaneous within the lesion
After placing the sutures, sclerosing agents were injected in the compartment followed by surgical resection with minimal risk of bleeding
The amount of infiltration is 3 cc to 35 cc depending upon the size of the lesion
Tracheotomy may be required To prevent airway compromise.