Autonomic Integration in Schizophrenia
18
PSYCHOSOMATIC MEDICINE—VOL. I, NO. 3,.JULY, I939 AUTONOMIC INTEGRATION IN SCHIZOPHRENIA AUTONOMIC STATUS DETERMINED STATISTICALLY, THE THYROID FACTOR, AND A POSSIBLE THYROID-OYPOTHALAMUS MECHANISM JOSEPH C. RHEINGOLD, M.D.* THE STUDIES IN THIS SERIES deal wit h problems of autonomic function in schizophrenia. The aim is ultimately to formulate the characteristic defect or defects of homeostasis. As a basis for an experimental ap- proach it is necessary first to define the vegetative pathoplasia of the disease. The contributions of the Memorial Foundation for Neuro-Endocrine Re- search do not serve the present purpose because its findings are derived mainly from study of long-hospitalized male patients and the need here is the de- scription of an unselected schizophreni c population in early stages of the psy- chosis. There seems, indeed, to be no report in the literature on objective findings in a group of incipient cases large enough to assure the validity of a statistical analysis (jo). To determine the vegetative charac- ters of schi zophrenia, first a survey was made of the organic data in the records of 129 schizophrenic subjects. The re- sults are reported in this paper to- gether with an attempt to appraise the influence of the thyroid gland in the production of the schizophrenic syn- drome. Then a single patient was stud- ied over a period of a year by the daily administration of a battery of tests. These results will be presented in a subsequent paper. * From the Psychiatric Institute (D r. H. Douglas Singer, Director) of the University of Illinois College of Medicine. PROCEDURE AND RESULTS Since schizophrenia presumably is not a disease entity, a reasonable de- gree of homogeneity of a schizophrenic group must be demonstrated before its statistical analysis may be profitably undertaken. The criteria of reasonable homogeneity are probably satisfied when the cases are classified by a uni- form practice, one body type pre- ponderates, the age range is not too great, the subjects are in about the same stage of the disease, the extremes of psychomotor activity are eliminated, and each sex and each clinical sub- group is analyzed separately. The patients in the present group were admitted to the Psychiatric Insti- tute between the years 1931 and 1936. The classification in each instance was made by Dr. H. Douglas Singer and was confirmed by the State hospitals to which some of the patients were later transferred. Of the 129 patients, 43.4 per cent were males and 56.6 pe r cent, females. The sex distribution in the several clinical subgroups is shown in Table I I. The charts show histograms of age, weight, pulse rate, blood pres- sure, oxygen consumption rate, and blood chemical findings in 129 cases of schizophrenia—ordinates represent fre- quency; solid line, males; broken line, females. The histogram of age shows that the subjects bulk in the third decade of life. The paranoid group is
-
Upload
urbota-inskraenkthet -
Category
Documents
-
view
217 -
download
0
Transcript of Autonomic Integration in Schizophrenia

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 1/17
PSYCHOSOMATIC MEDICINE—VOL. I, NO. 3,.JU LY , I9 3 9
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA
AUTONOMIC STATUS DETERMINED STATISTICALLY, THE THYROID FACTOR,
AND A POSSIBLE THYROID-OYPOTHALAMUS MECH ANISM
JOSEPH C. RHEINGOLD, M.D.*
THE STUDIES IN THIS SERIES d e a l w it h
problems of autonomic function inschizophrenia. The aim is ultimately toformulate the characteristic defect ordefects of homeostasis.
As a basis for an experimental ap-proach it is necessary first to define thevegetative pathoplasia of the disease.The contributions of the MemorialFoundation for Neuro-Endocrine Re-
search do not serve the present purposebecause its findings are derived mainlyfrom study of long-hospitalized malepatients and the need here is the de-scription of an unselected schizophrenicpopulation in early stages of the psy-chosis. There seems, indeed, to be noreport in the literature on objectivefinding s in a g roup of incipient caseslarge enough to assure the validity ofa statistical analysis (jo).
To determine the vegetative charac-
ters of schizophrenia, first a survey wasmade of the organic data in the recordsof 129 schizophrenic subjects. The re-sults are reported in this paper to-gether with an attempt to appraise theinfluence of the thyroid gland in theproduction of the schizophrenic syn-drome. Then a single patient was stud-ied over a period of a year by the dailyadministration of a battery of tests.These results will be presented in asubsequent paper.
* From the Psychiatric Insti tute (D r. H . DouglasSinger, Director) of the University of Illinois College
of Medicine.
PROCEDURE AND RESULTS
Since schizophrenia presumably isnot a disease entity, a reasonable de-gree of homogeneity of a schizophrenicgroup must be demo nstrated before itsstatistical analysis may be profitablyundertaken. The criteria of reasonablehomogeneity are probably satisfiedwhen the cases are classified by a uni-
form practice, one body type pre-ponderates, the age range is not toogreat, the subjects are in about thesame stage of the disease, the extremesof psychomotor activity are eliminated,and each sex and each clinical sub-group is analyzed separately.
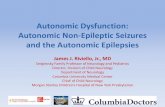
The patients in the present groupwere admitted to the Psychiatric Insti-tute between the years 1931 and 1936.The classification in each instance wasmade by Dr. H. Douglas Singer andwas confirmed by the State hospitalsto which some of the patients werelater transferred. Of the 129 patients,43.4 per cent were males and 56.6 percent, females. The sex distribution inthe several clinical subgroups is showninTable I I . The charts show histogramsof age, weight, pulse rate, blood pres-sure, oxygen consumption rate, andblood chemical findings in 129 cases ofschizophrenia—ordinates represent fre-quency; solid line, males; broken line,females. The histogram of age shows
that the subjects bulk in the thirddecade of life. The paranoid group is

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 2/17
398 JOSEPH C. RHEINGOLD
TABLE I
ORCANIC FINDINGS IN 129 CASES OF SCHIZOPHRENIA TABULATED FOR EACH SEX AND TOTAL GROUP
Weight—
Mean% Cases underMeans lbs. under% of prediction
% Cases normal% Cases over
Mean lbs. over
Pulse Rate-Blood Pressure—
Systolic
DiastolicPulse Pressure
Oxygen Consumption—
Mean minimal rate% Cases below —10
Mean% Cases —10 to +10
Mean% Cases above +10
MeanBlood Chemistry—
N. P. N.DextroseCholesterolCarbon-Dioxide C.P.
Blood Cytology—
Hemoglobin %
R. B. C. (millions)Color IndexW. B. C.% Neutrophils
Males
140.7
69.0
22.5
13-8
17.0
14.0
38-9
76
" 57639
- I5 - 753-o
— 22 .547-o
— 2 . 1
0
-
29.7
91.7
194.9
56.4
86.84.860.89
8,010.
61.2
Females
107.581.022.516.4
5 . 0
14.0
15-5
82—
10 5
7 2
33
- 1 6 . 769.0
— 2 1 . 2
29.0
0
1.56
+ 11
30.3
89.7218.8
53-9
77-44-370.87
7,840.
59-9
Total Group
124.175.022.515.111.0
14.0
26.4
79
n o
7436
— 16.261.0
- 2 1 . 838.0
- 1.050.78
+ 11
30.090.7
206.8
5 5 - i81.8 =
13.08 Gm.
4.62
0.88
7,920.
60.4
distinguisheld by a mean age which is
about eight years greater than the
mean ages of the other groups (Table
II). Photographs of the patients in thenude suggest a preponderance of theleptosomic habitus. The m ean du ration
TABLE II
ORGANIC FINDINGS IN 129 CASES OF SCHIZOPHRENIA TABULATED FOR EACH CLINICAL SUB-GROUP
No. of MalesMean AgeNo. of FemalesMean AgeWeight, % cases underWeight, mean lbs. underPulse RateSystolic B. P.
Diastolic B. P .Pulse PressureB. M. R., % cases below —10
B. M. R., MeanCholesterol
N . P. N.DextroseCarbon-Dioxide C.P.Hemoglobin %
R. B. C. (millions)Color IndexW. B. C.% Neutrophils
Simple
1 1
24.6
727.0
78*5-377
11 4
78365720.2
196.4
27.2
88.0
54.2
794.650.85
6,940 •
57-7
Hebephrenic
3 325.7
1925.4
89
22.578
10 6
71
356527.4
200.3
3O-5
91-357.081
4 - 5 50.89
7.550.
60.4
Catatonic
927.7
825.0
7322.4
7910 7
7 2
u16.0
221 .7
3O.1
87.555 -
1
8 44.690.89
8,250.61.2
Paranoid
835-42 2
31-75422.578'
1 1 4
734 1
6519.9
227.5
30-494.2
56.3834.680.88
7,440-
57-6
Other Types
526.8
1726.1
7819.8
8310 9
74356425-7
185.9
31.292.4
53-282
4-560.89
9.43O.
65-3

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 3/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 399
r —
*f c-J
IZ 15 7a 21 24 27 Id 33 36 5? 7z 45 4S 5>
POUNDS UNDZRWE/GHT OR
Z4
SI
l&
15
IZ
i
•5 ri
N0NPR0TE1N
NITROG-EN
i ng JO 3Z
CfTVT"

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 4/17
400 JOSEPH C. RHEINGOLD
28
M
Zc
IZ
6
A
o
. . . .
i
DEXT/2OSE
i i
to 45 W 75 fio 55 Too ^ Tio 775 T o 7^5 7«o Taj
0
a
:F hi CHOLESTEROL
j . . - ^ . . . . .
• i i " " * " !
Llo >+5 /bo Zo5 ZZO 235 zSo ZiS
MGM. PER QENT
CARBON- DIOXIDECOMBINING
POWER
Si , 40 fo¥ 48
VOLUME'S PER CENT

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 5/17

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 6/17
402 JOSEPH C. RHEINGOLD
PULSE RATE
55 io TO 75 8o 85 <fo
of the psychosis prior to admission wasabout five months and, in more thanhalf of the cases, less than one month.Clinical and laboratory examinationswere made w ithin th e two weeks follow-
ing admission. Psychomotor activity isa random error in a large series of casesbut in any event the more stuporousand more excited patients tend to ex-clude themselves because of non-co-operation. This exclusion, apart fromgeographic selection, is the only selec-tion factor. Patients with complicatingphysical illness affecting metabolicstatus were not included in the study.
One may therefore venture to saythat the findings for each sex, as shown
in Table I, characterize a homogeneousschizophrenic population. That sex isa significant variable is demonstratedby the consistently greater tendencyof the females to hypometabolism.In the case of the sub-groups (Table II)the numbers of subjects in each classi-fication, certainly in each sex-sub-group class, are too few to warrantstatistical analysis. It will be observed,however, that despite differences at theclinical level, the sub-groups yield verysimilar metabolic pictures.
The data reported on compriseweight, pulse rate , blood pressure, basal
metabolic (oxygen consumption) rate,blood chemistry, and blood cytology.Body temperature and respiratory ratewere excluded because they were notdetermined under standard conditions.
Urinalysis was qualitative only. Cere-brospinal fluid findings were in generalnormal. Insurance statistics served asstandards of weight. The rate of oxy-gen consumption was measured by theBenedict-Roth metabolimeter usingthe Boothby-Sandiford modification ofthe Du Bois standards. In 53 per centof the cases two to fourteen readingswere made. In these instances, theminimal rate, rather than the averageof the several readings was taken as themore reliable index of basal metabo-lism. The blood content of nonproteinnitrogen was determined by the modi-fied Koch-McMeekin Method; dex-trose, by the modified BenedictMetho d; cholesterol of the whole blood,by the modified Bloor Method; andcarbon-dioxide combining power of theplasma, by the Van Slyke and CullenMethod. Hemoglobin was measured bythe Dare instrument and blood countswere made in the usual way. Thisbattery of tests was not always ad-
ministered on the same day but neverover a period of more than a week.

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 7/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 403
There was of course no planned con-trol study but what may be used forthis purpose are the ranges of variation(2p) for blood chemical and cytologicaldeterminations made in thousands ofsubjects in the clinical laboratories ofthe Illinois Research and EducationalHospital of which the Psychiatric Insti-tute is a part. Unless the control sub-
jects match the schizophrenic patientsin at least the sex ratio, age range, andincidence of leptosomes there is prob-ably little point in setting up a specialcontrol group.
In the statistical analysis of theda ta the mean is used as the expressionof central tendency (Tables I and II)and the histogram as the expression ofvariability (see Charts).
Weight: Three-fourths of the pa-tients are about 15 per cent belowstandard weight. Hoskins (21) found
the mean weight of 57 male schizo-phrenics 16 per cent below prediction.Since this degree of underweight maybe characteristic of the leptosome, oneneed not conclude that a higher inci-dence of malnutrition exists in theschizophrenic group than in a normalgroup. Nor does low mean weightmirror chronicity since the incidence ofunderweight men (69 per cent) in thisseries is greater than that of patientsin Hoskins' series (55 per cent) who
were hospitalized a mean of 5.9 years.Pulse Rate: Mean values are withina normal range but group variabilityis probably greater than normal. Hos-kins and Sleeper (20) found an averagepulse rate of 59.2 in 57 schizophrenicmen. The discrepancy may possibly beaccounted for by the practice at theWorcester State- Hospital of determin-ing pulse rate , as well as blood pressure,under basal conditions.
Blood Pressure: The mean systolicand diastolic levels are lower than thoseof the general population (127.6/83.5 in150,000 life insurance applicants). The
systolic pressure is reduced relativelymore than the diastolic, producing adiminished pulse pressure. From Krae-pelin on, almost all investigators haveagreed that schizophrenia is character-ized by a lowering of the blood pres-sure. The literature was reviewed in1932 by Freem an, Hoskins, and Sleeper(9), who also reported a mean blood
pressure of 104.5/54.5 in 180 maleschizophrenics. The 323 control sub-jects likewise yielded low mean read-ings (115.7/71.2). The difference insystolic levels between patients andnormal subjects (11.2) is about thesame as the difference between themale patients in the present series andthe general population (12.6). Thelower readings at Worcester may bedue to the more nearly basal conditionsof testing.
Oxygen Consumption: Low metabolic
rates are frequent in patients of thePsychiatric Institute. Readings in therange of minus 40 to minus 30 are notuncommon amongst the schizophrenicsubjects. In the present group 61 percent of the patients have a mean rateof minus 21.8 per cent and only twopatients have rates (single determina-tions) above the conventional upperlimit of plus 10. This result is in con-formity with almost all other reportsof basal metabolism in schizophrenia.
The literature was summarized byHoskins (if) who later reported a meanminimal rate of minus 18.9 per cent inhis own series of 114 male schizo-phrenics (19).
An interesting find ing is the loweringof the basal metabolic rate followingexercise in 11 of 30 cases included inthe present series. The basal rates andthe rates after exercise were not deter-mined on the same day but the differ-ence between the two is too great to beaccounted for by lower basal levels onthe days of the experiment with exer-cise. Thus patient H-B. had rates of

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 8/17
404 JOSEPH C. RHEINGOLD
minus 17, minus 6, and minus 4 underbasal conditions on three successivedays, but on the fourth, after steppingon and off a chair for one minute, hada rate of minus 34.
Nonprotein Nitrogen: The mean re-sults are within a normal range and thecurve of distribution approaches anormal frequency curve. Worcester
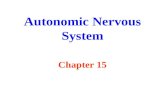
(20), too, finds a normal N.P.N. level.Dextrose: Mean values are againnormal. The literature was reviewed byW. Freeman (/ /) in 1933. He reportsa mean of 96.6 mgm. per cent for 347determinations in 59 patients and amean of 95.4 in 31 control subjects.
Cholesterol: Looney and Childs (j/)m I
933 collected the literature onblood cholesterol determinations inboth normal and schizophrenic persons.With the exception of two reports,normal subjects do not yield mean
values above 200 mgm. per cent, nomatter what method is used. The re-sult of 206.8 in our schizophrenic groupmay therefore indicate a trend to highnormal or slightly elevated bloodcholesterol content. Five authors havereported mean values over 200 inschizophrenia but three have reportedmean values between 140 and 200, andseven, below I40. Looney and Childsfound a mean level of 158 in 50 schizo-phrenic men and that of 175 in 26
normal men.Carbon-Dioxide Combining Power:
The means falls at the lower limit ofthe normal range. Variability is pro-nounced with a preponderance of fe-male cases in the 46 to 50 class inter-val. Worcester measures carbon-di-oxide content, not combining power.Looney and Freeman ( J J ) recently re-ported a venous content of 57.8 percent in both 112 male patients and 67control subjects.
Blood Cytology: (The histograms arereserved for a future paper dealingwith the blood morphology in schizo-
phrenia.) The blood picture is charac-terized by mild secondary anemia,normal absolute leucocyte count, andlow normal percentage of neutrophils.Worcester {4) reports the followingfindings in 57 men: R.B.C., 4,957,000;Hb, 15.3 gm.; W.B.C., 10,477; andneutrophils, 59.6 per cent.
DISCUSSION
Summarizing the foregoing resultsone may say that this group of schizo-phrenic patients shows trends to sub-standard weight; reduced oxygen con-sumption; normal pulse rate; loweredsystolic, diastolic, and pulse pressures;normal blood nonprotein nitrogen anddextrose levels; high normal or slightlyelevated blood cholesterol content; lownormal carbon-dioxide combining
power of the blood plasma; mild sec-ondary anemia; normal absolute leuco-cyte count; and low normal percentageof neutrophilic leucocytes. The dis-placements from normal means consti-tute one of the features of the disturb-ance of homeostasis in schizophrenia.Another feature is the greater thannormal range of variation of everymeasurement. This is demonstratedmathematically by the Worcester find-ing of greater standard deviations for
almost every determination in patientsas compared with the same determina-tion in normal control subjects. Mul-tiple determinations in the same pa-tient also reveal increased variability.This "physiologic clumsiness" may bethe fundamental aspect of the homeo-static fault. Hoskins (2/) ventures theprediction tha t in many cases of schizo-phrenia "the essential etiology willultimately prove to be defects of inte-gration . . . reflected in extreme varia-tion and atypical inter-action of vari-
ous functions". In the present paper,however, the discussion is based on

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 9/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 405
only the deviations from normal cen-tral tendencies.
The most striking departure fromnormality is the low oxygen consump-tion rate. A consistently elevated basalmetabolic rate in a schizophrenic sub-jec t is practically unknown. Since 1908the literature has been concordant onthe finding of a lowered basal m etabolic
level. "Schizophrenia", says Hoskins(/<?), "is a condition characterizedamong other physiologic abnormalitiesby a systematic downward displace-ment of the oxygen consumption rate".This trend is made more impressive bythe difficulty of obtaining standardconditions of testing in psychotic sub-jects: According to Hoskins (23) "thetrue basal rate in most cases is prob-ably considerably lower than the rateactually determined".
It seems reasonable to assume that
this depressed level of basal metabolismis an integral part of the disease pic-ture. It is not a characteristic of theperson predisposed to schizophrenia.In fact, the normal leptosome (43) withhis tendency to elevated basal meta-bolic rate, as well as tendencies to lowerblood cholesterol content, increasedcapillary permeability, greater oxida-tive preponderance, increased thyroid-adrenal activity, and more distinctlysympathicotonic reaction to epineph-
rine, shows trends opposite to thoseobserved in the schizophrenic subject.That inanition is not a factor in thediminished oxygen use is shown byabsence of correlation between weightand basal metabolic rate (r = .i2). It isonly in states of severe inanition as inanorexia nervosa that basal metabo-lism falls to levels comparable to thosefound in schizophrenic patients (5).Hospitalization as a cause of thealtered metabolic status is ruled out inthe present group of incipient cases;
that it plays no part in even long-hospitalized patients has been shown
recently by Hoskins (2j). The use ofsedatives has been invoked as explana-tion, but although they make for qui-escence and more nearly representativereadings, no evidence can be foundthat they depress the actual basal rate.Positively, the reversal of the metabolictendencies, the uniformity of the find-ing of low oxygen consumption rate,
the degree of reduction, and the tend-ency in most cases to rise of the ratewith clinical improvement (21) leavelittle doubt that the lowered basal me-tabolism is an important feature of theschizophrenic disorder.
Investigation of the pathogenesis ofschizophrenia therefore requires con-sideration of causes antecedent to thediminished use of oxygen. Three setsof such causes may be postulated:1) insufficient supply of oxygen to thetissues, 1) derangement of the chemo-
dynamic processes within the celkj and3) disturbance of the mechanisms con-trolling cell respiration.
The abnormality is probably not inthe transport of oxygen. The arterialblood of patients contains as muchoxygen as that of normal persons andthe tissues of the patients abstract evenmore oxygen from the blood than dothe tissues of the control subjects (33).Blood volume is reduced, but the devi-ation from normal disappears when
schizophrenic subjects are matched by"nutritional index" (23). The de-creased blood mass may be incidentalto the hypoplastic vascular system ofthe leptosome. Finally, although, H .Freeman (/o) has twice reported di-minished velocity of the blood flowunder basal conditions, Finesinger etal. (6), using the same method, foundthe average circulation time in 130patients to be within normal limits.
Oxygen may be supplied to the tis-sues in adequate amount and at anadequate ra te but m ay fail to enter intochemical reactions within the cells be-

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 10/17
406 JOSEPH C. RHEINGOLD
cause of a disturbance of enzyme ac-tion. A profitable investigation of thispossibility must await more exactknowledge of biologic oxidation. Somedoubt is cast upon the possible exist-ence of a primary intracellular dys-function in schizophrenia by the re-sults of the administration of dinitro-phenol. Looney and Hoskins (32) foundthat although the drug produced an in-crease in the basal metabolic rate ofabout 50 per cent, there was no con-current change in temperature, pulserate, or blood pressure, only a tem-porary increase of the nonprotein nitro-genous blood constituents, and no con-sistent trend in the blood cholesteroland lactic acid values. Presumably noclinical improvement was observed. Ifthe phenomena of schizophrenia wereconsequent to an altered ability of thecells to metabolize oxygen, correction
of this fault should restore the vitalsigns and body chemistry to normaland effect clinical change.
There remains then the possible roleof the mechanisms that regulate thespeed of metabolism—the trinity ofautonomic nervous system, endocrineglands, and non-hormonal chemicalsubstances. Out of the almost infinitepermutations of the interdependentfunctions of these vegetative mecha-nisms Qne may, a priori, isolate the
factor of thyroid insufficiency. Thyroiddisorders and schizophrenia grow outof the same constitutional soil. The in-fluence of the thyroid secretion uponthe brain is proved by experimentalwork (46) and clinical observation. Thedegree of reduction of basal m etabolismin schizophrenia suggests thyroid de-ficiency; in fact it is now consideredlikely that a persistent change in themetabolic rate implies altered thyroidfunction (57).
The possibility of thyroid insuffi-ciency as a factor in the hypometabolicstatus of the schizophrenic has sug-
gested itself to several investigators.The literature was brought together byHoskins and Sleeper {18) in 1930. Sincethen increased experimental and clini-cal knowledge has strengthened theassumption and a restatement of the"case" for the thyroid seems war-ranted.
It is now recognized that hypo-
thyroidism may exist as a part-syn-drome and that uncomplicated hypo-thyroidism presents a var iety of clinicalpictures more or less distinct fromclassical myxedema. Reviews of thesubject may be found in papers byWarn"eld (52) and by Seward (48). Ingeneral, these recently described formsof thyroid hypofunction are distin-guished by the absence of skin infiltra-tion and other gross signs of Gull'sdisease even when the basal metabolicrate is less than minus 40.
The symptomatology of non-myxe-dematous hypothyroidism is strikinglysimilar to that of schizophrenia. Com-mon to both is a usually insidious on-set, a chronic course, absence of adefinite group of symptoms or charac-teristic physical signs, lowering of thesense of well-being, tendency to under-weight (in the first half of life), loss ofstrength, fatigability, susceptibility toinfection, carious teeth, sensitivity tocold, anorexia, constipation, abdominal
complaints, headache, insomnia, vaso-motor disorders of the skin and itsappendages, disturbances of men strua-tion, and loss of sexual desire. The pa-tients reported here offered subjectivecomplaints in the following order offrequency: constipation, general poorhealth, fatigability, weakness, loss ofweight, anorexia, headache, sensitivityto cold, frequent colds, insomnia, andabdominal distress. Lack of uniformityin recording the results of physicalexamination makes it somewhat diffi-
cult to appraise the thyroid factor fromthe objective data. Little importance

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 11/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 407
probably is to be attached to a 28 percent incidence of goiter in patients fromthe Great Lakes region (5.2). More sig-nificant perhaps is the finding ofexoph-thalmos in 8.5 per cent of the cases.A pasty complexion was noted in fiveinstances, non-pitting edema in one.A pale, cold, moist skin is one of thecommonest observations. Dilatation ofthe pupils (not measured) was recordedin 18 per cent of the cases. Both sw eat-ing and pupillary dilatation, usuallyincluded in lists of the physical signs ofschizophrenia, are among the few phe-nomena not part of the symptoma-tology of thyroid failure. Hypertri-chosis and inverted hair distribution,found in 23 per cent of the female sub-jects, are more suggestive of pituitary-ovarian hypofunction. Menstrual dis-orders were noted in 22 per cent of thewomen and tremors of the fingers,
tongue, or lips in 31 per cent of allthe patients. Dental caries was com-mon.
The concordance of the laboratoryfindings in schizophrenia and in hypo-thyroidism may be judged by com-paring the data in Table I with theresults obtained by Lawrence andRowe (28) in 126 cases of uncompli-cated thyroid deficiency (males, 29 percent; females, 71 per cent). One-thirdof the patients were underweight, 14
per cent of prediction. Decreasedweight, rather than obesity, is charac-teristic of the hypothyroid patient inthe first half of life (21). Pulse rate was66. In more recent reports the pulserate is described as slow or normal orrapid . Blood pressure was 114/71, pulsepressure 43 . The mean basal metabolicrate of all cases was minus 24. BloodN.P.N. was 31, dextrose, 96. Bloodcholesterol and carbon-dioxide com-bining power were not determined.Hypercho lesterolemia, it is well known,
is a regular concomitant of thyroid de-ficiency, and in thyroidectomized ani-
mals the carbon-dioxide combiningpower trends to low levels (50). Theblood cytological picture was: Hb, 87per cent; R.B.C., 4,840,000; C.I., 0.9;W.B.C., 7,500; and neutrophils, 56 percent. In the respects of lower systolicblood pressure, smaller pulse pressure,lower blood sugar level, and secondaryanemia the schizophrenic patients maybe said to be more "hyp othyroid" thanthe patients of Lawrence and Rowe.The correspondence between the twoconditions is seen further in the pres-ence in schizophrenia of tendencies toreduced lung volume (20), depressionof the specific dynamic action of pro-tein food (<?), low heat production inresponse to cold (7), hypochlorhydria(2), and delayed emptying-time of thecolon {21), all of which are part of thehypothyroid syndrome (4).
So similar are the physical symp-
toms, signs, and laboratory findings inthe two diseases that in reading theliterature on hypothyroid states onehas the impression of an ambiguousfigure: now it is hypothyroidism, nowschizophrenia. This agreement is basedmainly on statistical results. To whatextent does analysis of individual casesof schizophrenia bear out the thyroidfactor ? To ascertain this, the cases weresummarized and, where possible, anendocrine diagnosis was made. Hypo-
thyroidism was considered probable in39.5 per cent of the cases. The sum-maries were reviewed by Dr. WilliamF. Petersen, Professor of Pathology,and Dr. S. A. Levinson, Assistant Pro-fessor of Medicine and Director of theHospital Laboratory, of the Universityof Illinois College of Medicine, both ofwhom regarded the data consistentwith the diagnosis in the full 39.5 percent of the patients, and by Dr. S.Soskin, Assistant Professor of Physi-ology, University of Chicago, who
checked 22.5 per cent of the cases ashypothyroid. The following are sum-

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 12/17
408 JOSEPH C. RHEINGOLD
maries of cases which happened to be
listed first under each of the four
customary sub-groups:
1) Simple Type: Female, age 25.
History of loss of strength and energy,
poor appetite, constipation, frequent
colds, scanty menstruation, and emo-
tional apathy. Skin cold and rough.
Isthmus of thyroid gland enlarged.
Teeth carious. About 20 pounds under-
weight. T 97.8, P 80, R 16, B.P. 110/75.
B.M.R. —24 per cent, Choi. 277, CO2
56. Hb 55 per cent, R.B.C. 3,330,000,
N 58 per cent. No free HC1 in gas-
tric contents, fasting or after Ewald
meal.
2) Hebephrenic Type: Male, age 27.
Always delicate, frequent spells of
weakness, easy fatigue, constipation,
headaches. Wore coat on ward in warm
weather. Thyroid gland normal to pal-
pation. Skin pale, hands and feet cold
and moist. Tremor of fingers. About35 pounds underweight. P very vari-
able, frequently in 5o's. B.P. 112/80.
B.M.R.—27 per cent (after exercise —34 per cent). Choi. 333, CO2 52. Hb
70 per cent, R.B.C. 5,300,000, N 54
per cent.
3) Catatonic Type: Female, age 38.
Three previous episodes with improve-
ment. Stuporous. Skin cold, rough,
with many eczematous areas and scars.
Tendency to masculine hair distribu-
tion. Teeth in very poor condition.Thyroid gland diffusely enlarged and
soft. Amenorrhea. Drooling of saliva.
Deep reflexes increased, abdominals
not elicited. Vincent's angina. About
40 pounds underweight. T 97.6, P 70,
R 15, B.P. 98/70. B.M.R.—14 per cent
(single determination). Choi. 290,
N.P.N. 51, CO2 51. Hb 70 per cent,
R.B.C. 3,530,000, W.B.C. 10,700, N
63 per cent.
4) Paranoid Type: Male, age 31. Im-
pairment of general health for two
years prior to admission. Felt cold even
when wearing fur coat. Adenoma of
left lobe of thyroid gland. Moderate
exophthalmos. Unilateral Von Graefe
sign. Tremor of fingers. Weight normal.
P 64, B.P. 100/65, B.M.R—29 per
cent, Choi. 278, N.P.N. 38, CO2 46.
Hb 80 per cent, R.B.C. 4,300,000, N
45 per cent. Urine, albumin one plus.
Among 130 schizophrenic patients
Hoskins and Sleeper (/<?) found a
group of 18 (13.8 per cent) that showedthyroid deficiency, uncomplicated or
in association with other glandular
disturbance.
The greater incidence of cases of
hypothyroidism in the patients of the
Illinois Psychiatric Institute, as well
as the larger percentage of patients in
this group with low basal metabolic
rates and the tendencies to hyper-
cholesterolemia, acidosis, and second-
ary anemia, suggests that the Institute
patients are more "hypothyroid" than
the patients in the Worcester StateHospital. This difference was to be
expected. The inclusion of females in
the present series shifts the averages to
the left. Further, the patients in Chi-
cago are selected from a goiter region,
those in Worcester from a non-goiter
region.
The total evidence seems to give
considerable warrant to the theory that
insufficient thyroid function plays an
important part in creating the vegeta-
tive status of schizophrenia. Thispathogenetic tie may exist more or less
in all cases of schizophrenia or may be
pertinent to a certain group only. The
relationship between hypothyroidism
and the psychic phenomenology of
schizophrenia is outside of the limits of
this discussion. But the suggestion is
offered that, no matter whether the
metabolic and the mental characters
arise simultaneously or in sequence, the
hypothyroid state once established is
capable of perpetuating the signs refer-
able to the brain. Integrated brain
function, as McFarland (j5) and Gell-

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 13/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 409
horn (/<?) have shown, depends uponadequate oxygenation of the brain.Anoxia induced in normal subjectsproduces disorders of behavior re-sembling the symptoms of schizo-phrenia. (But are acute experimentswith low oxygen tension comparable tothe persistent deficiency of oxygen as-similation assumed to exist in theschizophrenic brain?) In addition tothe direct metabolism-depressing ef-fect, hypothyroidism, through second-ary disturbances of water and calciummetabolism (16) may exert furtherdampering effect upon brain activity.The assumption of thyroid insufficiencyoffers help too in accounting for certainphysiologic and physical anomalies inschizophrenia. Since the thyroid hor-mone apparently controls the excita-bility of the respiratory center (27), itsdeficiency explains the schizophrenic's
insensitivity to carbon-dioxide stimu-lation, a finding upon which Golla (14)builds a pathogenesis of the disease.The hypofunction of the sympatheticnervous system, recently emphasizedby Gellhorn (13), may be the result ofthe decreased sensitization of the mech-anisms upon which epinephrine acts.That schizophrenic subjects are unableto comply normally with the homeo-static principles concerned with theregulation of heat (15) follows from thepart the thyroid hormone plays in tem-perature regulation apart from its con-trol over the total heat production ofthe body. Finally, hypothyroidism mayaccount for reduced blood volume {16).The influence of the thyroid secretionon capillary growth and morphology(26) may be the more basic cause, asOlkon (41) finds a reduction in thenumber and size of the skin capillariesin schizophrenic patients .
Since it is generally agreed that func-tional thyroid disorders do not arise abinitio within the gland, the investi-gative problem becomes a search for
the cause or causes antecedent to thy-roid deficiency. It is now believed thatthe pituitary thyrotropic hormoneexercises the chief control over thyroidsecretion {34)- That the sympatheticnerves are not involved in the produc-tion of the hypometabolic status ofschizophrenia follows from Cannon'sfinding that even total extirpation ofthe symp athetic chains in cats does notresult in a significant lowering of basalmetabolism (3). Our path leads to theanterior pituitary lobe; and there itends, because the mechanisms thatregulate prehypophyseal function arestill too speculative to warrant con-sideration.
Another path opens up, however,when we bring into the discussion theremarkable resistance of schizophrenicpatients to the effects of thyroid medi-cation. The bulk of the evidence speaks
against the efficacy of thyroid medica-tion, although there are reported casesof a clear association between a schizo-phrenic syndrome and thyroid defi-ciency, with recovery from the psy-chosis following the use of thyroid sub-stance (16a, 53, 54). Also, several in-vestigators have had more or less suc-cess with thyroid therapy in unselectedcases (18), and negative results, accord-ing to Hoskins, are usually inconclusive(/<?). There is no report on the adminis-
tration , of thyroxin intravenously inearly cases. After a long experience withglandular treatment Hoskins (42) isimpressed with the schizophrenic's hightolerance for thyroid preparations evenin those cases showing the character-istic hypothyroid picture, and by theexhaustibility of the effect, as well asby the diminishing efficacy with re-peated courses of treatment. If thetherapeutic test is the ultimate diag-nostic criterion of hypothyroidism,must one conclude that the refractori-
ness of the schizophrenic contradictsthe assumption of thyroid deficiency?

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 14/17
410 JOSEPH C. RHEINGOLD
Only if by thyroid deficiency is under-stood just decreased production of thehormone. The above discussion hasbeen oriented to the premise of such anabsolute deficiency because this is theimplicit assumption in the literature onhypo thy roidism. But a relative lack of 'the hormone—its deficient use by thecells—is not only theoretically possiblebut is beginning to receive attention asan explanation of the failure of somehypothyroid patients to respond tothyroid therapy. If we suppose that theschizophrenic is unable to use thyroidsecretion, we resolve the antinomy be-tween hypothyroidism and resistanceto substitutive treatment. The defi-ciency is probably not wholly in theutilization of the hormone since pa-tients in a goiter area appear to sufferof a greater degree of hypothyroidismthan those in a non-goiter area and
some patients respond to thyroid ad-ministration, if only with temporarybenefit. Inadequate iodine supply is acause of lessened production of secre-tion and thus presumably a factor inthe liability to schizophrenia, but io-dine metabolism may not be of funda-mental import because the major dis-turbance apparently lies not in thesynthesis of the hormone but in itsavailability to the body.
What may interfere with the action
of the thyroid hormone? Since the se-cretion of the thyroid gland is notidentical with thyroxin and is effectiveonly after a long latent period, it hasbeen suggested that it undergoes modi-fication in the body before it acquiresphysiologic potency (/<5). In the schizo-phrenic this final elaboration may notoccur. It is possible too that the secre-tion or the definitive hormone may bedepotentiated by anti-hormone or bysome other anti-body. Anselmino andHoffmann (/) have isolated an ant i-thyroid substance from normal bloodand tissues which exerts protection
against the hormone. In Graves' dis-ease the titer of this principle is muchless than normal. The presence of anexcess of the anti-body in schizophrenicpatients would account for the hypo-thyroid state, the resistance to thyroidfeeding, and the diminishing efficacy ofrepeated courses of treatment, andwould make unnecessary the assump-tion of overproduction of the thyro-tropic hormone which is apparentlyrequisite for formation of the thyroidanti-hormone. Other substances withanti-thyroid action, recently enumer-ated by Oehme (40), need not be con-sidered because it is unlikely that anyof them exists in excess in the schizo-phrenic. Finally, the hormone mayreach the cells but may be unable toexert its effect because of the absenceof a positive catalyst or the presence ofa negative catalyst. I t has already been
pointed out that the results of the ad-ministration of dinitrophenol speakagainst such an assumption in schizo-phrenia.
There is question whether thyroxinacts upon the peripheral cells at all.Experiments testing the effect of thy-roxin upon the oxygen consumption ofliving cells in vitro have yielded nega-tive or uncertain results (jp). Isolatedorgans are not sensitized to stimulationby thyroxin, yet do show increased
excitability if the animal is preparedwith thyroxin beforehand {37). Cold-blooded animals show none of theeffects of thyroxin administration (25).
On the other hand, there is evidencethat the nervous system is the site ofaction of the thyroid hormone. Investi-gators like Leon Asher and Hans H.Meyer subscribe to the theory of anexclusive central action. On the as-sumption that cold-blooded animalsare insensitive to thyroxin because theylack vegetative centers for temperatureregulation, Issekutz and Issekutz (25)made cats poikilothermic by narcotiz-

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 15/17
AUTONOMIC INTEGRATION IN SCHIZOPHRENIA 41 1
ing them with a dose of phenobarbitallarge enough to paralyze the vegetativecenters and found that they were to-tally unresponsive to thyroxin. De-capitated animals and animals withsection of the cord in the third to thefifth cervical segments were similarlyunresponsive. Phenobarbital is capableof exerting protection against the sensi-tization by thyroxin to the effect ofdrugs which disturb the temperature-regulating center (44), and in humans,of depressing the calorigenic and di-uretic action of thyroxin {36). It is alsoknown that resistance to the effects ofadministered thyroxin may accompanycertain brain diseases (36).
Probably the most convincing evi-dence that the localization of action ofthe thyroid hormone is in the hypo-thalamus is offered by Schittenhelmand Eisler (45) who found that after
the injection of thyroxin into animalsthe iodine-content of the tuber cine-reum increases tenfold whereas otherparts of the brain are unaffected. Inthis connection it is interesting to notethat Morgan and Gregory (38), in ahistologic study of various cell groupsin the thalamic and subthalamic re-gions and in the corpus striatum of thebrains of psychotic subjects, twelve ofwhom had been diagnosed schizo-phrenic, found pathologic changes only
in the tuber cinereum—the substantiagrisea and the nucleus tuberis lateralis.Just how the hypothalamus mediates
the effect of the thyroid hormone is notknown. The sym pathetic nerves wouldseem to be a necessary link between thebrain and the cells and a certainamount of evidence supports this as-sumption, yet Ring, Dworkin, andBacq (47) have reported that removalof the thoraco-lumbar chains in catsdoes not prevent the usual rise inmetabolism after thyroxin.
On the strength of this newer knowl-edge of thyroid physiology the opinion
is ventured that in schizophrenia wedeal, not with a disturbance of thepituitary-thyroid mechanism, but witha dysfunction of the hypothalamus.Neither the naturally produced hor-mone nor the exogenously introducedhormone is effective because of theelimination of the mechanism which insome way is essential to the hormone'sultimate action. That the hypothala-mus may be implicated not alone inschizophrenia but in the psychosesgenerally has been suggested by per-sons of such wide experience as Singer{49), Hoskins (22), and Ingham (24).The postulate of a thyroid-hypothala-mus relationship offers a way of ap-proach to the experimental testing ofthe role of the hypothalamus in thepsychoses.
SUMMARY AND CONCLUSIONS
As a point of depar ture in a stud y ofautonomic integration in schizophreniathe vegetative status was defined bymaking a statistical analysis of theorganic findings in a reasonably homo-geneous group of 129 schizophrenicpatients. The most noteworthy ab-normality is a tendency to low oxygenconsumption rate. Low blood pressure,slightly elevated blood cholesterol con-tent, low normal carbon-dioxide com-
bining power, and secondary anemiaattest to a state of general hypo-metabolism. The female subjects arerelatively more hypometabolic thanthe male subjects. The clinical sub-groups show no consistent differences.
Low oxygen consumption is prob-ably an integral feature of the disease.Since it does not seem to be dependentupon an inadequate supply of oxyg'ento the tissues or upon intracellular en-zyme dysfunction, a disturbance of themechanisms regulating cell respiration
may be postulated.. Thyroid insuffi-ciency is probably one factor in the

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 16/17
412 JOSEPH C. RHEINGOLD
pathogenes i s . T h e s y m p t o m s , p h y s i c alt i e n t s w i t n
dementia praecox to cold, J. Neurol. &
signs, and laboratory findings in schizo- t.^^^f:^^^vMetai^ bei
p h r en i a and in the n o n - m y x e d e m a t o u s schizophrenen, Klin. Wchnschr. 6:1987,1927.
form of thy ro id fa i lu re are very s imi la r 9- FREEMAN, H. HOSKINS, R. G. and SLEEPER,
and in- the group of patients reported ^ ^X^^^™' ^the d iagnos is of h y p o t h y r o i d i s m is be- 10. FREEMAN, H. : The arm-to-carotid circulationl ieved t e n a b l e in 39.5 per Cent of the
t i m e innormal and schizophrenic subjects, Psy-
r a w . Th e s e n a t i e n r s are nn-narenrlv chiatric Quart. 8: 290, 1934.cases . I h e s e p a t i e n t s are a p p a r e n t l y FREEMAN> H . : Variability of circulation time in
m o r e h y p o t h y r o i d t h a n p a t i e n t s normal and schizophrenic subjects, Arch. Neurol. &s tud ied in the W o r c e s t e r S t a t e Hos- Psychiat.,^p.-488,1938.niral whn are males ev r lns ive lv anH n. FREEMAN, WILLIAM: The fasting blood sugar inp i t a i wno are males exclusively an d scmZophrenia, Am. J. M. Sc. 186:621,1933.who are Selected from a non-gOlter 12. GELLHORN, ERNST: The integrated action of theregion organism exemplified by studies on anoxemia, Sigma
Thyroid hypofunction serves to e x - ^X
^ La» o ^ R t ;
9 3 7E f f e c t s o f h y p o g l y c e m i a a n d
pla in s o m e of the m e n t a l as well as they \ anoxia on the central nervous system, Arch. Neurol.
m e t ab o l i c p h e n o m e n a and a c c o u n t s for&
Psychiat. 40:125,1938.certain physiologic abnormalities com-
l^^^^Lt^^\^
m o n l y o b s e r v e d in sch izophren ia . j . Mem. Sc. 74: 443,1928.The schizophrenic's lack of response '5- GOTTLIEB, JACQUES S. and LINDER, FORREST E.:
rn t-lwrnirl feerlino- rlnes n n t nereSQar i luB o d y t e m
Pe ra (
:u r
es of persons with schizophrenia
,, 7 ,t e e C l m
,g d
°e S
rn,O t n e c e s s a r i l
y and of normal subjects, Arch. Neurol. & Psychiat.
nullify the p o s t u l a t e of thyroid insuffi- 33: 775,1935.ciency s ince the t h y r o id h o r m o n e a p - 16. HARINGTON, CHARLES ROBERT: The Thyroid
pears to act through the hypothalamus ^ ^ ^ ^ w^ts? A^ EWand a d iencepha l lC d is tu rbance wou ld N. : Mental derangement in hypothyroidism,
acco u n t for b o t h the h y p o t h y r o i d s t a t e J.A.M.A. 97.-164,1931.and the resistance to the effects of ad- ^ ^ m I % £ ^ ^ l 5 ^ " 2minis te red t h y r o id s u b s t a n c e . Th e thy- Psychiat. 21:887,1929.roid insufficiency may be r e l a t i v e
l8- HOSKINS, R. G. and SLEEPER, F. H.: The thy-
ra ther than absolute . ^ I T ' I ^ Od e m e n d a PraeC
°X> Am
'J'
P s y c h i a t'
19. HOSKINS, R. G.: Oxygen consumption ("Basal
Metabolic Rate") in schizophrenia, Arch. Neurol. &
B I B L I O G R A P H Y Psychiat. 28:1346,193a.
20. H O S K I N S , R. G. and S L E E P E R , F. H.: Organic
1. ANSE L MINO, KARL JUL IUS and H O F F M A N N , F R I E D - functions in schizophrenia, Arch. Neurol. &
RICH: Darstellung, Eigenschaften und Vorkomm en Psychiat. jo.- 123,1933.einer antithyreoiden Schutzsubstanz aus Blut und 21. HOSKINS, R. G. and JELLINEK, E. MORTON: T heGeweben, Klin. Wchnschr. 12: 99, 1933. Schizophrenic Personality with Special Regard to
2. BOWMAN, KARL M .: Endocrin an d biochemical Psychologic an d Organic Concomitants , Chap,studies in schizophrenia, J. Nerv . & Ment . Dis. 65: X I I I , Th e Proceedings of the Association for Re-465, 1927. ' . search in Nervous and Mental Disease, Vol. XIV ,
3. C A N N O N , W. B., N E W T O N , H. F. , B R I G H T , E. M. 1933.
an d MENKIN, V.: Some aspects of the physiology • 22. HOSKINS, R. G.: The Problem of Menta l Dis-
of animals surviving complete exclusion of sym- order, Section on Endocrinology, McGraw-Hill,pathetic nerve impulses, Am. J . Physiol . 89: 84 , Inc. New York, 1934.
1929. 23. HOSKINS, R. G.: Oxygen metabolism in schizo-4. ENGELBACH, WILLIAM: Endocrine Medicine, Vol. phrenia, Arch. Neurol. & Psychiat . 38: 1261, 1937.
I l l , Charles C Thomas, Springfield, 1932. xs/24. INGHAM, SAMUEL D .: Some neurologic aspects5. FARQUARSON, R. F. and HYLAND, H . H.: Anor- of psychiatry , J .A.M.A . / / / : 665, 1938.
exia nervosa, J.A.M.A. / / / : 1085,J93^- 25. ISSEKUTZ, B. V. an d ISSEKUTZ, J R . , B. V. : An -
6. FINESINGER, JACOB E., COHEN, MANDEL E. and griffsort des Thyroxins, Klin. Wchnschr. 13: 1060,
THOMSON, K. JEFFERSON: Velocity of blood flow 1934-
in schizophrenia, Arch. Neurol. & Psychiat . 39: 24, 26 . JAENSCH, W. : Grundzuge einer Physiologie und1936. Klinik der psycho-physischen Personlichkeit,
7. FINKELMAN, I. and STEPHENS, W. MARY: He at Springer, Berlin, 1926.
regulation in dementia praecox: Reactions of pa- 27 . LANDOLT, HERMANN: Die einvirkung.von Thy-

8/9/2019 Autonomic Integration in Schizophrenia
http://slidepdf.com/reader/full/autonomic-integration-in-schizophrenia 17/17
A U T O N O M I C I N T E G R A T I O N IN S C H I Z O P H R E N I A 41 3
r*
roxin auf das Zentralnervensystem bzw. Atemzen-trum beim Kaninchen, Z tschr. f. Biol. go : 327, 1930.
28. LA WREN CE, C. H. and R O W E , A. W.: Studies of
the endocrine glands: III . The Thyroid , Endo-crinology 12 : 377, 1928.
29. LEVINSON, SAMUEL A. and M A C F A T E , R O B E R T
P. : Clinical Laboratory Diagnosis, Lea and
Febiger, Philadelphia, 1937.30. LEWIS , N O LA N D. C : Research in dementia
precox, Northern Masonic Jurisdiction of the
Scottish Rite, 1936.31. LOONEV, JOSEPH M. and CH ILD S , H A ZEL M .:
The blood cholesterol in schizophrenia, Arch.Neurol . &Psychiat . 30 : 567, 1933.
32. LOONEY, J. M. and H O S K I N S , R. G.: Th e effect
of dinitrophenol on the metabolism as seen in
schizophrenic patients, New England, J. Med. 2/0:
1206, 1934.33. LOONEY, J. M. and F REEMA N , H. : Oxygen and
carbon dioxide contents of arterial and venous bloodof schizophrenic patients, Arch. Neurol. &P sychia t.j p : 276, 1938.
34. MA RIN E, D A V ID : The physiology and principal
interrelations of the thyroid, Symposium: Gland-ular Physiology and Therapy, A, M. A., Chicago,
1935-
35. MCFARLAND, R. A.: The psychological effect of '
oxygen deprivation (anoxemia) on human behavior,Arch. Psychol. No. 145, 1932.
36. MEYER, H . E. : Uber die Beziehungen zwischenSchilddriise und Zentralnervensystem, Zntrlbl. f.Inn. Med. 38 : 209, 1937.
37.. MEY ER, H A N S H.: Ueber Art und Ort der
Thyroxinwirkung, Arch, internat. de Pharmacodyn.et de Therapie 38 : 1, 1930.
38. MO RG A N , LA WREN CE 0. and G REG O RY , H U G H S. :
Pathological changes in the tuber cinereum in agroup of psychoses, J . Nerv. & Ment. Dis . 82:286, 1935.
39. OBERDISSE, K.: Stoffwechseluntersuchungen zur
Frage des Angriffspunktes der Schilddriisensub-stanz, Arch. f. Exp. Path . u . Pharm. 162: 150, 1931.
40. O EH ME, CU RT: Zur Beurteilung anti-thyreoid-
aler Wirkungen, insbesondere de s Glykokolls,Deutsche. Med. Wchnschr. 63 : 1573, 1937.
41. O LK O N , D A V ID M.: Paper submitted for pub-
lication.42. Personal Communication.
43. P ETERS EN , WILLIA M F.: The Pati ent and the
Weather, Vol. 1, Par t 2: Autonomic Integration,Edwards Bros., Inc., Ann Arbor, Mich., 1936.
44. PICK, E. P. : Ueber Beziehungen der Schilddriise
zum vegetativem Nervensystem, Deutsche. Med.Wchnschr. 57: 1532, 1931.
45. SCHITTENHELM, A. and E I S L E R , B.: Thyroxin
und Zentralnervensystem, Klin. Wchnschr. / / : 9,
1932.
46. SANTENOISE, D .: Pneumogastrique, ApparielThyroidien et Activity Ce>6brale, Am&ie'e Legrand,Paris, 1929.
47. RIN G , G. C , D W O R K I N , S. and BACO_, Z. M.:
Basal metabolism after thyroxin in sympathectom-ized animals, Am. J . Physiol. p7: 31J, 1931.
48. SEWA RD, BLANTON P. : A clinical stud y of the
mild grades of hypothyroidism, Ann. Int. Med. 9:
178, 193S-
49. SINGER, H . D O U G LA S : Psychosis and the central
autonomic nervous system, J.A.M.A. no: 2047,1938.
50. Personal Communication from Dr. S. Soskin,
Director of Metabolic an d Endocrine Research,Michael Reese Hospital, Chicago.
J I . WIG G ERS , CA RL J.: Physiology in Health and
Disease, Lea and Febiger, Philadelphia, 1937.
J 2 . WA RF IELD , LO U IS M.; Hypothyroidism , J.A.-
M.A. g§ : 1076, 1930.
53. WILTRA K IS , G EO RG E A. and P A R I I P I L O , A N -
THONY V.: Non-myxedematous hypothyroidism,
case repo rted with psychosis, 111. Med . J . 74 : 359,1938.
54. ZIEGLER, LLOYD H .: Psychosis associated withmyxoedema, J . Neurol. an d Psychopath. / / : 20,
1930.