Auto Anti-coagulation and VTE Prophylaxis
38
Auto Anti-coagulation and VTE Prophylaxis Hilary Rowe, BScPharm VIHA Pharmacy Resident 2009-10 Internal Medicine Rotation November 5th, 2009
description
Auto Anti-coagulation and VTE Prophylaxis. Hilary Rowe, BScPharm VIHA Pharmacy Resident 2009-10 Internal Medicine Rotation November 5th, 2009. Outline. Objectives Patient Case Background Clinical Question Review of Evidence Recommendation Monitoring. Objectives. - PowerPoint PPT Presentation
Transcript of Auto Anti-coagulation and VTE Prophylaxis

Auto Anti-coagulation and VTE Prophylaxis
Hilary Rowe, BScPharm
VIHA Pharmacy Resident 2009-10
Internal Medicine Rotation
November 5th, 2009

Outline
• Objectives
• Patient Case
• Background
• Clinical Question
• Review of Evidence
• Recommendation
• Monitoring

Objectives
• Review pathophysiology for auto anti-coagulation & clinical presentation
• Discuss evidence of auto anti-coagulation• Discuss therapeutic options for VTE
prophylaxis

Mr. JE
• ID: 33 yo Caucasian male, ht 170cm, wt 55kg
• CC: ER by ambulance Sept 1/09 for weakness & falls-jaundice, ascites
• HPI Oct 19/09: Small esophageal varices, ascites
• PMHx: chronic lower back pain, alcohol abuse x 14 years

Mr. JE
• Meds PTA: None
• Allergies: None
• SH: Homeless, estranged from family, smoker (30 pack yr hx), drinks 26 oz (780mL) vodka a day x 14 yrs
• Discharge Plan: To family

Review of Systems
System Findings Medications
CNS •Alert and Oriented x 3•Difficulty sleeping in hospital
Zopiclone 3.75 mg at hs prn
HEENT Unremarkable
Psych Anxiety, headache, seizures CIWA protocol

Review of Systems
System Findings Medications
Resp Unremarkable
Cardio Unremarkable
GI •No hematemesis, •FOB neg x 3•Endoscopy small esophageal varices
Nadolol 40mg od

Review of Systems
System Findings Medications
Liver •Alcoholic liver cirrhosis•Ascites•Negative paracentesis cultures
•Furosemide 100mg daily•Spironolactone 100mg bid
GU •SrCr 76 •CrCl 95ml/min

Review of Systems
System Findings Medications
Heme •↓ Hgb 101, MCV 98, ↑ RDW 21.4, ↓ Plt 92•Iron 8 ↓ , ferritin 50, B12 535, RBC folate 1134•↑ INR 1.9, ↑ Tbili 361, ↓Alb 25, ↑ GGT 78, ALP 129, ↑ AST 81
•Fe fumarate 600mg at hs•Multivitamin daily
Fluids & Lytes
↓ Na 125, K+ 4.3, ↓ Cl 89

Medical Problems List
• Alcohol addiction
• Alcoholic cirrhosis
• Ascites
• Esophageal varices
• Anemia of chronic disease & iron deficiency anemia
• Chronic lower back pain

DRP’s
• JE is at increased risk of COPD, CVD and cancer secondary to smoking, requiring tobacco cessation counseling
• JE has a mixed anemia secondary to iron deficiency and anemia of chronic disease, requiring monitoring of his anemia therapy

DRP’s
• JE is at an increased risk of VTE requiring assessment of his need for DVT prophylaxis despite his elevated INR of 1.9

Alcoholic Liver Cirrhosis
• Decrease in pro-coagulants– Can’t make II, VII, IX, X
• Decrease in anti-coagulants– Can’t make Protein C, S & antithrombin III
• PT & INR measures activity of pro-coagulants and doesn’t capture changes in anti-coagulants
• PT does not predict bleeding risk

Risk Factors For VTE
• Recent surgery or major trauma • Immobility or paralysis • Malignancy • Previous VTE • >80 years • Smoking• Varicose veins • Inherited or acquired thrombophilia

Rounds
• Team discussed that patient had been in hospital for a significant amount of time and might need VTE prophylaxis
• Team wanted to know if his elevated INR of 1.9 would protect him?
CTU Discussion

Clinical Question
P33 year old male with an elevated INR secondary to alcoholic liver disease
I VTE Prophylaxis
C No VTE Prophylaxis
O
Reduce the risk of DVT and PE
Reduce morbidity and mortality
Decrease hospitalization

Search Strategy
• PubMed, Embase, Google• Search terms:
– Liver cirrhosis– Risk of Thromboembolism– DVT, Pulmonary embolism– Auto anticoagulation
• Found– 2 retrospective case control studies

Northup et al. Am J Gastroenterol 2006
DesignRetrospective matched case control study 1993-2001
P•Patients from all admissions (medical, ICU, surgical) with cirrhosis assessed for diagnosis of VTE during hospitalization
I•Patients with an elevated prothrombin time and INR from cirrhosis with a VTE
C•Patients with an elevated prothrombin time and INR from cirrhosis without a VTE
O•VTE in cirrhosis patients: DVT, PE & both•Serum albumin

Northup et al. Am J Gastroenterol 2006
Inclusion & exclusion:•Patients from all admissions, (medical, ICU, surgical) with cirrhosis assessed for diagnosis of VTE during hospitalization•Matched with a cirrhotic patient with the same gender, age, race, # comorbidities, presence of cancer, occurrence & type of surgery•Excluded if previous VTE or portal vein, splanic vein, mesenteric vein or central line VTE

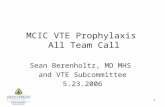
Northup et al. Am J Gastroenterol 2006
•Lower albumin in patients with VTE
*38-53g/L normal, 1g/dL=10g/L
•Elevated INR did not protect patients from VTE

Northup et al. Am J Gastroenterol 2006
Results:•VTE in cirrhosis patients 113/21,000 (0.5%)
-74/113 (65.5%) DVT
-22/113 (19.5%) PE
-17/113 (15%) Both DVT & PE
-Serum albumin independently predicts VTE (p<0.001, OR 0.24 95% CI 0.10-0.55)

Northup et al. Am J Gastroenterol 2006
Limits:•Retrospective•No “gold standard” for VTE diagnosis so events could have gone undetected•Small sample size = higher type II error•Factors that may have been unmatched•21% had prophylaxis (33% medically, rest SCD’s)•Did not discuss # in each group who got prophylaxis

Northup et al. Am J Gastroenterol 2006
Conclusions• Deficiencies of antithrombin III, protein C &
protein S are associated with ↑ risk of VTE• Serum albumin may be indicator for level of
proteins made by liver such as Antithrombin III, protein C & S
↑ INR does not decrease risk of VTE

Sogaard et al. Am J Gastroenterol 2009
Design Retrospective case control study 1980-2005
P•Patients with a discharge diagnosis of DVT or PE
I •Patients that developed a VTE
C •Patients that didn’t develop a VTE
O•Assessed association between liver disease & overall risk of VTE and unprovoked VTE

• Unprovoked VTE=patient without diagnosis of cancer before or within 90 days of VTE, or diagnosis of fracture, trauma, surgery, pregnancy 90 days before VTE
• Each case matched with 5 population controls without a VTE by age, gender, county
• Patients with several VTE’s had their first event used
Sogaard et al. Am J Gastroenterol 2009

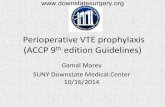
Sogaard et al. Am J Gastroenterol 2009

Results• 20% (99,444/496,872) had a VTE• 22% (67,519/308,614) had unprovoked VTE
Sogaard et al. Am J Gastroenterol 2009

Limits
• Retrospective
• Relied on coding of Danish nationwide registry for diagnosis of VTE
• No data on lifestyle factors
• Declining risk of VTE in past 10 years– Is this due to prophylaxis?
Sogaard et al. Am J Gastroenterol 2009

Conclusion
• Both cirrhotic and non-cirrhotic liver disease are risk factors for VTE
Sogaard et al. Am J Gastroenterol 2009

Goals of Therapy
Patients Goals• Abstinent from alcohol
Team Goals• Prevent VTE• Prevent hospitalization• Decrease morbidity & mortality• Minimize adverse drug events• Keep patient abstinent (quality of life)• Find housing (quality of life)

Therapeutic Options
•No DVT prophylaxis
•Sequential compression devices
•Heparin 5000 units sc bid
•Dalteparin 5000 units sc daily

Recommendation
• Dalteparin 5000 units subcutaneous daily• Try to mobilize patient as soon as possible• Initiate smoking cessation counseling

Monitoring
Adverse Events
Monitor Who When How Long
Pain & bruising at inj site
Patient After inj Daily while on therapy
Bleeding-in urine, bowel, nose etc.
Patient & nurse
Daily-after urination, bowel movements etc.
Daily while on therapy

Monitoring
Efficacy
Monitor Who When How Long
Shortness of breath
Patient & Physician
Daily Duration of therapy
Pain in the legs
Patient & Physician
Daily Duration of therapy
Redness & Swelling in legs
Patient & Physician
During physical exam
Duration of therapy

summary
Question: Does elevated INR protect patient from a VTE?
Answer:• ↑ INR does not decrease risk of VTE• ↓ albumin independently predicts VTE risk
Future:• Study VTE prophylaxis in this population &
predict benefit & risk of bleed
Summary

Questions?

References
• Northup PG, McMahon MM, Ruhl AP et al. Coagulopathy does not fully protect hospitalized cirrhosis patients from peripheral venous thromboebolism. Am J Gastroenterol 2006;101:1523-28.
• Sogaard KK, Horvath-Puho E, Gronbaek H et al. Risk of venous thromboembolism in patients with liver disease: a nationwide population-based case-control study. Am J Gastroenterol 2009;104:96-101.