ÆTIOLOGY OF BURKITT'S LYMPHOMA
2
200 progress of a number of families referred within their departments: a senior social worker, the superintendent health visitor, a paediatrician, and the consultant child psychiatrist. Its function complements that of the ad-hoc case- conferences summoned for children at urgent risk, and through having a bird’s-eye view of the total community situation the group has accumulated a certain pool of local wisdom about support systems and is developing ideas on prevention. We would be most grateful to be contacted by anyone with similar experience. 75 Sea Mills Lane, Bristol 9. ANTHONY C. FAIRBURN. HUMAN PLACENTAL LACTOGEN AND THE MANAGEMENT OF HIGH-RISK PREGNANCY SIR,-Measurement of human placental lactogen (H.P.L.) in maternal serum has been proposed by several investi- gators as a means of predicting the outcome of pregnancies at high risk for fetal jeopardy.1-6 Letchworth and Chard 7 suggested H.P.L. assays as a routine screening test in preg- nancy at each antenatal visit on all pregnant patients. Their Fig. 1-Mean H.P.L. values (0) and regression analysis at weekly intervals during the last half of pregnancy. data suggest that this immense laboratory undertaking would be rewarded by the antenatal identification of a significant number of infants destined for fetal distress and neonatal asphyxia. To date at least three groups of workers,2,5,7 using independent immunoassay methods, various purified H.P.L. standards, and separate antibody preparations, have delineated identical normal ranges in pregnancy. This reproducibility enhances the prognostic significance of values below 4 µg. H.P.L. per ml. of maternal serum during the fourth quartile of pregnancy. To ascertain the normal range of H.P.L. throughout the last half of pregnancy and to evaluate the optimum period in gestation to begin prospective serial analysis of H.P.L., 173 normal pregnancies were studied in the antenatal clinics of the Boston Hospital for Women, lying-in division. Serum-H.P.L. content was measured by micro-complement- fixation. 2 The results were analysed for covariance and 1. Saxena, B., Emerson, K., Selenkow, H. New Engl. J. Med. 1969, 281, 255. 2. Zuckerman, J. E., Fallon, V., Tashkian, A., Levine, L., Friesen, H. J. clin. Endocr. 1970, 30, 769. 3. Josimovich, J., Kosor, B., Boccella, L., Mintz, D., Hutchinson, D. Obstet. Gynec. 1970, 36, 244. 4. Singer, W., Desjardins, P., Friesen, H. ibid. p. 220. 5. Spellacy, W., Teoh, E., Buhi, M., Birk, S., McCreary, S. Am. J. Obstet. Gynec. 1971, 109, 588. 6. Keller, P., Baertschi, U., Bader, P., Gerber, C., Schmid, J., Solter- man, R., Kopper, E. Lancet, 1971, i, 729. 7. Letchworth, A., Chard, T. ibid. 1972, i, 704. Fig. 2-Regression analysis of mean H.P.L. levels for the 3rd and 4th quartiles of pregnancy. statistical significance of the level of H.P.L. relative to the duration of pregnancy. Fig. 1 shows the means and the regression analysis of the pooled data for the last 20 weeks of pregnancy. When these data were analysed separately for the last two quartiles of pregnancy (fig. 2), the slope (b) was found to be significantly steeper during weeks 31-40. This more rapid increase in maternal serum H.P.L. con- centration during the last 10 weeks of pregnancy serves to delineate more sharply those values deviating from normal in high-risk pregnancies characterised by placental insufficiency. The indication is that meaningful information can be derived from the serial measurement of H.P.L. begun after the 30th week, even if samples are not obtained at every antenatal examination. This consideration may be of particular importance in those areas of obstetrics where a premium’is placed on simplicity of method both in the clinic and supporting laboratory. Department of Obstetrics and Gynecology, Harvard Medical School, Boston, Massachusetts 02115, U.S.A. JAMES E. ZUCKERMAN. ÆTIOLOGY OF BURKITT’S LYMPHOMA SIR The reasons advanced by Dr Sadoff (Dec. 30, p. 1414) are persuasive, but none the less pyrimethamine may not be a cause of Burkitt’s lymphoma, and the Burnet theory of tumours has yet to be proved. Few, if any, patients with lymphomas associated with Hashimoto’s thyroid- itis, systemic lupus, cceliac disease, and myasthenia gravis received immunosuppressive drugs. The tumours occurring with renal transplants may likewise have arisen from the altered immunity rather than from the immuno- suppressants used to prevent rejection. The insult of transplantation may add up to a whole lifetime of immune experience, crammed into a few months. Time appears to be accelerated in this way, so that the risk of malignancy is much increased. When immune mechanisms are greatly stimulated by chronic infections, the normal inhibition of cell division is likely to become uncontrolled and tumours may result. On average, at least 40 years elapse before can- cer declares itself. But once it has developed, more and not less immunosuppression may be advisable during treatment. even though drugs with " antifol " activity are toxic. Immunocytes probably eliminate cells which initially are wrongly built. This policing of the body is presumably physiological. Invasion of human tissue, however, by external agents, such as plasmodia, mycobacteria, or the transmissible sarcoid agent, may lead to a different and sometimes sinister type of gang-warfare. Immune sur- 8. Snedecor, G., Cochran, W. Statistical Methods; p. 135. low 1967.
Transcript of ÆTIOLOGY OF BURKITT'S LYMPHOMA

200
progress of a number of families referred within theirdepartments: a senior social worker, the superintendenthealth visitor, a paediatrician, and the consultant child
psychiatrist.Its function complements that of the ad-hoc case-
conferences summoned for children at urgent risk, andthrough having a bird’s-eye view of the total communitysituation the group has accumulated a certain pool oflocal wisdom about support systems and is developingideas on prevention.We would be most grateful to be contacted by anyone
with similar experience.75 Sea Mills Lane,
Bristol 9. ANTHONY C. FAIRBURN.
HUMAN PLACENTAL LACTOGEN AND THEMANAGEMENT OF HIGH-RISK PREGNANCY
SIR,-Measurement of human placental lactogen (H.P.L.)in maternal serum has been proposed by several investi-gators as a means of predicting the outcome of pregnanciesat high risk for fetal jeopardy.1-6 Letchworth and Chard 7
suggested H.P.L. assays as a routine screening test in preg-nancy at each antenatal visit on all pregnant patients. Their
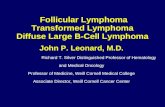
Fig. 1-Mean H.P.L. values (0) and regression analysis at weeklyintervals during the last half of pregnancy.
data suggest that this immense laboratory undertakingwould be rewarded by the antenatal identification of a
significant number of infants destined for fetal distressand neonatal asphyxia. To date at least three groups ofworkers,2,5,7 using independent immunoassay methods,various purified H.P.L. standards, and separate antibodypreparations, have delineated identical normal ranges in
pregnancy. This reproducibility enhances the prognosticsignificance of values below 4 µg. H.P.L. per ml. of maternalserum during the fourth quartile of pregnancy.To ascertain the normal range of H.P.L. throughout the
last half of pregnancy and to evaluate the optimum periodin gestation to begin prospective serial analysis of H.P.L.,173 normal pregnancies were studied in the antenatalclinics of the Boston Hospital for Women, lying-in division.Serum-H.P.L. content was measured by micro-complement-fixation. 2 The results were analysed for covariance and
1. Saxena, B., Emerson, K., Selenkow, H. New Engl. J. Med. 1969,281, 255.
2. Zuckerman, J. E., Fallon, V., Tashkian, A., Levine, L., Friesen, H.J. clin. Endocr. 1970, 30, 769.
3. Josimovich, J., Kosor, B., Boccella, L., Mintz, D., Hutchinson, D.Obstet. Gynec. 1970, 36, 244.
4. Singer, W., Desjardins, P., Friesen, H. ibid. p. 220.5. Spellacy, W., Teoh, E., Buhi, M., Birk, S., McCreary, S. Am. J.
Obstet. Gynec. 1971, 109, 588.6. Keller, P., Baertschi, U., Bader, P., Gerber, C., Schmid, J., Solter-
man, R., Kopper, E. Lancet, 1971, i, 729.7. Letchworth, A., Chard, T. ibid. 1972, i, 704.
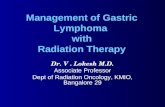
Fig. 2-Regression analysis of mean H.P.L. levels for the 3rdand 4th quartiles of pregnancy.
statistical significance of the level of H.P.L. relative to theduration of pregnancy. Fig. 1 shows the means and theregression analysis of the pooled data for the last 20 weeksof pregnancy. When these data were analysed separatelyfor the last two quartiles of pregnancy (fig. 2), the slope (b)was found to be significantly steeper during weeks 31-40.This more rapid increase in maternal serum H.P.L. con-centration during the last 10 weeks of pregnancy serves todelineate more sharply those values deviating from normalin high-risk pregnancies characterised by placentalinsufficiency.The indication is that meaningful information can be
derived from the serial measurement of H.P.L. begun afterthe 30th week, even if samples are not obtained at everyantenatal examination. This consideration may be of
particular importance in those areas of obstetrics where apremium’is placed on simplicity of method both in theclinic and supporting laboratory.
Department ofObstetrics and Gynecology,Harvard Medical School,
Boston, Massachusetts 02115, U.S.A. JAMES E. ZUCKERMAN.
ÆTIOLOGY OF BURKITT’S LYMPHOMA
SIR The reasons advanced by Dr Sadoff (Dec. 30,p. 1414) are persuasive, but none the less pyrimethaminemay not be a cause of Burkitt’s lymphoma, and the Burnettheory of tumours has yet to be proved. Few, if any, patientswith lymphomas associated with Hashimoto’s thyroid-itis, systemic lupus, cceliac disease, and myastheniagravis received immunosuppressive drugs. The tumours
occurring with renal transplants may likewise have arisenfrom the altered immunity rather than from the immuno-suppressants used to prevent rejection. The insult oftransplantation may add up to a whole lifetime of immuneexperience, crammed into a few months. Time appearsto be accelerated in this way, so that the risk of malignancyis much increased. When immune mechanisms are greatlystimulated by chronic infections, the normal inhibitionof cell division is likely to become uncontrolled and tumoursmay result. On average, at least 40 years elapse before can-cer declares itself. But once it has developed, more and notless immunosuppression may be advisable during treatment.even though drugs with " antifol
" activity are toxic.Immunocytes probably eliminate cells which initially are
wrongly built. This policing of the body is presumablyphysiological. Invasion of human tissue, however, byexternal agents, such as plasmodia, mycobacteria, or thetransmissible sarcoid agent, may lead to a different andsometimes sinister type of gang-warfare. Immune sur-
8. Snedecor, G., Cochran, W. Statistical Methods; p. 135. low1967.

201
veillance is probably preserved, but the intense stimulationcan produce several unpleasant side-effects. For instance,altered globulins secreted during the humoral responsemay cause hyperthyroidism, thrombocytopenia, or perhapsmyasthenia, while sensitised lymphocytes may later destroymany parenchymal cells, so that organs may fail. One end-result of the conflagration is
"
acquired immune deficiency ",but, even then, the increased liability to neoplasms remains,as long as the cell-mediated immunity persists. Those" pseudolymphomas
" and " invasive thymomas " which
surprisingly heal themselves, may be end-stages of sarcoid-osis. Unless lymphocyte sensitisation tests prove to be
specific in this disease, however, the diagnosis can be madeonly unsatisfactorily, by exclusion.
Wood Cottage,Chilworth,Surrey. GERALD A. MACGREGOR.
A NEW LYMPHOMA SYNDROME
SIR,-It is a pity that your interesting leading article on" sinus histiocytosis with massive lymphadenopathy "(Jan. 20, p. 139) carried the misleading title " a new lym-phoma syndrome " and that the disease is referred to as"
a new lymphoma ". As the article states elsewhere, thedisease " does not seem a malignant process ", and as
Rosai and Dorfman 1 state, " malignant lymphoma can be
excluded on clinical and pathological grounds ". Theclinical and histological features, indeed, strongly suggesta specific infective lesion. At present, an increasingnumber of lymphadenopathies, which might previouslyhave been labelled as lymphomas, are being recognised asreactive processes to a host of viral or other stimuli. It is
important, therefore, that this new lymphadenopathy shouldnot be lightly labelled as a neoplasm, or treated as such.
Christie Hospital andHolt Radium Institute,
Withington,Manchester M20 9BX. O. G. DODGE.
TUTANKHAMUN’S BREASTS
SIR,-George III must bear a heavy responsibility forthe current popularity of retrospective diagnosis uponhistorical figures. In your columns it has been proposedthat Tutankhamun suffered from adrenal feminisation(Dec. 16, p. 1312) and Klinefelter’s syndrome or Wilson’sdisease (Jan. 13, p. 109). It is true that some figures of thePharaoh do show female breast development and a saggingabdominal wall. The medical historian (clinical) shouldbear in mind, however, that such abnormalities are mildcompared with those shown by representations of hisimmediate predecessor, Akhenaten, who is represented insuch a grotesque and effeminate form that the diagnosisof Frohlich’s syndrome has been entertained.3 Even moreworrying for the retrospective diagnostician, members ofAkhenaten’s male entourage (e.g., Bek, the Master of
Works) are also shown as having female breast develop-ment which greatly exceeds that of Tutankhamun. Whilstclose in-breeding was common, it seems improbable tosay the least that pathological feminisation had reachedsuch epidemic proportions in the New Kingdom. It ismore likely that a style of representing the human formpersisted for a while after the death of Akhenaten. Thelatter’s influence is evident in other articles in Tutankha-mun’s tomb,4 which may date from the earlier part ofTutankhamun’s reign. Strong evidence is surely needed
1. Rosai, J., Dorfman, R. F. Cancer, 1972, 30, 1174.2. Butler, J. H. Natn. Cancer Inst. Monogr. 1969, 32, 233.3. Aldred, C. Akhenaten. London, 1968.4. Desroches-Noblecourt, C. Tutankhamun. Harmondsworth, 1965.
before we can accept the hypothesis that Tutankhamuninherited anything but an artistic convention from hiscurious predecessor.Department of Medicine,
Royal Infirmary,Manchester M13 9WL. J. D. SWALES.
TREATMENT OF VARICOSE VEINS
SIR,-We read with great interest the two articles 1,2on varicose veins, but we disagree profoundly with theconclusions. In a personal series (R. A. N.), more than4000 operations have been performed for varicose veins,and a larger number of patients have received only injec-tions. At present, a complete stripping for varicose veinsis being performed on a fully ambulatory basis (generalanaesthesia). The entire procedure has also been per-formed under local anxsthesia. The patient is admittedat 7.30 A.M. and is discharged at 5 P.M. that same day. Heis instructed to return to work and all usual activities theday after surgery. With this technique there has been agreat saving of hospital beds and work-hours lost to
industry. Chant et al.1 state that " there is no significantdifference between the results of these two forms oftreatment ". This has not been our experience. Everypatient is different and should be treated individually.If there are large varicose veins and severe valvular
insufficiency at the saphenofemoral junction or short-
saphenous/popliteal vein junction, operative treatment hasbeen very effective and injection treatment is followed by ahigh recurrence-rate. On the other hand, if the varicoseveins are scattered and there is no retrograde flow resultingfrom severe valvular insufficiency, injection treatment is
very effective. The authors also describe the operativetechnique as follows: " If the route of the stripper passedclose to the site of the i.p.v.s and associated varicosities,a simple strip was performed." In our experience, theoperative results are not satisfactory unless each and everysite of valvular insufficiency is ligated flush with the deepveins. In order to compare surgery and injection treat-ment, the surgical technique considered must be meticulous.The success of operation depends proportionately uponthe ability of the surgeon to detect and excise all sourcesof valvular insufficiency at their source. Many patientshave been operated upon several times and large varicescontinue to recur because the saphenous veins had notbeen ligated flush with the femoral or popliteal veins orincompetent perforators had been missed.The article 1 also states that " It is less disruptive to
family life to make six or seven attendances at an out-
patient clinic than to make the arrangements needed foradmission to hospital that may last two to three days orpossibly much longer." With the ambulatory surgicaltechnique there is very little disruption of family life. In
addition, an elastic support is necessary for one week
postoperatively, whereas with the injection/compressiontechnique the bandage is often used for six weeks or more.This extended use of a compression bandage would notbe acceptable to many of our patients.
Piachaud and Weddell 2 say that " the cost to the
patients, in terms of days taken off work, showed thatthose in the surgical group lost 31-3 days compared with6,4 days lost by those treated with injection/compressionsclerotherapy "; " The average loss of earnings in thetwo groups was £118 and E29 respectively." " It isconcluded that it would benefit the patient, the healthservice, and the community if the majority of patientswith varicose veins were treated as outpatients by injec-tion/compression sclerotherapy."
1. Chant, A. D. B., Jones, H. O., Weddell, J. M. Lancet, 1972, ii, 1188.2. Piachaud, D., Weddell, J. M. ibid. p. 1191.