Association of Dyslipidemia and Ischemic Stroke in Pakistan Institute of Medical Sciences (1)

of 3
-
Upload
venniariskia -
Category
Documents
-
view
219 -
download
0
Transcript of Association of Dyslipidemia and Ischemic Stroke in Pakistan Institute of Medical Sciences (1)
-
8/9/2019 Association of Dyslipidemia and Ischemic Stroke in Pakistan Institute of Medical Sciences (1)
1/3
Association of Dyslipidemia and Ischemic Stroke Urooj Taheed Baluch et al
Ann. Pak. Inst. Med. Sci. 2008;4(3): 165-167 165
Original Article
Association of Dyslipidemia and
Ischemic Stroke
Background: Stroke is leading cause of death world wide. Dyslipidemia is one of theimportant risk factor in patients with coronary heart disease.
Objective: To see the association of dyslipidemia in patients who have presented withischemic st roke in Pakistan Institute of Medical Sciences
Subjects and Methods: This retrospective study was conducted at neurologydepartment of Pakistan institute of medical sciences from January 1st 2008 to March 1st2008. A total of 53 patients having ischemic stroke which was confirmed on CT scan wereincluded and there lipid profiles were studied.
Results: In a total of 53 patients, 32 were male and 21 female. 28% of patient were in agegroup of 61-70 years.19% patient had dyslipidemia; of them, 18% had low HDL, while highLDL, cholesterol and triglycerides were observed in 26%, 24% and 32% patients,respectively. 42% of patients were hypertensive and 35% were diabetics. This data wassimilar to that of the western and Asian studies
Conclusion: Like HTN and diabetes, dyslipedemia is another important and modifiablerisk factor controlling which might reduce the incidence of ischemic stroke reducing thefinancial and emotional burden of the nation.
Key Words: Ischemic Stroke, Dyslipedemia, HDL, LDL, Cholesterol, Triglycerides
Urooj Taheed Baluch*
Ismaa Kiani*
Zaib-un-nisa*
Mazhar Badshah**
* Post graduate resident** Assistant professor department ofneurologyDepartment of Medicine andDepartment of NeurologyPakistan Institute of Medical SciencesIslamabad
Address for Correspondence:
Dr Urooj Taheed BaluchDepartment of MedicinePakistan Institute of Medical Sciences,Islamabad.Email: [email protected]
Introduction
Stroke, after heart diseases and cancer is thethird leading cause of death world wide.1Stroke is also
a leading cause of functional impairments, with 20% ofsurvivors requiring institutional care after 3 months and15-30% gets permanently disabled.
2Of all strokes, 88%
are classified as ischemic, and the remainders arehemorrhagic, either subarachnoid (9%) or intracerebral(3%).
3Ischemic stroke is mostly due to
thromboembolism secondary to atherosclerosis in themajor arteries. Other causes include infarction due toembolism from heart and intrinsic disease of the smallperforating vessels. Nikolai first proposed a link betweencholesterol and atherosclerosis in 1912.
4Kunitomo M. et
al worked on mice in Japan and found thatatherosclerotic lesions are formed in the aorta of micefed a high-cholesterol and high-linoleic diet, in parallelwith elevated serum lipid peroxide levels.
5Abnormalities
of serum lipids are major risk factors for coronary heartdisease and most recently established as risk factor incerebrovascular disease.
6Studies have shown that
lowering cholesterol may decrease carotid atheromathus resulting in a decline in carotid territory infarcts.
6
Two prospective studies in mensubsequently
showed increases in ischemic stroke rates at higher
levels of total cholesterol.7,8
The Asia Pacific CohortStudies Collaboration
found a 25% increase in
ischemic
stroke rates for every 1 mmol/L increase
in totalcholesterol.
9The US Womens Pooling Project
(24,343
women at risk) found a 25% increased risk of fatalischemic
stroke for each 1 mmol/L increase in total
cholesterol in women30 to 54 years of age.
10Only a few
studies have analyzed the relationship between LDL
cholesterol (the major component of total cholesterol)and ischemic
stroke.
No consistent association has been found,although the
total number of subjects at risk in these
studies are limited.11
An inverse relationship betweenHDL and stroke risk was demonstrated in both theOxford Shire Community Study and the Northern
Manhattan Stroke Study.
12
In a study
of subjects with CAD, ischemiccerebrovascular events
were significantly associated
with high triglyceride and lowHDL cholesterol levels.
13
Thus, there does appear to bea clear relationship
between dyslipidemia and the risk of ischemicstroke in
both men and women.14
This study was carried out to see the
association of dyslipidemia in patients who havepresented with ischemic stroke in our setup.
-
8/9/2019 Association of Dyslipidemia and Ischemic Stroke in Pakistan Institute of Medical Sciences (1)
2/3
Association of Dyslipidemia and Ischemic Stroke Urooj Taheed Baluch et al
Ann. Pak. Inst. Med. Sci. 2008;4(3): 165-167 166
Materials and Methods
Inclusion Criteria: All patients between 30 to 90 yearswho were admitted in department of Neurology of PIMSwith first ever stroke verified by CT scan brain during the2 months period from Jan 1st 2008 to Feb 29th 2008were included in the studyExclusion Criteria: We excluded the patients who hada recent myocardial infarction with left ventricular failure,history of previous stroke, syncopal attack, presumptivediagnosis of ischemic stroke with no evidence on the CTscan, neurological deficit secondary to epilepsy,infective or metastatic disorder, or pre-existing severephysical and cognitive disorder.
A detailed history was recorded and physicalexamination was undertaken. Blood samples of all thepatients were taken on the next morning or the secondday of stroke, as recommended
15and were sent for lipid
profile at laboratory of PIMS.ATP III classification was followed for
dyslipidemia:Low HDL < 40 mg/dlHigh LDL > 190 mg/dlHigh Cholesterol >200 mg/dlHigh Triglycerides >200 mg/dl
Results
A total of 60 patients were admitted during theperiod of study; seven of them were excluded, as 2 hadmyocardial infarction with left ventricular failure, 1patient had SLE, 1 patient was a case of brainmetastasis, 2 patients had infective endocarditis and 1patient had an episode of stroke a year back. Amongst atotal of 53 patients selected, 21(40%) were females and32(60 %) males (Table1).
Table 1: Demographic data of patientsTotal no of patientsNo of patients excludedNo of patients includedNo of female patientsNo of male patientsNo of patients with hypertensionNo of patients with diabetesNo of patients with dyslipidemia
60753213222199
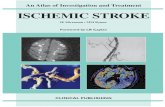
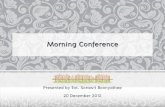
The no of patients increased as the age groupincreased and it was 28% in the age group of 61-70years (Figure 1). The classical risk factors likehypertension, diabetes along with dyslipedemia werestudied. Data (Figure 2) showed that 42% werehypertensive, 35% were diabetic, 19% weredyslipidemic, and in 34% of patients all the risk factors
were present. Only 5 % of the patients had none of therisk factors.
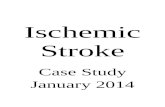
When all the dyslipedemia were consideredindividually it was seen that 18% of patients had lowHDL levels, 26%, 24% and 32% patient had high LDL,triglycerides, and cholesterol levels respectively (Figure3).
Figure 1: Age distribution of patientssuffering from stroke
Figure 2: Percentages of All Three RiskFactors in Patients of Stroke
Figure 3: Percentages of Different Types ofDyslipidemias in Patients with Stroke
Discussion
Stroke continues to have a great impact onpublic health. Stroke is frequent, recurring, and is moreoften disabling than fatal. Although some determinants
-
8/9/2019 Association of Dyslipidemia and Ischemic Stroke in Pakistan Institute of Medical Sciences (1)
3/3
Association of Dyslipidemia and Ischemic Stroke Urooj Taheed Baluch et al
Ann. Pak. Inst. Med. Sci. 2008;4(3): 165-167 167
of stroke, such as age, gender, race, ethnicity andheredity cannot be modified, they are risk markers.However more important are the modifiable factorscontrolling them can and will reduce the incidence of thedisease
16. Hypercholesterolemia and various
lipoproteins fractions have been associated with theseverity of carotid atherosclerosis. Associations of
stroke and dyslipidemia have become quantified inrecent studies.
Figure 4 compares our results with previousstudies. In our study dyslipidemia including highcholesterol, triglycerides and LDL along with low HDLwas 19%.while a Study done in Denmark it was 26%
17,
205 in a Yugoslavia study17
, and in Iran study.17
Theresult of other risk factors were also similar to thewestern and Asian studies. Hypertension was present in42% of our patients similar to 30%, 47.9% and 54% inDenmark
17, Yugoslavia
17 and Iran
17.However
association of diabetes was found to be higher 35% ascompare to 10-30% seen in western countries
18. Like in
a Yugoslavian study
17
it was 5.5%. While is similarwhen compared to Asian studies, 45 % in an Iranianstudy.
17
Figure 4: Comparison of Al l the Three RiskFactor between Our Study and Study from
Different Countries
Conclusion
Our study although had a small no of samplesize and was over a short period of 60 days has resultssimilar to that of the western studies revealing
association of 15.4% to 30% of dyslipedemia to theischemic stroke. It also shows that not only high levelsof LDL,TG and cholesterol but low levels of goodcholesterol, HDL, is also associated with atherosclerosisand in turn stroke. There is need of educating peopleregarding there dietary habits and life style to reduce theincidence of this disabling disease as prevention isbetter than cure.
References
1. Arboix A, Roig H, Rossich R, Martnez EM, Garca-Eroles L.Differences between hypertensive and non-hypertensive ischemicstroke Euro J of Neurol 2004;11: 687
2. American Heart Association. Heart Disease and Statistics Stroke.2004
3. American Heart Association. Heart disease and stroke statistics
2006 update: A report from the American Heart Association StatisticsCommittee and Stroke Statistics Committee. Circulation 2006 e85-e151.
4. Gotto AM. Some reflections on arteriosclerosis: past, present, andfuture. Circulation 1985; 72:8-17
5. Kunitomo M Oxidative stress and atherosclerosis. Yakugaku Zasshi.2007;127:1997-2014
6. Goldstein LB, Adams R, Becker K, Furberg CD, Gorelick PB,Hademenos G et al. Primary Prevention of Ischemic Stroke: AStatement for Healthcare Professionals from the Stroke Council of
the American Heart Association.Circulation.2001; 103:1637. Iso H, Jacobs DR , Wentworth D, et al. Serum cholesterol levels and
six-year mortality from stroke in 350,977 men screened for theMultiple Risk Factor Intervention Trial. N Engl J Med. 1989; 320:90410
8. Kagan A, Popper JS, Rhoads GG. Factors related to stroke incidence
in Hawaii Japanese men. The Honolulu Heart Study. Stroke 1980; 11:1421
9. Zhang X, Patel A, Horibe H, Wu Z, Barzi F, Rodgers A, et al; AsiaPacific Cohort Studies Collaboration. Cholesterol, coronary heartdisease, and stroke in the Asia Pacific region. Int J Epidemio. 2003;32: 56372
10. Horenstein RB, Smith DE, Mosca L. Cholesterol predicts strokemortality in the Womens Pooling Project. Stroke. 2002; 33: 18638
11. Shahar E, Chambless LE, Rosamond WD, Boland LL, BallantyneCM, McGovern PG, et al; Atherosclerosis Risk in Communities Study.Plasma lipid profile and incident ischemic stroke: the AtherosclerosisRisk in Communities (ARIC) Study. Stroke. 2003; 34: 623631
12. Kargman DE, Tuck C, Berglund LF, et al. Elevated high densitylipoprotein levels are more important in atherosclerotic ischemicstroke subtypes: the Northern Manhattan Stroke Study. Ann Neurol.1998;44:442443
13. Koren-Morag N, Tanne D, Graff E, Goldbourt U. Low- and high-density lipoprotein cholesterol and ischemic cerebrovascular disease:the bezafibrate infarction prevention registry. Arch Intern Med. 2002;162: 9939
14. Goldstein LB, Adams R, Alberts M, Appel LJ, Brass LM,Bushnell CDet all Primary Prevention of Ischemic Stroke:A Guideline From the
American Heart Association/American Stroke Association StrokeCouncil: Cosponsored by the Atherosclerotic Peripheral VascularDisease Interdisciplinary Working Group; Cardiovascular NursingCouncil; Clinical Cardiology Council; Nutrition, Physical Activity, andMetabolism Council; and the Quality of Care and OutcomesResearch Interdisciplinary Working Group: The American Academy ofNeurology affirms the value of this guideline. Stroke. 2006; 37:1583.
15. Aull S, Lalouschek W, Schnider P, Sinzinger H, Uhl F, Zeiler K.Dynamic changes of plasma lipids and lipoproteins in patientsafter transient ischemic attack or minor stroke. Am J Med. 1996;101:291-8
16. Sacco RL, Benjamin EJ, Broderick JP, et al. American HeartAssociation Prevention Conference IV: prevention and rehabilitationof stroke: risk factors. Stroke.
17. Masoud SA ; asurvey on the prevalence of stroke risk factors in cvadiagnosed patients,hospitalized in shahid beheshti hospital in1998,Iranian j.public health,2002 21-2
18. Sandercock PAG, Warlow CP, Starky IR. Predisposing factors forcerebral infarction: the Oxfordshire community stroke project. BMJ1989;298:75-81.