Ischemic Stroke Update Handouts
21
9/23/2013 1 Updates in Stroke Thomas G. Mattio PhD, MD Neuroscience Group of NE WI Epidemiology " Stroke is the third leading cause of death in the United States. More than 140,000 people die each year from stroke in the United States. " Stroke is the leading cause of serious, long- term disability in the United States. " Each year, approximately 795,000 people suffer a stroke. About 600,000 of these are first attacks, and 185,000 are recurrent attacks. Epidemiology " Leading cause of adult disability " Every 40 seconds someone has a stroke " Someone dies every 3.3 minutes from a stroke " Twice as many women die from stroke every year than from breast cancer " 4,000,000 stroke survivors Poll Question: " What percentage of all strokes are ischemic? A. 34% B. 50% C. 85% D. 95% Types of Strokes " Ischemic (85%) Thrombotic (54%) Embolic (31%) " Hemorrhagic (15%) Intracerebral = 10% Subarachnoid = 5% Ischemic Stroke: Thrombotic
-
Upload
adi-paramartha -
Category
Documents
-
view
36 -
download
4
description
klkk
Transcript of Ischemic Stroke Update Handouts
9/23/2013
1
Updates in Stroke
Thomas G. Mattio PhD, MDNeuroscience Group of NE WI
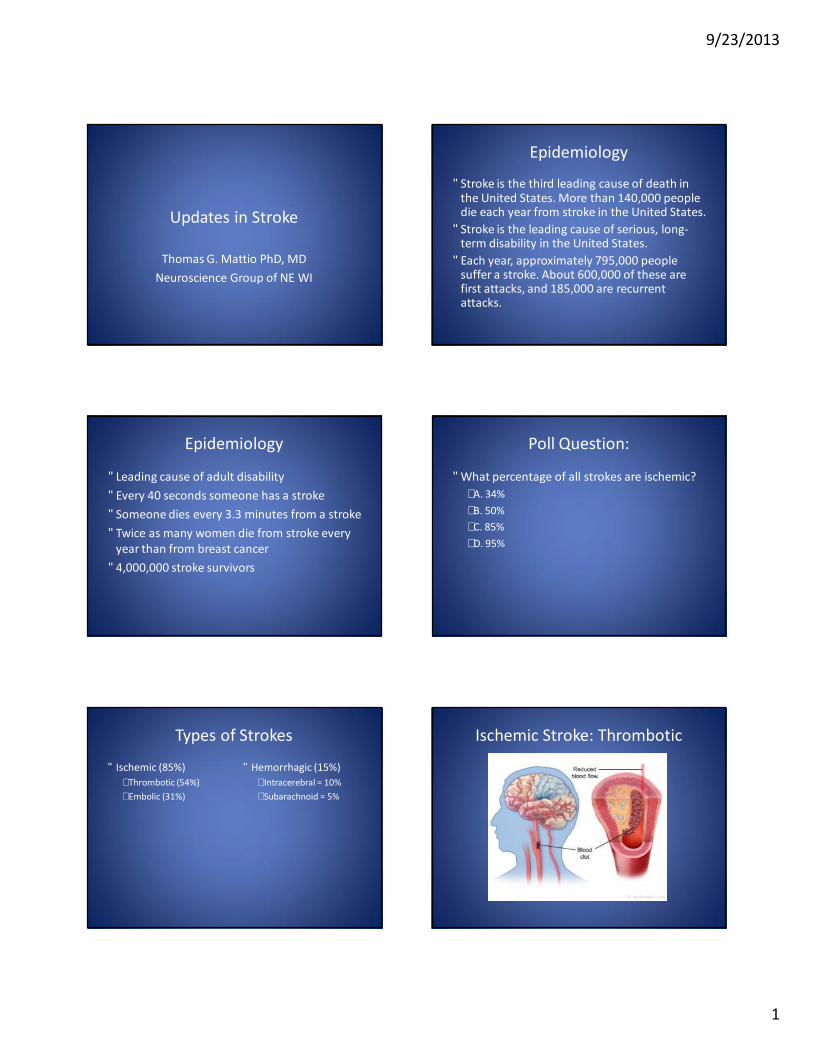
Epidemiology
• Stroke is the third leading cause of death in the United States. More than 140,000 people die each year from stroke in the United States.
• Stroke is the leading cause of serious, long-term disability in the United States.
• Each year, approximately 795,000 people suffer a stroke. About 600,000 of these are first attacks, and 185,000 are recurrent attacks.
Epidemiology
• Leading cause of adult disability• Every 40 seconds someone has a stroke• Someone dies every 3.3 minutes from a stroke• Twice as many women die from stroke every
year than from breast cancer• 4,000,000 stroke survivors
Poll Question:
• What percentage of all strokes are ischemic?– A. 34%– B. 50%– C. 85%– D. 95%
Types of Strokes
• Ischemic (85%)– Thrombotic (54%)– Embolic (31%)
• Hemorrhagic (15%)– Intracerebral = 10%– Subarachnoid = 5%
Ischemic Stroke: Thrombotic
9/23/2013
2
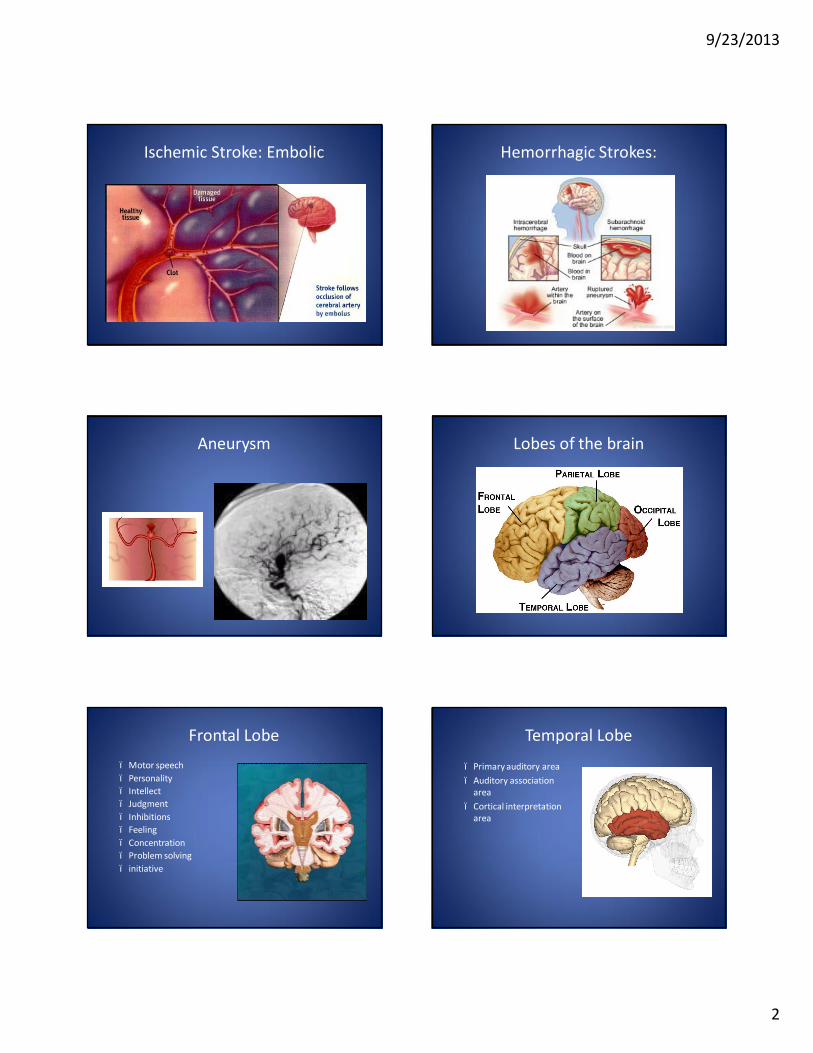
Ischemic Stroke: Embolic Hemorrhagic Strokes:
Aneurysm Lobes of the brain
Frontal Lobe– Motor speech– Personality– Intellect– Judgment– Inhibitions– Feeling – Concentration– Problem solving– initiative
Temporal Lobe
– Primary auditory area– Auditory association
area– Cortical interpretation
area
9/23/2013
3
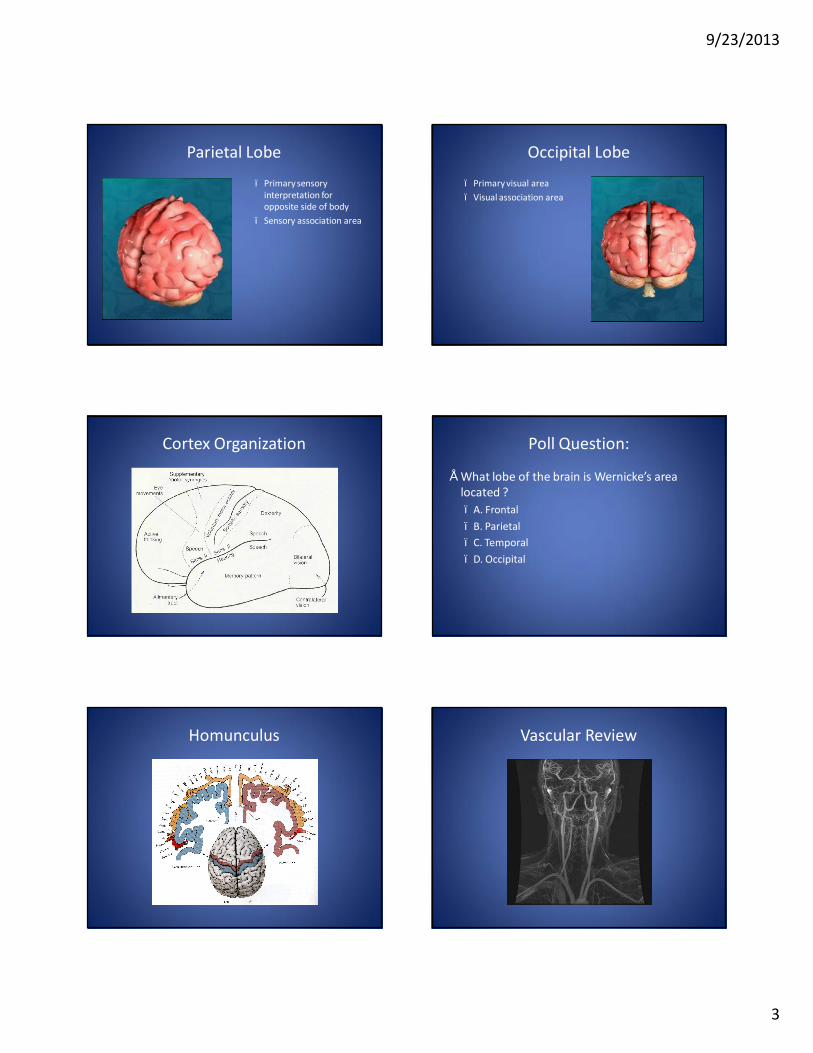
Parietal Lobe
– Primary sensory interpretation for opposite side of body
– Sensory association area
Occipital Lobe
– Primary visual area– Visual association area
Cortex Organization Poll Question:
• What lobe of the brain is Wernicke’s area located ?– A. Frontal– B. Parietal– C. Temporal– D. Occipital
Homunculus Vascular Review
9/23/2013
4
Cerebrovascular Territories
Anterior Circulation Syndromes
• Contralateral hemiparesis or hemiplegia of the foot and leg (Foot drop is a common finding), sensory loss in the toes, foot, and leg
• Mental status impairment including confusion, amnesia, perseveration, and personality changes such as apathy or flat effect
• Abulia (i.e., inability to make decisions or perform voluntary acts).
Anterior Cerebral Artery Stroke:Case Review
• HPI:– 65 y/o man acute onset left leg weakness. Went to leave home at 9am
for a short walk. Had immediate left leg weakness and was unable to walk. Wife called 911, patient arrived at TC around 10am
• PMH:– MI two weeks prior– Hypertension, coronary artery disease– Medications: ASA and Plavix– Family hx: coronary artery disease, mother had one stroke but
recovered well• Social hx:
– Married, had 2 grown children– Former 2ppd smoker, quit 2 years ago
9/23/2013
5
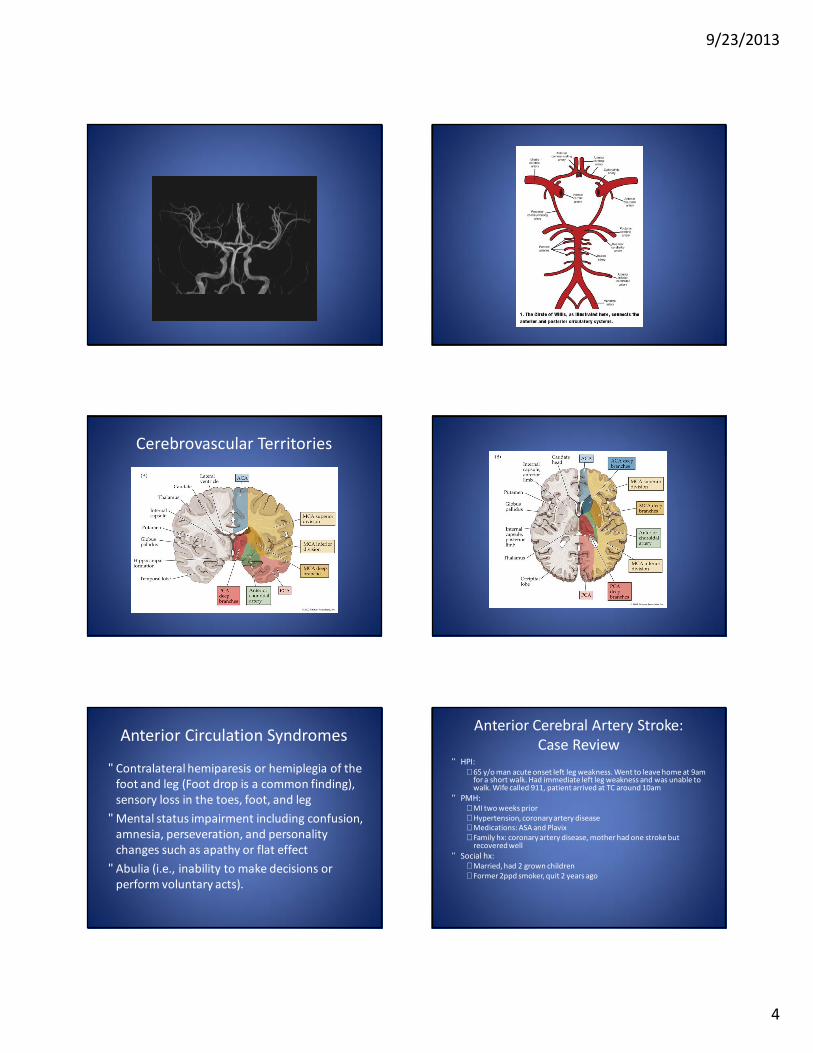
• Physical Exam:– left leg weakness with hyperreflexia– Exam otherwise negative
• Diagnostic Studies:– MRI: clear cut right anterior cerebral artery stroke– Echocardiogram showed thrombus overlying hypokinetic
left ventricle• Hospital Course:
– Worked with therapies– By day 2 had significant left leg improvement– Discharged home with outpatient therapies, walking with
walker, was anticoagulated and recovered well
Anterior Cerebral Artery Stroke:Case Review
Middle Cerebral Artery Syndromes• Contralateral hemiparesis or hemiplegia of the face
and arm (The leg is spared or has fewer deficits than the arm.)
• Contralateral hemisensory in the same area• Contralateral vision loss (hemianopia; left hemisphere
has right visual field cuts and right hemisphere has left visual field cuts)
• In LEFT hemisphere, aphasia and difficulty reading, writing, and calculating are more likely
• In RIGHT hemisphere, neglect of left visual spaces, extinction of left-sided stimuli, and spatial disorientation are more likely
Middle Cerebral Artery Syndromes
• Gerstman syndrome:– Agraphia (inability to write)– Acalculia (inability to calculate)– Right-left confusion– Finger agnosia (inability to recognize fingers)
Right MCA Stroke:Case Review
• HPI:– 48 y/o male from outlying hospital presenting with left sided
hemiplegia. Had this same weakness one week earlier and went to a different outlying hospital who diagnosed him with a UTI and started him on Cipro. They made him a follow up with his primary care physican, and appointments for an outpatient MRI and carotid ultrasound.
– Received t-PA 2 hours and 8 minutes after onset of symptoms at outlying hospital, patient transferred to TC
• PMH:– Gastric bypass– Daily drinker
• Social hx: – Married
Right MCA Stroke:Case Review
• Physical Exam on arrival to TC:– Forced deviation of eyes to right– Left sided hemiplegia– Severe left side neglect with extinction– Speech intact but dysarthric– Left facial paralysis– NIHSS: 17
• Diagnositic Studies:– Code stroke CT: showed fixed deficit with an abrupt
cut off of R MCA and subarachnoid blood
9/23/2013
6
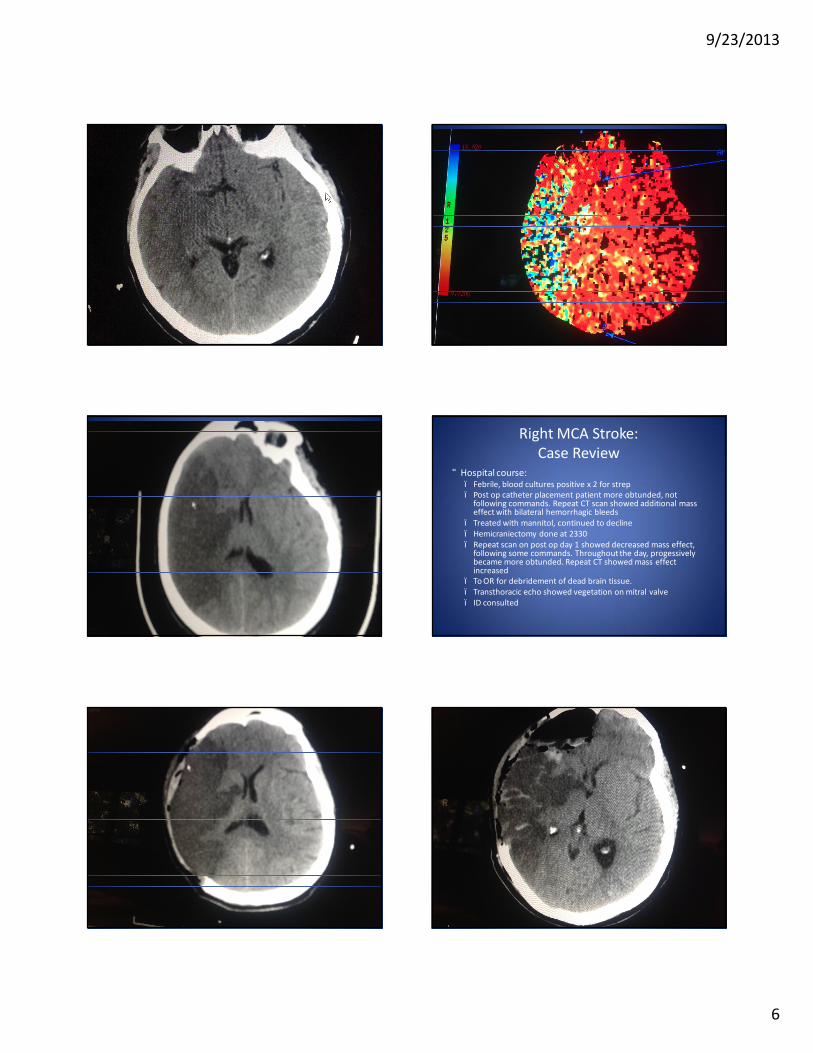
Right MCA Stroke:Case Review
• Hospital course:– Febrile, blood cultures positive x 2 for strep– Post op catheter placement patient more obtunded, not
following commands. Repeat CT scan showed additional mass effect with bilateral hemorrhagic bleeds
– Treated with mannitol, continued to decline– Hemicraniectomy done at 2330– Repeat scan on post op day 1 showed decreased mass effect,
following some commands. Throughout the day, progessivelybecame more obtunded. Repeat CT showed mass effect increased
– To OR for debridement of dead brain tissue.– Transthoracic echo showed vegetation on mitral valve– ID consulted
9/23/2013
7
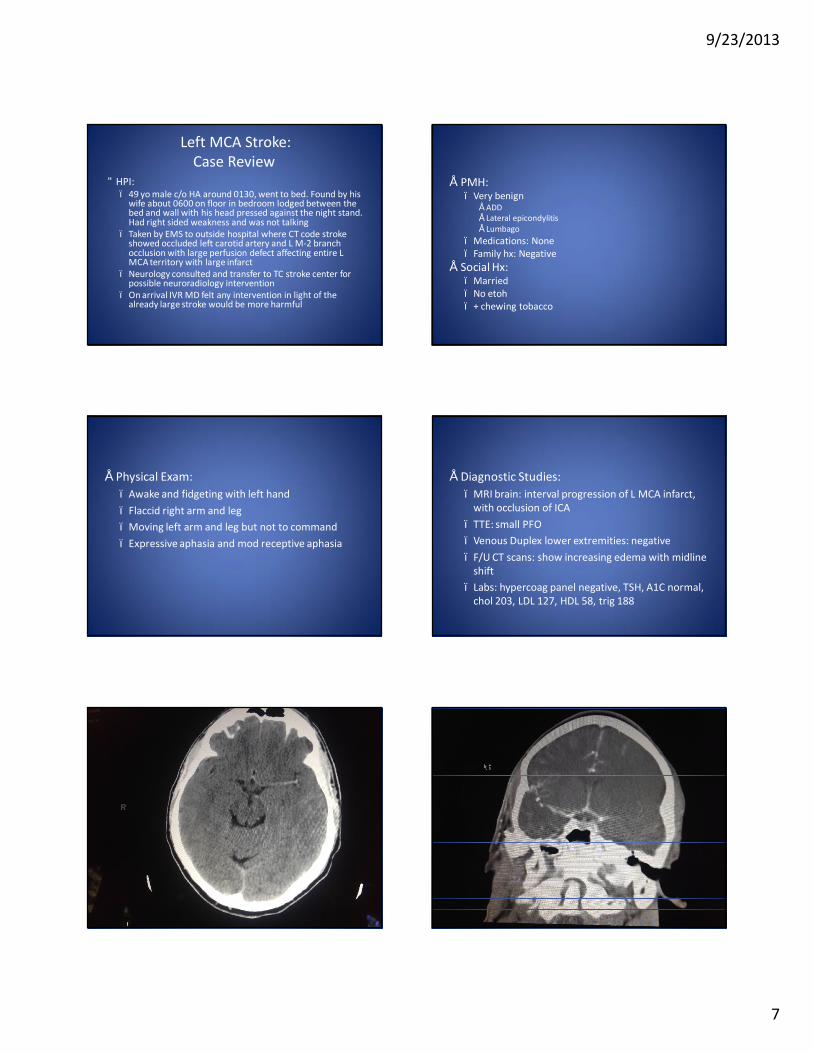
Left MCA Stroke:Case Review
• HPI:– 49 yo male c/o HA around 0130, went to bed. Found by his
wife about 0600 on floor in bedroom lodged between the bed and wall with his head pressed against the night stand. Had right sided weakness and was not talking
– Taken by EMS to outside hospital where CT code stroke showed occluded left carotid artery and L M-2 branch occlusion with large perfusion defect affecting entire L MCA territory with large infarct
– Neurology consulted and transfer to TC stroke center for possible neuroradiology intervention
– On arrival IVR MD felt any intervention in light of the already large stroke would be more harmful
• PMH:– Very benign
• ADD• Lateral epicondylitis• Lumbago
– Medications: None– Family hx: Negative
• Social Hx:– Married– No etoh– + chewing tobacco
• Physical Exam:– Awake and fidgeting with left hand– Flaccid right arm and leg– Moving left arm and leg but not to command– Expressive aphasia and mod receptive aphasia
• Diagnostic Studies:– MRI brain: interval progression of L MCA infarct,
with occlusion of ICA– TTE: small PFO– Venous Duplex lower extremities: negative– F/U CT scans: show increasing edema with midline
shift – Labs: hypercoag panel negative, TSH, A1C normal,
chol 203, LDL 127, HDL 58, trig 188
9/23/2013
8
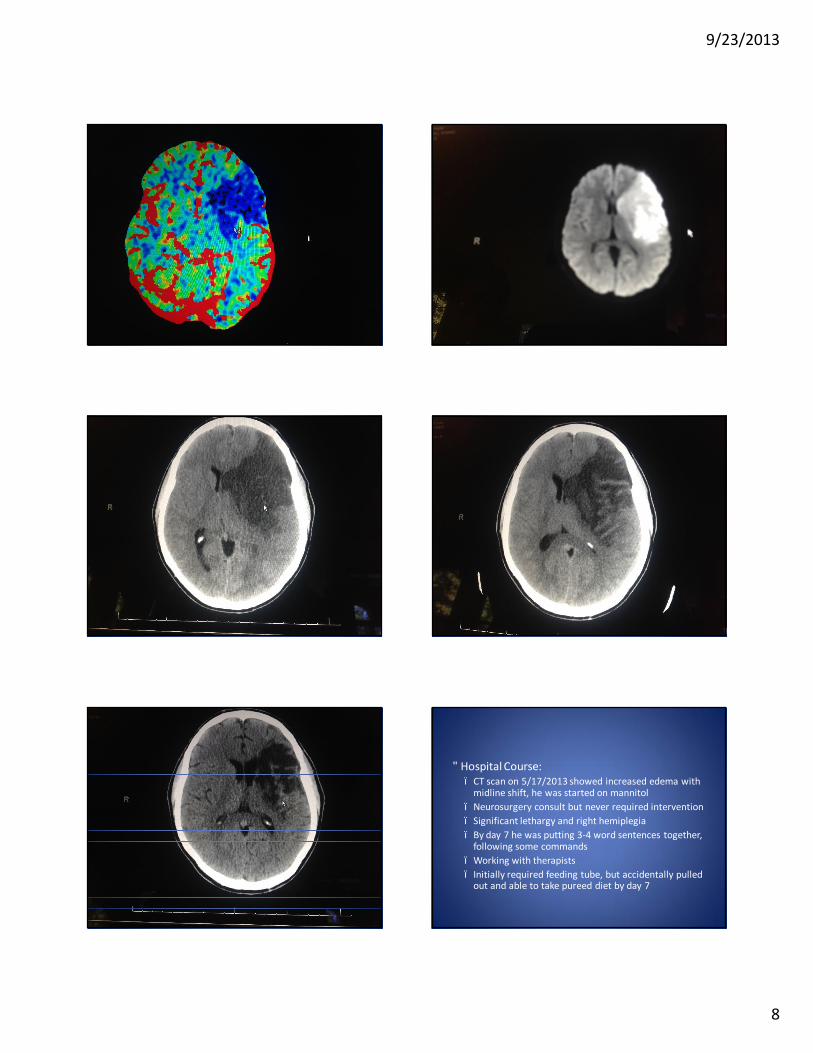
• Hospital Course:– CT scan on 5/17/2013 showed increased edema with
midline shift, he was started on mannitol – Neurosurgery consult but never required intervention– Significant lethargy and right hemiplegia– By day 7 he was putting 3-4 word sentences together,
following some commands– Working with therapists– Initially required feeding tube, but accidentally pulled
out and able to take pureed diet by day 7
9/23/2013
9
• Hospital Course continued:– Acute inpatient hospital 5/15 – 5/30– Acute Inpatient Rehab 5/30 – 6/27– Discharged home with in home PT, OT, ST– Admitted to Peabody 7/19 due to not meeting home
care goals– Discharged from Peabody to VA rehab center in
Madison on 9/10/2013• Still with significant deficits. Has severe expressive aphasia,
flaccid right upper extremity, minimal hip flexion, and knee flexion/extension of right lower extremity
Internal Carotid Artery Syndromes
• Contralateral paralysis of the face, arm, and leg• Contralateral sensory deficits of the face, arm,
and leg• Aphasia, if the dominant hemisphere is involved• Hemianopia, ipsilateral episodes of visual
blurring, or amaurosis fugax (temporary blindness in one eye)
• Carotid bruit
Lacunar Stroke
• Occlusion of a single deep penetrating artery
• Infarct is less than 15mm
• Deep subcortical white matter
• Affects thalmus, internal capsule, basal ganglia, centrumsemiovale, brainstem
Lacunar Syndromes
• Pure motor stroke / hemiparesis (33-50%)• Pure sensory stroke• Ataxic hemiparesis• Dysarthria / clumsy hand (pons)
Lacunar Stroke:Case Review
• HPI: – 71 y/o man presented to ER with fluctuating left sided weakness for 24
hours then developed fixed left sided weakness (for greater than 8 hours). Prior to weakness lived alone with no children nearby, and called friend to bring him to ER.
• PMH:– Hyperlipidemia, HTN– Diabetes– Did not see primary care physician, no f/u done for diabetes or HTN– Medications: stopped taking over 3 years ago– Family hx: father died of MI
• Social hx:– Widowed, 2 adult children living out of state– +chewing
• Physical Exam:– Right facial paralysis– Left arm = Left leg weakness with right sided ataxia
• Diagnostic Studies:– TTE normal– MRI: small R lacunar stroke
• Hospital Course:– Work up shows no large vessel stensosis.– Went to rehab– Ambulating with walker at 3 weeks– Discharge to home with outpatient therapies.– Follow-up at 3 months: ambulating with cane mainly for balance
9/23/2013
10
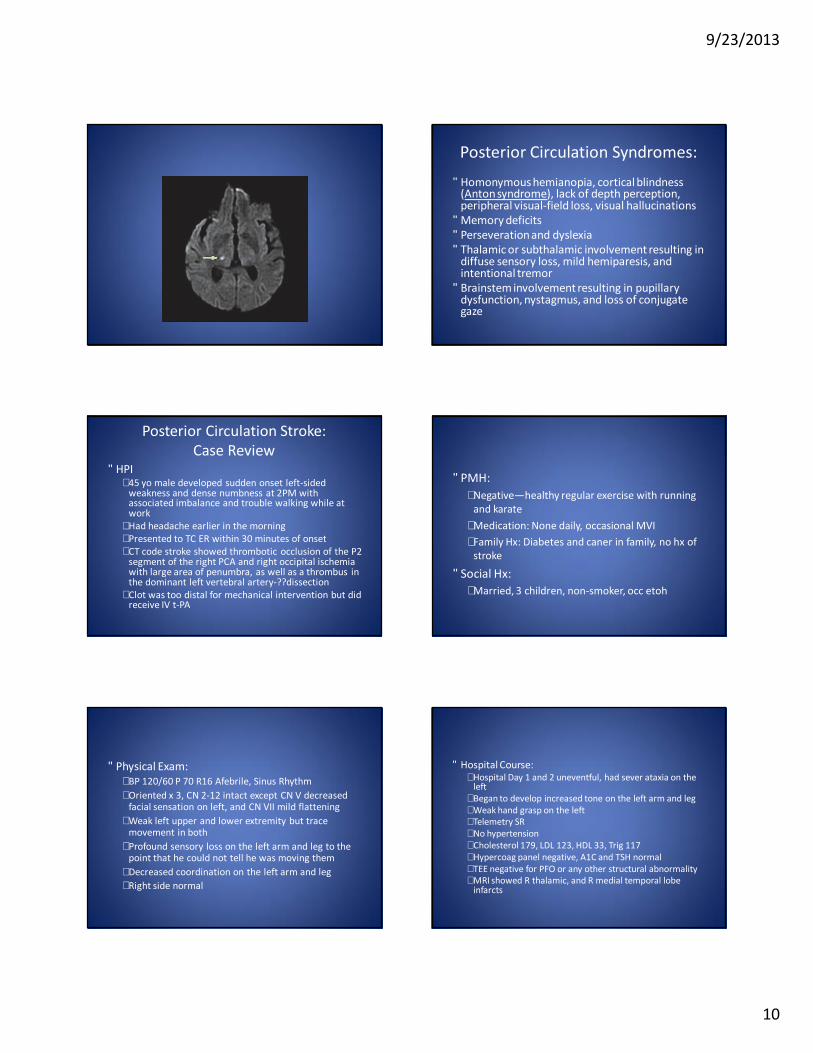
Posterior Circulation Syndromes:
• Homonymous hemianopia, cortical blindness (Anton syndrome), lack of depth perception, peripheral visual-field loss, visual hallucinations
• Memory deficits• Perseveration and dyslexia• Thalamic or subthalamic involvement resulting in
diffuse sensory loss, mild hemiparesis, and intentional tremor
• Brainstem involvement resulting in pupillarydysfunction, nystagmus, and loss of conjugate gaze
Posterior Circulation Stroke:Case Review
• HPI– 45 yo male developed sudden onset left-sided
weakness and dense numbness at 2PM with associated imbalance and trouble walking while at work
– Had headache earlier in the morning– Presented to TC ER within 30 minutes of onset– CT code stroke showed thrombotic occlusion of the P2
segment of the right PCA and right occipital ischemia with large area of penumbra, as well as a thrombus in the dominant left vertebral artery-??dissection
– Clot was too distal for mechanical intervention but did receive IV t-PA
• PMH:– Negative—healthy regular exercise with running
and karate– Medication: None daily, occasional MVI– Family Hx: Diabetes and caner in family, no hx of
stroke
• Social Hx:– Married, 3 children, non-smoker, occ etoh
• Physical Exam:– BP 120/60 P 70 R16 Afebrile, Sinus Rhythm– Oriented x 3, CN 2-12 intact except CN V decreased
facial sensation on left, and CN VII mild flattening– Weak left upper and lower extremity but trace
movement in both– Profound sensory loss on the left arm and leg to the
point that he could not tell he was moving them– Decreased coordination on the left arm and leg– Right side normal
• Hospital Course:– Hospital Day 1 and 2 uneventful, had sever ataxia on the
left – Began to develop increased tone on the left arm and leg– Weak hand grasp on the left– Telemetry SR– No hypertension– Cholesterol 179, LDL 123, HDL 33, Trig 117– Hypercoag panel negative, A1C and TSH normal– TEE negative for PFO or any other structural abnormality– MRI showed R thalamic, and R medial temporal lobe
infarcts

9/23/2013
11
• Hospital Course continued:– Hospital day 4 received call from nursing staff of
increased dizziness, trouble talking and dysarthria– Stat head CT negative for hemorrhage– Became more drowsy, only moaning, right gaze
preference– MRI brain: new infarcts occipital/parietal lobe on
L, R occipital lobe, and possible infarct temporal lobe and L pons, possible thrombus in the basilar tip, stenosis or occlusion L vertebral artery
• Hospital Course continued:– Went for stat cerebral angiogram
• L vertebral artery origin dissection with thrombus formation• Successful thrombectomy• Successful angioplasty L vertebral artery
– Day 1 post angiogram had weak left hand grasp, able to wiggle toes on left but not lift leg or left arm off bed, weakness of right and left leg as well, continued with sensory loss
– Required neosynephrine to keep SBP 110 – 140– By day 11 of hospitalization was able to go to
inpatient rehab on aspirin, plavix and lipitor
• Hospital Course continued:– On day 7 of his inpatient rehab stay he developed sudden
hypotension with SBP 61/41, with associated dizziness, diaphoresis, and nausea
– Transferred to ICU, required vasopressors for BP– MRI no new stroke, CT angio negative for PE, no signs of
infection, – Started on florinef, midodrine, salt tablets, pyridostigmine,
and compression stockings.– Bp’s remained low, but was able to wean off IV pressors
without clinical symptoms of orthostasis– Spent an additional 15 days in acute care before being
transferred back to rehab

9/23/2013
12
• Hospital Course continued:– Continued inpatient rehab for another 3 weeks– At discharge from inpatient rehab was
• Independent to supervision with bathing, independent with dressing• Independent with bed mobility, transfers, and ambulation with a
wheeled walker • Had mild memory deficits and trouble with higher functioning
– 1 months post discharge was• Mildly spastic dysarthria, ataxia with f-f-n bilaterally, still walking with
walker• Began to wean florinef
– 4 months post discharge:• Able to ride 3 wheeled bike, able to go up and down steps, spastic
hemiparetic gait on left, no further walker or cane significant sensory loss on the left, still some cognitive issues with numbers and memory
Vertebro-basilar Artery Syndromes
• Hemiplegia/hemiparesis or quadriplegia/quadriparesis
• Ipsilateral numbness and weakness of face• Dysarthriaand dysphagia• Vertigo, nausea, and dizziness• Ataxic gait and clumsiness• Dipolopia, homonymous hemianopia, nystagmus,
conjugate gaze paralysis, and opthalmoplegia• Locked-in syndrome
Basilar Artery Stroke:Case Review
• HPI:– 44 yo female transferred to outside hospital for thrombectomy of
basilar artery clot– Hx of unintentional 25 lb weight loss over 3 months– 2 weeks prior to admission c/o palpitations, prescribed beta blocker– Presented to outside hospital with SOB and found to have 2 large PE’s
bilaterally, she was intubated, sedated with propofol and placed on a heparin drip.
– Also found to be anemic and transfused – 4 days after admission to outside hospital propofol was weaned at
3PM and she was found to have left eye ptosis, and inability to move any of her extremities.
– At 7pm MRI showed midbrain and upper pons ischemia and MR showed basilar artery occlusion
– Transferred to TC stroke center and went directly to specials for clot retrieval
• PMH:– Migraines– No history of bleeding disorder or other clots– No history of heavy menstruation– Avoided seeing MD’s– Medication: Excedrin twice weekly for headaches,
no prescription drugs– Family hx: negative of blood clots or miscarriages,
only + for cardiac problems
• Social Hx:– Married– No children – Non smoker– 6 alcoholic beverages per week– No history of illicit drug use
• Physical Exam:– BP 133/63, P 70– Intubated, blinking and only moving left toes to command– Pupils = and reactive– Conjugate gaze in all directions– No nystagmus– Ptosis OS– Appeared nearly locked in– Labs
• Hgb 8.9• CMP normal
9/23/2013
13
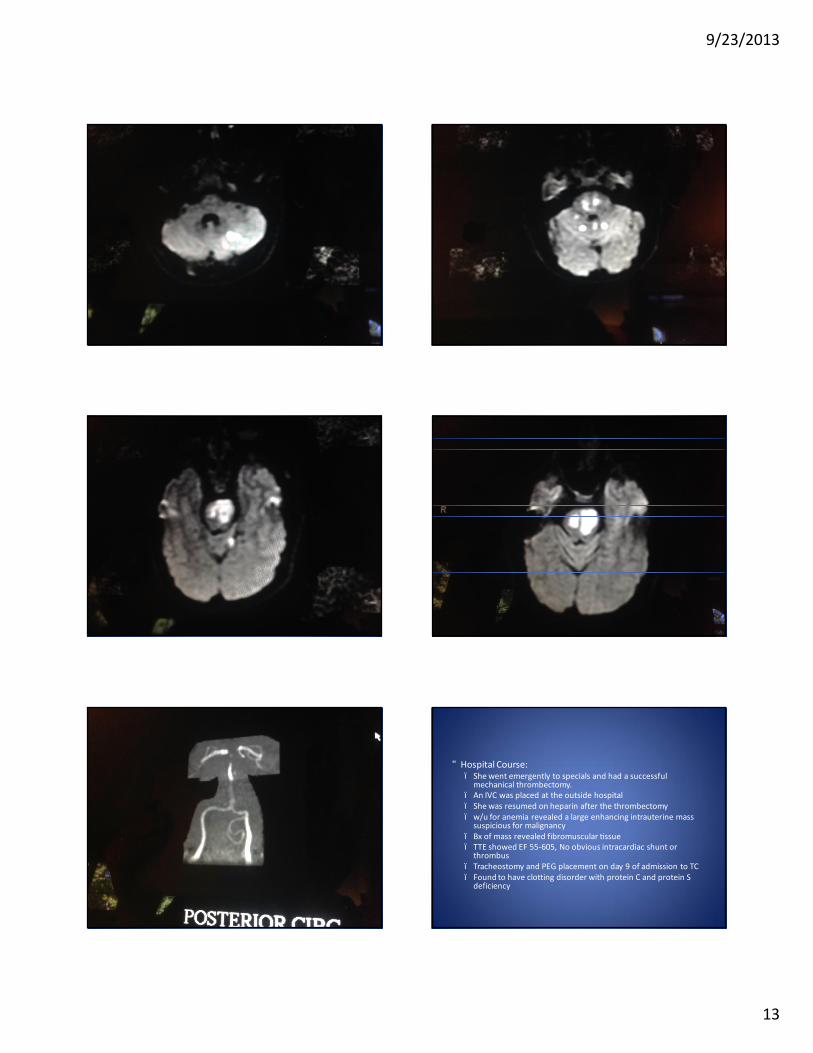
• Hospital Course:– She went emergently to specials and had a successful
mechanical thrombectomy.– An IVC was placed at the outside hospital– She was resumed on heparin after the thrombectomy– w/u for anemia revealed a large enhancing intrauterine mass
suspicious for malignancy– Bx of mass revealed fibromuscular tissue– TTE showed EF 55-605, No obvious intracardiac shunt or
thrombus– Tracheostomy and PEG placement on day 9 of admission to TC– Found to have clotting disorder with protein C and protein S
deficiency

9/23/2013
14
• Hospital Course continued:– Approx day 12 of hospital stay, palliative care consult
placed as she remained locked in. Husband wanted to continue with aggressive management
– Approx 2 weeks post admission, she was awake, had left sided ptosis, but could open right eye and track. Unable to mouth words or phonate. Attempting to communicate with upward and downward eye movements with significant inconsistency. Limited voluntary movements in the left arm and leg with significant extensor tone.
– Mobility at 2 weeks with max assist or 2, total assist for all ADL’s
• Hospital Course continued:– Approx week 3 of hospitalization she was more awake
and attentive, able to move her head a little, able to move her left arm. She was able to follow some simple commands. And shave head yes and no to questions
– Started on warfarin– Able to be weaned from ventilator– Admitted to inpatient Rehab about 1 months after
initial admission– Discharged from Rehab after spending 2 months in
acute inpatient rehab
• Physical Exam at time of discharge:– Independent with bed mobility, minimal assist with
transfers, ambulating 150 feet with rolling walker and R AFO and standby assist
– Standby assist with OT for grooming, min-mod assist for bathing, min assist for dressing
– Dysphonia improved, mild ataxic speech, mild cognitive deficits in attention, insight, reasoning, and calculation
– On soft diet with thin liquids– Discharged to home with husband with in-home PT, OT , ST
as well as nursing services– Underwent elective hysterectomy 1 week after discharge
from rehab
• Physical Exam 1 ½ years post admission to hospital:– Walking with single prong cane, gait slightly narrow– A & O x 3, but still with cognitive impairments– Motor strength was 5/5 with normal tone– Mild dysmetria with f-f-n on the right– Rapid alternating movement impaired in the feet
bilaterally– Independent with dressing, grooming, bathing,
toileting.

9/23/2013
15
Posterior-Inferior Cerebellar Artery Syndromes
• Also known as Wallenberg Syndrome and includes the following:– dysarthria, dysphagia, and dysphonia– Nystagmus– Cerebellar signs including unsteady gait, vertigo, and
ataxia– Ipsilateral horner syndrome– Nausea and vomitting– Contralateral loss of pain and temperature sensation,
and loss of pain and temperature on the ipsilateralface
Posterior-Inferior Cerebellar Artery StrokeCase Review
• HPI:– 66 yo male with sudden onset of dysarthria and
dizziness on day of admission, found by wife on garage floor. He was disoriented but no LOC. Associated ptosis of left eye, double vision with left gaze, incoordination of left upper extremity as well as numbness of left upper extremity
– Initially admitted by cardiology due to bradycardia in the 30’s to 40.
• PMH:– Cirrhosis of unknown etiology– Atrial fibrillation (no warfarin due to multiple
paracentesis)– Acute on chronic renal failure– PVD– Barrett’s esophagus– Primary pulmonary hypertension d/t cirrhosis
• Social Hx:– Nonsmoker– No alcohol (etiology of cirrhosis is unknown)– Retired– Married
• Physical Exam:– BP 113/58, Pulse 53, RR 16, T 97.6– Oriented x3, able to give history accurately– VFF, Nystagmus with both left and right gaze, diplopia
with left gaze, both pupils reactive– Left facial weakness, decreased facial sensation on the
left, decreased palate elevation on the left, tongue midline, + dysphagia
– + upper extremity drift, strong hand grasp bilaterally, lower extremity strength 5/5 bilaterally
– Ataxia with F-F-N on left with past-pointing and dysmetria
• Diagnostic Studies:– MRI of brain shows large left cerebellar and posterior medullary
stroke (PICA distribution)– MRA shows focal filling defect left vertebral artery– F/U CT scan showed above stroke with mass effect on the 4th
ventricle– TTE: severe pulmonary hypertension, severe biatrial
enlargement, mod to severe tricuspid regurgitation, moderate concentric mitral regurgitation, a-fib, no shunting
– Labs on admission showed Na 123 improved with IV saline, acute on chronic renal failure, improved with conservative measures, A1C, TSH, and lipids normal
– Transferred to TC on 7/23 for possible neurosurgical intervention

9/23/2013
16
• Hospital Course:– Required feeding tube for nutrition, which was accidentally
pulled out, unable to re-insert even under radiology. Not a candidate for PEG due to ascities
– Required TPN temporarily– Transferred to inpatient Rehab for about 2 ½ weeks at TC
5 days after admission to TC– Video swallow showed no triggering of swallow– NG tube eventually able to be passed and he required
nocturnal feeding– Discharged to home on 8/16/2013 with home PT/OT/ST– Secondary stroke prevention treated with aspirin only due
to his frequent paracentesis
• Outpatient Follow-up (9/12/13):– Still requiring nocturnal tube feedings with NG tube– Voice soft and hoarse– Making slow steady progress– Walking with walker and standby assist– Still with ataxia but truncal control better– Repeat video swallow still showing frank aspiration– Requiring some help with ADL’s
Poll Question
• While having her morning cup of coffee, a 63 year old female drops her cup from her right hand and has difficulty communicating with her husband. What cerebral blood vessel is most likely affected?– A. Right ACA– B. Left ACA– C. Right MCA– D. Left MCA
Poll Question
• What clinical manifestation is commonly found when the right hemisphere is affected?– A. Right arm and leg weakness– B. Aphasia– C. Neglect/inattention– D. Bilateral vision loss

9/23/2013
17
Treatment options for Ischemic Stroke
• Reperfusion– IV TPA– IA TPA
• Mechanical clot disruption– Merci Retrieval– Penumbra– Stent retrieval
Treatment options for SAH
• Clipping• Coiling• Triple H:
– Hypertension– Hemodilutional– Hypervolemia
• Nimodipine
NURSING CARE ASSOCIATED WITH STROKE
• First 10 minutes:– Vital signs, ABC assessment– Oxygen –titrate to maintain oxygen saturation >
92%– IV access—establish 2 IV’s with one being an 18
gauge in the antecubital– Labs– cbc, lytes, PT/INR, PTT, blood sugar– Complete neurological assessment using NIHSS
• First 25 minutes:– Fully document history– Establish time of onset of stroke symptoms– Completion of physical exam– Neurologic exam
• Glasgow Coma Scale• NIHSS• Hunt and Hess (usually done by neurologist or
neurosurgeon)
• BP management prior to administration of IV t-PA
• BP > 185/110, IV t-PA contraindicated• BP lowered to < 185/110, IV t-PA can be used
– May use anti-hypertensives» Labetolol» Nicardipine» Stay away from Nipride
9/23/2013
18
• BP management:– If t-PA given goal is < 180/105 for at least 24 hours– If no t-PA permissive hypertension in early
ischemic stroke is acceptable up to 200-220 Systolic -- GOAL IS BRAIN PERFUSION
– If ICH goal SBP is < 160– If SAH SBP < 140 if aneurysm is unsecured– If SAH and aneurysm is secured, driving of SBP
acceptable to avoid cerebral vasospasm
• Nursing Care Post Admission– DVT prophylaxis
• Pneumatic devices to lower extremities (no matter which type of stroke—ischemic, SAH, ICH)
• Lovenox SQ—begin on admission for ischemic stroke, need to wait if ICH, or SAH.
– Peptic ulcer prophylaxis-especially if intubated– Swallow screening– Nutrition consult– Aspiration precautions– Physical therapy, Occupational therapy, and Speech
therapy
Statins and Stroke Prevention
Goal:• LDL goal < 100 mg/dl and possibly even < 70 mg/dl
Theories:• Decreased lipids
– Improved endothelial function– Plaque stabilization– Decreased atherosclerosis
• Anti-inflammatory effects– Thought to decrease inflammation in body and in blood vessels
therefore decreasing stroke risk
Hyperglycemia and Stroke
• Hyperglycemia accelerates large-artery atherosclerosis
• Hyperinsulinemia stimulates endothelial proliferation and promotes platelet adhesion and cholesterol deposition
• Patients with asymptomatic high glucose ( >220 mg/dl) or known diabetics have a 1.4-2.45 times higher relative risk of stroke
• Infarct size and edema occur with acute and chronic hyperglycemia
Hyperglycemia and Stroke
• High serum glucose is an independent risk factor for hemorrhage when t-PA given
• Treat with SQ or s/s insulin • Blood sugar target </= 140.
Temperature and Stroke
• Elevated temperature is associated with increased mortality and morbidity– Fever increases metabolic demands on the brain
which can lead to further tissue damage
• Elevated temperature may be due to infection or neurogenic– Assess for pneumonia or UTI
• Treat with antipyretics—goal is normothermia

9/23/2013
19
Seizure and Stroke
• Seizures are a potential complication of stroke• If not treated can potentially be life threatening• Can occur at any time—at time of stroke, during first
few day, several months after stroke, or even years after stroke
• Routine preventative use of anticonvulsants in stroke is not recommended.
Fluid Management in Stroke
• Avoid hypervolemia and hypovolemia in ischemic stroke
• Dehydration is associated with a more unfavorable outcome
• Hypervolemia can lead to cardiac complications especially in the elderly
• Use isotonic fluids for at least the first 24 hours after admission
• Nursing to monitor I & O• CVP monitoring especially in SAH
Nutrition and Stroke• Compromise of nutrition interferes with recovery• Swallow assessment by RN and then if warranted by SLP• Initiate nutrition within 48 – 72 hours after admission• Formal dietary consult to address metabolic and nutritional needs• Enteral nutrition superior to parenteral
– Advantages• Simpler application• Lower risk of infection• Normal physiologic functions of digestion and absorption• Maintenance of intestinal mucosa• Lower cost• May need motility stimulant ( i.e. metoclopramide)
• Parenteral nutrition indicted if– GI bleeding– GI leakage– GI tract unable to tolerate oral or enteral feedings
Dysphagia and Stroke
• Nurses need to monitor for choking, coughing, pocketing, garbled speech facial weakness, delayed or absent swallow reflex, drooling, watery eyes after any intake, gurgling voice
• Observe for silent aspiration• Perform aggressive oral care
– Minimizes the bacterial count which can decrease the risk of aspiration pneumonia if patient aspirates
Infection and Stroke• Pneumonia and UTI most common• Death from pneumonia occurs in approx 35% of
patients with acute stroke• Immobility leads to development of atelectasis which
leads to pneumonia• Pneumonia associated with longer duration or stay,
higher costs, and higher mobility• Treat with antibiotics• Initiate early mobility• Initiate good pulmonary toileting (SMI q 1 hour while
awake)
Infection and Stroke
• UTI’s occur in 15 - 60% of stroke patients• Increased risk of UTI in the stroke patient due
to changes in sphincter control and frequent use of indwelling catheters
• Avoid indwelling catheters if at all possible• Change in LOC is often a presenting sign of UTI• Obtain urinalysis and culture• Treat with antibiotics if necessary

9/23/2013
20
Bowel and Bladder Issues with Stroke
• Bowel and bladder dysfunction can lead to skin breakdown, UTI’s, decreased self-esteem, depression and interference with rehab progression
• Constipation is most common bowel problem post stroke– Assess bowel sounds– Assess for abdominal distension – Evaluate I&O and hydration status– Assess premorbid bowel-elimination pattern and attempt to
duplicate this pattern– Evaluate for impaction every 2 days– Bowel program including stool softeners, laxatives,
suppositories, digital stimulation, and enemas may be used
Bowel and Bladder Issues with Stroke
• Incontinence is the most common urinary complication post stroke
• AHA guidelines recommend avoiding indwelling catheters
• If needed remove as soon as possible• Never insert for nursing convenience• Intermittent catheterization may be necessary• Assess for post-void residuals.• Offer commode, bedpan or urinal every 2 hours
while awake and every 4 hours at night
Pulmonary Embolism and DVT• Up to 50% mortalities post stroke are due to PE• PE occur between 3 and 120 days post stroke, with a
mean of 20 days• Usually originate from DVT• Patient at risk of DVT due to immobilization, and weak or
paralyzed lower extremity• Passive or active ROM can be started during the first 24
hours post stroke• SQ unfractionated heparin, low-molecular-weight
heparin, and heparinoids may be used• The most effective prevention is EARLY MOBILIZATION
Mobility and Musculoskeletal Issues Post Stroke
• Complications of immobility include contractures orthopedic complications, atrophy, nerve-pressure palsies
• Nursing interventions include ROM, positioning techniques
• Need to monitor for shoulder adduction; flexion contractures of the hand, wrist and elbow; external rotation of the hip; plantar flexion of the foot. Subluxation of affected shoulder is also common, so avoid pulling on the affected arm/shoulder when moving the patient in any way
• Nursing can instruct family in ROM as well
Skin Care Post Stroke• Stroke patients at risk of skin breakdown due to loss of
sensation and impaired circulation• 9% of all hospitalized patients develop pressure ulcers• Increased risk to stroke patients due to immobility and
incontinence, as well as PVD, diabetes, and end-stage renal failure
• Reposition q 2 hours• Avoid friction when transferring• Use appropriate skin-care products• Keep skin clean and dry
Depression Post Stroke• Common with stroke patients• May be due to chemical and physical changes in the brain• Left frontal infarcts are 70% more likely to become
depressed than those with similar devastating injuries• Many need pharmacological intervention• Nursing to educated the patient and family on signs of
depression before discharge as this may occur once home• Depression can affect mobility and ADL’s• Pseudobulbar Affect is inappropriate and involuntary
laughing and crying– Frequently under recognized and undertreated

9/23/2013
21
Poll Question
• The systolic blood pressure for a patient who is to receive tPA should be less than:– A. 220 mmHg– B. 185 mmHg– C. 160 mmHg– D. 140 mmHg