
ARTICLE arthroscopic synovectomy for villo-nodular ... · villo-nodular synovitis of the knee:...
7
Orthopaedics & Traumatology: Surgery & Research (2013) 99, 937—943 Available online at ScienceDirect www.sciencedirect.com ORIGINAL ARTICLE Primary arthroscopic synovectomy for pigmented villo-nodular synovitis of the knee: Recurrence rate and functional outcomes after a mean follow-up of seven years J.C. Aurégan a,∗ , Y. Bohu a,b,c , N. Lefevre b,c , S. Klouche a,b,c , J.F. Naouri c , S. Herman b,c , P. Hardy a,d a Hôpitaux Universitaires Paris Île-de-France Ouest, AP—HP, 92100 Boulogne-Billancourt, France b Institut de l’Appareil Locomoteur Nollet, 75017 Paris, France c Sport Clinical Center, Paris V, 75005 Paris, France d Université de Versailles Saint-Quentin-en-Yvelines, UFR des Sciences de la Santé, 78035 Versailles, France Accepted: 21 August 2013 KEYWORDS Synovitis; Pigmented villo-nodular; Knee; Surgery; Arthroscopic synovectomy Summary Background: Pigmented villo-nodular synovitis (PVNS) is an uncommon proliferative condition of the synovial membrane that chiefly affects the knee. Arthroscopic synovectomy may carry lower morbidity rates but higher recurrence rates than open synovectomy. Here, our objective was to evaluate recurrence rates and functional outcomes after primary arthroscopic synovectomy for PVNS of the knee. Hypothesis: Primary arthroscopic synovectomy preserves knee function while producing low recurrence and complication rates. Materials and methods: We retrospectively included consecutive patients with histologically documented PVNS managed with primary arthroscopic synovectomy at two centres between 1998 and 2011. Twenty-three patients, 13 men and 10 women with a mean age of 41 ± 12 years, were reviewed including 16 patients with nodular and 7 with diffuse form of this disease. Patients with localized disease underwent partial synovectomy and those with diffuse disease complete synovectomy followed by chemical synovectomy of any residual lesions. The primary outcome measure was recurrence. Secondary outcome measures were the Tegner-Lysholm and Ogilvie-Harris scores. Results: Follow-up data were obtained after a mean of 7 ± 4 years in 21 patients (14 with nodu- lar and 7 with diffuse disease), of whom 2 had recurrences, after 2 and 5 years, respectively. ∗ Corresponding author. E-mail addresses: [email protected], [email protected] (J.C. Aurégan). 1877-0568/$ – see front matter © 2013 Elsevier Masson SAS. All rights reserved. http://dx.doi.org/10.1016/j.otsr.2013.08.004
-
Upload
phungkhuong -
Category
Documents
-
view
220 -
download
0
Transcript of ARTICLE arthroscopic synovectomy for villo-nodular ... · villo-nodular synovitis of the knee:...
Orthopaedics & Traumatology: Surgery & Research (2013) 99, 937—943
Available online at
ScienceDirectwww.sciencedirect.com
ORIGINAL ARTICLE
Primary arthroscopic synovectomy forpigmented villo-nodular synovitis of theknee: Recurrence rate and functionaloutcomes after a mean follow-up of sevenyears
J.C. Aurégana,∗, Y. Bohua,b,c, N. Lefevreb,c, S. Klouchea,b,c,J.F. Naouri c, S. Hermanb,c, P. Hardya,d
a Hôpitaux Universitaires Paris Île-de-France Ouest, AP—HP, 92100 Boulogne-Billancourt, Franceb Institut de l’Appareil Locomoteur Nollet, 75017 Paris, Francec Sport Clinical Center, Paris V, 75005 Paris, Franced Université de Versailles Saint-Quentin-en-Yvelines, UFR des Sciences de la Santé, 78035 Versailles, France
Accepted: 21 August 2013
KEYWORDSSynovitis;Pigmentedvillo-nodular;Knee;Surgery;Arthroscopicsynovectomy
SummaryBackground: Pigmented villo-nodular synovitis (PVNS) is an uncommon proliferative condition ofthe synovial membrane that chiefly affects the knee. Arthroscopic synovectomy may carry lowermorbidity rates but higher recurrence rates than open synovectomy. Here, our objective wasto evaluate recurrence rates and functional outcomes after primary arthroscopic synovectomyfor PVNS of the knee.Hypothesis: Primary arthroscopic synovectomy preserves knee function while producing lowrecurrence and complication rates.Materials and methods: We retrospectively included consecutive patients with histologicallydocumented PVNS managed with primary arthroscopic synovectomy at two centres between1998 and 2011. Twenty-three patients, 13 men and 10 women with a mean age of 41 ± 12 years,were reviewed including 16 patients with nodular and 7 with diffuse form of this disease.Patients with localized disease underwent partial synovectomy and those with diffuse diseasecomplete synovectomy followed by chemical synovectomy of any residual lesions. The primary
outcome measure was recurrence. Secondary outcome measures were the Tegner-Lysholm andOgilvie-Harris scores.Results: Follow-up data were obtained after a mean of 7 ± 4 years in 21 patients (14 with nodu-lar and 7 with diffuse disease), of whom 2 had recurrences, after 2 and 5 years, respectively.∗ Corresponding author.E-mail addresses: [email protected], [email protected] (J.C. Aurégan).
1877-0568/$ – see front matter © 2013 Elsevier Masson SAS. All rights reserved.http://dx.doi.org/10.1016/j.otsr.2013.08.004

938 J.C. Aurégan et al.
At last follow-up, neither patient had any evidence of recurrence. The mean Tegner-Lysholmscore was significantly improved (from 68 ± 10 to 90 ± 8, P = 0.0004) and the mean Ogilvie-Harrisscore indicated excellent function (11 ± 1).Discussion: Primary arthroscopic synovectomy ensures satisfactory control of PVNS while pre-serving knee function. A full recovery remains possible even in patients with diffuse disease. Inthe event of a recurrence, open synovectomy can be performed.Level of evidence: Level IV, retrospective study of consecutive patients.© 2013 Elsevier Masson SAS. All rights reserved.
I
PbannTcv
ol(tf
saPss[owckealaf
pPsl
M
Wipa
P
At
aawoo
i2wtmtp1Aidf1
2PomdiwaIanshm
S
TAwaslatinely. Posterior synovectomy in patients with diffuse
ntroduction
igmented villo-nodular synovitis (PVNS) is an idiopathicenign proliferative disorder of the synovial membrane withn estimated incidence of 1.8/106 population [1]. Althougho age group is exempt, younger patients seem predomi-antly affected, with no difference between genders [1].he knee is the main site of involvement [2,3] but any jointan be affected [4]. Untreated PVNS rapidly results in irre-ersible joint destruction.
In 1976, Granowitz et al. [5] distinguished two variantsf PVNS based on whether the intra-articular lesions wereocalised (nodular PVNS) or affected the entire synoviumdiffuse PVNS). Extra-articular extension of the lesions tohe adjacent muscles and tendons can occur, chiefly in dif-use forms [6].
Complete surgical excision of all the lesions is thetandard treatment for PVNS [7]. The surgical modalitiesre poorly standardised, however, as the low incidence ofVNS precludes large treatment trials. In general, open totalynovectomy is preferred in diffuse PVNS [8] and arthro-copic synovectomy is reserved for localised nodular PVNS9,10]. Compared to open synovectomy, arthroscopic syn-vectomy may ensure better preservation of knee functionhile producing acceptable local recurrence rates and fewomplications [10,11]. Both the local recurrence rate andnee function recovery have been reported to vary with thextent of the lesions [12]. Nevertheless, PVNS is probably
continuum with no clear-cut separation between nodu-ar and diffuse forms. The better functional outcomes withrthroscopy compared to open surgery constitute a rationaleor broadening the indications of arthroscopic treatment.
Here, our main objective was to evaluate outcomes afterrimary arthroscopic synovectomy for nodular or diffuseVNS. Our study hypothesis was that primary arthroscopicynovectomy would preserve knee function while producingow recurrence and complication rates.
aterial and methods
e conducted a retrospective study in two centres special-zed in arthroscopic surgery of the knee. In both centres, allatients with PVNS of the knee were managed with primaryrthroscopic synovectomy.
atient selection
ll patients managed with arthroscopic synovectomy for his-ologically documented PVNS of the knee between 1998
dfTn
nd 2011 were eligible, including those with recurrent PVNSfter arthroscopic synovectomy. We did not include patientsith extra-articular lesions and/or a history of open syn-vectomy of the same knee and/or recurrent PVNS afterpen surgery at the same knee.
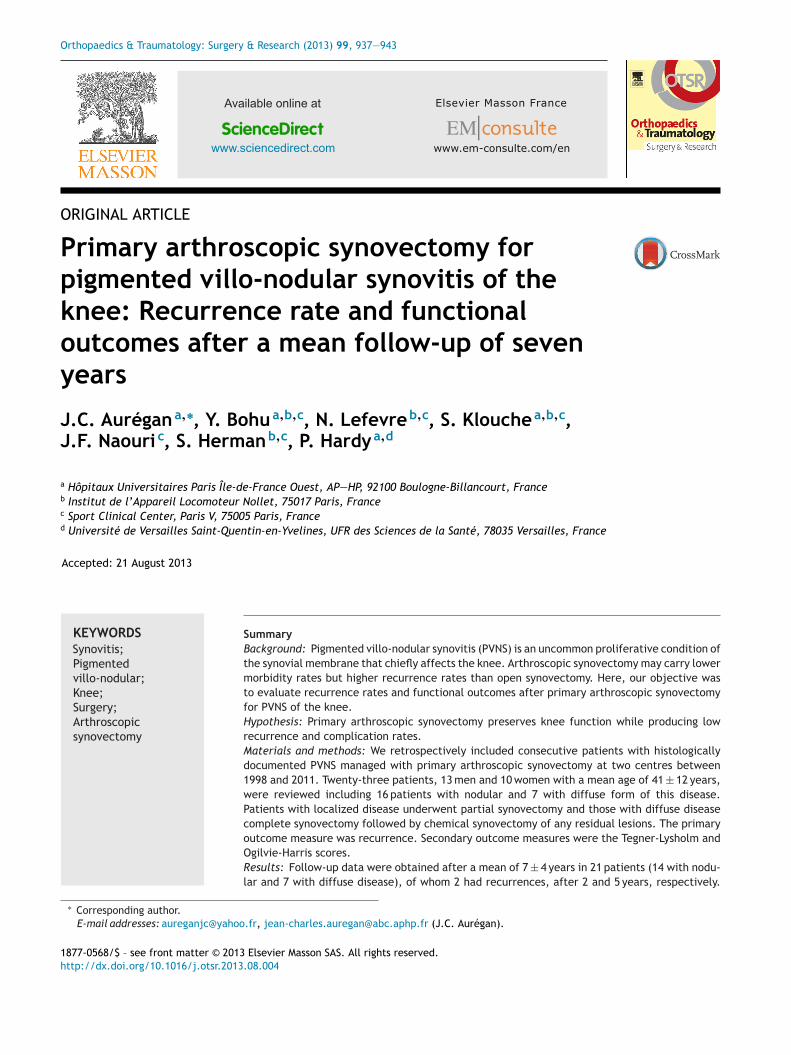
During the study period, 28 patients underwent surgeryn either centre for PVNS of the knee (Fig. 1). Among them,
had superficial lesions extending extra-articularly andere managed with open surgery. Of the 26 arthroscopically
reated patients, 3 had recurrent diffuse PVNS after pri-ary open synovectomy performed elsewhere and were
herefore not included in our study. Of the 23 includedatients, 7 had diffuse and 16 nodular disease. There were3 men and 10 women with a mean age of 41 ± 12 years.mong these 23 patients, 3 had recurrent PVNS, includ-
ng 1 after partial arthroscopic synovectomy for nodularisease and 2 after incomplete arthroscopic synovectomyor diffuse disease. Mean maximum knee flexion was26 ± 12◦.
Magnetic resonance imaging (MRI) was performed in2 of the 23 patients (Figs. 2 and 3). Changes suggestingVNS were recorded including thickening and heterogeneityf the synovial membrane with post-gadolinium enhance-ent and low-signal foci consistent with hemosiderineposits within the joint [13]. The findings indicated def-nite PVNS in 14 patients and possible PVNS in 6 patients,hereas 2 patients had no suggestive MRI features. MRIlso served to assess the extent of the synovial lesions.n 1 patient, a metallic foreign body precluded MRInd computed arthrotomography was performed instead:o changes suggesting PVNS were found. The diagno-is was confirmed postoperatively in all 23 patients byistological examination of the synovial membrane speci-en.
urgical technique
he 23 procedures were performed by 3 senior surgeons. 30◦ arthroscope was used. A synovial membrane biopsyas obtained routinely. Synovectomy was achieved using
motorised shaver with a 5.5-mm blade and the threetandard portals (antero-medial, antero-lateral, and supero-ateral). In patients with nodular lesions confined to thenterior knee, the posterior knee was not explored rou-
isease (Fig. 4) or posterior nodular disease (Fig. 5) was per-ormed via the postero-medial and postero-lateral portals.he postero-medial approach was achieved by transillumi-ation [9].
Primary arthroscopic synovectomy for pigmented villo-nodular synovitis of the knee 939
PVN S of th e kn ee (N=28 )
MRI (N=27/28 )
Exclud ed (N=5)
Local ized PVNS (N=16 )
Type of PVN S Diffuse PVNS
(N=7)
ymotcevonys latot cipocsorhtrA ymotcevonys desilacol cipocsorhtrA
seY oNRisk of residu al
lesion (Y / N)
No adjuv ant trea tment (N=16 locali sed and 2 diff use)
Chemic al synovec tomy at 3 mon ths (N=5)
o-no
Tfe1
S
Sfwcps
R
Oane2
C
Ath1
R
Figure 1 Patient flow chart (PVNS = pigmented vill
Postoperative chemical synovectomy
In patients with diffuse PVNS, the joint cavity was care-fully explored after total synovectomy to assess the riskof residual lesions. When the risk was deemed non-existent, no additional treatment was given. Otherwise,chemical synovectomy was performed 3 to 6 months afterthe arthroscopic procedure. Osmic acid was used until2007, when the French drug safety agency withdrew thiscompound, and triamcinolone hexacetonide (Hexatrione®)thereafter.
Postoperative management
A drain was placed routinely in the joint cavity then removedafter 24 to 72 hours. Passive and active rehabilitation ther-apy was started on the first postoperative day and continuedfor 1 month. A knee-extension splint was worn between therehabilitation sessions for 1 month to avoid flexion contrac-ture. Patients were re-evaluated after 1, 3, 6, and 12 monthsthen once a year. MRI with gadolinium injection was per-formed after 1 year. For this study, all patients were askedto come in for re-evaluation.
Outcome measures
The primary evaluation criterion was the rate of local recur-rence at last follow-up. Local recurrence was suspectedbased on the clinical and or MRI findings then confirmedhistologically.
Secondary outcome measures were the scores at lastfollow-up on two knee-function scales, the Tegner-LysholmKnee Scoring Scale for general knee function [14] and theOgilvie-Harris scale developed specifically for PVNS [12].
M2l
dular synovitis; MRI = magnetic resonance imaging).
egner-Lysholm score categories were 0—64, poor; 65—83,air; and 84—100, excellent. Ogilvie-Harris scores were cat-gorized as follows: 0—3, poor; 4—6, fair; 7—9, good; and0—12, excellent.
tatistical analysis
TATA.10 (StataCorp, College Station, TX, USA) was usedor the statistical analyses. Given the small sample size,e chose non-parametric tests. Quantitative variables wereompared using the Mann-Whitney test or Wilcoxon test foraired data. Values of P smaller than 0.05 were consideredignificant.
esults
f the 23 patients, 2 were lost to follow-up, after 2 monthsnd 13 years, respectively. Both had nodular disease andeither experienced recurrences. These 2 patients werexcluded from the analyses. Mean follow-up in the remaining1 patients was 7 ± 4 years.
omplications
25-year-old woman with diffuse PVNS managed byotal arthroscopic synovectomy experienced postoperativeaemarthrosis. Surgical drainage of the joint was required
month after surgery.
ecurrence rate
RI was performed 1 year postoperatively in 17 of the3 patients and showed no signs of recurrence. Neverthe-ess, histologically documented recurrences developed in
940 J.C. Aurégan et al.
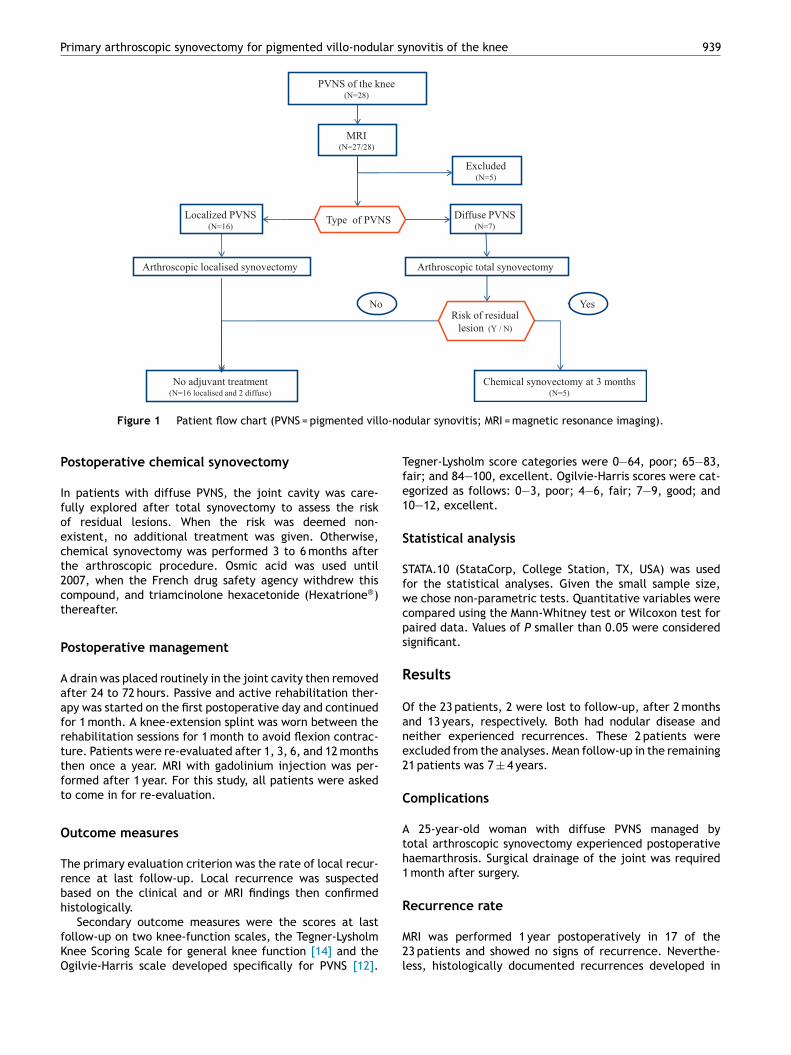
Figure 2 Magnetic resonance imaging in a patient with nodular pigmented villo-nodular synovitis of the knee. a: coronal section,T2 fast spin-echo Fat-Sat sequence: well-delineated intra-articular ovoid mass overhanging the anterior inter-meniscal ligament onthe midline, generating higher signal than the surrounding tissue, and surrounded by a low-signal shell; b: sagittal section, T2 fastspin-echo Fat-Sat sequence: mass in contact with Hoffa’s triangle, with no evidence of infiltration. Markedly low signal from theshell. Heterogeneous content, with relative high signal contrasting with low-signal foci. No joint effusion; c: axial section, T2 fastspin-echo Fat-Sat sequence: the mass is located on the midline; d: sagittal section, T1 sequence: ovoid mass anterior to the insertiono rates y a l
2wtcbaslPsradflAr
sMs
F
Tf(cdm
f the anterior cruciate ligament, from which it is clearly sepaignal relative to the gastrocnemius muscle and is surrounded b
patients, both with diffuse disease. A 41-year-old manith diffuse PVNS of the right knee initially treated with
otal arthroscopic synovectomy followed 3 months later byhemical synovectomy had normal MRI findings after 1 yearut was diagnosed with a recurrence 5 years after therthroscopic procedure. He was managed with open totalynovectomy and had no evidence of recurrence 3 yearsater. The other patient was a 27-year-old man with diffuseVNS of the left knee. He underwent incomplete arthro-copic synovectomy at another centre then experienced aecurrence managed with arthroscopic total synovectomyt one of the study centres. The risk of residual lesions waseemed non-existent and chemical synovectomy was there-
ore not performed. A recurrence was diagnosed 2 yearsater and managed with arthroscopic total synovectomy.t last follow-up 6 months later, he had no signs of recur-ence.anPo
d. The mass is sharply marginated. Its content generates highow-signal shell.
Repeat arthroscopy was performed in 2 patients with per-istent pain suggesting a recurrence despite the absence ofRI abnormalities. The gross and histological features of the
ynovial membrane ruled out a recurrence.
unctional outcomes
he mean Tegner-Lysholm score improved significantlyrom 68 ± 10 pre-operatively to 90 ± 8 at last follow-upP = 0.0004). Mean values at last follow-up were not signifi-antly different between the groups with diffuse and nodularisease (90 ± 7 and 90 ± 10, respectively, P = 0.91). Theean Ogilvie-Harris score at last follow-up was 11 ± 1 over-
ll, with no significant difference between the groups withodular and diffuse disease (11 ± 1 and 10 ± 1, respectively;
= 0.53). Both score values indicated excellent functionalutcomes at last follow-up.
Primary arthroscopic synovectomy for pigmented villo-nodular synovitis of the knee 941
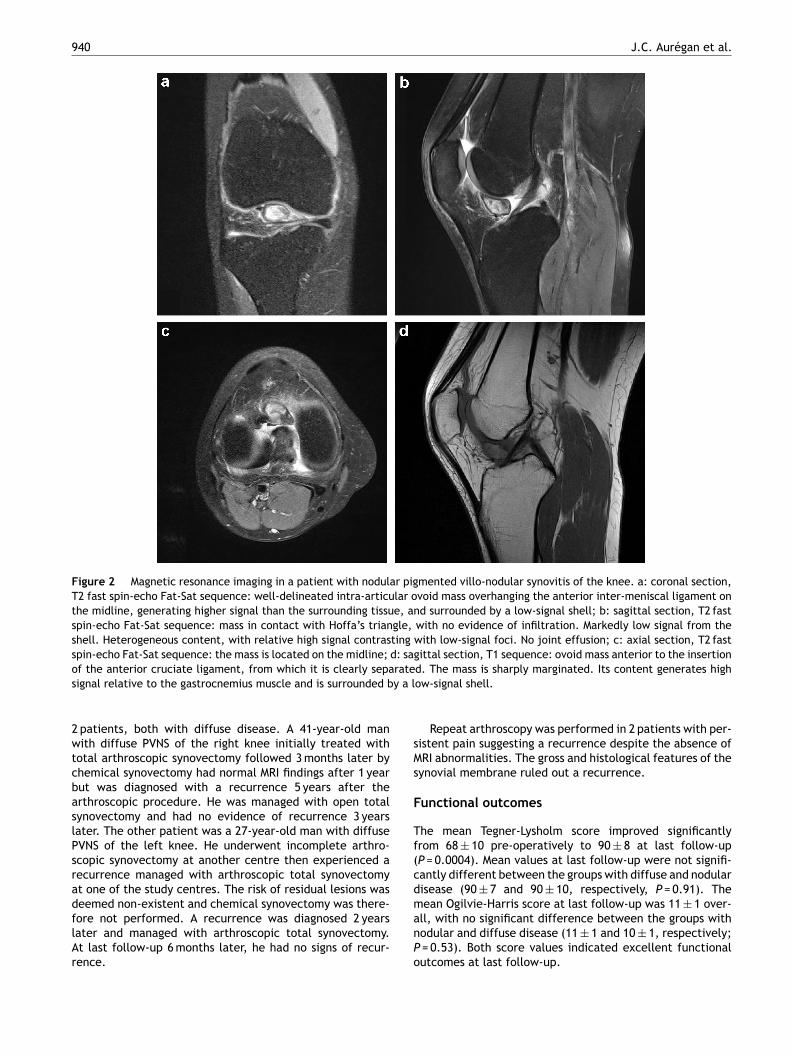
Figure 3 Magnetic resonance imaging in a patient with diffuse villo-nodular synovitis of the knee. T1-sequence before (a) andafter (b) injection. Diffuse thickening and enhancement of the anterior and posterior synovial membrane. Joint effusion.
Figure 4 Arthroscopic appearance of diffuse pigmented villo-nodular synovitis of the knee. The arthroscope has been insertedg exmorr
bi7twnmem(wp[o
via the antero-lateral portal and the quadricipital recess is beintypical appearance of thick tan-coloured villi with pinpoint hae
Discussion
This study shows that primary arthroscopic synovectomy forPVNS of the knee is associated with few complications andproduces an overall low recurrence rate while preservingknee function.
Whereas nodular PVNS is associated with few or norecurrences [10,15], diffuse PVNS can recur regardless ofthe treatment modality used [16]. In our study, none of thepatients with nodular disease experienced recurrences, inkeeping with findings from two other case-series studies[10,15]. In contrast, in a study of 20 patients with nodu-lar PVNS, 4 (20%) patients had recurrences [17]. Recurrencerates after open synovectomy for nodular PVNS have rangedfrom 0% [18] to 15% [19] and 29% [8]. In our patients with
diffuse disease, the 29% (2/7 patients) recurrence rate isconsistent with recurrence rates reported after open syn-ovectomy (25% [20], 33%, [21], and 46% [19]). However, onegroup reported a recurrence rate of only 8% [22].t
ra
plored. Villi are seen to line the entire joint surface. Note thehagic effusions.
Mean functional scores in our study were excellent inoth nodular and diffuse disease. No significant differencen function was found between these two groups, but only
patients had diffuse lesions. In previous studies, func-ional outcomes seemed better in nodular disease and variedith the treatment modality. In a study of 20 patients withodular PVNS managed with arthroscopic synovectomy, theedian Tegner-Lysholm score at last follow-up indicated
xcellent function (85.5; range, 83—88) [17]. In 25 patientsanaged arthroscopically for diffuse (n = 20) or nodular
n = 5) PVNS, the mean postoperative Ogilvie-Harris scoreas 11.3 (excellent) after nodule excision, 7.8 (good) afterartial synovectomy, and 9.3 (good) after total synovectomy12]. In contrast to arthroscopic surgery, open surgery isften associated with range-of-motion limitation (24% [22]
o 50% [21] of patients).Thus, routine primary arthroscopic synovectomy allowsemoval of the largest possible number of lesions while prob-bly providing better function than open surgery and also
942 J.C. Aurégan et al.
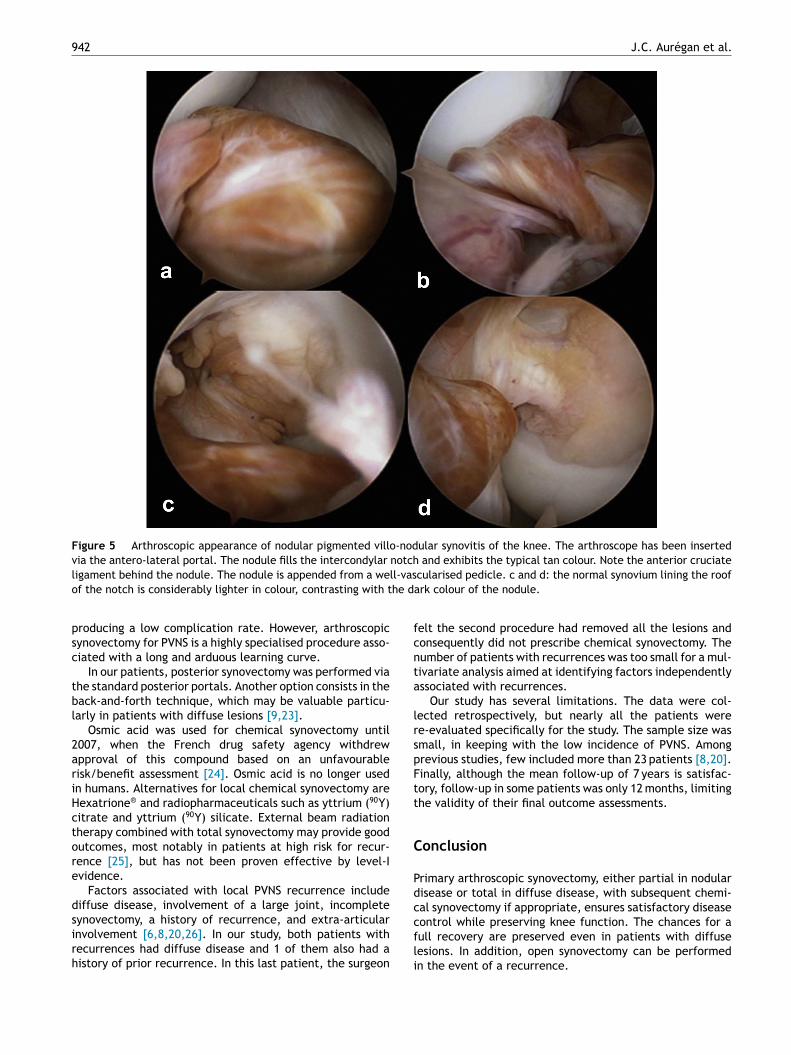
Figure 5 Arthroscopic appearance of nodular pigmented villo-nodular synovitis of the knee. The arthroscope has been insertedvia the antero-lateral portal. The nodule fills the intercondylar notch and exhibits the typical tan colour. Note the anterior cruciatel ll-vaso he d
psc
tbl
2ariHctore
dsirh
fcnta
lrspFtt
C
Pdc
igament behind the nodule. The nodule is appended from a wef the notch is considerably lighter in colour, contrasting with t
roducing a low complication rate. However, arthroscopicynovectomy for PVNS is a highly specialised procedure asso-iated with a long and arduous learning curve.
In our patients, posterior synovectomy was performed viahe standard posterior portals. Another option consists in theack-and-forth technique, which may be valuable particu-arly in patients with diffuse lesions [9,23].
Osmic acid was used for chemical synovectomy until007, when the French drug safety agency withdrewpproval of this compound based on an unfavourableisk/benefit assessment [24]. Osmic acid is no longer usedn humans. Alternatives for local chemical synovectomy areexatrione® and radiopharmaceuticals such as yttrium (90Y)itrate and yttrium (90Y) silicate. External beam radiationherapy combined with total synovectomy may provide goodutcomes, most notably in patients at high risk for recur-ence [25], but has not been proven effective by level-Ividence.
Factors associated with local PVNS recurrence includeiffuse disease, involvement of a large joint, incomplete
ynovectomy, a history of recurrence, and extra-articularnvolvement [6,8,20,26]. In our study, both patients withecurrences had diffuse disease and 1 of them also had aistory of prior recurrence. In this last patient, the surgeoncfli
cularised pedicle. c and d: the normal synovium lining the roofark colour of the nodule.
elt the second procedure had removed all the lesions andonsequently did not prescribe chemical synovectomy. Theumber of patients with recurrences was too small for a mul-ivariate analysis aimed at identifying factors independentlyssociated with recurrences.
Our study has several limitations. The data were col-ected retrospectively, but nearly all the patients weree-evaluated specifically for the study. The sample size wasmall, in keeping with the low incidence of PVNS. Amongrevious studies, few included more than 23 patients [8,20].inally, although the mean follow-up of 7 years is satisfac-ory, follow-up in some patients was only 12 months, limitinghe validity of their final outcome assessments.
onclusion
rimary arthroscopic synovectomy, either partial in nodularisease or total in diffuse disease, with subsequent chemi-al synovectomy if appropriate, ensures satisfactory disease
ontrol while preserving knee function. The chances for aull recovery are preserved even in patients with diffuseesions. In addition, open synovectomy can be performedn the event of a recurrence.
lar sy
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Primary arthroscopic synovectomy for pigmented villo-nodu
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
Acknowledgements
We are deeply grateful to Ms. Pauline Ajoux, scientific sec-retary, for her valuable assistance.
References
[1] Myers B, Masi A, Feigenbaum S. Pigmented villonodular syn-ovitis and tenosynovitis: a clinical epidemiologic study of onehundred and sixty-six cases and literature review. Medicine1980;59:223—8.
[2] Molfetta L, Vavalle G, Ippolito B, et al. Sinovite villo-nodularepigmentosa dell’anca. Contributo casistico. Min Orthop Trau-mat 1993;44:25—9 [In Italian].
[3] Dorwart RH, Genant HK, Johnston WH, et al. Pigmentedvillonodular synovitis of the shoulder: radiologic-pathologicassessment. AJR Am J Roentgenol 1984;143:886—8.
[4] Mahieu X, Chaouat G, Blin JL, Frank A, Hardy P. Arthroscopictreatment of pigmented villonodular synovitis of the shoulder.Arthroscopy 2001;17:81—7.
[5] Granowitz SP, D’Antonio J, Mankin HL. The pathogenesis andlong-term end results of pigmented villonodular synovitis. ClinOrthop Relat Res 1976;114:335—51.
[6] Chin KR, Barr SJ, Winalski C, Zurakowski D, Brick GW. Treat-ment of advanced primary and recurrent diffuse pigmentedvillonodular synovitis of the knee. J Bone Joint Surg Am2002;84—A:2192—202.
[7] De Ponti A, Sansone V, Malcherè M. Result of arthroscopictreatment of pigmented villonodular synovitis of the knee.Arthroscopy 2003;19:602—7.
[8] Sharma V, Cheng EY. Outcomes after excision of pigmentedvillonodular synovitis of the knee. Clin Orthop Relat Res2009;467:2852—8.
[9] Charrois O, Louisia S, Beaufils P. [Arthroscopic synovec-tomy of the knee]. Rev Chir Orthop Reparatrice Appar Mot2004;90:771—5.
[10] Kim SJ, Shin SJ, Choi NH, Choo ET. Arthroscopic treatment forlocalized pigmented villonodular synovitis of the knee. Clin
Orthop Relat Res 2000;(379):224—30.[11] Ogilvie-Harris DJ, Weisleder L. Arthroscopic synovec-tomy of the knee: is it helpful? Arthroscopy 1995;11:91—5.
[
novitis of the knee 943
12] Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villon-odular synovitis of the knee: the results of total arthroscopicsynovectomy, partial arthroscopic synovectomy and arthro-scopic local excision. J Bone Joint Surg Am 1992;74:119—23.
13] Mandelbaum BR, Grant TT, Hartzman S, et al. The use of MRI toassist in diagnosis of pigmented villonodular synovitis of kneejoint. Clin Orthop Relat Res 1988;231:135—9.
14] Tegner Y, Lysholm J. Rating systems in the evaluation of kneeligament injuries. Clin Orthop Relat Res 1985;198:43—9.
15] Ozalay M, Tandogan RN, Akpinar S, Cesur N, Hersekli MA,Ozkoc G, et al. Arthroscopic treatment of solitary benign intra-articular lesions of the knee that cause mechanical symptoms.Arthroscopy 2005;21:12—8.
16] Pinaroli A, Aït Si Selmi T, Servien E, Neyret P. [Surgicalmanagement of pigmented villonodular synovitis of the knee:retrospective analysis of 28 cases]. Rev Chir Orthop ReparatriceAppar Mot 2006;92:437—47 [In French].
17] Loriaut P, Djian P, Boyer T, Bonvarlet JP, Delin C, MakridisKG. Arthroscopic treatment of localized pigmented villonodu-lar synovitis of the knee. Knee Surg Sports Traumatol Arthrosc2012;20:1550—3.
18] Dines JS, DeBerardino TM, Wells JL, Dodson CC, ShindleM, DiCarlo EF, et al. Long-term follow-up of surgicallytreated localized pigmented villonodular synovitis of the knee.Arthroscopy 2007;23:930—7.
19] Byers PD, Cotton RE, Deacon OW. The diagnosis and treat-ment of pigmented villonodular synovitis. J Bone Joint SurgBr 1968;50:290—305.
20] Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodularsynovitis: a retrospective review of affected large joints. ClinOrthop 1989;247:243—55.
21] Johansson JE, Ajjoub S, Coughlin LP, et al. Pigmented villon-odular synovitis of the joints. Clin Orthop 1982;163:159—66.
22] Flandry FC, Hughston JC, Jacobson KE, et al. Surgical treat-ment of diffuse pigmented villonodular synovitis of the knee.Clin Orthop Rel Res 1994;300:183—92.
23] Louisia S, Charrois O, Beaufils P. Posterior ‘back and forth’approach in arthroscopic surgery on the posterior knee com-partments. Arthroscopy 2003;19:321—5.
24] http://ansm.sante.fr/S-informer/Informations-de-securite-Lettres-aux-professionnels-de-sante/Utilisation-de-l-acide-osmique-en-therapeutique-humaine accessed on 15 July2013.
25] O’Sullivan B, Cummings B, Catton C, Bell R, Davis A, FornasierV, et al. Outcome following radiation treatment for high-riskpigmented villonodular synovitis. Int J Radiat Oncol Biol Phys
1995;32:777—86.26] Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affectsthe recurrence and clinical outcome of pigmented villonodularsynovitis? Clin Orthop Relat Res 2006;450:172—8.

















![Case Report Arthroscopic Synovectomy in Bilateral Lipoma ...Open synovectomy was previously selected as curative treatment option [10]. In recent years, many authors have published](https://static.fdocuments.net/doc/165x107/60df52301d297a2cf21d2745/case-report-arthroscopic-synovectomy-in-bilateral-lipoma-open-synovectomy-was.jpg)
