Antioxidant and prooxidant properties of ascorbic acid on hepatic dysfunction induced by cold...
6
Antioxidant and prooxidant properties of ascorbic acid on hepatic dysfunction induced by cold ischemia/reperfusion Sang-Won Park, Sun-Mee Lee ⁎ College of Pharmacy, Sungkyunkwan University, 300 Cheoncheon-dong, Jangan-gu, Suwon-si, Gyeonggi-do 440-746, South Korea Received 26 July 2007; received in revised form 30 October 2007; accepted 10 November 2007 Available online 23 November 2007 Abstract Oxidative stress, which has been generated during reperfusion after a liver transplant, has been implicated in the higher rates of postoperative organ dysfunction. The aim of this study was to examine the effect of ascorbic acid on reperfusion injury after hepatic cold preservation. Isolated perfused rat livers were preserved in a University of Wisconsin solution for 30 h at 4 °C. The bile output was significantly lower after cold ischemia/ reperfusion. In contrast, the portal pressure, lactate dehydrogenase and purine nucleoside phosphorylase activities were elevated by cold ischemia/ reperfusion. These changes were attenuated at ascorbic acid concentrations of 0.25 and 0.5 mM. However, they were augmented at a concentration of 2 mM. Cold ischemia/reperfusion decreased the reduced to oxidized glutathione ratio, whereas it increased the level of lipid peroxidation and mitochondrial swelling. These changes were prevented exposing the liver to 0.5 mM ascorbic acid but were augmented at 2 mM ascorbic acid. These results suggest that cold ischemia/reperfusion injury is associated with a higher level of oxidative stress and ascorbic acid may act not only as an antioxidant but also as a prooxidant during cold ischemia/reperfusion. © 2007 Elsevier B.V. All rights reserved. Keywords: Ascorbic acid; Hepatic cold ischemia; University of Wisconsin solution; Oxidative stress; Mitochondrial permeability transition 1. Introduction Cold ischemia/reperfusion injury is one of the major obstacles to liver transplantation. In a clinical setting, 15% to 25% of liver allografts do not show full functional recovery when reperfused, and as many as 6% of them fail postoperatively for no known reason (Deschenes et al., 1998). This primary graft nonfunction is caused by ischemia/reperfusion injury and is a dreaded complication because there is no effective treatment other than retransplantation. The current shortage of organs has created the need for a better understanding of the pathophysiol- ogy responsible for cold ischemia/reperfusion injury so that new strategies for hepatic protection can be developed. Reactive oxygen species have been implicated in the pathogenesis of hepatic reperfusion injury. Several studies have shown no evidence for any relevant intracellular oxidant stress in hepatocytes during reperfusion. Subsequent studies indicated the formation of extracellular reactive oxygen species by Kupffer cells and neutrophils, which begins immediately after reperfusion (Jaeschke and Farhood, 1991). Therefore, enhancing the liver antioxidant capacity can be viewed as a promising therapeutic strategy. Many approaches involving the administration of various antioxidants have been attempted with varying effectiveness (De Tata et al., 2005). Natural antioxidants oppose oxidative stress by reducing the reactive oxidants. A previous study suggested that α-tocopherol requires several days of pretreatment to have any antioxidative benefits, while ascorbic acid may act more rapidly during oxidative stress on account of its water solubility (Wu et al., 1991). Ascorbic acid, which is a strong antioxidant, has been used to reduce the oxidative indices after ischemia/reperfusion. Paradoxically, ascorbic acid has also been associated with prooxidant effects, and is known for its ability to reduce metals to forms that react with oxygen to form lipid peroxidation initiators (Prat and Turrens, 1990). Recently, we reported that ascorbic acid acts primarily as an antioxidant in hepatic warm ischemia/reperfusion at low doses but as a prooxidant at high doses (Seo and Lee, 2002). However, there is no information on Available online at www.sciencedirect.com European Journal of Pharmacology 580 (2008) 401 – 406 www.elsevier.com/locate/ejphar ⁎ Corresponding author. Tel.: +82 31 290 7712; fax: +82 31 292 8800. E-mail address: [email protected] (S.-M. Lee). 0014-2999/$ - see front matter © 2007 Elsevier B.V. All rights reserved. doi:10.1016/j.ejphar.2007.11.023
-
Upload
sang-won-park -
Category
Documents
-
view
212 -
download
0
Transcript of Antioxidant and prooxidant properties of ascorbic acid on hepatic dysfunction induced by cold...
Available online at www.sciencedirect.com
gy 580 (2008) 401–406www.elsevier.com/locate/ejphar
European Journal of Pharmacolo
Antioxidant and prooxidant properties of ascorbic acid on hepaticdysfunction induced by cold ischemia/reperfusion
Sang-Won Park, Sun-Mee Lee ⁎
College of Pharmacy, Sungkyunkwan University, 300 Cheoncheon-dong, Jangan-gu, Suwon-si, Gyeonggi-do 440-746, South Korea
Received 26 July 2007; received in revised form 30 October 2007; accepted 10 November 2007
Available online 23 November 2007
Abstract
Oxidative stress, which has been generated during reperfusion after a liver transplant, has been implicated in the higher rates of postoperativeorgan dysfunction. The aim of this study was to examine the effect of ascorbic acid on reperfusion injury after hepatic cold preservation. Isolatedperfused rat livers were preserved in a University of Wisconsin solution for 30 h at 4 °C. The bile output was significantly lower after cold ischemia/reperfusion. In contrast, the portal pressure, lactate dehydrogenase and purine nucleoside phosphorylase activities were elevated by cold ischemia/reperfusion. These changes were attenuated at ascorbic acid concentrations of 0.25 and 0.5 mM. However, they were augmented at a concentrationof 2 mM. Cold ischemia/reperfusion decreased the reduced to oxidized glutathione ratio, whereas it increased the level of lipid peroxidation andmitochondrial swelling. These changes were prevented exposing the liver to 0.5 mM ascorbic acid but were augmented at 2 mM ascorbic acid.These results suggest that cold ischemia/reperfusion injury is associated with a higher level of oxidative stress and ascorbic acid may act not only asan antioxidant but also as a prooxidant during cold ischemia/reperfusion.© 2007 Elsevier B.V. All rights reserved.
Keywords: Ascorbic acid; Hepatic cold ischemia; University of Wisconsin solution; Oxidative stress; Mitochondrial permeability transition
1. Introduction
Cold ischemia/reperfusion injury is one of the majorobstacles to liver transplantation. In a clinical setting, 15% to25% of liver allografts do not show full functional recoverywhen reperfused, and as many as 6% of them fail postoperativelyfor no known reason (Deschenes et al., 1998). This primary graftnonfunction is caused by ischemia/reperfusion injury and is adreaded complication because there is no effective treatmentother than retransplantation. The current shortage of organs hascreated the need for a better understanding of the pathophysiol-ogy responsible for cold ischemia/reperfusion injury so that newstrategies for hepatic protection can be developed.
Reactive oxygen species have been implicated in thepathogenesis of hepatic reperfusion injury. Several studieshave shown no evidence for any relevant intracellular oxidantstress in hepatocytes during reperfusion. Subsequent studies
⁎ Corresponding author. Tel.: +82 31 290 7712; fax: +82 31 292 8800.E-mail address: [email protected] (S.-M. Lee).
0014-2999/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.ejphar.2007.11.023
indicated the formation of extracellular reactive oxygen speciesby Kupffer cells and neutrophils, which begins immediatelyafter reperfusion (Jaeschke and Farhood, 1991). Therefore,enhancing the liver antioxidant capacity can be viewed as apromising therapeutic strategy. Many approaches involving theadministration of various antioxidants have been attempted withvarying effectiveness (De Tata et al., 2005).
Natural antioxidants oppose oxidative stress by reducing thereactive oxidants. A previous study suggested that α-tocopherolrequires several days of pretreatment to have any antioxidativebenefits, while ascorbic acid may act more rapidly duringoxidative stress on account of its water solubility (Wu et al.,1991). Ascorbic acid, which is a strong antioxidant, has beenused to reduce the oxidative indices after ischemia/reperfusion.Paradoxically, ascorbic acid has also been associated withprooxidant effects, and is known for its ability to reduce metalsto forms that react with oxygen to form lipid peroxidationinitiators (Prat and Turrens, 1990). Recently, we reported thatascorbic acid acts primarily as an antioxidant in hepatic warmischemia/reperfusion at low doses but as a prooxidant at highdoses (Seo and Lee, 2002). However, there is no information on

402 S.-W. Park, S.-M. Lee / European Journal of Pharmacology 580 (2008) 401–406
the effect of ascorbic acid on reperfusion injury after cold storageof the liver.
Therefore, this study examined the effects of ascorbic acid onthe preservation/reperfusion injury in an isolated perfused ratliver model.
2. Materials and methods
2.1. Reagents
The University of Wisconsin solution (Viaspan®, Bristol-Myers Squibb, Co., Princeton, NY, USA) was donated by theJeil Pharmaceutical Company of Korea. Unless otherwisenoted, all reagents were obtained from Sigma Chemicals Co.(St. Louis, MO, USA) and used as received.
2.2. Isolated perfused rat liver
Male Sprague-Dawley rats (270–300 g) were fasted over-night, but allowed access to water ad libitum. The use and careof animals were approved by Sungkyunkwan UniversityAnimal Care Committee guidelines. The rats were anesthetizedwith sodium pentobarbital (40 mg/kg i.p.). After the abdomenwas opened, the rats received 400 U/kg of heparin via theinferior vena cava before the liver was isolated. The bile ductwas cannulated with a polyethylene tube-10, a polyethylenetube-190 was inserted into the portal vein and the livers wereperfused with Krebs–Henseleit bicarbonate buffer at a constantflow rate of 4 ml/min/g liver. The Krebs–Henseleit bicarbonatebuffer contained 118 mM NaCl, 4.8 mM KCl, 2.5 mM CaCl2,1.2 mM KH2PO4, 1.2 mM MgSO4, 25 mM NaHCO3, 0.1 mMEDTA, 5 mM glucose and 0.03 mM sodium taurocholate. Theinferior vena cava was then cannulated through the right atriumand ligated above the right renal vein. The liver was dissectedfree and transferred to the perfusion chamber. In all experi-mental groups, the livers were perfused with Krebs-Henseleitbicarbonate buffer at 37 °C in a nonrecirculating manner. Theperfusion buffer was gassed with a mixture of 95% O2 and 5%CO2 using an oxygenator. The bile output was measured gra-vimetrically in pretared tubes. The portal pressure was mo-nitored manometrically from the tubing attached to the inflowcannula (Charrueau et al., 2002).
2.3. Experimental protocol
One group of rats was exposed to continuous liver perfusionwithout ischemia and five groups were subjected to cold ische-mia/reperfusion. Group 1 (control, n=8) underwent continuousperfusion for 120 min. The livers of groups 2–6 were perfusedwith Krebs–Henseleit bicarbonate buffer for 20 min. The liverswere then rinsed with 10 ml University of Wisconsin solution(4 °C) and stored at 4 °C in 50 ml University of Wisconsinsolution for 30 h. Arai et al. (2001) showed that after storage for30 h in University of Wisconsin solution, rat liver graft failurewas similar to the graft failure occurring in human livers. Aftercold storage, the livers were reperfused for 120 min as follows:untreated (group 2, n=10), 60 min or 120 min of reperfusion
with Krebs–Henseleit bicarbonate buffer; ascorbic acid wasadded to make total concentrations of 0.25, 0.5, 1 or 2 mM,respectively. These ascorbic acid concentrations were selectedbecause they had been previously evaluated in an isolatedperfused rat liver model of hypoxia and reoxygenation (Youneset al., 1992). The ascorbic acid concentrations used in the as-corbic acid treatment for 60 min or 120 min (groups 3–6) wereas follows: the reperfusion of the liver with 0.25 mM (group 3,n=10), 0.5 mM (group 4, n=10), 1 mM (group 5, n=10), or2 mM (group 6, n=10). The liver was weighed at the end ofreperfusion and used for the experiments.
2.4. Analytical procedures
The sinusoidal efflux of lactate dehydrogenase and purinenucleoside phosphorylase were measured as the indices of livercell damage (Bailey and Reinke, 2000). The activity of lactatedehydrogenase in the perfusate was analyzed by thespectrophotometry procedures in the ChemiLab LDH assaykit (IVDLab Co., Ltd., Suwon, Korea). The purine nucleosidephosphorylase activity was determined from the xanthineoxidase-coupled formation of uric acid at 293 nm accordingto the method reported by Hoffee et al. (1978). The totalglutathione concentration in the perfusate was measured usingthe glutathione reductase and 5,5'-dithio-bis-(2-nitrobenzoicacid) method (Brehe and Burch, 1976). GSSG concentrationwas determined after derivatization of the GSH with 2-vinylpyridine. The GSH concentration was calculated fromthe difference between the total glutathione and GSSGconcentrations. The steady-state level of malondialdehyde inthe liver tissues, which is the end product of lipid peroxidation,was determined by measuring the level of the thiobarbituricacid-reactive substances spectrophotometrically at 532 nm, asdescribed by Buege and Aust (1978). The rat liver mitochondriawere isolated using the method described by Johnson and Lardy(1967). The rate of mitochondrial swelling, which indicates theextent of the mitochondrial permeability transition, wasdetermined by measuring the change in the absorbance of amitochondrial suspension at 520 nm, according to theprocedure reported by Elimadi et al. (2001). The proteincontent was estimated by the dye-binding assay reported byBradford (1976).
2.5. Statistics
All the results are presented as the mean±S.E.M. The overallsignificance of the experimental results was examined by two-way analysis of variance. The differences between the groupswere considered significant at Pb0.05 with the appropriateBonferroni correction made for multiple comparisons.
3. Results
3.1. Bile output and portal pressure
The bile output measured before cold storage was 2.34±0.33 μl/min/g liver and was constant throughout the 120 min
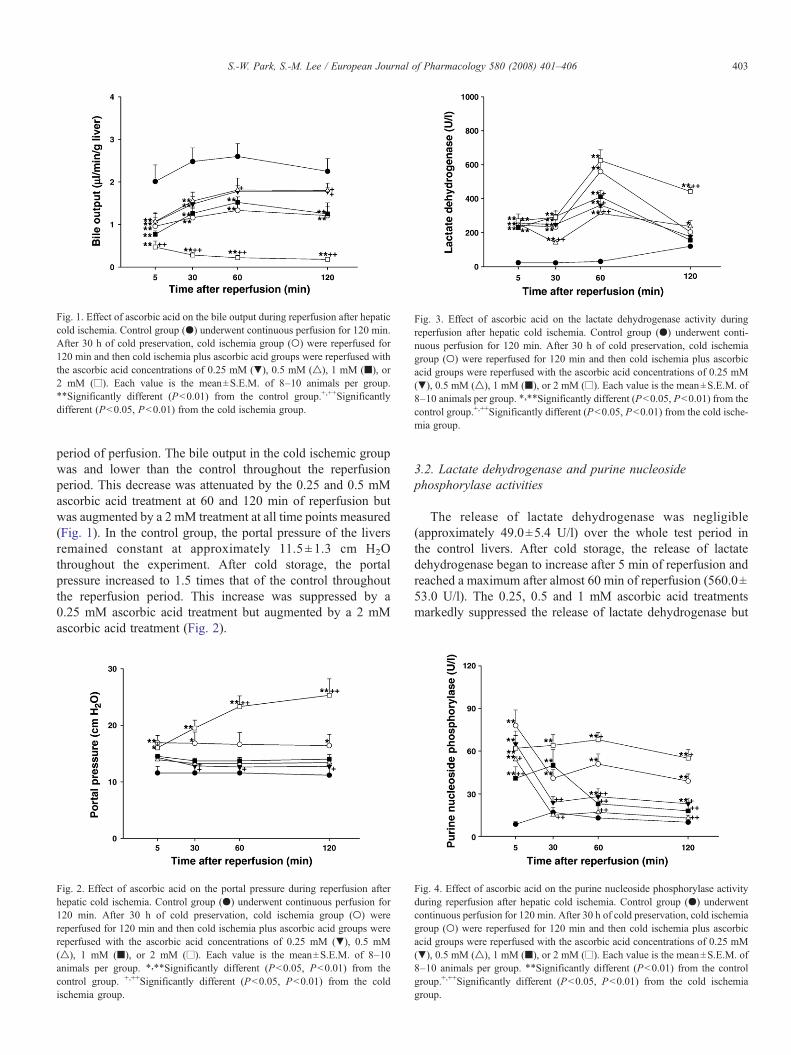
Fig. 1. Effect of ascorbic acid on the bile output during reperfusion after hepaticcold ischemia. Control group (●) underwent continuous perfusion for 120 min.After 30 h of cold preservation, cold ischemia group (○) were reperfused for120 min and then cold ischemia plus ascorbic acid groups were reperfused withthe ascorbic acid concentrations of 0.25 mM (▼), 0.5 mM (△), 1 mM (■), or2 mM (□). Each value is the mean±S.E.M. of 8–10 animals per group.⁎⁎Significantly different (Pb0.01) from the control group.+,++Significantlydifferent (Pb0.05, Pb0.01) from the cold ischemia group.
Fig. 3. Effect of ascorbic acid on the lactate dehydrogenase activity duringreperfusion after hepatic cold ischemia. Control group (●) underwent conti-nuous perfusion for 120 min. After 30 h of cold preservation, cold ischemiagroup (○) were reperfused for 120 min and then cold ischemia plus ascorbicacid groups were reperfused with the ascorbic acid concentrations of 0.25 mM(▼), 0.5 mM (△), 1 mM (■), or 2 mM (□). Each value is the mean±S.E.M. of8–10 animals per group. ⁎,⁎⁎Significantly different (Pb0.05, Pb0.01) from thecontrol group.+,++Significantly different (Pb0.05, Pb0.01) from the cold ische-mia group.
403S.-W. Park, S.-M. Lee / European Journal of Pharmacology 580 (2008) 401–406
period of perfusion. The bile output in the cold ischemic groupwas and lower than the control throughout the reperfusionperiod. This decrease was attenuated by the 0.25 and 0.5 mMascorbic acid treatment at 60 and 120 min of reperfusion butwas augmented by a 2 mM treatment at all time points measured(Fig. 1). In the control group, the portal pressure of the liversremained constant at approximately 11.5 ±1.3 cm H2Othroughout the experiment. After cold storage, the portalpressure increased to 1.5 times that of the control throughoutthe reperfusion period. This increase was suppressed by a0.25 mM ascorbic acid treatment but augmented by a 2 mMascorbic acid treatment (Fig. 2).
Fig. 2. Effect of ascorbic acid on the portal pressure during reperfusion afterhepatic cold ischemia. Control group (●) underwent continuous perfusion for120 min. After 30 h of cold preservation, cold ischemia group (○) werereperfused for 120 min and then cold ischemia plus ascorbic acid groups werereperfused with the ascorbic acid concentrations of 0.25 mM (▼), 0.5 mM(△), 1 mM (■), or 2 mM (□). Each value is the mean±S.E.M. of 8–10animals per group. ⁎,⁎⁎Significantly different (Pb0.05, Pb0.01) from thecontrol group. +,++Significantly different (Pb0.05, Pb0.01) from the coldischemia group.
3.2. Lactate dehydrogenase and purine nucleosidephosphorylase activities
The release of lactate dehydrogenase was negligible(approximately 49.0±5.4 U/l) over the whole test period inthe control livers. After cold storage, the release of lactatedehydrogenase began to increase after 5 min of reperfusion andreached a maximum after almost 60 min of reperfusion (560.0±53.0 U/l). The 0.25, 0.5 and 1 mM ascorbic acid treatmentsmarkedly suppressed the release of lactate dehydrogenase but
Fig. 4. Effect of ascorbic acid on the purine nucleoside phosphorylase activityduring reperfusion after hepatic cold ischemia. Control group (●) underwentcontinuous perfusion for 120 min. After 30 h of cold preservation, cold ischemiagroup (○) were reperfused for 120 min and then cold ischemia plus ascorbicacid groups were reperfused with the ascorbic acid concentrations of 0.25 mM(▼), 0.5 mM (△), 1 mM (■), or 2 mM (□). Each value is the mean±S.E.M. of8–10 animals per group. ⁎⁎Significantly different (Pb0.01) from the controlgroup.+,++Significantly different (Pb0.05, Pb0.01) from the cold ischemiagroup.
404 S.-W. Park, S.-M. Lee / European Journal of Pharmacology 580 (2008) 401–406
these significant increases were augmented by the 2 mMascorbic acid treatment (Fig. 3). As shown in Fig. 4, the purinenucleoside phosphorylase level in the perfusate was low (12.2±2.7 U/l) and at a constant level. In the cold ischemic livers thepurine nucleoside phosphorylase levels peaked after 5 min ofreperfusion, remained high during the 120 min of reperfusionperiod. This increase was attenuated by a treatment with 0.25,0.5 and 1 mM ascorbic acid. In contrast, 2 mM ascorbic acidaugmented the increases that occurred after 60 and 120 min ofreperfusion in the cold ischemic livers.
3.3. Glutathione efflux
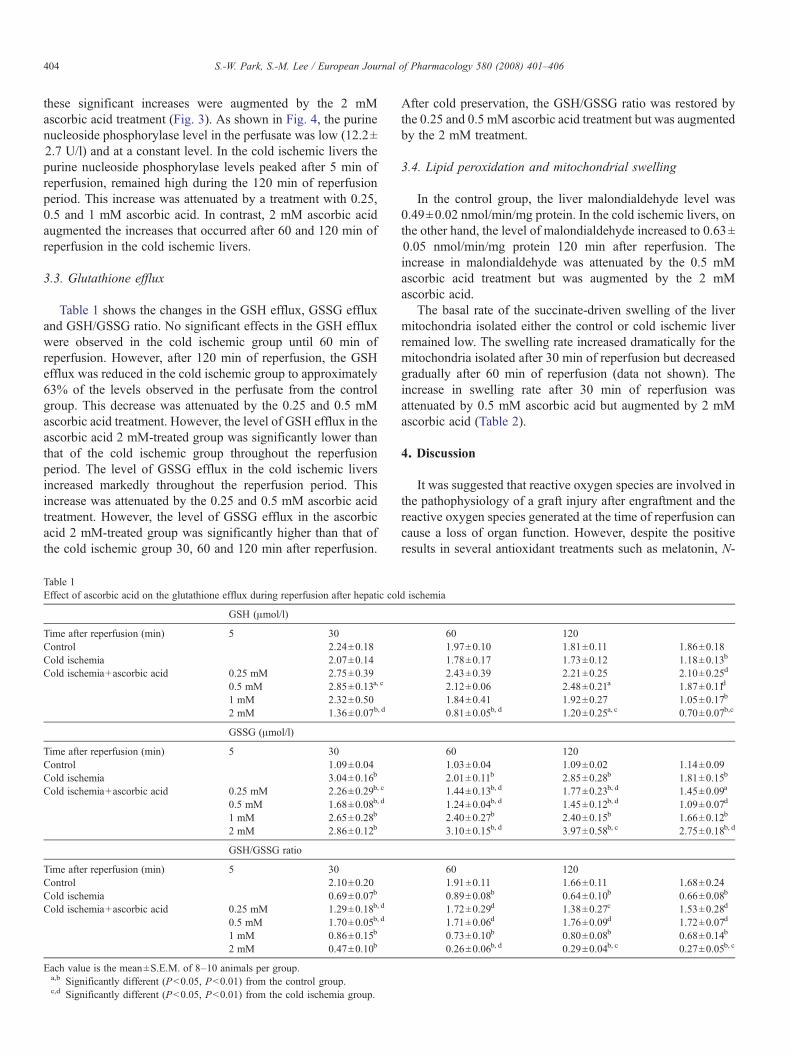
Table 1 shows the changes in the GSH efflux, GSSG effluxand GSH/GSSG ratio. No significant effects in the GSH effluxwere observed in the cold ischemic group until 60 min ofreperfusion. However, after 120 min of reperfusion, the GSHefflux was reduced in the cold ischemic group to approximately63% of the levels observed in the perfusate from the controlgroup. This decrease was attenuated by the 0.25 and 0.5 mMascorbic acid treatment. However, the level of GSH efflux in theascorbic acid 2 mM-treated group was significantly lower thanthat of the cold ischemic group throughout the reperfusionperiod. The level of GSSG efflux in the cold ischemic liversincreased markedly throughout the reperfusion period. Thisincrease was attenuated by the 0.25 and 0.5 mM ascorbic acidtreatment. However, the level of GSSG efflux in the ascorbicacid 2 mM-treated group was significantly higher than that ofthe cold ischemic group 30, 60 and 120 min after reperfusion.
Table 1Effect of ascorbic acid on the glutathione efflux during reperfusion after hepatic col
GSH (μmol/l)
Time after reperfusion (min) 5 30Control 2.24±0.18Cold ischemia 2.07±0.14Cold ischemia+ascorbic acid 0.25 mM 2.75±0.39
0.5 mM 2.85±0.13a, c
1 mM 2.32±0.502 mM 1.36±0.07b, d
GSSG (μmol/l)
Time after reperfusion (min) 5 30Control 1.09±0.04Cold ischemia 3.04±0.16b
Cold ischemia+ascorbic acid 0.25 mM 2.26±0.29b, c
0.5 mM 1.68±0.08b, d
1 mM 2.65±0.28b
2 mM 2.86±0.12b
GSH/GSSG ratio
Time after reperfusion (min) 5 30Control 2.10±0.20Cold ischemia 0.69±0.07b
Cold ischemia+ascorbic acid 0.25 mM 1.29±0.18b, d
0.5 mM 1.70±0.05b, d
1 mM 0.86±0.15b
2 mM 0.47±0.10b
Each value is the mean±S.E.M. of 8–10 animals per group.a,b Significantly different (Pb0.05, Pb0.01) from the control group.c,d Significantly different (Pb0.05, Pb0.01) from the cold ischemia group.
After cold preservation, the GSH/GSSG ratio was restored bythe 0.25 and 0.5 mM ascorbic acid treatment but was augmentedby the 2 mM treatment.
3.4. Lipid peroxidation and mitochondrial swelling
In the control group, the liver malondialdehyde level was0.49±0.02 nmol/min/mg protein. In the cold ischemic livers, onthe other hand, the level of malondialdehyde increased to 0.63±0.05 nmol/min/mg protein 120 min after reperfusion. Theincrease in malondialdehyde was attenuated by the 0.5 mMascorbic acid treatment but was augmented by the 2 mMascorbic acid.
The basal rate of the succinate-driven swelling of the livermitochondria isolated either the control or cold ischemic liverremained low. The swelling rate increased dramatically for themitochondria isolated after 30 min of reperfusion but decreasedgradually after 60 min of reperfusion (data not shown). Theincrease in swelling rate after 30 min of reperfusion wasattenuated by 0.5 mM ascorbic acid but augmented by 2 mMascorbic acid (Table 2).
4. Discussion
It was suggested that reactive oxygen species are involved inthe pathophysiology of a graft injury after engraftment and thereactive oxygen species generated at the time of reperfusion cancause a loss of organ function. However, despite the positiveresults in several antioxidant treatments such as melatonin, N-
d ischemia
60 1201.97±0.10 1.81±0.11 1.86±0.181.78±0.17 1.73±0.12 1.18±0.13b
2.43±0.39 2.21±0.25 2.10±0.25d
2.12±0.06 2.48±0.21a 1.87±0.11d
1.84±0.41 1.92±0.27 1.05±0.17b
0.81±0.05b, d 1.20±0.25a, c 0.70±0.07b,c
60 1201.03±0.04 1.09±0.02 1.14±0.092.01±0.11b 2.85±0.28b 1.81±0.15b
1.44±0.13b, d 1.77±0.23b, d 1.45±0.09a
1.24±0.04b, d 1.45±0.12b, d 1.09±0.07d
2.40±0.27b 2.40±0.15b 1.66±0.12b
3.10±0.15b, d 3.97±0.58b, c 2.75±0.18b, d
60 1201.91±0.11 1.66±0.11 1.68±0.240.89±0.08b 0.64±0.10b 0.66±0.08b
1.72±0.29d 1.38±0.27c 1.53±0.28d
1.71±0.06d 1.76±0.09d 1.72±0.07d
0.73±0.10b 0.80±0.08b 0.68±0.14b
0.26±0.06b, d 0.29±0.04b, c 0.27±0.05b, c

Table 2Effect of ascorbic acid on the lipid peroxidation and mitochondrial permeabilitytransition during reperfusion after hepatic cold ischemia
Malondialdehyde(nmol/min/mgprotein)
Mitochondrial swelling(ΔA×10−2/min/mgprotein)
Control 0.49±0.02 0.0017±0.0003Cold ischemia 0.63±0.05a 0.0229±0.0015b
Cold ischemia+ascorbic acid 0.25 mM 0.54±0.07 0.0180±0.0021a
0.5 mM 0.49±0.03c 0.0158±0.0015a, c
1 mM 0.58±0.05 0.0229±0.0019b
2 mM 0.73±0.03b, c 0.0431±0.0042b, d
Each value is the mean±S.E.M. of 8–10 animals per group.a,b Significantly different (Pb0.05, Pb0.01) from the control group.c,d Significantly different (Pb0.05, Pb0.01) from the cold ischemia group.
405S.-W. Park, S.-M. Lee / European Journal of Pharmacology 580 (2008) 401–406
acetylcysteine and glutathione, the poor graft function hasnecessitated further study (Vairetti et al., 2005).
Ascorbic acid is a major antioxidant that reduces theoxidative indices after ischemia/reperfusion. The ischemia/reperfusion phenomena are associated with the depletion ofascorbic acid in plasma (Taha et al., 2004). Indeed, recentstudies have suggested that ascorbic acid 2-glucoside, whichis a chemically stable ascorbic acid derivative, contributes tothe improvement in survival by preventing sinusoidalendothelial cell apoptosis in preserved grafts (Matsukawa etal., 2000). In contrast to the antioxidant properties of ascorbicacid, ascorbic acid has also been shown to oxidize the cellularcomponents under certain in vitro experimental conditionsand induce cell death in a number of different cell lines(Sakagami and Satoh, 1997) but the mechanism is not wellunderstood.
The sinusoidal endothelium is particularly susceptible toischemic damage, even under cold storage and the free radicalinjury presumably occurs within the extracellular matrix whenthe endothelium is altered (Jaeschke, 1991). The pathologicaldamage or death of the endothelium may subsequently lead tochanges in the endothelial or stellate cell contractility, which canresult in significant changes in hepatic hemodynamics. Theportal pressure is an indicator of the hepatic microcirculation,and a high portal pressure is of clinical relevance as an indicatorof the severity of endstorage hepatic diseases before transplan-tation as well as in patients suffering from acute liver rejection(Hadengue et al., 1993). In this study, reperfusion followingcold preservation resulted in significant injury to themicrovascular endothelial cell, as reflected by the elevatedlevels of purine nucleoside phosphorylase. The portal pres-sure increased dramatically after cold storage and was sus-tained for 120 min, indicating prolonged deterioration of thehepatic circulation. The improvement in the hepatic hemo-dynamics was only shown in the livers treated with lowascorbic acid concentrations (0.25 and 0.5 mM). The highconcentrations (2 mM) used in these experiments exacerbatedthe cold ischemia/reperfusion-induced changes in the hepatichemodynamics.
There is accumulating evidence suggesting that microcircu-latory disturbances are responsible for the poor hepatocyte
function during graft reperfusion (Koeppel et al., 1996). A lowascorbic acid concentration has a protective effect against hepa-tocellular injury because the activity of lactate dehydrogenasereleased into the perfusate sample was significantly lower in theascorbic acid group than in the control group. The significantlyincreased bile production in the low ascorbic acid concentrationgroup indicates that the ascorbic acid treatment improved thehepatocellular integrity, because bile production has been usedas a reliable and accurate measure of the hepatocellular integrityand correlates well with the hepatocellular ATP content duringboth preservation of the donor liver and experimental liverperfusion (Kamiike et al., 1985). The high ascorbic acid con-centration further decreased the level of biliary secretion aftercold storage.
Accumulating evidences indicate that reactive oxygenspecies play a major role in cell damage associated with thereperfusion of ischemic tissues. Reactive oxygen species attackon biological membrane can lead to the oxidative destructionof the membrane polyunsaturated fatty acids by lipidperoxidation. It has been shown that the levels of lipidperoxidation products are lowered when GSH is added toorgan storage fluids (Bryan et al., 1994). In cold ischemiclivers, hepatic lipid peroxidation significantly increased120 min after reperfusion. The hepatic GSH efflux was notchanged until 60 min after reperfusion but was only decreased120 min after reperfusion. However, a large increase in theefflux of GSSG from the liver was observed after the beginningof reperfusion. This is consistent with previous reportsshowing that the biliary and sinusoidal export of GSSG is awell established and sensitive indicator of oxidative stress in anisolated perfused rat liver (Jaeschke et al., 1988). Therefore,these results suggest that reactive oxygen species, whenproduced in cold ischemic livers, can cause direct cell damagethough thiol oxidation and subsequent lipid peroxidation.Interestingly, a treatment with low ascorbic acid concentrationspreserved the endothelial GSH/GSSG redox status andattenuated lipid peroxidation, which suggests that low ascorbicacid concentrations have an antioxidant effect by scavengingradicals. However, a high concentration aggravated the coldischemia/reperfusion-induced GSSG efflux and lipid peroxida-tion. This means that at low ascorbic acid concentrations, eachascorbic acid molecule can trap two peroxyl radicals. However,at high concentrations, the number of radicals trapped perascorbic acid approaches zero. This behavior is explained bythe susceptibility of ascorbic acid to undergo peroxyl radical-catalyzed autoxidative destruction (Wayner et al., 1986).Therefore, the GSH efflux decreased by high ascorbic acidconcentrations is believed to be due to an increase in GSHconsumption by the reduction of dehydroascorbate toascorbate.
Many studies have associated a mitochondrial dysfunctioncaused by reactive oxygen species with both necrotic andapoptotic cell death (Eum et al., 2007). The mitochondria arealso the main source of intracellular reactive oxygen speciesproduction, which when overproduced, damage to themitochondrial membranes and proteins through lipid perox-idation. These lipid peroxidation damages can increase the

406 S.-W. Park, S.-M. Lee / European Journal of Pharmacology 580 (2008) 401–406
permeability of the mitochondrial membrane, ultimatelyleading to a loss of mitochondrial integrity. As a biochemicalmarker for mitochondrial damage, this study measured theinitial rate of mitochondrial swelling, which is an indicator ofan increase in mitochondrial permeability transition poreopening. The results show that the rate of mitochondrialswelling driven by succinate addition increased dramaticallyin the mitochondria isolated from the liver at 30 min intoreperfusion. The spontaneous swelling of the mitochondriasubjected to cold ischemia/reperfusion was inhibited by lowascorbic acid concentration but was amplified by highascorbic acid concentrations. This indicates that mitochondrialpermeability transition opening during cold ischemia/reperfu-sion might be related to the production of reactive oxygenspecies.
In conclusion, these results suggest that oxidative stress byreactive oxygen species is a direct cause of both parenchymaland nonparenchymal cell injury during hepatic cold ischemia/reperfusion, and treating the cold-preserved livers with lowconcentrations of ascorbic acid upon reperfusion might preventthe damage to the hepatocytes and the deterioration in thehepatic microcirculation. However, high ascorbic acid concen-trations might act as a prooxidant due to its autooxidizing pro-perties. The precise cellular mechanisms involved will requirefurther study. In this respect, ascorbic acid appears to be apromising candidate for the prevention of reperfusion injury to aliver allograft but the prooxidant effect at high ascorbic acidconcentrations should be avoided.
Acknowledgements
“This work was supported by the Korea Research Founda-tion Grant funded by the Korean Government (MOEHRD)”(KRF-2006-521-E00023). We gratefully acknowledge the JeilPharmaceutical Company of Korea for donating the Universityof Wisconsin solution.
References
Arai, M., Thurman, R.G., Lemasters, J.J., 2001. Ischemic preconditioning of ratlivers against cold storage-reperfusion injury: role of nonparenchymal cellsand the phenomenon of heterologous preconditioning. Liver Transpl. 7,292–299.
Bailey, S.M., Reinke, L.A., 2000. Effect of low flow ischemia–reperfusioninjury on liver function. Life Sci. 66, 1033–1044.
Bradford, M.M., 1976. A rapid and sensitive method for the quantitation ofmicrogram quantities of protein utilizing the principle of protein-dye bind-ing. Anal. Biochem. 72, 248–254.
Brehe, J.E., Burch, H.B., 1976. Enzymatic assay for glutathione. Anal.Biochem. 74, 189–197.
Bryan, C.L., Patefield, A.J., Cohen, D., Nielsen, J.L., Emanuel, B., Calhoon,J.H., 1994. Assessment of injury in transplanted and nontransplanted lungsafter 6 h of cold storage with glutathione. J. Appl. Physiol. 76,1232–1241.
Buege, J.A., Aust, S.D., 1978. Microsomal lipid peroxidation. MethodsEnzymol. 52, 302–310.
Charrueau, C.A., Carayon, A., Thurman, R.G., 2002. Long-term cold liverstorage induces endothelin-1 release and a time-dependent increase in portalpressure at reperfusion in the rat. J. Gastroenterol. 37, 717–725.
De Tata, V., Brizzi, S., Saviozzi, M., Lazzarotti, A., Fierabracci, V., Malvaldi,G., Casini, A., 2005. Protective role of dehydroascorbate in rat liverischemia–reperfusion injury. J. Surg. Res. 123, 215–221.
Deschenes, M., Belle, S.H., Krom, R.A., Zetterman, R.K., Lake, J.R., 1998.Early allograft dysfunction after liver transplantation: a definition andpredictors of outcome. National institute of diabetes and digestive andkidney diseases liver transplantation database. Transplantation 66, 302–310.
Elimadi, A., Sapena, R., Settaf, A., Le Louet, H., Tillement, J., Morin, D., 2001.Attenuation of liver normothermic ischemia–reperfusion injury by pre-servation of mitochondrial functions with S-15176, a potent trimetazidinederivative. Biochem. Pharmacol. 62, 509–516.
Eum, H.A., Cha, Y.N., Lee, S.M., 2007. Necrosis and apoptosis: sequence ofliver damage following reperfusion after 60 min ischemia in rats. Biochem.Biophys. Res. Commun. 358, 500–505.
Hadengue, A., Lebrec, D., Moreau, R., Sogni, P., Durand, F., Gaudin, C.,Bernuau, J., Belghiti, J., Gayet, B., Erlinger, S., et al., 1993. Persistence ofsystemic and splanchnic hyperkinetic circulation in liver transplant patients.Hepatology 17, 175–178.
Hoffee, P.A., May, R., Robertson, B.D., 1978. In: Hoffee, P., Jones, M.A.(Eds.), Purine nucleoside phosphorylase from Salmonella typhimurium andrat liver. Method in enzymology, vol. 51. Academic press, New York, NY,pp. 517–524.
Jaeschke, H., 1991. Reactive oxygen and ischemia/reperfusion injury of theliver. Chem. Biol. Interact. 79, 115–136.
Jaeschke, H., Farhood, A., 1991. Neutrophil and Kupffer cell-induced oxidantstress and ischemia-reperfusion injury in rat liver. Am. J. Physiol. 260,G355–G362.
Jaeschke, H., Smith, C.V., Mitchell, J.R., 1988. Reactive oxygen species duringischemia-reflow injury in isolated perfused rat liver. J. Clin. Invest. 81,1240–1246.
Johnson, D., Lardy, H., 1967. Isolation of liver and kidney mitochondria.Methods Enzymol. 10, 456–470.
Kamiike, K., Nakahara, M., Nakao, K., Koseki, M., Nishida, T., Kawashima, Y.,Watanabe, F., Tagawa, K., 1985. Correlation between cellular ATP level andbile excretion in the rat liver. Transplantation 39, 50–55.
Koeppel, T.A., Lehmann, T.G., Thies, J.C., Gehrcke, R., Gebhard, M.M.,Herfarth, C., Otto, G., Post, S., 1996. Impact of N-acetylcysteine on thehepatic microcirculation after orthotopic liver transplantation. Transplanta-tion 61, 1397–1402.
Matsukawa, H., Yagi, T., Matsuda, H., Kawahara, H., Yamamoto, I., Matsuoka,J., Tanaka, N., 2000. Ascorbic acid 2-glucoside prevents sinusoidalendothelial cell apoptosis in supercooled preserved grafts in rat livertransplantation. Transplant. Proc. 32, 313–317.
Prat, A.G., Turrens, J.F., 1990. Ascorbate-and hemoglobin-dependent brainchemiluminescence. Free Radic. Biol. Med. 8, 319–325.
Sakagami, H., Satoh, K., 1997. Modulating factors of radical intensity andcytotoxic activity of ascorbate. Anticancer Res. 17, 3513–3520.
Seo, M.Y., Lee, S.M., 2002. Protective effect of low dose of ascorbic acid onhepatobiliary function in hepatic ischemia/reperfusion in rats. J. Hepatol. 36,72–77.
Taha, M.O., Souza, H.S., Carvalho, C.A., Faqundes, D.J., Simoes, M.J.,Novo, N.F., Caricati-Neto, A., 2004. Cytoprotective effects of ascorbicacid on the ischemia–reperfusion injury of rat liver. Transplant. Proc. 36,296–300.
Vairetti, M., Ferrigno, A., Bertone, R., Rizzo, V., Richelmi, P., Berte, F., Reiter,R.J., Freitas, I., 2005. Exogenous melatonin enhances bile flow and ATPlevels after cold storage and reperfusion in rat liver: implications for livertransplantation. J. Pineal Res. 38, 223–230.
Wayner, D.D., Burton, G.W., Ingold, K.U., 1986. The antioxidant efficiency ofvitamin C is concentration-dependent. Biochim. Biophys. Acta 884,119–123.
Wu, T.W., Hashimoto, N., Au, J.X., Wu, J., Mickle, D.A., Carey, D., 1991.Trolox protects rat hepatocytes against oxyradical damage and the ischemicrat liver from reperfusion injury. Hepatology 13, 575–580.
Younes, M., Kayser, E., Strubelt, O., 1992. Effect of antioxidants on hypoxia/reoxygenation-induced injury in isolated perfused rat liver. Pharmacol.Toxicol. 71, 278–283.