Anthony N. DeMaria Judith and Jack White Chair in Cardiology Founding Director, Sulpizio...
64
Anthony N. DeMaria Judith and Jack White Chair in Cardiology Founding Director, Sulpizio Cardiovascular Center UCSD School of Medicine
-
Upload
kayleigh-cullimore -
Category
Documents
-
view
216 -
download
2
Transcript of Anthony N. DeMaria Judith and Jack White Chair in Cardiology Founding Director, Sulpizio...
Anthony N. DeMariaAnthony N. DeMaria
Judith and Jack White Chair in CardiologyFounding Director, Sulpizio Cardiovascular
CenterUCSD School of Medicine
Judith and Jack White Chair in CardiologyFounding Director, Sulpizio Cardiovascular
CenterUCSD School of Medicine

(Adapted from Glagov et al.)
Coronary RemodelingCoronary Remodeling
Normalvessel
MinimalCAD
Progression
Compensatory expansionmaintains constant lumen
Expansion overcome:
lumen narrows
SevereCAD
ModerateCAD
Glagov et al, N Engl J Med, 1987.
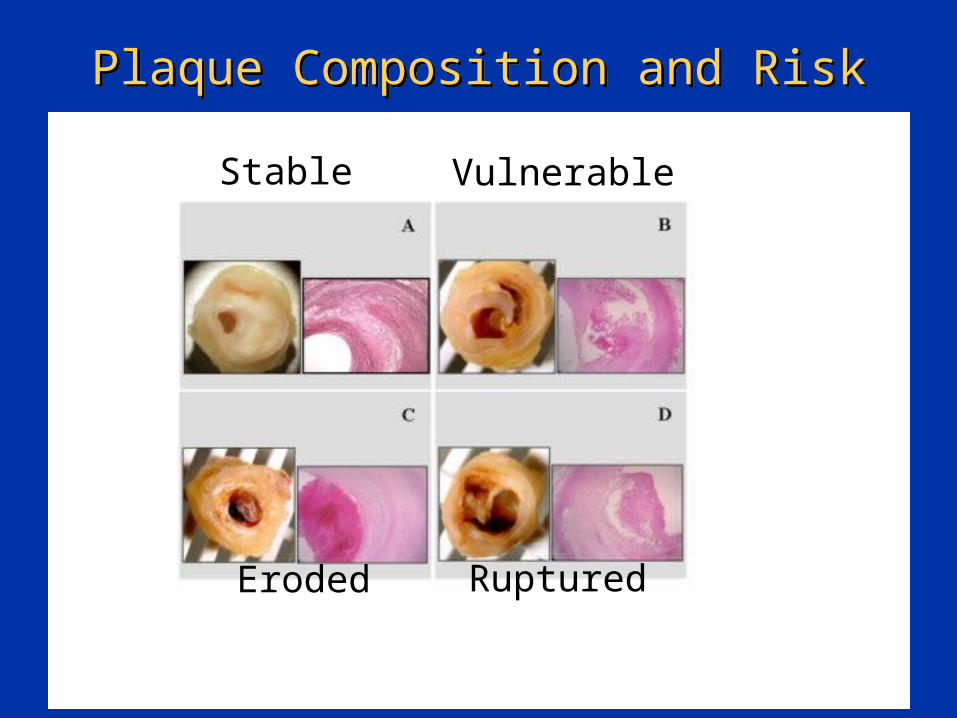
Plaque Composition and RiskPlaque Composition and Risk
Stable Vulnerable
Eroded Ruptured
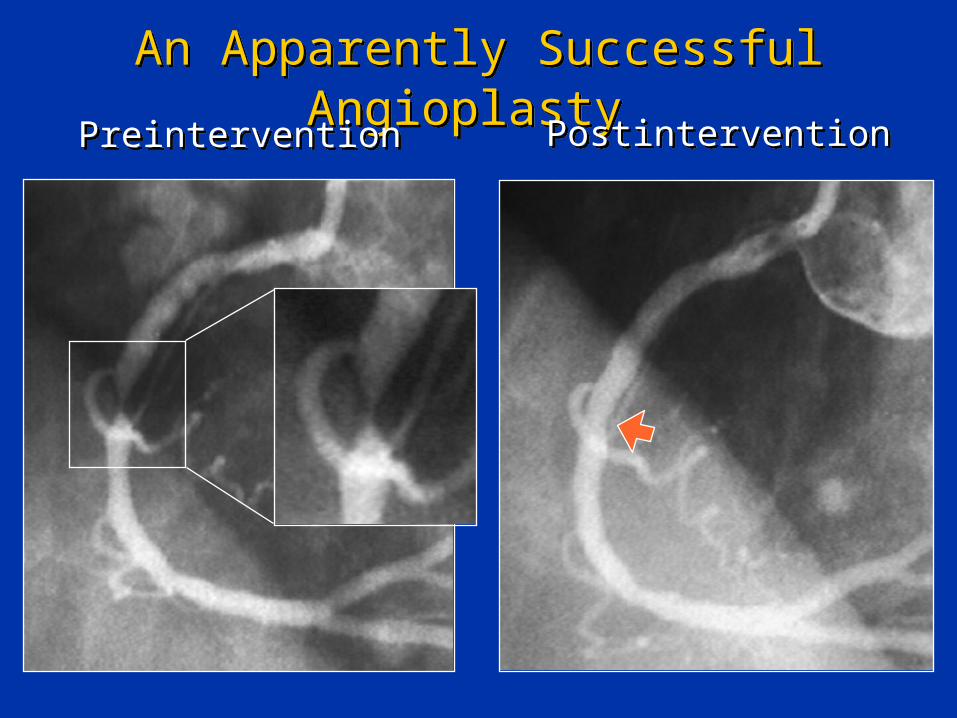
An Apparently Successful Angioplasty An Apparently Successful Angioplasty
PreinterventionPreintervention PostinterventionPostintervention
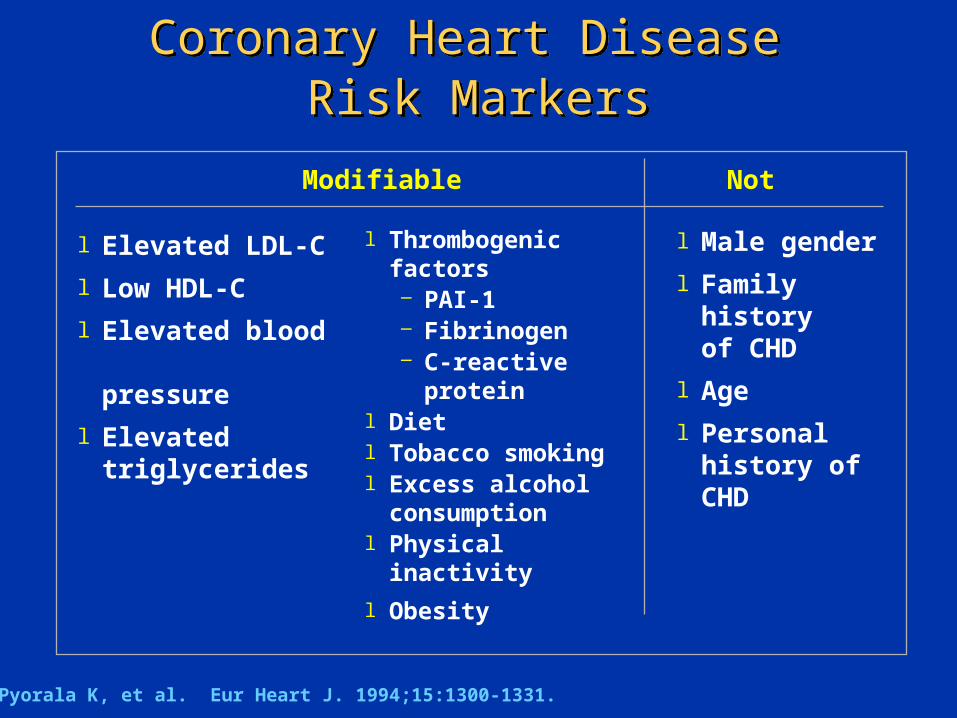
Coronary Heart Disease Risk Markers
Coronary Heart Disease Risk Markers
Modifiable Not
l Elevated LDL-C
l Low HDL-C
l Elevated blood
pressure
l Elevated triglycerides
Pyorala K, et al. Eur Heart J. 1994;15:1300-1331.
l Male gender
l Family history of CHD
l Age
l Personal history of CHD
l Thrombogenic factors– PAI-1– Fibrinogen– C-reactive
proteinl Dietl Tobacco smokingl Excess alcohol
consumptionl Physical inactivity
l Obesity
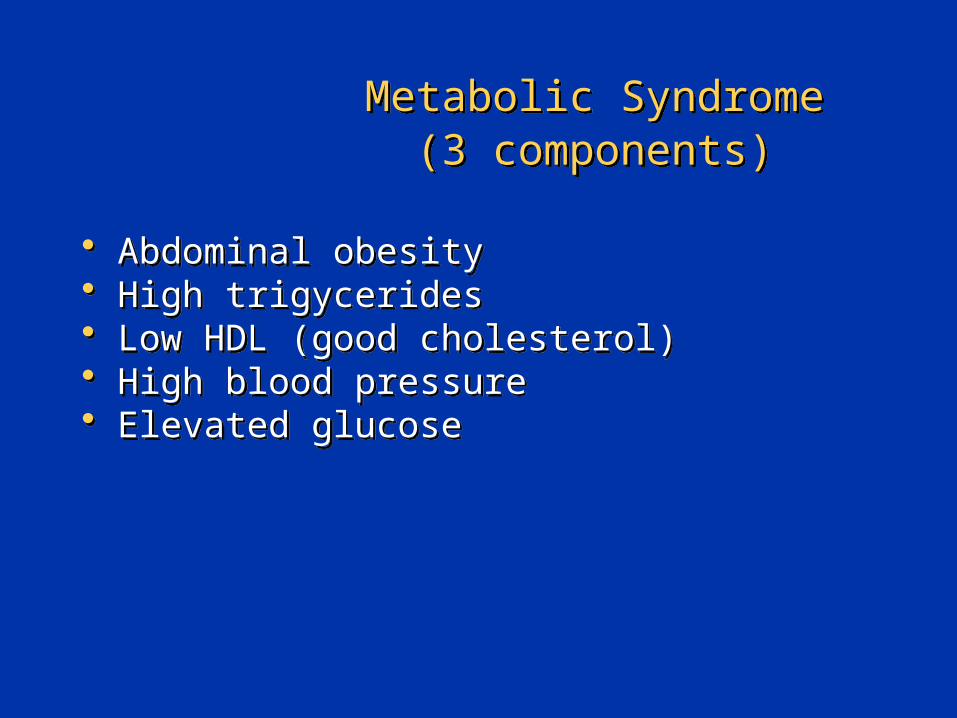
Metabolic Syndrome(3 components)
Metabolic Syndrome(3 components)
• Abdominal obesity• High trigycerides• Low HDL (good cholesterol)• High blood pressure• Elevated glucose
• Abdominal obesity• High trigycerides• Low HDL (good cholesterol)• High blood pressure• Elevated glucose

JAMA 1999;282:16, JAMA 2001;286:10.
Obesity Trends* Among U.S. Adults: BRFSS1985
Obesity Trends* Among U.S. Adults: BRFSS1985
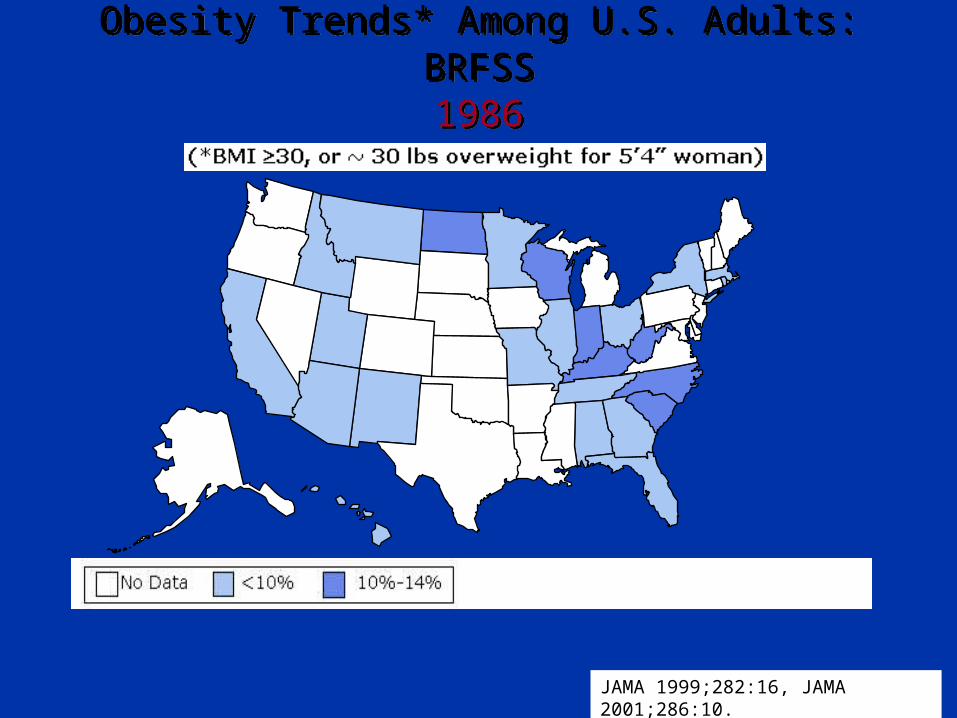
Obesity Trends* Among U.S. Adults: BRFSS1986
Obesity Trends* Among U.S. Adults: BRFSS1986
JAMA 1999;282:16, JAMA 2001;286:10.
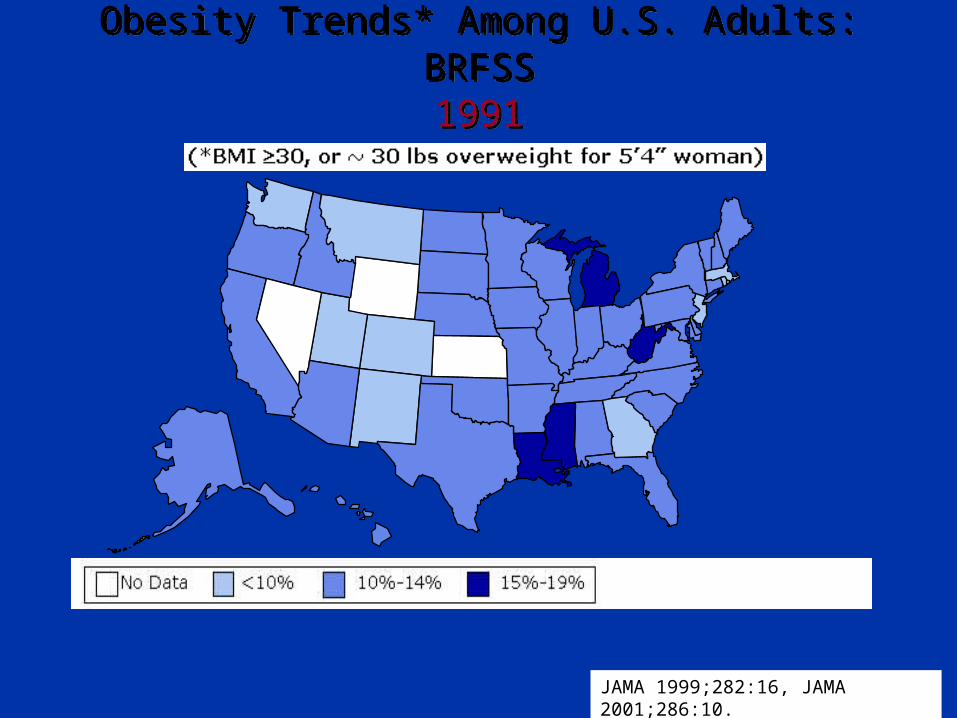
Obesity Trends* Among U.S. Adults: BRFSS1991
Obesity Trends* Among U.S. Adults: BRFSS1991
JAMA 1999;282:16, JAMA 2001;286:10.

Obesity Trends* Among U.S. Adults: BRFSS1995
Obesity Trends* Among U.S. Adults: BRFSS1995
JAMA 1999;282:16, JAMA 2001;286:10.
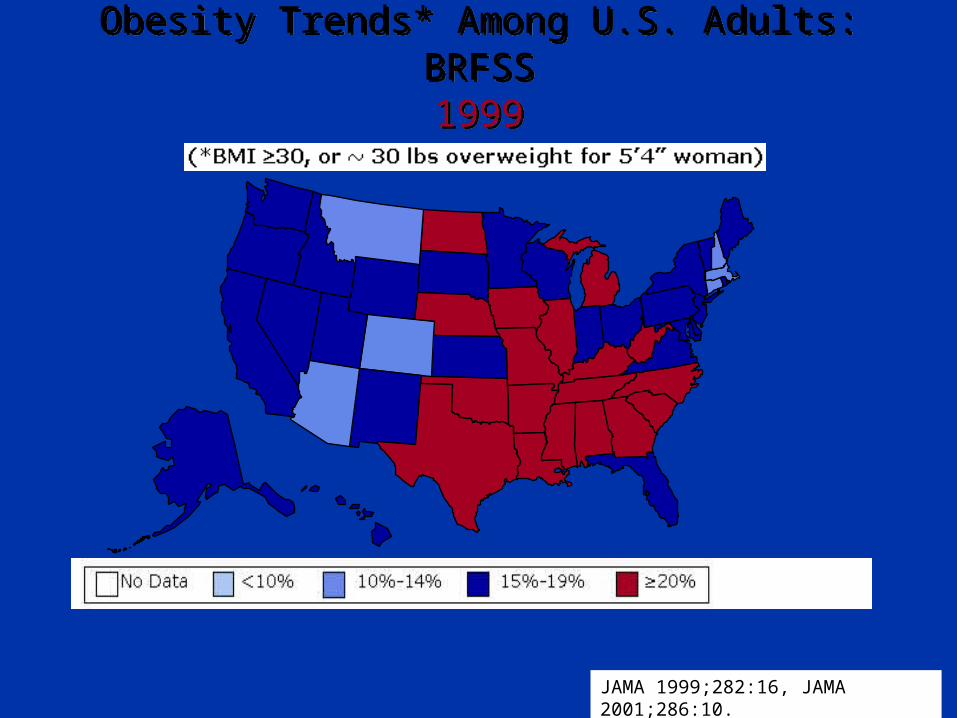
Obesity Trends* Among U.S. Adults: BRFSS1999
Obesity Trends* Among U.S. Adults: BRFSS1999
JAMA 1999;282:16, JAMA 2001;286:10.

Obesity Trends* Among U.S. Adults: BRFSS2001
Obesity Trends* Among U.S. Adults: BRFSS2001
JAMA 1999;282:16, JAMA 2001;286:10.
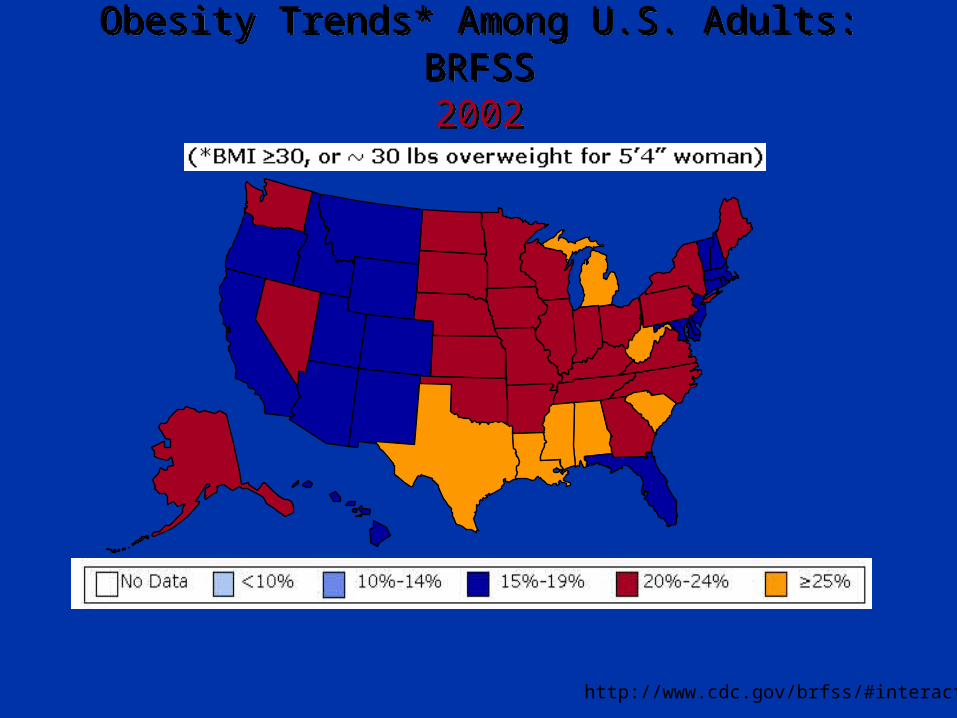
Obesity Trends* Among U.S. Adults: BRFSS2002
Obesity Trends* Among U.S. Adults: BRFSS2002
http://www.cdc.gov/brfss/#interactive
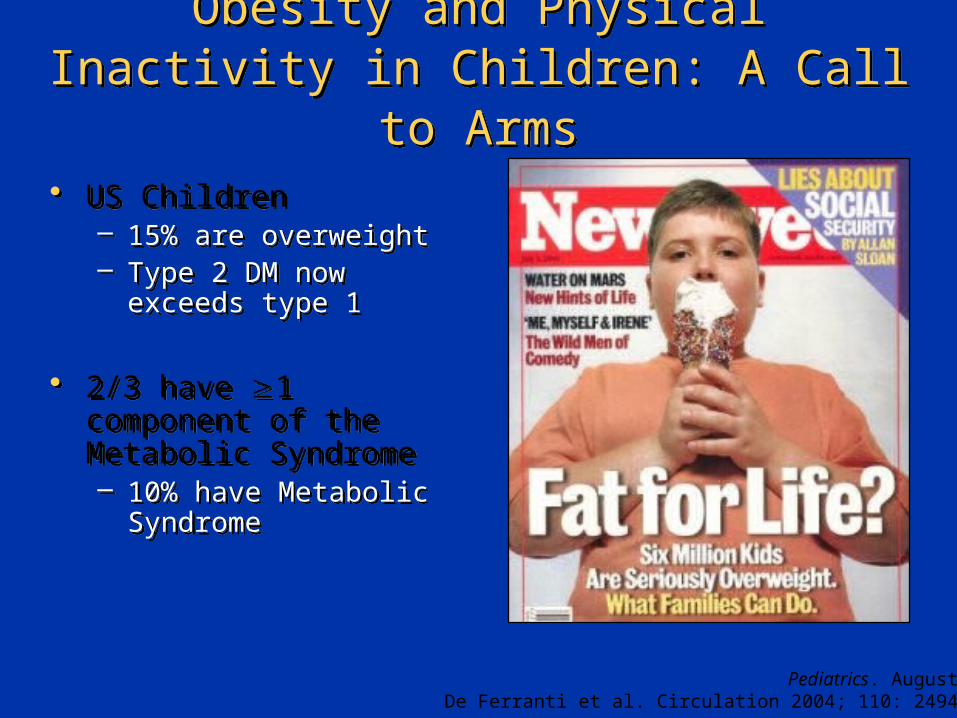
Obesity and Physical Inactivity in Children: A Call to Arms
Obesity and Physical Inactivity in Children: A Call to Arms
• US Children– 15% are overweight– Type 2 DM now exceeds
type 1
• 2/3 have 1 component of the Metabolic Syndrome– 10% have Metabolic
Syndrome
• US Children– 15% are overweight– Type 2 DM now exceeds
type 1
• 2/3 have 1 component of the Metabolic Syndrome– 10% have Metabolic
Syndrome
Pediatrics. August 2003De Ferranti et al. Circulation 2004; 110: 2494-2497

Hardee's "Monster Thickburger2 1/3-pound slabs of Angus beef
4 strips of bacon3 slices of cheese
MayonnaiseButtered sesame seed bun
1420 Calories107 g Fat
Portion DistortionPortion Distortion

Meal and Desert in One: Fried Ice Cream BurgerMeal and Desert in One: Fried Ice Cream Burger

Beware the Fried TwinkieBeware the Fried Twinkie
Deep Fried Butter BallsDeep Fried Butter Balls
Physical inactivity: A call to armsPhysical inactivity: A call to arms
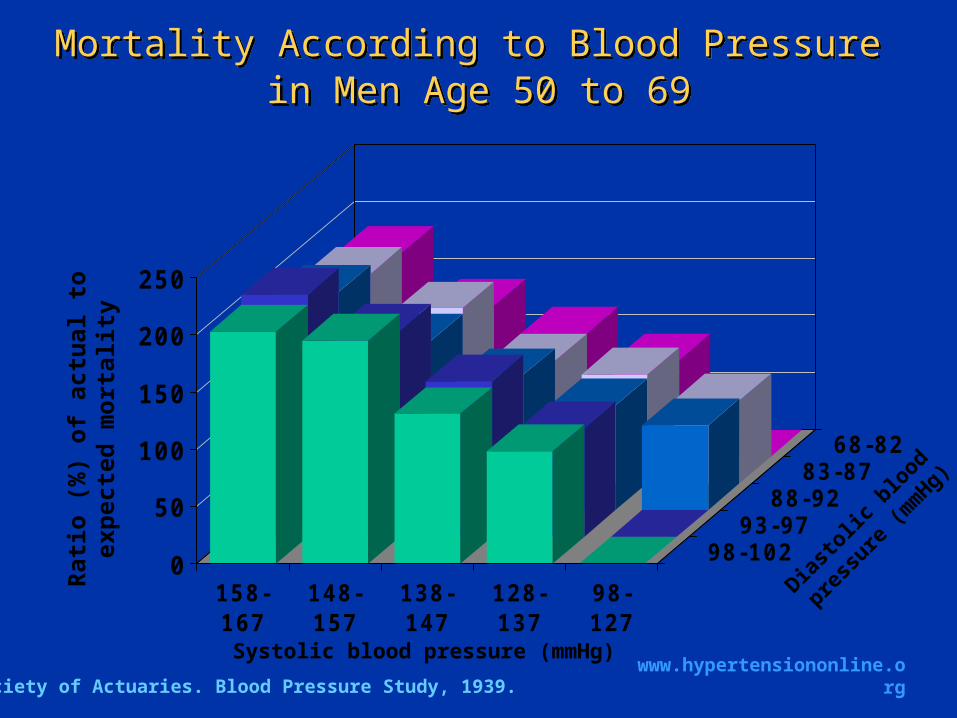
Mortality According to Blood Pressure in Men Age 50 to 69
Mortality According to Blood Pressure in Men Age 50 to 69
0
50
100
150
200
250
158-167
148-157
138-147
128-137
98-127
98-10293-97
88-9283-87
68-82
Society of Actuaries. Blood Pressure Study, 1939.
Rat
io (
%)
of a
ctua
l to
exp
ecte
d
mor
tali
ty
Systolic blood pressure (mmHg)
Diasto
lic b
lood
pressu
re (m
mHg)
www.hypertensiononline.org

0
1
2
3
4
Rel
ativ
e ri
sk o
f C
HD
mor
tali
ty
He J, et at. Am Heart J. 1999;138:211-219.Copyright 1999, Mosby Inc.
<112
<71
Risk of CHD Death According to SBP and DBP in MRFIT
Risk of CHD Death According to SBP and DBP in MRFIT
1 2 3 4 5 6 7 8 9 10Decile
112-
71-
118-
76-
121-
79-
125-
81-
129-
84-
132-
86-
137-
89-
142-
92-
>151
>98
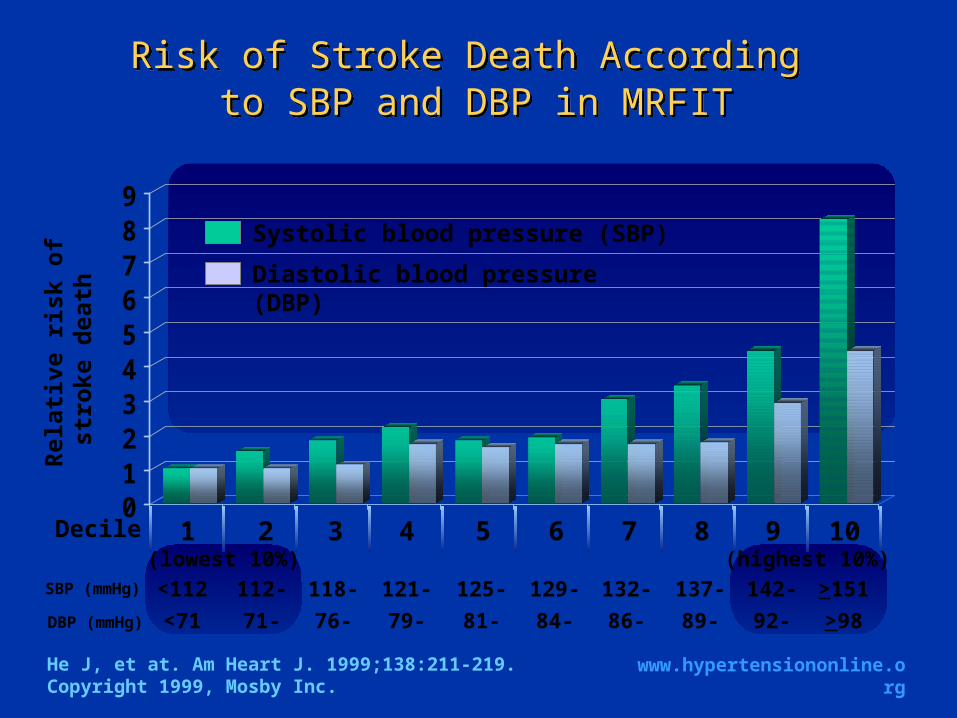
(lowest 10%) (highest 10%)SBP (mmHg)
DBP (mmHg)
Systolic blood pressure (SBP)
Diastolic blood pressure (DBP)
www.hypertensiononline.org
CHD=coronary heart disease
0123456789
Rel
ativ
e ri
sk o
f st
rok
e de
ath
<112
<71
Risk of Stroke Death According to SBP and DBP in MRFIT
Risk of Stroke Death According to SBP and DBP in MRFIT
1 2 3 4 5 6 7 8 9 10Decile
112-
71-
118-
76-
121-
79-
125-
81-
129-
84-
132-
86-
137-
89-
142-
92-
>151
>98
(lowest 10%) (highest 10%)SBP (mmHg)
DBP (mmHg)
www.hypertensiononline.org
Systolic blood pressure (SBP)
Diastolic blood pressure (DBP)
He J, et at. Am Heart J. 1999;138:211-219.Copyright 1999, Mosby Inc.
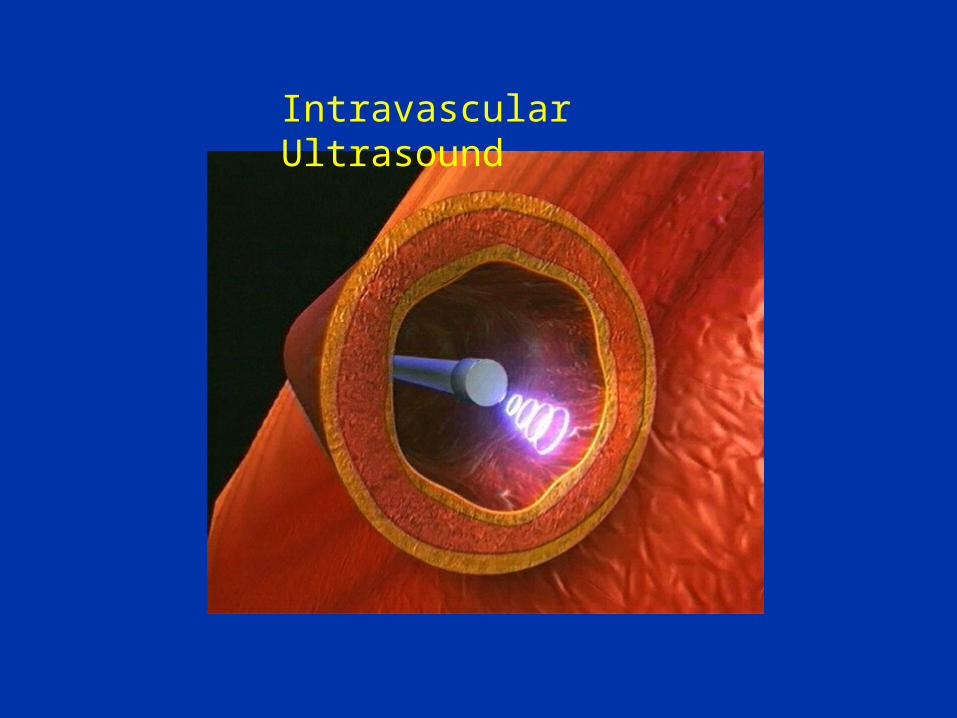
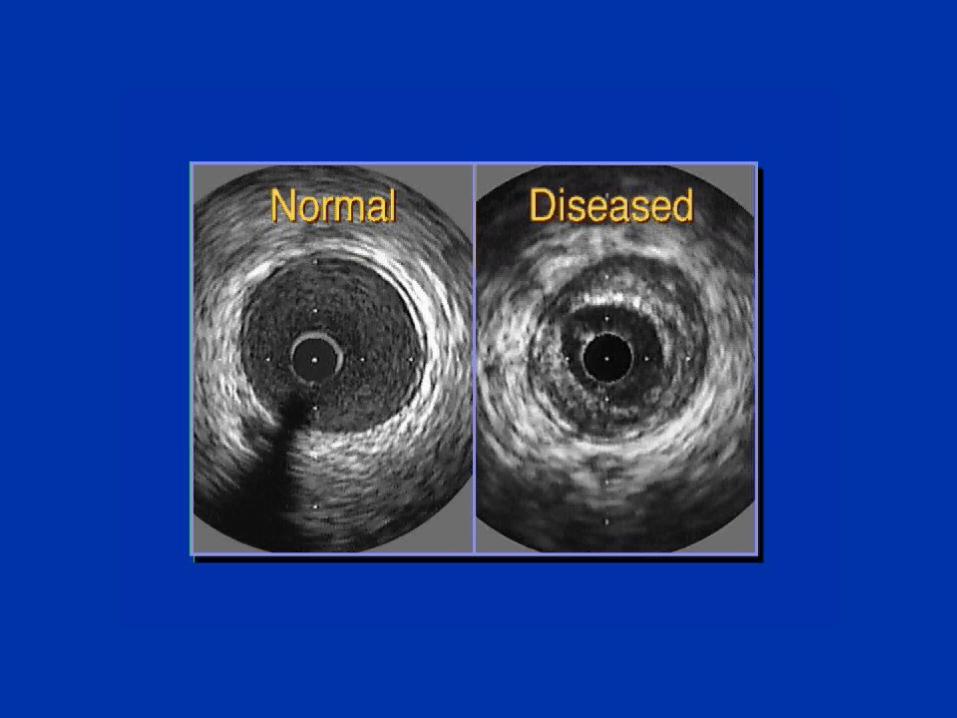
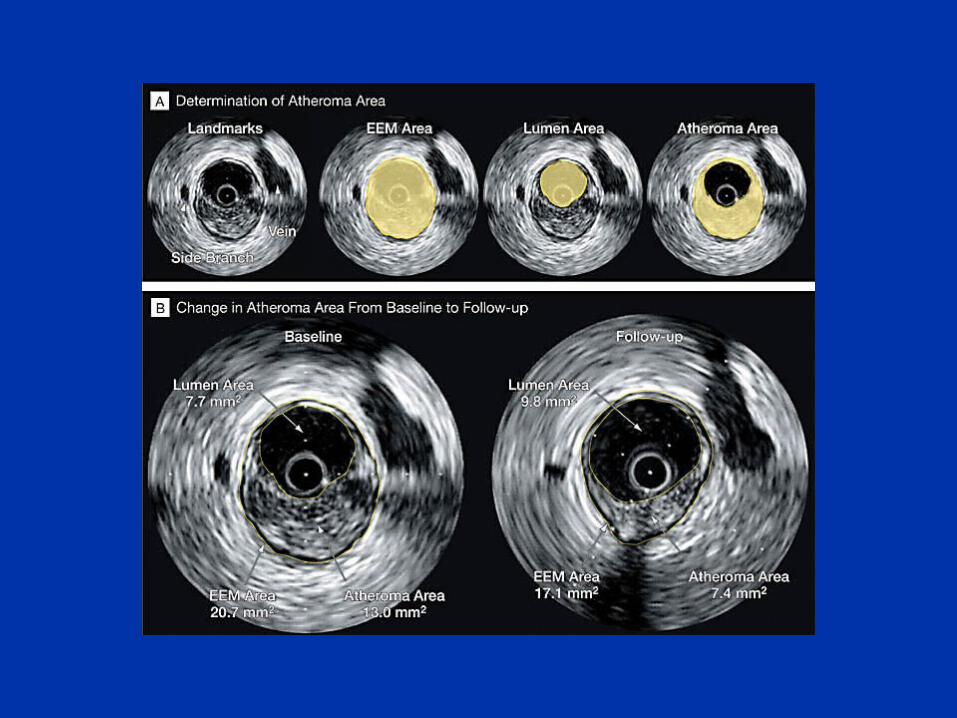
Intravascular Ultrasound
JAMA. 2004;291:1071-1080.
Effect of Intensive Compared With Moderate Lipid-Lowering Therapy on Progression of Coronary Atherosclerosis; A Randomized Controlled Trial
Steven E. Nissen, MD; E. Murat Tuzcu, MD; Paul Schoenhagen, MD; B. Greg Brown, MD; Peter Ganz, MD; Robert A. Vogel, MD; Tim Crowe, BS; Gail Howard, MS; Christopher J. Cooper, MD; Bruce Brodie, MD; Cindy L. Grines, MD; Anthony N. DeMaria, MD; for the REVERSAL Investigators
Statin Trials Utilizing IVUS: REVERSALStatin Trials Utilizing IVUS: REVERSAL
Primary hypothesis• A large (vs moderate) reduction in LDL-C will cause
a greater decrease in the total atherosclerotic burden in patients with established CAD measured by IVUS
Secondary hypothesis• The reduction in plaque burden as assessed by
IVUS will be evident despite the absence of any angiographically apparent improvement
Primary hypothesis• A large (vs moderate) reduction in LDL-C will cause
a greater decrease in the total atherosclerotic burden in patients with established CAD measured by IVUS
Secondary hypothesis• The reduction in plaque burden as assessed by
IVUS will be evident despite the absence of any angiographically apparent improvement
Data on file, Pfizer Inc., New York, NY.
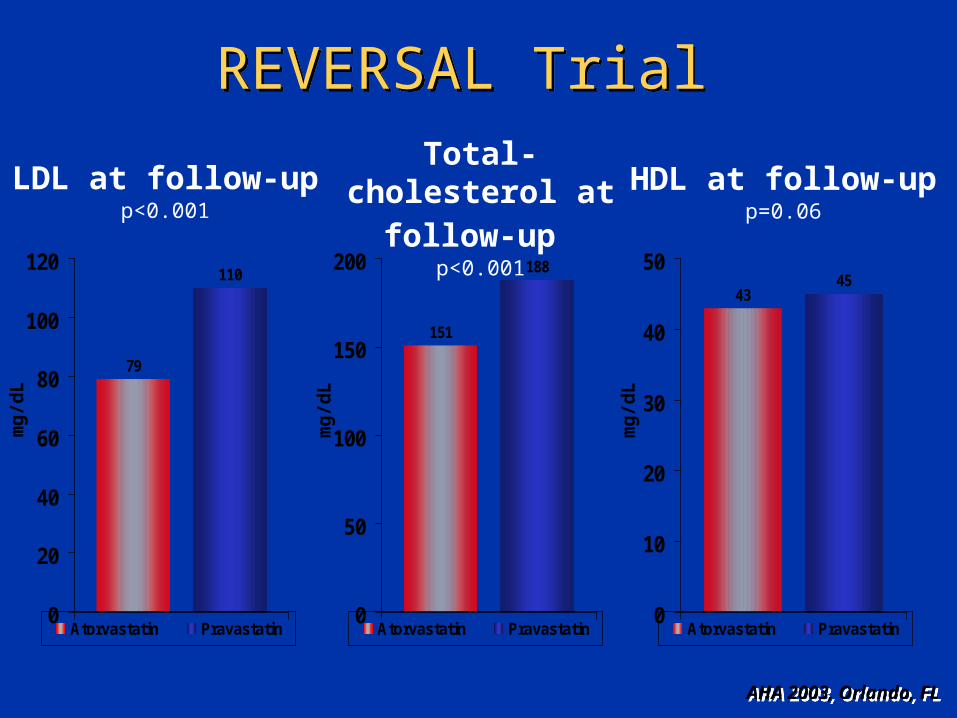
REVERSAL Trial REVERSAL Trial
79
110
0
20
40
60
80
100
120
Atorvastatin Pravastatin
LDL at follow-up p<0.001
AHA 2003, Orlando, FLAHA 2003, Orlando, FL
mg
/dL
151
188
0
50
100
150
200
Atorvastatin Pravastatin
Total-cholesterol at follow-up
p<0.001
mg
/dL
4345
0
10
20
30
40
50
Atorvastatin Pravastatin
HDL at follow-up p=0.06
mg
/dL
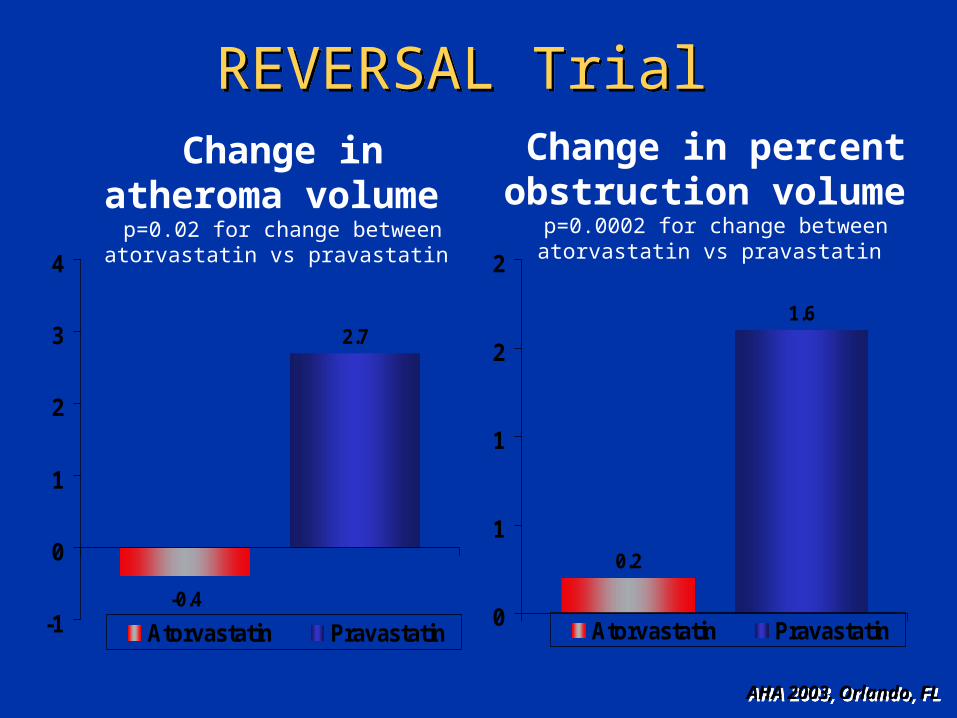
REVERSAL Trial REVERSAL Trial
-0.4
2.7
-1
0
1
2
3
4
Atorvastatin Pravastatin
Change in atheroma volume
p=0.02 for change between atorvastatin vs pravastatin
Change in percent obstruction volume
p=0.0002 for change between atorvastatin vs pravastatin
0.2
1.6
0
1
1
2
2
Atorvastatin Pravastatin
AHA 2003, Orlando, FLAHA 2003, Orlando, FL

REVERSAL Trial REVERSAL Trial
• Among patients with symptomatic CAD and elevated LDL, use of an aggressive lipid-lowering strategy through treatment with 80-mg atorvastatin was associated with a reduction in percent change in atheroma volume compared with a more moderate lipid-lowering strategy through treatment with 40-mg pravastatin
• Primary endpoint used an IVUS endpoint and the trial was not designed to assess mortality or clinical events, and a much larger trial would be needed to assess superiority of one statin over another for these endpoints
• Among patients with symptomatic CAD and elevated LDL, use of an aggressive lipid-lowering strategy through treatment with 80-mg atorvastatin was associated with a reduction in percent change in atheroma volume compared with a more moderate lipid-lowering strategy through treatment with 40-mg pravastatin
• Primary endpoint used an IVUS endpoint and the trial was not designed to assess mortality or clinical events, and a much larger trial would be needed to assess superiority of one statin over another for these endpoints
PRavastatin Or atorVastatin Evaluation and Infection
Therapy (TIMI 22)
PRavastatin Or atorVastatin Evaluation and Infection
Therapy (TIMI 22)
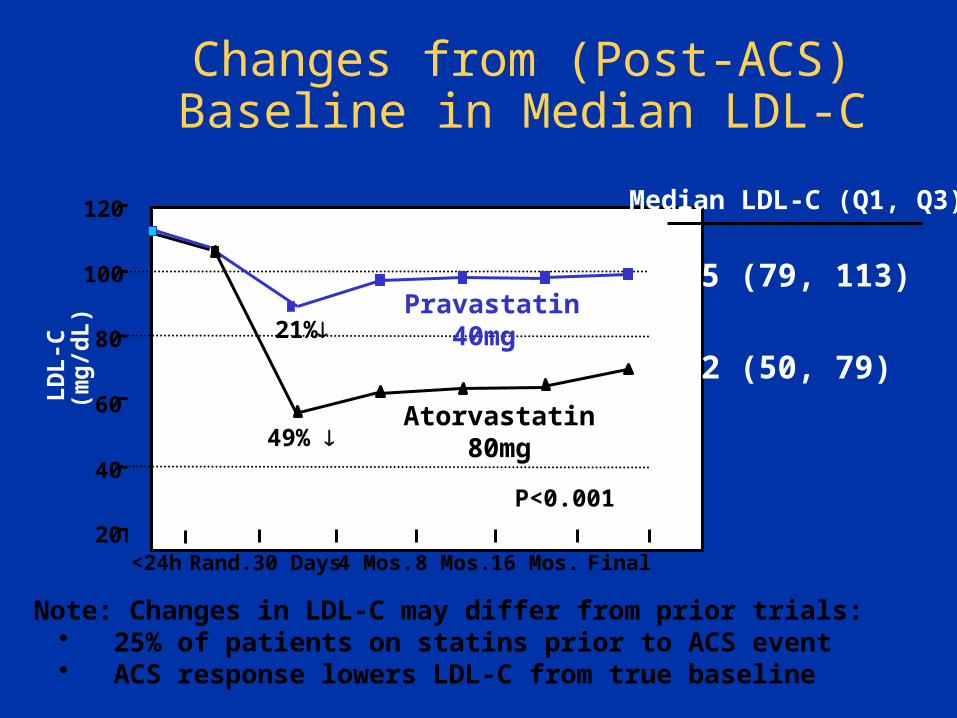
Changes from (Post-ACS) Baseline in Median LDL-C
Note: Changes in LDL-C may differ from prior trials: • 25% of patients on statins prior to ACS event• ACS response lowers LDL-C from true baseline
LD
L-C
(m
g/d
L)
20
40
60
80
100
120
Rand. 30 Days 4 Mos. 8 Mos. 16 Mos. Final
Pravastatin 40mg
Atorvastatin 80mg49%
21%
P<0.001
Median LDL-C (Q1, Q3)
95 (79, 113)
62 (50, 79)
<24h
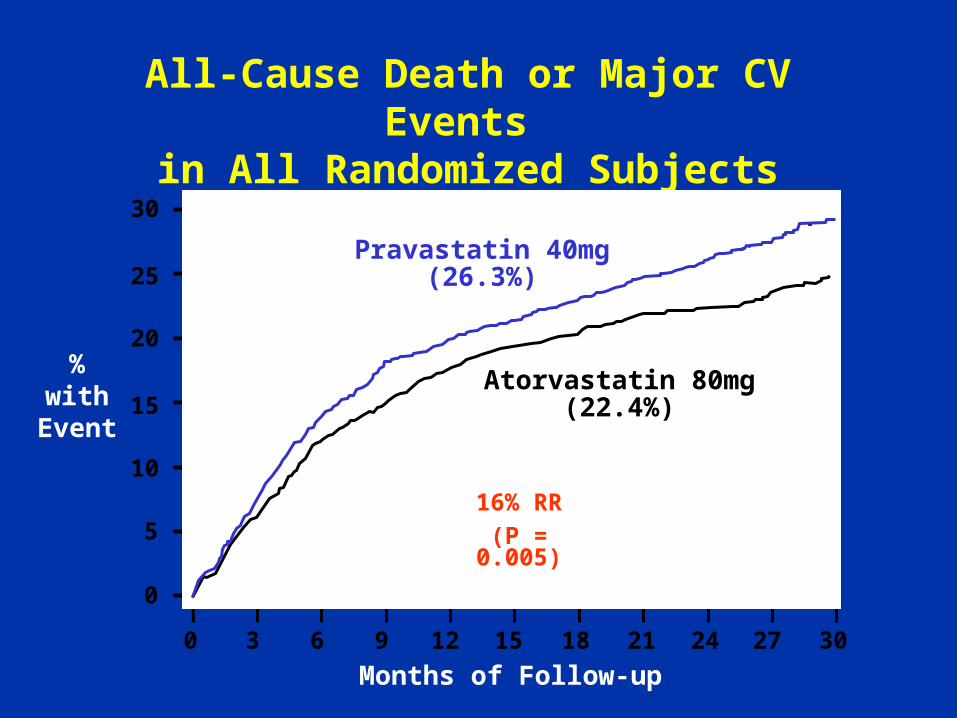
All-Cause Death or Major CV Events in All Randomized Subjects
0 3 18 21 24 27 306 9 12 15
% with
Event
Months of Follow-up
Pravastatin 40mg(26.3%)
Atorvastatin 80mg(22.4%)
16% RR
(P = 0.005)
30
25
20
15
10
5
0
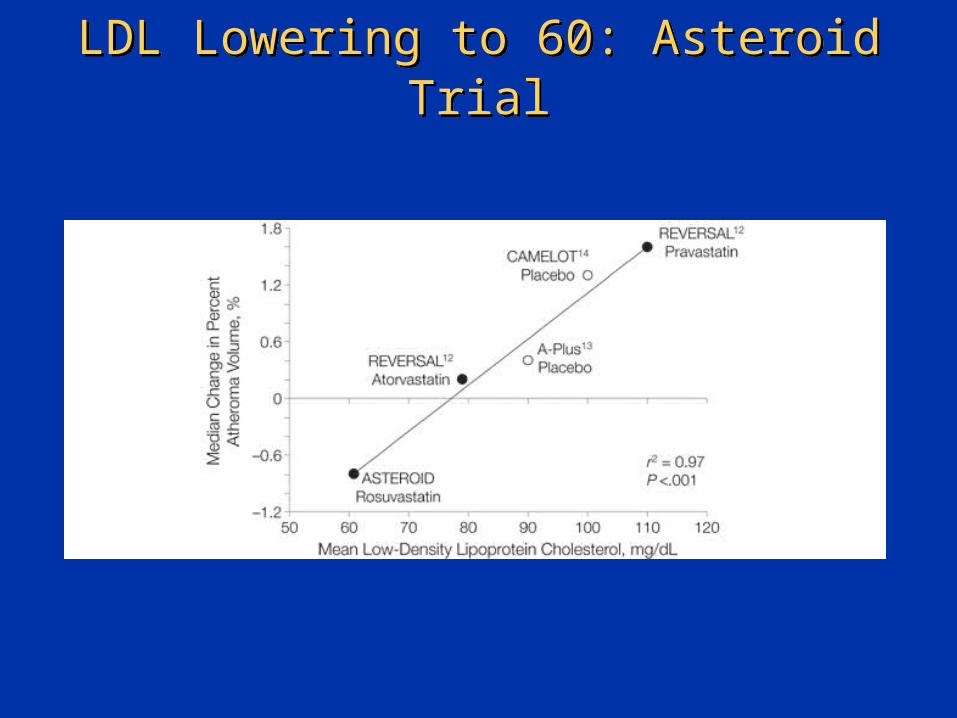
LDL Lowering to 60: Asteroid TrialLDL Lowering to 60: Asteroid Trial
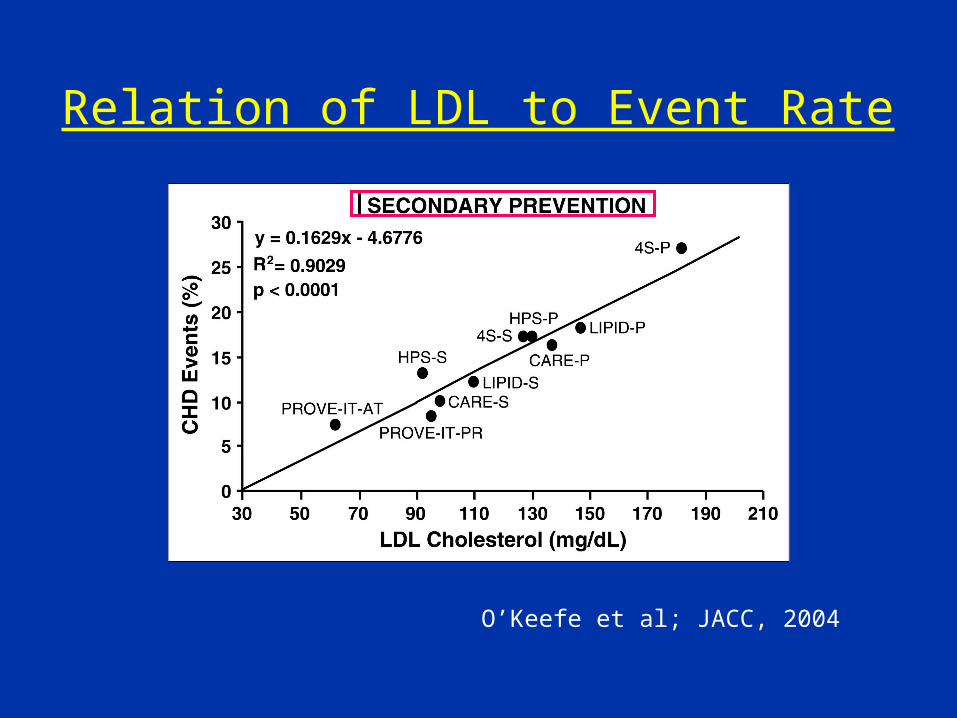
Relation of LDL to Event Rate
O’Keefe et al; JACC, 2004
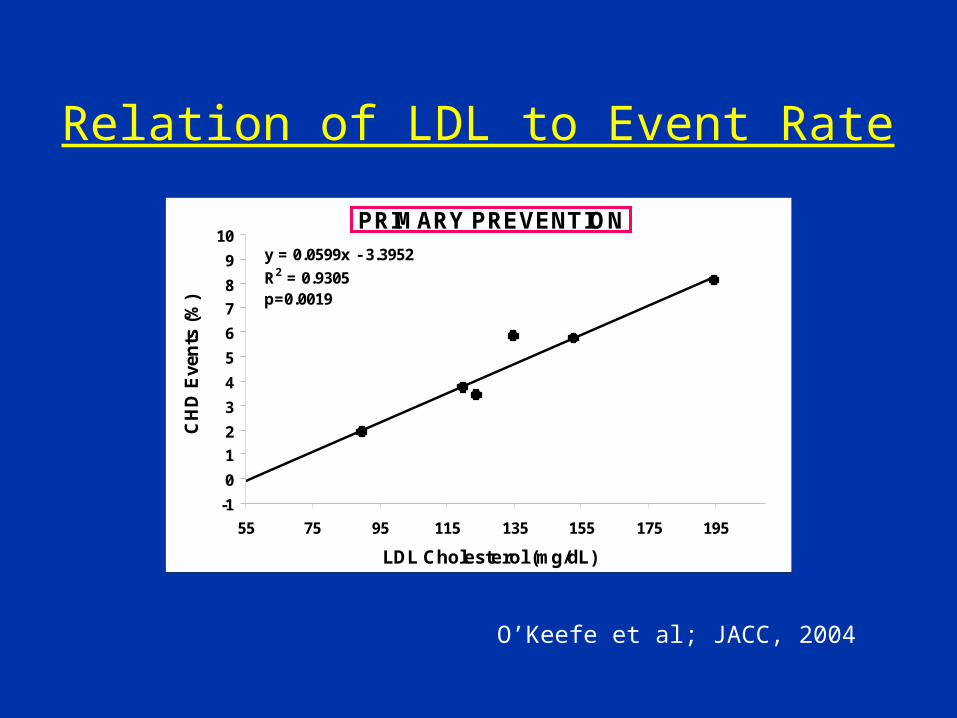
PRIMARY PREVENTION
y = 0.0599x - 3.3952
R2 = 0.9305p=0.0019
-1
0
1
2
3
4
5
6
7
8
9
10
55 75 95 115 135 155 175 195
LDL Cholesterol (mg/dL)
CH
D E
ven
ts (
%) WOSCOPS-P
AFCAPS-P
WOSCOPS-S
AFCAPS-S
ASCOT-P
ASCOT-S
Relation of LDL to Event Rate
O’Keefe et al; JACC, 2004
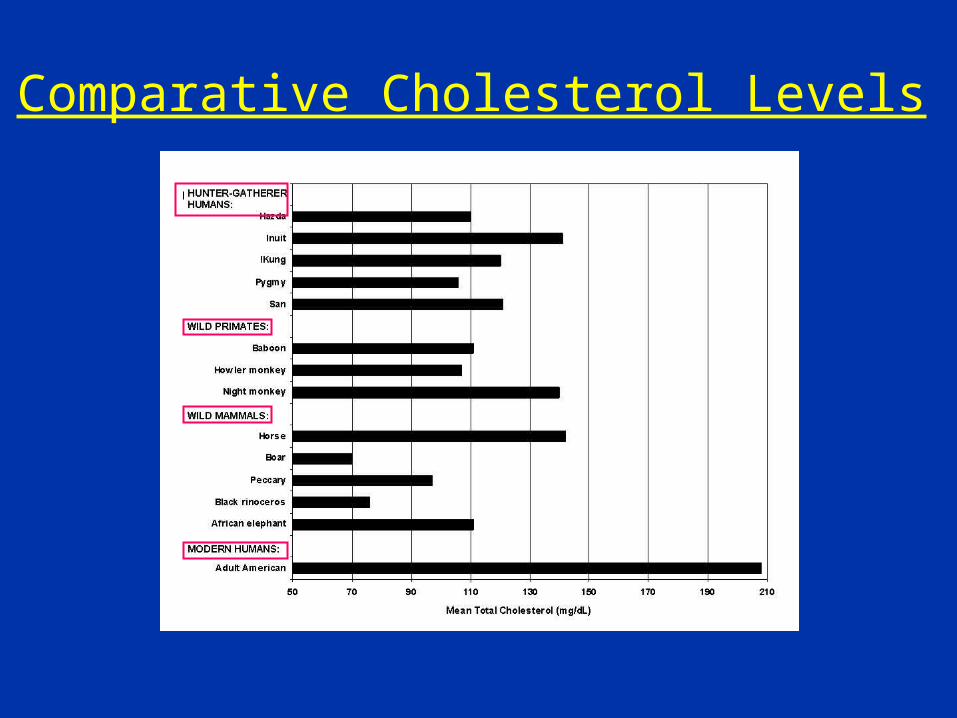
Comparative Cholesterol Levels

“Be There”: Making San Diego County a Heart Attack and Stroke-Free Zone
“Be There”: Making San Diego County a Heart Attack and Stroke-Free Zone
Anthony DeMaria, MDJudith and Jack White Chair in Cardiology
University of California, San DiegoChair, San Diego Right Care-Be There Campaign
Anthony DeMaria, MDJudith and Jack White Chair in Cardiology
University of California, San DiegoChair, San Diego Right Care-Be There Campaign
108
GR MH Tony 1st subm TJ edits 9Feb2012
BackgroundBackground
• Cardiovascular disease (CVD) remains the leading cause of death in the United States
• San Diego and CVD
– Heart disease and stroke together are the leading cause of death
• Nearly 5,000 deaths annually from heart disease (rate 112)
• Quick comparison of rates to those nationwide
• Risk factors have been identified for which effective interventions exist (ABCS)
• Cardiovascular disease (CVD) remains the leading cause of death in the United States
• San Diego and CVD
– Heart disease and stroke together are the leading cause of death
• Nearly 5,000 deaths annually from heart disease (rate 112)
• Quick comparison of rates to those nationwide
• Risk factors have been identified for which effective interventions exist (ABCS)
109

San Diego County Health and Human Services: Stakeholders in CVD Prevention
San Diego County Health and Human Services: Stakeholders in CVD Prevention
• Live Well San Diego • Live Well San Diego
110
http://www.sdcounty.ca.gov/hhsa/programs/sd/health_strategy_agenda/index.html
Communities Putting Prevention to Work (CDC grant) Reduce chronic disease by physical activity, nutrition, and
school environments Community Transformation Grant (CDC grant)
Tobacco free, active living, healthy eating, reduce hypertension and high cholesterol
Beacon Grant (NIH) Awarded across the country to serve as pilots for wide-scale use of health information technology through the Beacon Community program
How It All StartedHow It All Started
• Coordinated effort to improve quality– State Department of Managed Health Care– Medical groups beyond managed care organizations– UC Berkeley School of Public Health– Rand Health (GO Grant)
• Goal: Achieve national HEDIS 90% percentile targets– Blood pressure, lipids, blood sugar
• University of Best Practices meetings– Monthly meetings– Physicians, nurses, administrators, pharmacist– Discuss successful strategies– Now sharing data among group participants
• Coordinated effort to improve quality– State Department of Managed Health Care– Medical groups beyond managed care organizations– UC Berkeley School of Public Health– Rand Health (GO Grant)
• Goal: Achieve national HEDIS 90% percentile targets– Blood pressure, lipids, blood sugar
• University of Best Practices meetings– Monthly meetings– Physicians, nurses, administrators, pharmacist– Discuss successful strategies– Now sharing data among group participants
111
HEDIS, Healthcare Effectiveness Data and Information Set
Be There CampaignBe There Campaign
• Concept: “Heart Attack and Stroke-free Zone” – Audacious goal to capture attention– Extends the risk reduction efforts to all citizens– Actively engages persons in their own health (care)– Conveys ownership to population – Taps in to community pride
• Aim: Achieve both screening for risk factors and compliance with interventions
• Funding: $650,000; philanthropy• Steering Committee: Private-public partnership
• Concept: “Heart Attack and Stroke-free Zone” – Audacious goal to capture attention– Extends the risk reduction efforts to all citizens– Actively engages persons in their own health (care)– Conveys ownership to population – Taps in to community pride
• Aim: Achieve both screening for risk factors and compliance with interventions
• Funding: $650,000; philanthropy• Steering Committee: Private-public partnership
112

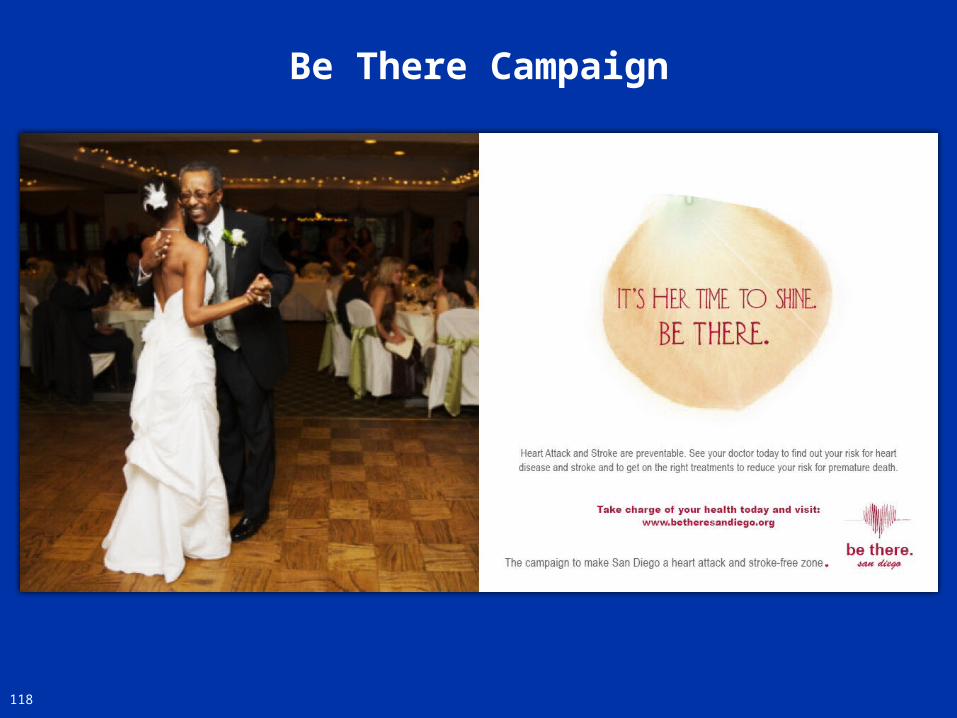
San Diego Demonstration ProjectGoing Emotional!
San Diego Demonstration ProjectGoing Emotional!
Emotional “tug” is critical for commitment to change one’s behavior
Benefit to those we love can be a bigger driver than benefit to oneself
Caring for one’s own health makes it possible to “be there”
for those we love!
Emotional “tug” is critical for commitment to change one’s behavior
Benefit to those we love can be a bigger driver than benefit to oneself
Caring for one’s own health makes it possible to “be there”
for those we love!
113
“When something is missing in your life,
it usually turns out to be someone”.
Robert Brault
Be There CampaignSteering Committee
• Anthony N. DeMaria, MD Judith and Jack White Chair in Cardiology, Professor of Medicine, University of California, San Diego, Editor-in-Chief, Journal of the American College of Cardiology, Chair, San Diego Right Care-Be There Campaign
• Daniel Dworski, MD, Medical Director, Scripps Medical Group
• Jim Dudl, MD, Vice-Chair, Steering Committee, Clinical Lead, Kaiser Care Management Institute
• James Dunford, MD, FACEP, City of San Diego Medical Director of Emergency Medical Services. President,San Diego American Heart Association
• Nora Faine, MD, MPH, Medical Director, Sharp Health Plan
• Scott Flinn, MD, Medical Director, Arch Medical Group
• Lawrence Friedman, MD, Medical Director, Managed Care, Ambulatory Care and Medical Group Quality and Safety, University of California, San Diego
• Anthony N. DeMaria, MD Judith and Jack White Chair in Cardiology, Professor of Medicine, University of California, San Diego, Editor-in-Chief, Journal of the American College of Cardiology, Chair, San Diego Right Care-Be There Campaign
• Daniel Dworski, MD, Medical Director, Scripps Medical Group
• Jim Dudl, MD, Vice-Chair, Steering Committee, Clinical Lead, Kaiser Care Management Institute
• James Dunford, MD, FACEP, City of San Diego Medical Director of Emergency Medical Services. President,San Diego American Heart Association
• Nora Faine, MD, MPH, Medical Director, Sharp Health Plan
• Scott Flinn, MD, Medical Director, Arch Medical Group
• Lawrence Friedman, MD, Medical Director, Managed Care, Ambulatory Care and Medical Group Quality and Safety, University of California, San Diego
• Lisa Gleason, MD CMIO, Cardiology Department Head, Naval Medical Center San Diego
• Hattie Rees Hanley, MPP, Right Care Initiative Project Director and Special Advisor to the Dean for Outcomes Improvement and Innovation, UC Berkeley School of Public Health and Department of Managed Health Care
• Elizabeth Helms, Executive Director, CA Chronic Care Coalition and Right Care San Diego Coordinator
• Susan Kaweski, MD, President, San Diego County Medical Society
• Jerry Penso, MD, Medical Director, Continuum of Care, Sharp Rees-Stealy Medical Group, Chair: University of Best Practices
• James Schultz MD, Council of Community Clinics
• Robert Smith, MD, Chief Medical Officer, Veteran’s Administration San Diego Medical Center
• Melissa J. Wilimas, Executive Director, American Heart Association
• Nick Yphantides, MD, MPH, Executive Medical Consultant, San Diego County Public Health and Human Services
• Lisa Gleason, MD CMIO, Cardiology Department Head, Naval Medical Center San Diego
• Hattie Rees Hanley, MPP, Right Care Initiative Project Director and Special Advisor to the Dean for Outcomes Improvement and Innovation, UC Berkeley School of Public Health and Department of Managed Health Care
• Elizabeth Helms, Executive Director, CA Chronic Care Coalition and Right Care San Diego Coordinator
• Susan Kaweski, MD, President, San Diego County Medical Society
• Jerry Penso, MD, Medical Director, Continuum of Care, Sharp Rees-Stealy Medical Group, Chair: University of Best Practices
• James Schultz MD, Council of Community Clinics
• Robert Smith, MD, Chief Medical Officer, Veteran’s Administration San Diego Medical Center
• Melissa J. Wilimas, Executive Director, American Heart Association
• Nick Yphantides, MD, MPH, Executive Medical Consultant, San Diego County Public Health and Human Services
114

Wireless Heart Monitors
Technology Integration Important differentiating component of the Campaign Incorporation of innovative medical and health related
technological advancements to enhance target user groups’ interest, adherence, and participation in the program
Wireless monitors to track exercise regime
Smart Phones to track and report vitals
115
Be There Campaign
Pill bottles that monitor medication adherence
Selected Implementation Activities
Detailed implementation tactics have been developed but as an overview, here is a summary of some of the patient engagement strategies that will be used by the “Be There San Diego” campaign
Recruit physicians using University of Best Practices
Screening events Shopping malls, pharmacies, schools, faith based groups
“Be There San Diego” Pins worn by pharmacists and medical office staff Bus to implement screening across county
Multimedia advertising campaign across all media platforms
Social media viral campaign to connect with community
116

117
Be There Campaign
Be There Campaign
118
Be There Campaign
119
Be There Campaign
120

Be There Campaign
122

Important Low HDL-C Facts:Independent Risk Factor for CHD
Important Low HDL-C Facts:Independent Risk Factor for CHD
• 70% of all infarctions occur in patients with low HDL-C (<45 mg/dl) based on the Framingham
• A 1 mg/dl increase in HDL-C reduces MI risk by 3-4%, based on Framingham
• Low HDL-C is identified as an independent CHD risk factor in the NCEP guidelines
• Low HDL-C was the second most important risk factor in 4S
• 70% of all infarctions occur in patients with low HDL-C (<45 mg/dl) based on the Framingham
• A 1 mg/dl increase in HDL-C reduces MI risk by 3-4%, based on Framingham
• Low HDL-C is identified as an independent CHD risk factor in the NCEP guidelines
• Low HDL-C was the second most important risk factor in 4S
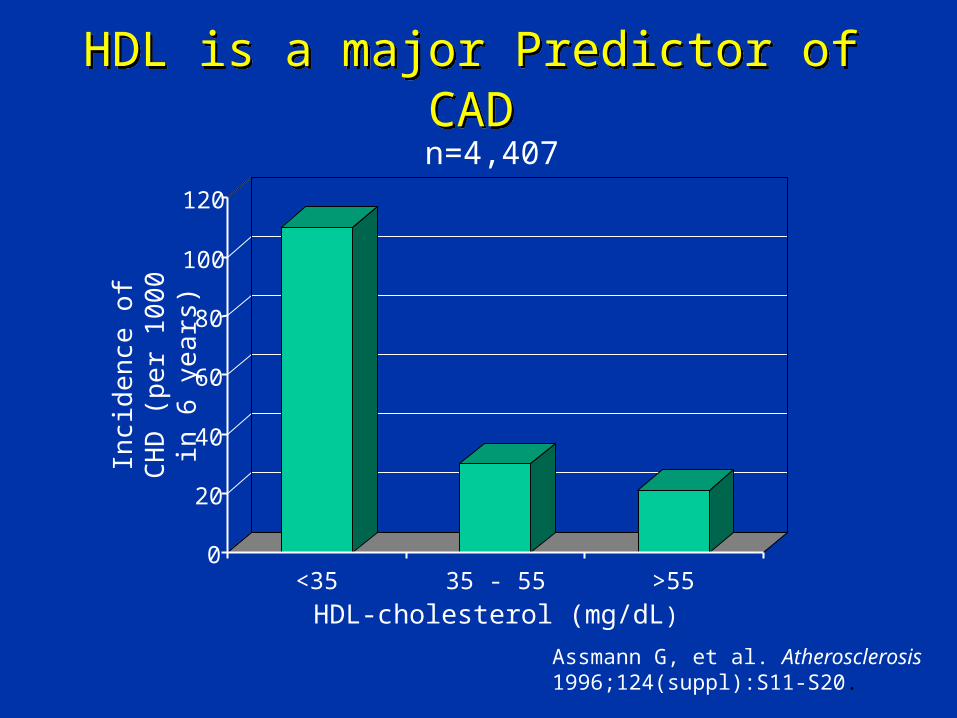
HDL is a major Predictor of CADHDL is a major Predictor of CAD
0
20
40
60
80
100
120
<35 35 - 55 >55HDL-cholesterol (mg/dL)
Incid
ence
of C
HD
(per
100
0 in
6 y
ears
)n=4,407
Assmann G, et al. Atherosclerosis 1996;124(suppl):S11-S20.
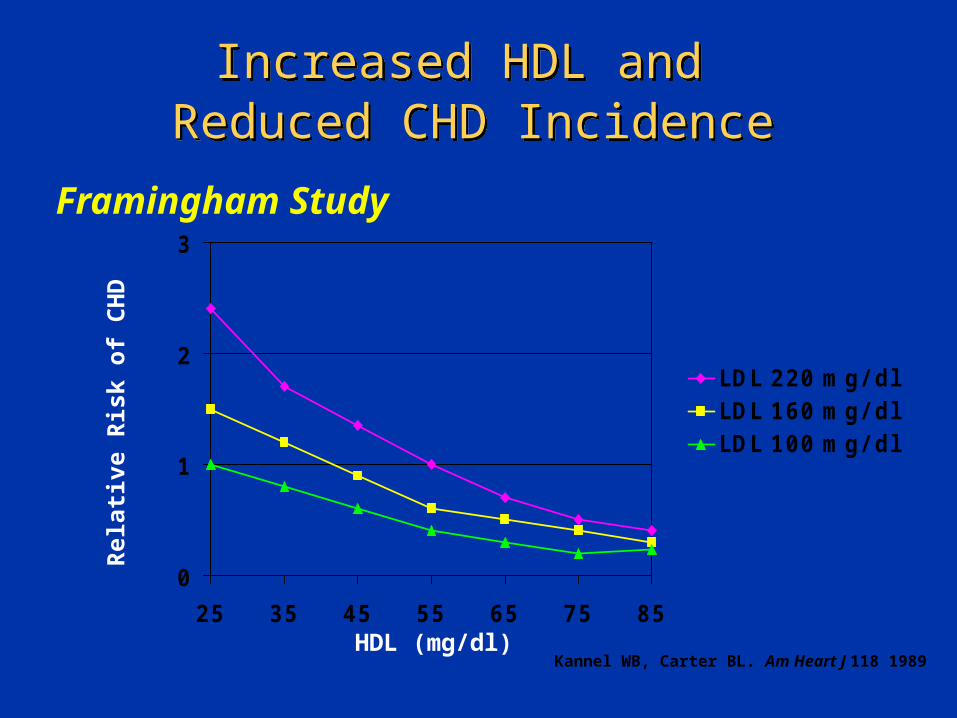
Increased HDL and Reduced CHD Incidence
Increased HDL and Reduced CHD Incidence
Framingham Study
0
1
2
3
25 35 45 55 65 75 85
LDL 220 mg/ dlLDL 160 mg/ dlLDL 100 mg/ dl
Rel
ativ
e R
isk
of
CH
D
HDL (mg/dl)Kannel WB, Carter BL. Am Heart J 118 1989
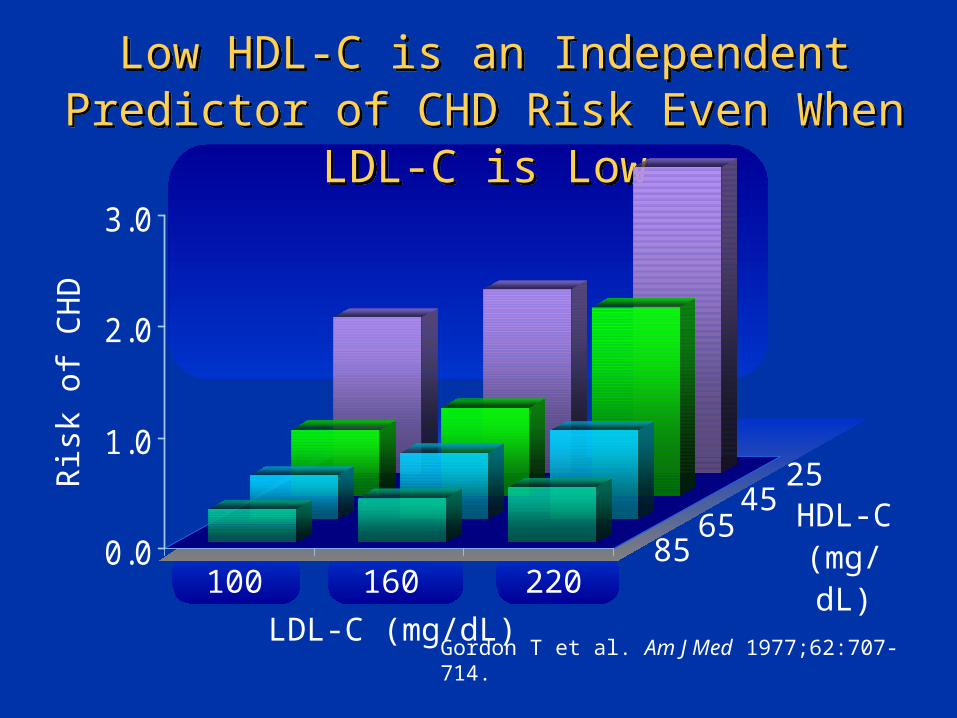
100 160 2200.0
1.0
2.0
3.0
Ris
k of
CH
DLow HDL-C is an Independent Predictor of
CHD Risk Even When LDL-C is LowLow HDL-C is an Independent Predictor of
CHD Risk Even When LDL-C is Low
HDL-C(mg/dL)
LDL-C (mg/dL)
25
Gordon T et al. Am J Med 1977;62:707-714.
4565
85
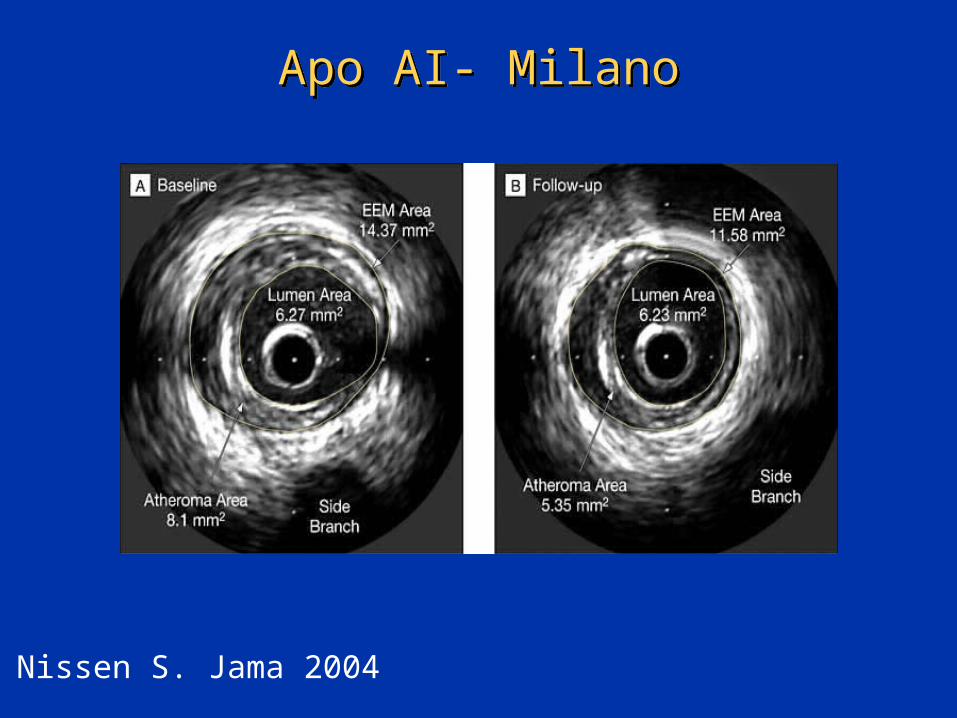
Apo AI- MilanoApo AI- Milano
Nissen S. Jama 2004

Role of HDL for RegressionRole of HDL for Regression
Nichols et al; JAMA, 2007
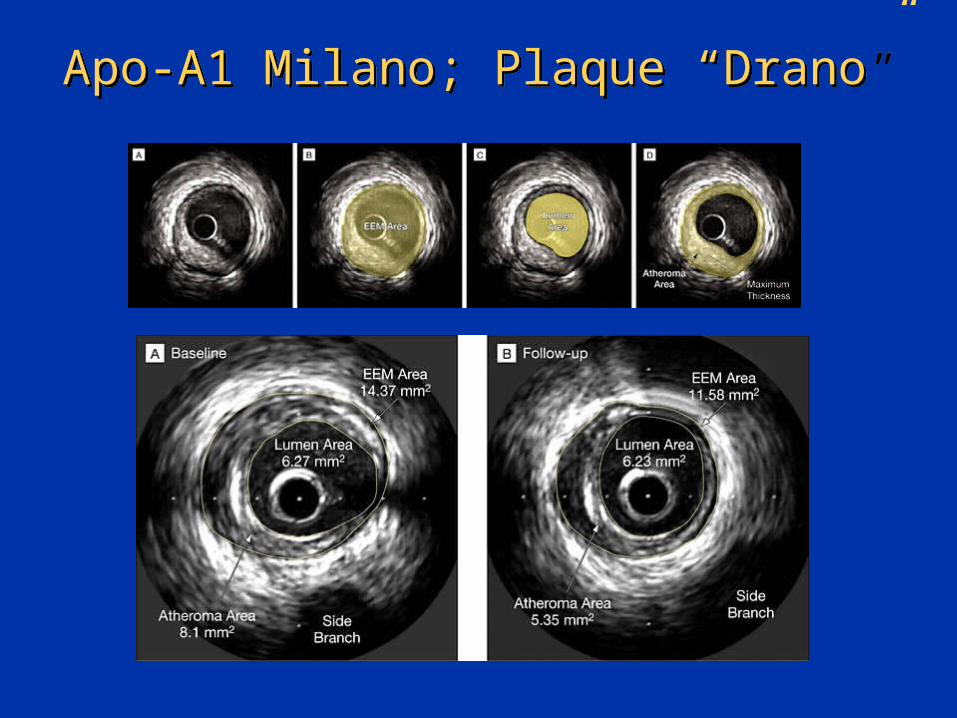
Apo-A1 Milano; Plaque “Drano”Apo-A1 Milano; Plaque “Drano”
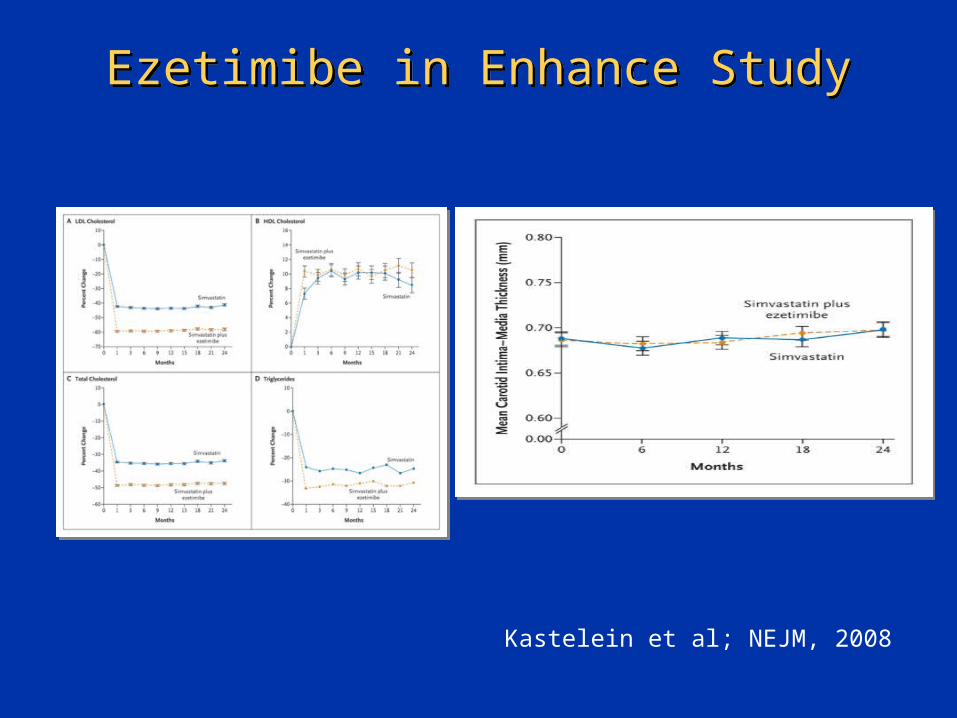
Ezetimibe in Enhance StudyEzetimibe in Enhance Study
Kastelein et al; NEJM, 2008

CAD: A Changing ParadigmCAD: A Changing Paradigm
Old Paradigm:
Focal disease
High grade stenoses account for morbidity and mortality
Rx: PCI and CABG
Old Paradigm:
Focal disease
High grade stenoses account for morbidity and mortality
Rx: PCI and CABG
New Paradigm:
Diffuse Disease of the entire artery
High grade stenoses cause angina- vulnerable plaques cause MI’s
Rx: Lipid lowering rx, ASA, ACE Inhibitors
CABG/PCI for angina, ischemic cardiomyopathy
New Paradigm:
Diffuse Disease of the entire artery
High grade stenoses cause angina- vulnerable plaques cause MI’s
Rx: Lipid lowering rx, ASA, ACE Inhibitors
CABG/PCI for angina, ischemic cardiomyopathy

Hunter/GathererHunter/Gatherer
ANDAND