ANORECTAL MALFORMATION.ppt

of 40
Transcript of ANORECTAL MALFORMATION.ppt
-
7/24/2019 ANORECTAL MALFORMATION.ppt
1/40
Presented ByAnu George
MSc Nsg(Peadiatrics) Student
Supervisor:Dr.(Mrs.) Raman Kaia
!ecturer
-
7/24/2019 ANORECTAL MALFORMATION.ppt
2/40
Imperforate anusIncludes agenesis and atresiaof the rectum and anus
Etiology: unknownIncidence: 1 in 4,500
SEX: 0!male
-
7/24/2019 ANORECTAL MALFORMATION.ppt
3/40
"#$: Em%ryologyThe cloaca&which is a common cham%er into the hindgut and allantois'
Separated into:
(ownward growth
of a septum
Fusion during the )rdmonth of intrauterine life
when there is imperfect fusion imperforate anus
The bladderpost-allantoic gut
)rectum(
Proctadeum
)epiplastic bud(
-
7/24/2019 ANORECTAL MALFORMATION.ppt
4/40
Imperforate anus
Low abnormalities*ermination of %owel %elow
the pel+ic floor
Easy to (iagnoseSimple to #
utlook is good
1'-o+ered anus.'Ectopic anus
)'Stenosed anus
4'$em%ranous stenosis
High abnormalities*ermination of %owel a%o+e
the pel+ic floor
ften ha+e a fistula into theurinary tract with
deficient pel+ic floor
(ifficult to R
1'"norectal agenesis
.'#ectal atresia
)'-loaca
-
7/24/2019 ANORECTAL MALFORMATION.ppt
5/40
-
7/24/2019 ANORECTAL MALFORMATION.ppt
6/40
1'-o+ered anus"nal canal co+ered %y a %ar of skinwith a
trackrunning forwards to the perinealraphe/ *his track is called ucket 2andle3
midline #aphe fistula/
-
7/24/2019 ANORECTAL MALFORMATION.ppt
7/40
.'Ectopic anus
"nus situated anteriorly in , it opens in" perineum
in , it opens in# +ul+a&more commonly'+ul+al
ectopic anusor +agina&rare'
-
7/24/2019 ANORECTAL MALFORMATION.ppt
8/40
)'Stenosed anusi/e/ microscopic anus
*here is a minute openingthat can %e seen if
eamined carefuly
-
7/24/2019 ANORECTAL MALFORMATION.ppt
9/40
4'$em%ranous stenosis#are"nus is normally sited
co+ered with a thin mem%rane that%ulges with retained meconium
-
7/24/2019 ANORECTAL MALFORMATION.ppt
10/40
-ould %e associated with:a fistulasconnection %etween the %lind rectalstump and the %ladder
or other pel+ic structures a%normally
-
7/24/2019 ANORECTAL MALFORMATION.ppt
11/40
1'"norectal "genesis
#arelind rectal pouch lies 6ust a%o+e the pel+icfloor
In " anterior aspect attached tothe%ladder 7 often there is a recto+esical fistulaor rectourethral fistula&manifested %y passageof gas or meconium in the urine' or perinealfistula
In # fistula to the posterior forni
recto+esti%ular &or recto+aginal' low #89 Easy to correctost;op/ 9unction is good
high #89 (ifficult to correct
ost;op function is poor
-
7/24/2019 ANORECTAL MALFORMATION.ppt
12/40
-
7/24/2019 ANORECTAL MALFORMATION.ppt
13/40
-
7/24/2019 ANORECTAL MALFORMATION.ppt
14/40
.'#ectal atresia#areAnal canalis normal %ut ends %lindlyat the le+el
of pel+ic floor 7 the rectumalso ends %lindlya%o+e the pel+ic floor without a fistulas opening/
-
7/24/2019 ANORECTAL MALFORMATION.ppt
15/40
)'-loacaccurs only in #owel, urinary7 genital tractsall open into a
common wide ca+ity
-ommonly associated with otherde+elopmental a%normalities e/g/tracheoesophagial fistula
-
7/24/2019 ANORECTAL MALFORMATION.ppt
16/40
"pproach2istory the systems in+ol+edEamination ((
In+estigation ($anagement
-
7/24/2019 ANORECTAL MALFORMATION.ppt
17/40
2istory9ailure to pass meconiumwithin the 1st.4
hours of life/
atients with anterior ectopic anusmaypresent in childhood or in adulthood/ *hesepatients ha+e lifelong histories of constipation
and painful defecationand usually ha+ere
-
7/24/2019 ANORECTAL MALFORMATION.ppt
18/40
Eamination
Inspectionalone is sufficient for management plan in 90%of patients/
Low=ucket handle defect
=>as?meconium from perineum
=erineal fistula if skin %ridge%etween +esti%ule and fistula/
="nterior ectopic anusi/e/ normal si@ed anussurrounded %y normal muscle/
=Arine free of meconium&B a+erage of .0 hrs for meconium to appear in urine'/
High=9lat %ottom
=Short sacrum
=Cittle muscle contraction=$econium per urethra
=#ecto+esti%ular fistula if within mucosalmargin of the +esti%ule/
=Sphincter located close to the scrotumor %ifid scrotum often associated
with a rostatic 9istula/=-loacae are often missed if urethralopening is not identified in female
with a recto;+aginal3 fistula/=9urthermore, cloacae often ha+e small
openings and may %e a cause ofreferral for am%iguous genitalia/
?
-
7/24/2019 ANORECTAL MALFORMATION.ppt
19/40
In+estigationVery Important to:
1/ Eclude other anomaliesDD
./(etermine whether a%normality is highor lowDD
-
7/24/2019 ANORECTAL MALFORMATION.ppt
20/40
1/ Eclude other "nomaliesDDD"nal atresia may occur as a part of the VAT!"L
groupof anomaliesV Verte%ral %ody segmentation defect
A Anal atresia ardio+ascular &(", 8S('T! Tracheo esophagial fistula" unilateral "enal agenesis
L Lim% anomaly &radial ray hypoplasia'
So, +ery careful eamination of the %a%y must %e madeto eclude these anomalies
-
7/24/2019 ANORECTAL MALFORMATION.ppt
21/40
Eclude other "nomaliesDDD
&contd'Associated abnormality Investigation
"V" Vertebral Abnormality )butterflyvertebrae, hemi-vertebrae(
pinal ultrasound, pinal !-ray
"" ardiac, #eart Abnormalityardiac $#% )V&, A&, P&A(
ardiac $#%
"R" Renal, 'idney abnormality )solitaryidney, horse shoe idney(
Renal ultrasound, Voiding cysto-urethra-gram )V*(
"T$" tracheoesophogeal abnormality)T$+(
Physical e!amination
"" imb deformity Physical e!amination, !-rays
. ( h h % l
-
7/24/2019 ANORECTAL MALFORMATION.ppt
22/40
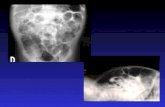
./(etermine whether a%normality ishighor lowDD
#$Inertogram:with a metal buttonor a coinstrapped to the site of the anus or
a metal bougieinserted into the %lind anal canalInfant is held upside downfor );4 minutes*hen radiograph in the in+erted lateral position & %oth the
greater trochanters should %e on the same line'*he gas in the rectum will rise to the top indicates the distance%etween the site of the metal indicator and the %lind end of therectum &&& if the distance ./5 cm, the a%normality is highDD
if the rectum ends a%o+e the - line &pu%ococcygeal line F fromthe symphysis pu%is to the last +erte%ra', the a%normality is Cow
7 +ise +ersa or according to ischeal line &%etween ant/;sup/ Iliacspines'/Ghen to %e doneH"lthough it is a useful method, sometimes +itiated %y a plug of
meconium in the rectum causing an apparent gap far in ecess ofthat actually present/ So, it may %e necessary to wait until the
%a%y is .4 hrs old%efore rectal gas appears
-
7/24/2019 ANORECTAL MALFORMATION.ppt
23/40
' line
(etal button
gas in the rectum
-
7/24/2019 ANORECTAL MALFORMATION.ppt
24/40
-
7/24/2019 ANORECTAL MALFORMATION.ppt
25/40
)$*rine culture:resence of meconium
resence of proteusor pseu+omonasusually signifies that a fistulais present
,$*-:*o e+aluate the lesion type
.$("I:If we suspected comple malformation
/$(icturating cystourethrogram:y in6ecting a dye in the urethra
-
7/24/2019 ANORECTAL MALFORMATION.ppt
26/40
-
7/24/2019 ANORECTAL MALFORMATION.ppt
27/40
Treatment of Low abnormalities:
#$oere+ anus:
*he track should %e opened %y scissors
9ollowed %y routine dilatationof the anus
)$!ctopic anus:
lastic cut;%ack3operation
,$-tenose+ anus:#egular dilatation
-
7/24/2019 ANORECTAL MALFORMATION.ppt
28/40
Treatment of High Abnormalities:
8ery difficult pro%lem 7 each case must %e consideredon its merits*he possi%ilities are:Twostage operation:1ststage laparotomy
(i+ision of rectourethral fistula *rans+erse colostomy.ndstage rectal pull;through3 operation1nestage operation:
laparotomy (i+ision of fistula pull;through3 operation(i+ision of fistula 7 rectal pull;down3 operation
through the perinum& now rarely used'
-
7/24/2019 ANORECTAL MALFORMATION.ppt
29/40
Treatment of High abnormalities
2cont+3$*he new techni
-
7/24/2019 ANORECTAL MALFORMATION.ppt
30/40
ull;through peration
Cower %owel is mo%ili@edBew passage is created through thepel+ic floor %y passing a pair of cur+edforceps7 through it, keeping close tothe urethra, to the site of the futureanus/
*his is dilated %y 2egars dilatorsothat the %owel can %e pulled down andits mucosa stitched to the skinof the
newly formed anus/(aily dilatationwill %e re
-
7/24/2019 ANORECTAL MALFORMATION.ppt
31/40
'-A"'*he S"# dissection is along the midline pro+idinge4cellent e4posurewith minimal trauma toneres an+ musculature5
It inoles:= Stimulation of musclesto demonstrate the midline
and sphincter
= osterior sagittal incision; length depends onse+erity of a%normality and re
-
7/24/2019 ANORECTAL MALFORMATION.ppt
32/40
osition for S"#
-
7/24/2019 ANORECTAL MALFORMATION.ppt
33/40
Incision in S"#
-
7/24/2019 ANORECTAL MALFORMATION.ppt
34/40
osterior sagittal repair of a recto+esti%ular
fistula/
-
7/24/2019 ANORECTAL MALFORMATION.ppt
35/40
rognosisIn high %of cases, imperforate anus is associatedwith other congenital a%normalities especially ofthe urinary organs 7 nearly /0%of deaths incases of imperforate anus are due to othermalformations
-
7/24/2019 ANORECTAL MALFORMATION.ppt
36/40
Bursing $anagementIdentification of "#$ at %irth and promptmanagement? #eferral
repare for colostomy(emonstrate to the parents the care ofcolostomy
Ensure competent home care and regular follow
upreparation for surgeryost;p Bursing $anagement
-
7/24/2019 ANORECTAL MALFORMATION.ppt
37/40
Bursing $anagement&contd''ost1pImmediate post;op care
re+ent Infection and promote healing: -are ofthe suture line, anti%ioticsButritionSystematic (ilation
re+ention of constipationowel training-are of colostomy
-
7/24/2019 ANORECTAL MALFORMATION.ppt
38/40
In a Summary# opening -loaca) openings anorectal agenesis with
recto+aginal fistula, openings ectopic anus, stenosed anus,
mem%ranous anus, rectal atresia or e+ennormal anusDDD
*he most important in+estigation is the
in+ertogramIt is +ery important to rule out other
anomalies*he %est 7 the newest operation is S"#
-
7/24/2019 ANORECTAL MALFORMATION.ppt
39/40
i%liography1/ $arlow (/# and #edding /"/ *et%ook of
edatric Bursing/ th
Edition/ p: /./(onna C Gong/ Essentials of ediatricBursing/ 5thEdition/ p: J45;J4K
)/Lliegman and et al&.00K'M Belson *et%ook of
ediatricsM 1Jth editionM pages: 1)5;)N/
-
7/24/2019 ANORECTAL MALFORMATION.ppt
40/40
THA6781*THA6781*