ANNALS Celiac Disease

of 16
Transcript of ANNALS Celiac Disease
-
7/29/2019 ANNALS Celiac Disease
1/16
-
7/29/2019 ANNALS Celiac Disease
2/16
The risk for celiac disease is be-
tween 5% to 10% in newborn chil-dren of parents with the diseaseand 10% to 20% of siblings. Breast-feeding and delaying the introduc-tion of gluten into the diet of theimmunologically immature infantgut might prevent or delay glutensensitization (6, 7). Population-based studies have shown an in-crease in celiac disease autoimmu-nity in infants ingesting glutenduring the first 3 months, and
decreased rates when gluten is re-
moved from infant diets (8).Whether the lifetime risk for celiacdisease is reduced or merely delayedby reduced gluten ingestion ininfancy is unknown. Current rec-ommendations are to begin intro-ducing gluten into the diet of agenetically susceptible infant at 4 to6 months of age while the mothercontinues to breastfeed (9), but on-going studies will hopefully deter-mine the optimum practice.
2011 American College of Physicians ITC5-2 In the Clinic Annals of Internal Medicine 3 May 2011
1. Fasano A, Berti I, Ger-arduzzi T, et al. Preva-lence of celiac dis-ease in at-risk andnot-at-risk groups inthe United States: a
large multicenterstudy. Arch InternMed. 2003;163:286-92. [PMID: 12578508]
2. Kagnoff MF. Celiacdisease: pathogenesisof a model immuno-genetic disease. J ClinInvest. 2007;117:41-9.[PMID: 17200705]
3. Rubio-Tapia A, KyleRA, Kaplan EL, et al.Increased prevalenceand mortality in un-diagnosed celiac dis-ease. Gastroenterolo-gy. 2009;137:88-93.[PMID: 19362553]
4. Ludvigsson JF, Mont-gomery SM, EkbomA, Brandt L, Granath F.Small-intestinalhistopathology andmortality risk in celiacdisease. JAMA.2009;302:1171-8.[PMID: 19755695]
5. Catassi C, Bearzi I,Holmes GK. Associa-tion of celiac diseaseand intestinal lym-phomas and othercancers. Gastroen-terology.2005;128:S79-86.[PMID: 15825131]
6. Ivarsson A, Hernell O,Stenlund H, PerssonLA. Breast-feeding
protects against celi-ac disease. Am J ClinNutr. 2002;75:914-21.[PMID: 11976167]
7. Akobeng AK, Ra-manan AV, Buchan I,Heller RF. Effect ofbreast feeding on riskof coeliac disease: asystematic reviewand meta-analysis ofobservational studies.Arch Dis Child.2006;91:39-43.[PMID: 16287899]
8. Norris JM, Barriga K,Hoffenberg EJ, et al.Risk of celiac diseaseautoimmunity andtiming of gluten in-
troduction in the dietof infants at in-creased risk of dis-ease. JAMA.2005;293:2343-51.[PMID: 15900004]
9. Guandalini S. Risk ofceliac disease au-toimmunity and tim-ing of gluten intro-duction in the diet ofinfants at increasedrisk of disease. J Pedi-atr GastroenterolNutr. 2005;41:366-7.[PMID: 16131999]
Celiac disease, also known as gluten-sensitive enteropathy (as well as twoolder and less preferred terms, nontropical sprue and celiac sprue) is amultisystem disorder estimated to affect approximately 1% of Americans
(1). It results from an inappropriate T-cellmediated immune response to ingestedgluten that causes inflammatory injury to the small intestine in genetically predis-posed persons. Damage to the proximal small intestinal mucosa results in themalabsorption of nutrients. The average age of diagnosis is in the fifth decade oflife but only an estimated 10% to 15% of persons with celiac disease in the UnitedStates have been diagnosed (2). The prevalence of celiac disease in the United
States seems to have increased 4- to 5-fold over the past 3 to 4 decades (3). Dis-ease manifestations are protean, and gastrointestinal symptoms are not alwayspresent. Virtually every body system can be affected, with dermatologic, hemato-logic, neurologic, musculoskeletal, endocrine, reproductive, and digestive systemsmost commonly involved. Moreover, celiac disease is associated with a variety ofautoimmune conditions whose clinical course may be affected by the diagnosisand treatment of celiac disease. Although patients respond well to treatment witha gluten-free diet, unrecognized or untreated celiac disease is associated with bothincreased mortality (3, 4) and risk for intestinal lymphoma (5).
Prevention
Screening [11] and Turner [12] syndromes) arealso candidates for screening (Box:Symptoms and Conditions ThatShould Prompt Consideration ofCeliac Disease). Individual patientsshould be tested only if the patientis willing to undergo endoscopywith intestinal biopsies if necessaryfor disease confirmation and embarkupon treatment with a gluten-freediet. The role of widespread popula-
tion screening remains controversial.
Patients with certain autoimmunedisorders seem to be at increased riskfor celiac disease. Three to seven per-cent of children and adults with pri-mary biliary cirrhosis or autoimmunehepatitis have concomitant celiacdisease (13), which may contribute togastrointestinal symptoms, including
Which patients should be screened?
Screening is recommended when afirst-degree family member or otherclose relative has biopsy-confirmedceliac disease. Inherited HLA-DQ2and/or HLA-DQ8 genes are neces-sary but not sufficient for celiac dis-ease to develop. The absence ofHLA-DQ2 and HLA-DQ8 has ahigh negative predictive value for di-agnosing celiac disease (10), which
is useful in selecting family memberswho require additional screeningand prevention strategies. Individu-als with autoimmune diseases shar-ing these HLA susceptibility geneswith celiac disease (e.g., type 1 dia-betes mellitus and autoimmune thy-roid and hepatobiliary disorders)and conditions known to be associ-ated with celiac disease (e.g., Down
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
3/16
2011 American College of PhysiciansITC5-3In the ClinicAnnals of Internal Medicine3 May 2011
diarrhea, lactose intolerance, bloating,weight loss, and steatorrhea.
Screening for celiac disease shouldbe considered in patients with type 1diabetes mellitus, particularly thosewith gastrointestinal symptoms orfrequent hypoglycemic episodes,although the benefit of screening
diabetic patients without such symp-toms is unclear. Three to seven per-cent of patients with type 1 diabetesmellitus have subclinical celiac dis-ease, and this may also contribute topoor glycemic control and failure tothrive (14). Treatment may reducerisk for osteoporosis or cancer laterin life, and some studies suggest animprovement in glycemic control.
Two to five percent of patients withautoimmune hypo- or hyperthy-roidism have celiac disease, and ad-herence to a gluten-free diet mayhelp manage the endocrinopathy.Celiac disease prevalence is increasedin many other autoimmune diseases,including the Sjgren syndrome, mi-croscopic colitis, and other forms ofinflammatory bowel disease and var-ious connective tissue disorders.
How should screening be done?Serum IgA antibodies to tissue
transglutaminase (tTG), a ubiquitousenzyme also called transglutaminase2 (TG2), are increased in most casesof active celiac disease, and testingfor these antibodies is the recom-mended screening procedure in olderchildren and adults (15). One excep-tion is that patients with IgA defi-ciency should be screened with anIgG test if available (see Diagnosis).
A recent meta-analysis reported that the anti-tTG IgA serum antibody marker had high sen-
sitivity (89%) and very high specificity (98%)for celiac disease in patients with abdominalsymptoms (16). A related antibody, antien-domysial IgA antibody, detecting the sametTG protein as tTG antibodies by immunoflu-orescence assay, was reported to have a simi-lar sensitivity (90%) and specificity (99%) (16).
Antibodies to gliadin were previouslyused to screen for celiac disease butare no longer recommended in
adults because of the low sensitivitiesand specificities of both antibodiesto gliadin IgA and IgG (15). Re-cently available tests for IgG andIgA antibodies to deamidatedgliadin peptide were initially report-ed to match the performance ofanti-tTG/antiendomysial IgA anti-body tests in some studies, and were
even believed to increase the diag-nostic sensitivity and specificity forceliac disease (17). However, a recentmeta-analysis indicates that deami-dated gliadin peptide is less sensitivethan tTG IgA (18).
The recommended screening testfor relatives of patients with celiacdisease is polymerase chain reactiontesting of a blood sample or acheek swab for HLA DQ2 orHLA DQ8 (Box: HLA DQ2 andHLA DQ8 Testing).
Persons who are positive for eitherHLA DQ2 or HLA DQ8 shouldthen have serum tTG IgA screen-ing. tTG IgA testing in geneticallyat-risk children should begin after2 years of age and following at least1 year of a wheat-containing diet orwith suggestive signs or symptoms.Previous guidelines recommendedtesting children with a family histo-
ry with tTG IgA every 3 years;however, this is now considered un-necessary unless they have HLADQ2 or DQ8 genes. Because celiacdisease can develop at virtually anytimewith an average age of diag-nosis in the fifth decade of lifeidentifying family members who areactually at risk for celiac disease by
Symptoms and Conditions That
Should Prompt Consideration of
Celiac Disease
First- and second-degree relatives withceliac disease
Gastrointestinal symptoms
Irritable bowel syndromelikesymptoms
Heartburn Dyspepsia Diarrhea Altered bowel habits Bloating Lactose intolerance
Extraintestinal presentations
Dermatitis herpetiformis Iron deficiency Folate deficiency Osteopenic bone disease Chronic fatigue Neuropsychiatric manifestations Short stature Infertility Recurrent fetal loss Low birthweight
Autoimmune endocrine disorders Type 1 diabetes mellitus Autoimmune thyroid disease Autoimmune adrenal disease
Autoimmune connective tissue disorders
The Sjgren syndrome Rheumatoid arthritis Systemic lupus erythematosus
Hepatobiliary conditions
Primary sclerosing cholangitis Primary biliary cirrhosis Autoimmune cholangitis Elevated transaminase levels
Other inflammatory luminalgastrointestinal disorders
Lymphocytic gastritis Microscopic colitis Inflammatory bowel disease
Miscellaneous conditions
IgA deficiency IgA nephropathy The Down syndrome The Turner syndrome
HLA DQ2 and HLA DQ8 Testing
How to test:
Polymerase chain reaction of RNA extracted from cells in a cheek swab or blood sampleWhom to test:
Close relatives of patients with confirmed celiac disease who want to know if they areat risk
Patients on a gluten-free diet who are candidates to undergo a gluten challenge toconfirm possible celiac disease; only genetically susceptible patients at risk for celiacdisease should be challenged
Equivocal histologic and serologic findings in which a negative test result would makeceliac disease highly unlikely
How often to test:
Once in a lifetime
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
4/16
10. Pietzak MM,Schofield TC, McGin-niss MJ, NakamuraRM. Stratifying riskfor celiac disease ina large at-risk UnitedStates population byusing HLA alleles.Clin G astroenterolHepatol. 2009;7:966-71. [PMID: 19500688]
11. Nisihara RM, KotzeLM, Utiyama SR,Oliveira NP, FiedlerPT, Messias-ReasonIT. Celiac disease inchildren and adoles-cents with Downsyndrome. J Pediatr(Rio J). 2005;81:373-6. [PMID: 16247538]
12. Bonamico M,Pasquino AM, Mari-ani P, et al; Italian So-ciety Of PediatricGastroenterologyHepatology (SIGEP).Prevalence and clini-cal picture of celiacdisease in Turnersyndrome. J Clin En-docrinol Metab.2002;87:5495-8.[PMID: 12466343]
13. Dickey W, McMillan
SA, Callender ME.High prevalence ofceliac sprue amongpatients with pri-mary biliary cirrhosis.J Clin Gastroenterol.1997;25:328-9.[PMID: 9412913]
14. Mohn A, Cerruto M,Iafusco D, et al. Celi-ac disease in chil-dren and adoles-cents with type Idiabetes: impor-tance of hypo-glycemia. J PediatrGastroenterol Nutr.2001;32:37-40.[PMID: 11176322]
2011 American College of Physicians ITC5-4 In the Clinic Annals of Internal Medicine 3 May 2011
Diagnosiscommonly encountered. Steator-rhea is relatively uncommon, butapproximately half of celiac patientshave lactose intolerance at the timeof presentation. Maldigestion ofsugars may cause postprandialbloating, flatulence, and diarrhea.
Although not advised with typicalirritable bowel syndrome (IBS), pa-tients with diarrhea-predominant IBSor mixed-type IBS should have sero-logic testing for celiac disease (19).
A recent systematic review and meta-analysis of 14 studies found that the likeli-
hood of biopsy-proven celiac disease in
patients meeting criteria for IBS was in-
creased more than 4-fold compared with
non-IBS controls (20). Whether such find-
ings truly reflect an increased associationbetween these 2 clinical entities remains a
matter of debate.
Iron deficiency is common in celiacdisease and is often seen in newly di-agnosed patients. When patients re-ferred for upper endoscopy as part ofthe investigation of iron deficiencyanemia are examined for celiac dis-ease by duodenal biopsies, 6% to10% will have celiac disease even inthe absence of other signs and
What signs and symptoms shouldlead clinicians to consider adiagnosis of celiac disease?Celiac disease may affect multipleorgan systems and may have proteanmanifestations. More commonly rec-ognized gastrointestinal symptomsinclude diarrhea (occurring in ap-proximately 50% of patients), altered
bowel habits, flatus, dyspepsia, heart-burn, and weight loss. Less readilyrecognized manifestations mayinclude headaches, depression, pares-thesia, joint symptoms, rashes, fa-tigue, miscarriages, and many others.Except for the dermatitis herpeti-formis rash, celiac disease is usuallynot associated with specific physicalsigns, and physical examination maynot yield specific findings. Patientswith severe forms of celiac diseasemay have nonspecific findings, al-though only a small subset of pa-tients currently has such severe man-ifestations at the time of diagnosis(Box: Physical Findings in PatientsWith Severe Celiac Disease).
Diarrhea is a common presentingsymptom of the more classicalform of celiac disease, althoughatypical forms are now more
Screening... Serologic testing for celiac disease should be considered in relatives ofpersons with proven celiac disease and in those with such conditions as type 1 dia-betes mellitus, autoimmune thyroid disease, autoimmune hepatobiliary diseases, anda number of other autoimmune diseases. Screening persons with the Down or Turn-er syndrome has also been recommended. In these patients, tTG IgA should be usedto screen adults and older children, unless there is IgA deficiency, in which IgG test-ing should be used if available. All persons with a positive tTG antibody screeningtest should undergo definitive diagnostic testing. Close relatives of patients withceliac disease should first have polymerase chain reaction testing for HLA DQ2 orHLA DQ8 to identify those at risk and the need for serum testing. As celiac diseasemay not manifest until later in life, repeated serum tTG IgA testing may be required,as initial negative test results do not preclude the possibility of future development.The optimal frequency of subsequent testing has not been determined.
CLINICAL BOTTOM LINE
Physical Findings in Patients With
Severe Celiac Disease
Muscle wasting
Loss of adipose tissue
Pallor of anemia
Bruising
Edema (due to hypoproteinemia)
Stomatitis
Aphthoid ulceration of the oral mucosa
Cheilosis
Vertebral fractures and limb girdleweakness and pain (osteoporosis orosteomalacia)
Postural hypotension from dehydration
Tetany (Trousseau or Chvostek signs)
Finger clubbing
Protuberant abdomen (more common inchildren; rare in adults)
Short stature
Dental enamel defects
in patients with an autoimmunedisorder at increased risk (e.g., pri-mary biliary cirrhosis, type 1 dia-betes, autoimmune hepatitis, or thy-roid disease) when endoscopy isbeing done for another reason.
using HLA DQ testing is recom-mended to prevent unnecessarytTG IgA testing in those with vir-tually no risk. In addition to sero-logic testing, duodenal biopsiesshould be considered for screening
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
5/16
15. Rostom A, Dub C,Cranney A, et al. Thediagnostic accuracyof serologic tests forceliac disease: a sys-tematic review. Gas-troenterology.2005;128:S38-46.[PMID: 15825125]
16. van der Windt DA,Jellema P, Mulder CJ,Kneepkens CM, vander Horst HE. Diag-nostic testing forceliac diseaseamong patients withabdominal symp-toms: a systematicreview. JAMA.
2010;303:1738-46.[PMID: 20442390]
17. Kaukinen K, Collin P,Laurila K, Kaartinen
T, Partanen J, MkiM. Resurrection ofgliadin antibodies incoeliac disease.Deamidated gliadinpeptide antibodytest provides addi-tional diagnosticbenefit. Scand J Gas-troenterol.2007;42:1428-33.[PMID: 17852878]
2011 American College of PhysiciansITC5-5In the ClinicAnnals of Internal Medicine3 May 2011
symptoms (21). Celiac diseaseshould be considered in menstruat-ing women as well as in individualsyounger than 50 years with unex-plained iron deficiency, especially ifthey are resistant to oral iron supple-mentation. Patients older than 50years with unexplained iron deficien-cy anemia should be referred for gas-
trointestinal testing, including upperendoscopy and duodenal biopsies.
Celiac disease can result in vitaminD and calcium malabsorption, andpatients with unexplained metabol-ic bone disease or severe osteopo-rosis should be assessed for celiacdisease, even in the absence of gas-trointestinal symptoms. This ap-plies especially to osteomalacia orreduced bone density at a young
age, or males who develop osteo-porosis. A gluten-free diet correctsbone loss in patients with mild dis-ease and provides significant ame-lioration in patients with severemalabsorption. Diminished bonedensity is associated with increasedrisk for fractures in patients withceliac disease (22). A gluten-freediet reduces the risk for fractures.
An evaluation for celiac diseasestarting with serologic tests shouldbe considered in women and menwith unexplained infertility andwomen with recurrent spontaneousabortion. The mechanism of theseproblems may be abnormal hormonelevels, general malnutrition, or otherautoimmune disorders (23). Preg-nancy in women with untreatedceliac disease may result in small-for-gestational age babies and in-trauterine growth restriction (23-25).Treating celiac disease seems to im-
prove fertility in men and womenand pregnancy outcomes (23, 26), al-though systematic follow-up studieshave not been done.
Axonal neuropathy and cerebellarataxia are among the more commonextraintestinal symptoms associatedwith celiac disease (27) and havebeen associated with elevated levels
of antigliadin antibodies, even whenpathologic mucosal characteristicsare lacking. Migraine headaches, de-pression, behavioral disorders,autism, and other neurologic or psy-chiatric conditions have been report-ed, but there is no proof that celiacdisease is causal in most of theseconditions (28). As some patients
have been reported to respond to agluten-free diet, serologic assessmentfor celiac disease should be consid-ered in idiopathic peripheral neurop-athy or cerebellar ataxia.
What is the significance ofdermatitis herpetiformis in patientswith suspected celiac disease?Dermatitis herpetiformis is anuncommon but characteristicpapulovesicular rash affecting the ex-
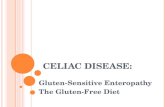
tensor surfaces of the elbows, knees,and trunk; the rash is intensely pru-ritic (Figure 1). Although intestinalbiopsies of patients with this disor-der are indistinguishable from thosewith celiac disease (29), typicalsymptoms of malabsorption are of-ten absent when the skin disease ispresent. Dermatitis herpetiformis isan immunologic response to intes-tinal gluten sensitivity, but the rela-tionship is frequently not recognized,and treatment of the dermatologicproblem alone is often pursued withsuppressive therapy, such as dapsone.As a result, the underlying cause ofthe rash is not addressed, leaving thepotential for other symptoms to de-velop later as well as the malignantconsequences of untreated intestinalinflammation (30). Dermatitis her-petiformis should prompt a derma-tologic consultation to obtain skinbiopsies of perilesional areas for his-tologic and immunofluorescence
staining. Granular IgA deposits atthe dermalepidermal junction of af-fected skin are characteristic. Whenskin biopsy confirms the diagnosis,intestinal biopsies are not needed.Dermatitis herpetiformis is the resultof intestinal gluten sensitivity (as op-posed to a direct dermal response),and despite Web sites and other re-sources instructing patients with
Figure 1. Dermatitis herpetiformis. This dis-order is an intensely pruritic papulovesicularrash affecting extensor surfaces, such as theshoulders (top), elbows, knees, back, and but-tocks (bottom). Although all patients withdermatitis herpetiformis have the intestinallesions of celiac disease, few have gastro-intestinal symptoms. Immunofluorescentdetection of IgA deposits at the dermalepidermal junction in a perilesional biopsy of afresh skin lesion is sufficient for diagnosis andprecludes the need for intestinal biopsies.
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
6/16
18. Lewis NR, Scott BB.Meta-analysis:deamidated gliadinpeptide antibodyand tissue transglut-aminase antibody
compared as screen-ing tests for coeliacdisease. AlimentPharmacol Ther.2010;31:73-81.[PMID: 19664074]
19. Brandt LJ, BjorkmanD, Fennerty MB, et al.Systematic reviewon the managementof irritable bowelsyndrome in NorthAmerica. Am J Gas-troenterol. 2002;97(11 Suppl):S7-26.[PMID: 12425586]
2011 American College of Physicians ITC5-6 In the Clinic Annals of Internal Medicine 3 May 2011
celiac disease and dermatitis herpeti-forms to avoid lotions and other top-ically applied products containinggluten, only ingested gluten willcause problems. A lifelong gluten-free diet is recommended, even inpatients whose dermatologic diseasehas responded to dapsone or sulfa-pyridine (31).
What other diagnoses shouldclinicians consider?Many conditions can be confusedwith celiac disease. These includesuch common disorders as intoler-ance to lactose and other carbohy-drates, functional gastrointestinaldisorders, idiopathic inflammatorydisorders of the intestine (inflamma-tory bowel diseases), other food pro-teinmediated conditions (hypersen-sitivity, protein enteropathies), andmalabsorptive disorders (Box: Con-ditions or Disorders to Consider).
What blood tests should be sentto evaluate a patient withsuspected celiac disease?Serum anti-tTG IgA should bemeasured to assess clinically sus-pected celiac disease and to deter-mine which patients should haveintestinal biopsy (15, 32). Measure-ments of other antibodies are not
routinely recommended for diagno-sis, although antideamidatedgliadin peptide testing is now morewidely available. As with screening,if the results of anti-tTG or en-domysial antibody or antideami-dated gliadin peptide antibody testsare positive, or if results are nega-tive when clinical suspicion is high,intestinal biopsies should be ob-tained. Although the absence ofHLA DQ2 or DQ8 makes celiacdisease highly unlikely (with a neg-ative predictive value of 100%),adding this test to either TTG IgAor endomysial IgA antibody meas-urement does not change test per-formance, underscoring that HLAtesting does not play a role in diag-nosing celiac disease (33).
Anti-tTG IgA testing is not helpfulin evaluating possible celiac disease
in patients with IgA deficiency. Se-lective IgA deficiency affects 1 in500 to 700 persons in the generalpopulation and is found in about2% to 5% of celiac patients, whichmay cause false-negative results onserologic testing. In addition, celiacdisease is more common in patientswith selective IgA deficiency (34).
An IgG-based serologic test (e.g.,antideamidated gliadin peptideIgG, anti-tTG IgG, and AGAIgG), and if not already assessed,measurement of the total IgA level,should be obtained if the tTG IgAvalues are in the low-normal rangeor are negative. tTG IgG antibodiesare usually positive in IgA-deficientpatients with celiac disease (35). Ifresults of IgA or IgG tests are posi-tive, an endoscopy with biopsies
should be done. Other blood testingin suspected cases of celiac diseaseshould look for disease complica-tions, including vitamin and miner-al deficiencies, anemia, electrolyteimbalances, elevated transaminases,and coagulopathies.
Wheat allergy skin testing cannotbe used to diagnose celiac disease.Celiac disease is not an IgE-mediated allergic condition, and
wheat allergy is very different fromceliac disease; therefore, wheat al-lergy tests are not relevant.
What is the role of endoscopy inthe evaluation of a patient with
possible celiac disease?Endoscopy is used primarily toconfirm the diagnosis by obtainingbiopsies of the proximal small intes-tine in patients with positive serolog-ic test results or there is high clinicalsuspicion of celiac disease in the
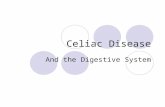
absence of positive serologic test re-sults. A pattern visible on endoscopicexamination, including scalloping ornotching of mucosal folds, is quitespecific for the disease (Figure 2)and suggests the diagnosis to thetrained endoscopist (36). However,endoscopic changes have low sensi-tivity and biopsies should be ob-tained in their absence (37).
Conditions or Disorders to Consider
in the Diagnosis of Celiac Disease
The irritable bowel syndrome
Inflammatory bowel diseases
Microscopic colitis
Lactose intolerance
Other carbohydrate intolerances
Eosinophilic gastroenteritis
Food proteininduced enteropathies
Small intestinal bacterial overgrowth
Giardia infection
Pancreatic insufficiency
Intestinal lymphoma
IgA deficiency
Common variable immunodeficiency
Autoimmune enteropathy
Note: Some of these conditions cancoexist with or complicate celiacdisease.
Figure 2. Endoscopic appearance of celiacdisease. Such features include scalloping or
notching of the folds, as shown. Fissuring orcracking of the flat intervening mucosabetween the folds can also be seen. Theseendoscopic features are helpful for targetingbiopsy sites, but their absence does notrule out the diagnosis; as such, intestinalbiopsies should be obtained during upperendoscopy for evaluation of potentialceliac disease.
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
7/16
20. Ford AC, Chey WD,Talley NJ, MalhotraA, Spiegel BM,Moayyedi P. Yield ofdiagnostic tests forceliac disease in in-dividuals with symp-toms suggestive ofirritable bowel syn-drome: systematicreview and meta-analysis. Arch InternMed. 2009;169:651-8. [PMID: 19364994]
21. Ackerman Z, EliakimR, Stalnikowicz R,Rachmilewitz D. Role
of small bowel biop-sy in the endoscopicevaluation of adultswith iron deficiencyanemia. Am J Gas-troenterol.1996;91:2099-102.[PMID: 8855729]
22. Vasquez H, MazureR, Gonzalez D, et al.Risk of fractures inceliac disease pa-tients: a cross-sec-tional, case-controlstudy. Am J Gas-troenterol.2000;95:183-9.[PMID: 10638580]
23. Soni S, Badawy SZ.Celiac disease and
its effect on humanreproduction: a re-view. J Reprod Med.2010;55:3-8.[PMID: 20337200]
24. Tata LJ, Card TR, Lo-gan RF, Hubbard RB,Smith CJ, West J. Fer-tility and pregnancy-related events inwomen with celiacdisease: a popula-tion-based cohortstudy. Gastroenterol-ogy. 2005;128:849-55. [PMID: 15825068]
2011 American College of PhysiciansITC5-7In the ClinicAnnals of Internal Medicine3 May 2011
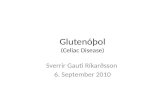
Small intestinal biopsies show vary-ing degrees of villous blunting andlymphocytic and plasma cell infil-trates (Figure 3). Although notpathonomic for celiac disease, thesefindings are highly predictive of aresponse to a gluten-free diet. Biop-sies must be carefully evaluated tohelp differentiate celiac from other
conditions, such as peptic duodeni-tis, the effects of nonsteroidal anti-inflammatory drugs, tropical sprue,radiation damage, recent chemo-therapy, graft-versus-host disease,chronic ischemia, severe giardiasis,Crohn disease, common variableimmunodeficiency, and autoim-mune and other enteropathies (38).A pathologist with expertise in gas-trointestinal diseases should ideallyexamine the biopsy slides, especially
if the diagnosis is uncertain.
How can a patient already on agluten-free diet be diagnosed?An empirical trial of a gluten-freediet without a biopsy-establisheddiagnosis of celiac disease is notrecommended because a beneficialresponse may be seen in other dis-orders. Many dietary componentsin addition to gluten are typicallyeliminated in a gluten-free diet,
which also provides symptom reliefin such functional gastrointestinaldisorders as IBS, gastroesophagealreflux disease, and functional dys-pepsia. In one study, the positivepredictive value of a beneficial re-sponse resulting from celiac diseasewas only 36% (39). Differentiatingbetween celiac disease and otherdisorders that may respond to agluten-free diet is important to helpdetermine whether life-long dietarychanges are required and because ofthe implications for long-termmanagement and risk assessment ofrelatives if celiac disease is present.
Many patients initiate a gluten-freediet before appropriate diagnostictesting. In such cases, the effect ofgluten withdrawal on the accuracyof diagnostic serologic testing orbiopsies depends on the duration of
the gluten-free diet, the degree towhich gluten has been avoided, andthe severity of the underlying dis-ease. For example, up to 2 monthsof a partially gluten-free diet is un-likely to affect the findings of an in-testinal biopsy or a sensitive tTGassay in a patient with a severe mal-absorptive presentation. The histo-logic abnormalities often takemonths and even years to return tonormal on a gluten-free diet. It istherefore reasonable to obtain sero-logic studies for celiac disease at thefirst visit, even if the patient reportsa gluten-free diet. If tTG IgA is el-evated, an intestinal biopsy shouldbe obtained; if it is not (and lack ofelevation is not attributable to IgAdeficiency), further diagnostic test-ing may be deferred until gluten has
been reintroduced into the diet for asufficient duration to reproduce theserologic abnormality and the char-acteristic intestinal damage.
Initial HLA DQ2/DQ8 testing isnow recommended, and a glutenchallenge should be performed onlyin persons genetically susceptible toceliac disease. Because a severe reac-tion to a gluten challenge may occurin some patients, a gradual increase
in gluten may be advised. Patientsshould be challenged for 3 to 4weeks with enough gluten to pro-duce symptoms (an average of 3 to 4slices of whole wheat bread per day).If symptoms do not recur, develop-ment of antibodies may be used toguide the timing of intestinal biopsy,although data are insufficient andthere are no specific guidelines re-garding the use of antibody testingin such cases. If there are no clinical
symptoms or characteristic serology(anti-tTG or antiendomysial anti-body) with the initial gluten chal-lenge, it should be continued for atleast 3 to 6 months and intestinalbiopsies should be obtained. Patientswho have followed a gluten-free dietfor prolonged periods may take sev-eral years to relapse after gluten isreintroduced.
Figure 3. Histologic appearance of celiacdisease. Characteristic features of the intes-tinal mucosa in celiac disease include in-flammation and varying degrees of villousatrophy. Inflammation comprises lympho-cytes, plasma cells, macrophages, and otherchronic inflammatory cells in the laminapropria. It also includes intraepithelial lym-phocytes, which are more prominent towardthe tips of the villi. The biopsy depicted hereshows partial villous atrophy with charac-teristic inflammatory changes.
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
8/16
25. Ludvigsson JF,Montgomery SM, Ek-bom A. Celiac dis-ease and risk of ad-verse fetal outcome:a population-basedcohort study. Gas-troenterology.2005;129:454-63.[PMID: 16083702]
26. Farthing MJ, ReesLH, Edwards CR,Dawson AM. Malegonadal function incoeliac disease: 2.Sex hormones. Gut.1983;24:127-35.[PMID: 6682819]
27. Sander HW, MagdaP, Chin RL, et al.Cerebellar ataxia andcoeliac disease.Lancet.2003;362:1548.[PMID: 14615111]
28. Bushara KO. Neuro-logic presentation ofceliac disease. Gas-troenterology.2005;128:S92-7.[PMID: 15825133]
29. Primignani M, AgapeD, Ronchi G, et al.Prevalence of duo-denal and jejunal le-
sions in dermatitisherpetiformis. RicClin Lab.1987;17:243-9.[PMID: 3671997]
30. Askling J, Linet M,Gridley G, Hal-stensen TS, EkstrmK, Ekbom A. Cancerincidence in a popu-lation-based cohortof individuals hospi-talized with celiacdisease or dermatitisherpetiformis. Gas-troenterology.2002;123:1428-35.[PMID: 12404215]
31. Garioch JJ, LewisHM, Sargent SA,
Leonard JN, Fry L. 25years experience ofa gluten-free diet inthe treatment ofdermatitis herpeti-formis. Br J Derma-tol. 1994;131:541-5.[PMID: 7947207]
2011 American College of Physicians ITC5-8 In the Clinic Annals of Internal Medicine 3 May 2011
It is not clear how to manage pa-tients who improve on a gluten-freediet but are not genetically suscepti-ble to celiac disease or those whohave HLA susceptibility genes butdo not develop antibodies or intes-tinal lesions after gluten challenge.A growing population is gluten-sensitive, meaning that they im-
prove on a gluten-free diet. Thisgroup encompasses persons withceliac disease (both diagnosed andundiagnosed) and an unknownnumber with so-called gluten-sensitivity without celiac disease.Gluten sensitivity is ill-defined
because currently there are no crite-ria to define this disorder. To whatdegree gluten-sensitive persons whodo not have celiac disease shouldadhere to a gluten-free diet is alsonot known. It is common practice toadvise gluten-sensitive adults with-out the HLA genes that predisposeto celiac disease to remain on a
gluten-free diet to an extent suffi-cient to control symptoms andmaintain good health; otherwisetheir diets may be unnecessarily re-stricted. Further studies are neededto guide medical practice for thisemerging clinical entity.
Diagnosis... Celiac disease should be considered in a wide variety of clinicalpresentations that may manifest from malabsorption, including gastrointestinaland nongastrointestinal syndromes, such as endocrine and bone diseases. Celiacdisease may mimic common conditions, such as IBS and dyspepsia. Dermatitis
herpetiformis, while characteristic, is rare. Celiac disease is diagnosed by the pres-ence of tTG antibodies in the serum; characteristic histologic findings on intestin-al biopsies; and observing the expected clinical, serologic, and in some caseshistologic response to a gluten-free diet (40).
CLINICAL BOTTOM LINE
Indications for Admission to
Hospital
Acutely ill patients needing rehy-
dration and/or parenteral nutri-tional support
Presence of tetany, frank dehy-dration, severe electrolyte disor-ders, or severe malnutrition
Weight loss of more than 10%of body weight in a short period
Refractory celiac disease beingtransitioned from parenteral nutri-tion to enteral tube-feeding withconcern for relapse and severediarrhea and malabsorption
Treatmenteven small amounts of glutenaslittle as 50 mg/dmay result in thereturn of symptoms in previouslywell-controlled cases (41) and may be
associated with histologic changes ofthe small bowel, even in the absenceof overt clinical symptoms.
A systematic review provides evidence thatadherence to a gluten-free diet and mu-cosal healing prevent or ameliorate thecomplications of celiac disease (42). Theauthors suggest that long-term follow-upis essential, but they acknowledge that theevidence is limited. In general, outcomestudies of celiac disease are limited by theirretrospective nature and the inherent diffi-culty of assessing compliance.
Even though symptoms often re-solve within days or weeks of theonset of treatment, damage willrecur if gluten is reintroduced intothe diet because immunologic intol-erance to gluten does not go away.Patients may incorrectly believe thatthe absence of noted symptomswhen eating gluten-containing food
When should patients behospitalized?Hospitalization is rarely requiredfor celiac disease but may be neces-
sary when severe malabsorption hasresulted in fluid or electrolyte ab-normalities in need of short-termtreatment. Closer monitoring mayalso be required in some patientswith severe disease when enteralfeeding is resumed (Box: Indica-tions for Admission to Hospital).
What is the importance of diet?A gluten-free diet is the cornerstoneof therapy for celiac disease. Removalof the antigenic substance responsible
for the abnormal immune responseand enteropathy nearly always revers-es disease manifestations, includingdermatitis herpetiformis. However,the diet is complex and has manypotential pitfalls. Patient motivationand education are crucial, particularlybecause there is no alternative treat-ment. Noncompliance is common,especially in adolescents. Ingestion of
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
9/16
32. Catassi C, Kryszak D,Louis-Jacques O, etal. Detection of celi-ac disease in primarycare: a multicentercase-finding study inNorth America. Am JGastroenterol.2007;102:1454-60.[PMID: 17355413]
33. Hadithi M, vonBlomberg BM, Cru-sius JB, et al. Accura-
cy of serologic testsand HLA-DQ typingfor diagnosing celiacdisease. Ann InternMed. 2007;147:294-302.[PMID: 17785484]
34. Richter D. Celiac dis-ease and IgA defi-ciency [Letter]. Pedi-atr Allergy Immunol.2004;15:191.[PMID: 15059200]
35. Korponay-Szab IR,Dahlbom I, Laurila K,et al. Elevation ofIgG antibodiesagainst tissue trans-glutaminase as a di-agnostic tool for
coeliac disease in se-lective IgA deficien-cy. Gut.2003;52:1567-71.[PMID: 14570724]
36. Oxentenko AS,Grisolano SW, Mur-ray JA, Burgart LJ,Dierkhising RA,Alexander JA. The in-sensitivity of endo-scopic markers inceliac disease. Am JGastroenterol.2002;97:933-8.[PMID: 12003429]
2011 American College of PhysiciansITC5-9In the ClinicAnnals of Internal Medicine3 May 2011
supplementation, should be encour-aged. Lactose intolerance shouldresolve with intestinal recovery re-sulting from the gluten-free diet;however, lactase insufficiency iscommon in many races worldwide,and in such cases, low-lactose dairyproducts and lactase supplementsare required long-term. Patients
must be instructed not to avoid alldairy productsmany of them, in-cluding hard cheeses, yogurt, andother fermented milk products, arenaturally low in lactose.
Celiac disease can lead to malab-sorption of fat-soluble vitamins (D,E, A, and K) as well as folic acidand iron, which are preferentiallyabsorbed through the proximalsmall intestine. Deficiencies of thi-amin, B
6, and B
12, may occur but
are less common. Certain minerals,including magnesium, copper, zinc,and selenium, can be low depend-ing on disease severity and dietaryintake. Vitamin and mineral re-placement is typically recommend-ed in addition to a gluten-free dietuntil the intestine has healed andpreviously low levels are replete.
How should patients be monitored?Although evidence-based guidelinesfor follow-up and lifelong manage-ment are lacking, follow-up within afew weeks of diagnosis to discuss theintestinal biopsy results and othertests is recommended. At that time,the diagnosis of celiac disease is dis-cussed along with answering ques-tions and evaluating disorders thatmay complicate the disease, such asnutritional deficiencies and osteo-porosis. Ideally, a visit with an expertdietitian should be scheduled for thesame day or very soon thereafter. As
recommended by the AGA (40), fol-low-up is necessary to confirm thediagnosis by an objective response toa gluten-free diet and to assess di-etary compliance. Typically, clinical,laboratory, and serologic responsesto dietary therapy are sufficient togauge the response. Patients shouldbe evaluated at regular intervals bya health care team, including a
indicates that it can be consumedwithout harm. Accordingly, patientsshould be actively encouraged tostrictly adhere to the diet to avoidsuch complications as bone loss andincreased risk for cancer. The mostrecent medical position statement onthe diagnosis and management ofceliac disease published by the
American Gastroenterological Asso-ciation (AGA) recommends lifelongadherence to a gluten-free diet as thetreatment of choice for celiac disease(40). Although dapsone may managethe dermatitis herpetiformis, it doesnot ameliorate intestinal mucosal in-jury. A gluten-free diet is required.
What specific dietaryrecommendations should be made?Eating gluten-free processed foodscombined with gluten-free flours
that were not vitamin-enrichedprobably contributes to nutritiondeficiencies (e.g., in iron, B or Dvitamins, or fiber) that may occurin patients treated with a gluten-free diet. Current recommendationsfocus on what can be eaten and onchoosing naturally gluten-freeproducts of high nutritional value(Box: Nutritional Advice for Pa-tients With Celiac Disease).
Are vitamin supplements required?Although vitamin D production bymeans of sun exposure may partial-ly compensate for the lack of vita-min D absorption, repletion maynot be complete and patients livingin northern latitudes will be partic-ularly prone to deficiency. Lactoseintolerance is common in celiacdisease, and the resultant avoidanceof milk and other dairy productsfurther reduces intake of vitamin Dand calcium-containing foods. If
vitamin D levels are low, supple-mental vitamin D is necessary andshould be monitored to ensure nor-mal blood levels. Bone densityshould also be assessed in newlydiagnosed patients, especially ifvitamin D levels are low. Dietarysources are excellent sources ofbioavailable calcium, and consump-tion of these, in addition to calcium
Nutritional Advice for Patients
With Celiac Disease
Maintain a gluten-free diet for life
Optimize the nutritional content ofmeals and snacks
Choose naturally gluten-free foods Minimize processed or packaged
foodsFocus on what can be eaten rather than
what cannot
Avoid lactose-containing dairy products(milk, cream, ice cream, fresh cheeses)for the first few weeks after starting agluten-free diet until intestinallactase levels are restored
Continue to eat naturally low-lactosedairy products, such as yogurt, oldercheeses, kiefer
Choose foods rich in bioavailable iron,especially dark meat, poultry, and fish(plant sources or oral supplements areless bioavailable).
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
10/16
37. Hopper AD, Cross
SS, Sanders DS.Patchy villous atro-phy in adult patientswith suspectedgluten-sensitive en-teropathy: is a multi-ple duodenal biopsystrategy appropri-ate? Endoscopy.2008;40:219-24.[PMID: 18058655]
38. Goldstein NS. Non-gluten sensitivity-re-lated small bowelvillous flatteningwith increased in-traepithelial lympho-cytes: not all thatflattens is celiacsprue. Am J Clin
Pathol.2004;121:546-50.[PMID: 15080306]
39. Campanella J, BiagiF, Bianchi PI, Zanel-lati G, Marchese A,Corazza GR. Clinicalresponse to glutenwithdrawal is not anindicator of coeliacdisease. Scand J Gas-troenterol.2008;43:1311-4.[PMID: 18609173]
40. AGA Institute. AGAInstitute Medical Po-sition Statement onthe Diagnosis andManagement ofCeliac Disease. Gas-
troenterology.2006;131:1977-80.[PMID: 17087935]
41. Catassi C, Fabiani E,Iacono G, et al. Aprospective, double-blind, placebo-con-trolled trial to estab-lish a safe glutenthreshold for pa-tients with celiac dis-ease. Am J Clin Nutr.2007;85:160-6.[PMID: 17209192]
42. Haines ML, Ander-son RP, Gibson PR.Systematic review:
The evidence basefor long-term man-agement of coeliac
disease. AlimentPharmacol Ther.2008;28:1042-66.[PMID: 18671779]
43. Rubio-Tapia A,Rahim MW, See JA,Lahr BD, Wu TT, Mur-ray JA. Mucosal re-covery and mortalityin adults with celiacdisease after treat-ment with a gluten-free diet. Am J Gas-troenterol.2010;105:1412-20.[PMID: 20145607]
2011 American College of Physicians ITC5-10 In the Clinic Annals of Internal Medicine 3 May 2011
physician and a dietitian. The fre-quency of the visits is individualizedto the needs of the patient and thefamily and should take into accountthe complexity of the medical condi-tion. In general, life-long follow-upis recommended, although healthcare visits may be as infrequent asthose in a normal population for
persons who have returned to nor-mal health on a gluten-free diet.
Are repeated endoscopies andbiopsies required for follow-up?Most patients can be followed basedon symptom resolution, improvedlaboratory abnormalities, and declin-ing levels of celiac disease serology.Antibodies that are initially elevatedare typically measured every 3 to 6months until they fall into the nor-
mal range, but this practice is notbased on scientific studies. Initiallyhigher antibody titers generally takelonger to return to normal than low-er levels. If antibodies remain elevat-ed or become positive after 6 to 12months of treatment, repeated en-doscopy with biopsies should beconsidered. Despite normal levels ofantibodies, intestinal healing lags be-hind serologic response, and histol-ogy may remain abnormal for years
with persistent inflammation, even ifthe diet seems to be strictly gluten-free (43). This may be due to lowlevels of gluten contamination, a per-sistent immune response independ-ent of gluten, or other unknownmechanisms. The clinical conse-quences of such low-grade inflam-mation are not known in apparentlyhealthy, asymptomatic individuals,and as such, the rationale for repeat-ed biopsies in such cases is limited.
What are the reasons for failureto respond to a gluten-free diet?Although most patients respond rap-idly to a gluten-free diet, approxi-mately 5% do not. The primary causeof failure is continued ingestion ofgluten, whether unintentional or in-tentional. The first step in evaluatinga patient with so-called nonrespon-sive celiac disease is to carefully
review the dietary history, usually inconjunction with an expert dietitian.
Other reasons for a lack of responseare conditions that complicate orcoexist with celiac disease, such aslactose and other carbohydrate intol-erance; pancreatic insufficiency; mi-croscopic colitis; and small intestinal
bacterial overgrowth, with or with-out IgA deficiency. Gastroparesis,IBS, and other forms of functionalgastrointestinal disorders are com-mon and may be postinflammatoryin nature. Rarely, patients may haveboth celiac disease and IBD. Thesepossibilities should be evaluated andaddressed by a specialist.
A tertiary referral center reported a 70-foldincreased risk for microscopic colitis in per-sons with celiac disease compared with the
general population (44), underscoring theimportance of obtaining biopsies from thecolon in patients with persistent diarrhea de-spite adherence to a gluten-free diet. In mostcases, microscopic colitis was detected afterdiagnosis of celiac disease and often re-quired therapy beyond a gluten-free diet.
Under certain circumstances, it mayalso be important to reconsiderwhether the diagnosis of celiac dis-ease is correct. An erroneous diag-nosis may result from false-positive
serologic results, particularlyantigliadin IgG antibodies. Intes-tinal specimens also may have beenfalsely interpreted. Consultationwith a gastroenterologist expert inceliac disease should be considered.
The most feared cause of nonre-sponsive celiac disease is refractoryceliac disease. This disease is de-fined as persistent or recurrent mal-absorption symptoms and villousatrophy despite strict adherence to
a gluten-free diet for 6 to 12months in the absence of othercauses of nonresponsiveness or thepresence of overt cancer (45). Thecomplications of refractory celiacdisease include ulcerative jejunitis,collagenous sprue, and low-gradeand ultimately high-grade T-celllymphoma arising from the in-traepithelial lymphocytes (46).
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
11/16
44. Green PH, Yang J,Cheng J, Lee AR,Harper JW, Bhagat G.An association be-tween microscopic
colitis and celiac dis-ease. Clin Gastroen-terol Hepatol.2009;7:1210-6.[PMID: 19631283]
45. Rubio-Tapia A, Mur-ray JA. Classificationand management ofrefractory coeliacdisease. Gut.2010;59:547-57.[PMID: 20332526]
46. Cellier C, DelabesseE, Helmer C, et al.Refractory sprue,coeliac disease, andenteropathy-associ-ated T-cell lym-phoma. FrenchCoeliac Disease
Study Group. Lancet.2000;356:203-8.[PMID: 10963198]
47. Abdulkarim AS, Bur-gart LJ, See J, MurrayJA. Etiology of non-responsive celiacdisease: results of asystematic ap-proach. Am J Gas-troenterol.2002;97:2016-21.[PMID: 12190170]
48. Leffler DA, Dennis M,Hyett B, Kelly E,Schuppan D, KellyCP. Etiologies andpredictors of diag-nosis in nonrespon-sive celiac disease.
Clin GastroenterolHepatol. 2007;5:445-50. [PMID: 17382600]
49. Malamut G, AfchainP, Verkarre V, et al.Presentation andlong-term follow-upof refractory celiacdisease: comparisonof type I with type II.Gastroenterology.2009;136:81-90.[PMID: 19014942]
50. Rubio-Tapia A, KellyDG, Lahr BD, DoganA, Wu TT, Murray JA.Clinical staging andsurvival in refractoryceliac disease: a sin-gle center experi-
ence. Gastroenterol-ogy. 2009;136:99-107; quiz 352-3.[PMID: 18996383]
51. Matysiak-Budnik T,Malamut G, de SerreNP, et al. Long-termfollow-up of 61coeliac patients di-agnosed in child-hood: evolution to-ward latency ispossible on a normaldiet. Gut.2007;56:1379-86.[PMID: 17303598]
2011 American College of PhysiciansITC5-11In the ClinicAnnals of Internal Medicine3 May 2011
In a series of 55 patients being investigated fornonresponsive celiac disease, almost 50%had inadvertent gluten contamination. Six ofthese patients proved not to have celiac dis-ease after biopsy review. Other causes of fail-ure to respond were microscopic colitis, IBS,
pancreatic exocrine insufficiency, and bacter-ial overgrowth. True refractory celiac diseasemade up 18% of this referral group (47).
In a larger, more recent series of patients in-vestigated for nonresponsive celiac diseaseat another tertiary center, more than onethird had inadvertent gluten contamina-tion. Other common causes of failure to re-spond were IBS (22%), lactose intolerance(8%), and microscopic colitis (6%). Only10% of this referral group had true refrac-tory celiac disease (48).
When is immunosuppressivetherapy required?Most patients with refractory celiac
disease require treatment beyond (orother than) a gluten-free diet. Suchpatients should be referred to agastroenterologist for evaluation andtreatment. Various drugs, usuallybeginning with corticosteroids andthen immunomodulators, includingthiopurines (azathioprine, 6-mercap-topurine), cyclosporin, and other im-munosuppressive agents, have beenused (49, 50). Steroids are very effec-tive in improving symptoms but
should be avoided because manypatients already have poor bone den-sity. There are no randomized trialsof immunosuppressive agents fortreatment of refractory disease, andthe limited observational studies thathave been done do not always showa consistent benefit.
Which patients are at risk forlymphoma?Patients with refractory celiac diseaseare at greatest risk for T-cell lym-
phoma, and such patients, as well asthose who develop new or recurrentsymptoms of malabsorption, abdomi-nal pain, fever, and weight loss despitecompliance with a gluten-free diet,require evaluation for potential smallintestinal cancer. The evaluationshould include imaging with bariumradiography and computed tomogra-phy scanning as well as capsule
endoscopy. An endoscopic examina-tion is also required to assess for can-cer, and multiple biopsies should beobtained from the duodenum andmore distal small intestine, dependingon the findings of radiologic andendoscopic studies. In addition tohistologic appraisal, evaluation of thebiopsy samples should include im-
munohistochemistry and moleculardiagnostic studies to assess for abnor-mal lymphoid cells. Molecular geneticstudies for rearrangement of T-cellgenes are used to categorize refractoryceliac disease into type I (withoutgene rearrangement) and type II(with gene rearrangement). Severalretrospective studies indicate that the5-year mortality rate of patients withtype II refractory celiac disease is ap-proximately 50% (49, 50), but no
prospective studies have documentedthe natural history of persons identi-fied to have this presumed prelym-phoma state. Causes of death in pa-tients with refractory celiac diseaseinclude malnutrition; lymphoma; andinfection, including sepsis.
When lymphoma or prelymphoma issuspected, bone marrow biopsy andconsultation with a hematologist/oncologist is indicated. Full-thickness
surgical biopsies of the small intestineto evaluate for lymphoma may beneeded. Management is complex, andonly small case series are available forguidance in this rare cancer; parenter-al nutrition is typically needed. Giventhe complexity of care, patients withrefractory celiac disease are often re-ferred to tertiary centers specializingin celiac disease.
Is it ever safe to discontinue the
gluten-free diet?
There are few studies to indicatewhen, if ever, a gluten-free diet canbe relaxed or discontinued. In fact,gluten-free diets are often not com-pletely gluten-free, and what effectthis has on long-term health is un-known. One study (51) suggeststhat some patients start to tolerategluten in their diet over time, butthis is not endorsed by other
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
12/16
52. Biagi F, Corazza GR.Mortality in celiac
disease. Nat RevGastroenterol Hepa-tol. 2010;7:158-62.[PMID: 20125093]
53. Rostom A, MurrayJA, Kagnoff MF.American Gastroen-terological Associa-tion (AGA) Institutetechnical review onthe diagnosis andmanagement of celi-ac disease. Gastroen-terology.2006;131:1981-2002.[PMID: 17087937]
2011 American College of Physicians ITC5-12 In the Clinic Annals of Internal Medicine 3 May 2011
studies or experts in the field. Forexample, a retrospective U.S. studyindicates that the mortality of un-treated celiac disease was increased4- to 5-fold over control popula-tions (3). It has been proposed thatmortality in celiac disease is in-creased if gluten intake is high bothbefore and after diagnosis (52). An
exception to the need for continuedgluten-free diet is in patients with aterminal illness in whom troublingsymptoms are not precipitated byconsuming gluten-containingfoods. Recent studies indicatingthat elderly patients with unrecog-nized, untreated celiac disease inthe United States and Scandinaviado not have worse overall outcomesthan their peers without celiac dis-ease. These observations suggest
variability in the prognosis andhighlights the limitations of cate-gorizing celiac disease as one uni-form disease entity.
When should a nutritionist beconsulted?Patients with celiac disease shouldbe referred to a registered dietitianwho has expertise in celiac diseaseand the gluten-free dietnot alldieticians have such expertise. Thegluten-free diet is challenging to
both teach and learn, and very fewdoctors, including gastroenterolo-gists, have the detailed knowledgeof food ingredients, training, ortime to effectively instruct pa-tients. Important topics for
dietary counseling include hiddensources of gluten, ensuring ade-quate nutrition while eliminatinggluten, focusing on what can beeaten as opposed to what cannot,the increased costs of preparedgluten-free foods, and the impor-tance of lifelong adherence to agluten-free diet. Additional coun-
seling may be required for con-comitant issues, such as diabetesmellitus, obesity, hyperlipidemia,vegetarianism, and food allergies.
When should a gastroenterologistbe consulted?Patients with serology indicative ofceliac disease should be referred to agastroenterologist for esophagogas-troduodenoscopy with intestinalbiopsies to confirm the diagnosis. A
gastroenterologist should also beconsulted for evaluation of unex-plained iron deficiency anemia,chronic diarrhea, malabsorption,weight loss, and other problems sug-gesting celiac disease despite nega-tive results on serology tests; thesemight include unexplained osteo-porosis or infertility. Referral to agastroenterologist with expertise inceliac and other malabsorptive dis-eases is indicated in patients withbiopsy-proven celiac disease who
have not responded to a gluten-freediet or if relapse occurs despite con-tinuation of the gluten-free diet.Symptoms that may indicate canceralso warrant involvement of the gas-troenterologist and other specialists.
Treatment... A lifelong gluten-free diet is the cornerstone of treatment for celiacdisease. An expert dietitian should be involved to teach the patient and familymembers about the intricacies of the gluten-free diet and to follow progress. Ini-tially, other dietary modifications may be necessary, including a low-lactose dietand nutritional supplements, such as iron, vitamin D, and other vitamins and
minerals. Lack of response to a gluten-free diet should signal the physician anddietitian to look for intentional or inadvertent gluten ingestion. If not present,many additional conditions can cause nonresponsiveness, including comorbidconditions, an incorrect initial diagnosis, and complications of celiac disease. Truerefractory celiac disease or lymphoma should also be considered. In many ofthese situations, treatments other than a gluten-free diet are necessary and usu-ally require involvement of a gastroenterologist who specializes in the manage-ment of nonresponsive celiac disease.
CLINICAL BOTTOM LINE
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
13/16
54. Hill ID, Dirks MH, Lip-tak GS, et al; NorthAmerican Society for
Pediatric Gastroen-terology, Hepatologyand Nutrition.Guideline for the di-agnosis and treat-ment of celiac dis-ease in children:recommendations ofthe North AmericanSociety for PediatricGastroenterology,Hepatology and Nu-trition. J Pediatr Gas-troenterol Nutr.2005;40:1-19.[PMID: 15625418]
2011 American College of PhysiciansITC5-13In the ClinicAnnals of Internal Medicine3 May 2011
The 2006 AGA Position Statementand a Technical Review on the Di-agnosis and Management of CeliacDisease (40, 53) recommend a strictlifelong adherence to a gluten-freediet, including patients with der-matitis herpetiformis. Clinicians
must ensure adequate education,motivation, and support to achievethis goal. Consultation with an expe-rienced dietitian, referral to a support
group, and clinical follow-up forcompliance are recommended. Treat-ment of nutritional deficiency states(e.g., iron, folate, vitamin B
12) is es-
sential, and bone mineral densityshould be measured (40). The NorthAmerican Society for Pediatric
Gastroenterology, Hepatology andNutrition published guidelines fordiagnosis and treatment of celiacdisease in children in 2005 (54).
70%, depending on assessmentmethod, patient age, and definitionof nonadherence. Patients should beinformed that noncompliance witha gluten-free diet may be associatedwith increased risk for certain typesof cancer and death. Patients shouldbe told that the absence of symp-toms (or the ability to tolerate cer-tain symptoms) resulting fromnonadherence to a gluten-free dietdoes not reduce the health risks forgluten exposure.
What resources are available?Celiac diseaserelated research anddisease awareness among bothhealth care providers and the gener-al public has increased dramatically
in the past 10 years. Many books,Web sites, and patient supportgroups offer information on celiacdisease. Unfortunately, not allinformation being conveyed is evi-dence-based and misinformation isincluded in some otherwise-helpfulWebsites and books. Physicianswith expertise in celiac disease canhelp patients and other less-expertprofessional colleagues by recom-mending appropriate local or na-tional support. Patients involved insupport groups are generally morecompliant with a gluten-free dietand may benefit from the interac-tions with other individuals livingwith celiac disease.
The National Institutes of Healthhas a Celiac Disease AwarenessCampaign that can be accessedonline (http://celiac.nih.gov). This
What is the role of patienteducation?Education of patients and theirfamilies is central to the manage-ment of celiac disease. Patientsshould understand the causes ofceliac disease, the medical compli-cations of insufficiently controlleddisease, the risk for family membersto develop celiac disease, and theimportance of maintaining a strict-ly gluten-free diet lifelong. Adietitian expert in celiac diseasemanagement should help providepatient education.
Although the theory of gluten avoid-ance may seem self-evident, livinggluten-free is not simple in a society
where eating outside the home andconsumption of processed foods arethe norm. As a result, compliancewith a gluten-free diet may be diffi-cult. Specific challenges include mealplanning, eating out, traveling, con-suming adequate calories, and meet-ing the needs of growth and develop-ment in children and teenagers.Many foods contain derivatives ofwheat, rye, or barley that may causedamage to the intestine. Some pa-tients have specific nutritionally relat-ed needs to address in addition toceliac disease, including obesity, mul-tiple nutritional deficiencies, diabetes,or low bone mass. Other dietary re-strictions due to religious or personalbeliefs may need to be factored intothe gluten-free diet as well.
Dietary noncompliance has beenestimated to vary between 5% and
PatientEducation
PracticeImprovement
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
14/16
Int
he
Clini
cTool KitIn the Clinic
Celiac Disease
PIER Modulehttp://pier.acponline.org/physicians/diseases/d631/d631.htmlPIER module on celiac disease from the American College of
Physicians. PIER modules provide evidence-based, updatedinformation on current diagnosis and treatment in an electronicformat designed for rapid access at the point of care.
Patient Informationhttp://pier.acponline.org/physicians/diseases/d631/d631-pi.htmlPatient information material that appears on the following pages for
duplication and distribution to patients.http://digestive.niddk.nih.gov/ddiseases/pubs/celiac/index.htmwww.celiac.nih.gov/Information on celiac disease from the National Institute of Diabetes
and Digestive and Kidney Diseases, and learn about its CeliacDisease Awareness Campaign, which provides news and educationon celiac disease.
www.nlm.nih.gov/medlineplus/celiacdisease.htmlInformation from MedlinePLUS about celiac disease, including an
interactive tutorial available in both English and Spanish.
Clinical Guidelineswww.bmj.com/content/338/bmj.b1684.longGuidelines on the recognition and assessment of celiac disease in
children and adults from the British National Institute for Health
and Clinical Excellence in 2009.www.adaevidencelibrary.com/topic.cfm?cat=3677Evidence-based nutrition practice guideline for celiac disease from
the American Dietetic Association in 2009.www.worldgastroenterology.org/assets/.../guidelines/04_celiac_disease.pdfPractice guideline for celiac disease from the World Gastroenterology
Organization released in 2007.www.ncbi.nlm.nih.gov/pmc/articles/PMC2842922/?tool=pubmedMedical position statement on the diagnosis and management of
celiac disease from the AGA Institute in 2006.
Diagnostic Tests and Criteriawww.annals.org/content/147/5/294.full
Algorithm for Managing Nonresponsive Celiac Disease; use formanaging nonresponsive celiac disease.
Hadithi M, von Blomberg BM, Crusius JB, et al. Accuracy of serologic testsand HLA-DQ typing for diagnosing celiac disease. Ann Intern Med.2007;147:294-302. [PMID: 17785484].
Data on the accuracy of serologic tests and HLA-DQ typing fordiagnosing celiac disease
Quality-of-Care Guidelineswww.ahrq.gov/downloads/pub/evidence/pdf/celiac/celiac.pdfComprehensive systematic review of 5 areas of celiac disease:
prevalence and incidence; diagnostic tests; testing consequences;associated lymphoma; and tools for promoting and monitoringadherence to a gluten-free diet, released in 2004.
3 May 2011Annals of Internal MedicineIn the ClinicITC5-14 2011 American College of Physicians
Web site, which includes helpfuleducational materials and resources,lists professional and voluntary
organizations that are devoted toceliac disease awareness and pro-vides examples of a gluten-free diet.
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
15/16
In the Clinic
Annals of Internal Medicine
PatientIn
formation
THINGS YOU SHOULDKNOW ABOUT CELIACDISEASE
What is celiac disease? A digestive disease that hinders how the body
absorbs nutrients from food. When people with celiac disease eat foods or use
products containing gluten, an abnormal immunereaction is triggered that damages the lining of thesmall intestine.
Gluten is a protein in wheat, rye, and barley, and iscommonly found in bread, pasta, and breakfastcereals.
People with celiac disease can become malnourisheddespite a nutritious diet if damage to the smallintestines is extensive.
What are the symptoms? Digestive symptoms, including diarrhea, consti-
pation, vomiting, stomach bloating, pain, andirritability are more common in infants and children.
Adults may experience bone or joint pain, tiredness,depression or anxiety, numbness in the hands andfeet, seizures, canker sores inside the mouth, and anitchy rash.
Long-term complications include intestinal cancer;liver disease; and malnutrition, which may lead toosteoporosis, anemia, and miscarriage.
The longer a person goes undiagnosed anduntreated, the greater the risk for long-termcomplications.
How is it diagnosed?
If celiac disease is suspected, your doctor will checkif your blood has higher-than-normal levels ofcertain autoantibodies. Be aware that if you stopeating foods with gluten before this test, the resultsmay be negative even if you have the disease.
The doctor may order a biopsy of the small intestineto check for damage. For this test, a long, thin tubecalled an endoscope is passed through your mouthand stomach into the small intestine.
The doctor may order a skin test if you have a rash.Dermatitis herpetiformis, an itchy, blistering rash
usually found on the elbows, knees, and buttocks,
occurs in up to 25% of people with celiac disease. Celiac disease may go unrecognized if the symptoms
are nonspecific or similar to other diseases, such asirritable bowel syndrome. As awareness of celiacdisease improves, diagnosis rates are increasing.
How is celiac disease treated? The only treatment is a lifelong gluten-free diet. Following this diet stops symptoms in most people,
heals intestinal damage, and prevents furtherdamage.
People who do not improve on the gluten-free dietmay be consuming small amounts of gluten withoutknowing it.
Gluten is used in some medications and as anadditive in products, such as lipstick and PlayDough. Reading product labels is important.
A dietitian can help you create a gluten-free dietplan. Gluten-free bread, pasta, and other productsare increasingly available in grocery stores.
In rare cases, intestinal injury continues despite thegluten-free diet. In patients with this condition,called refractory celiac disease, the intestines are soseverely damaged that they cannot heal. Nutrientsmay need to be provided through a vein into thebloodstream.
For More Information
http://digestive.niddk.nih.gov/ddiseases/pubs/celiac_ez/
http://digestive.niddk.nih.gov/spanish/pubs/celiac_ez/index.htmWhat I need to know about Celiac Disease, a handout available
in English and Spanish from the National Institute of Diabetesand Digestive and Kidney Diseases.
www.gastro.org/patient-center/brochure_Celiac.pdfUnderstanding Celiac Disease, a handout from the AGA.
www.gluten.net/downloads/print/Diningflat.pdfTips for staying gluten-free while dining out, from the Gluten
Intolerance Group.
wnloaded From: http://annals.org/ by Jose Roel on 10/04/2012
-
7/29/2019 ANNALS Celiac Disease
16/16
CME Questions
3 May 2011Annals of Internal MedicineIn the ClinicITC5-16 2011 American College of Physicians
Questions are largely from the ACPs Medical Knowledge Self-Assessment Program (MKSAP, accessed at
http://www.acponline.org/products_services/mksap/15/?pr31). Go to www.annals.org/intheclinic/
to complete the quiz and earn up to 1.5 CME credits, or to purchase the complete MKSAP program.
1. A 25-year-old man is evaluated afterbeing turned down as a blood donorbecause of abnormal liver chemistrytests. The patient is healthy, takes no
medications, does not smoke, and drinksalcohol socially. His parents and siblingsare alive and healthy; his maternalgrandfather developed type 2 diabetesmellitus at age 75 years. The review ofsystems is normal.
On physical examination, vital signs andbody mass index are normal. Laboratorystudies show the following: hemoglobin,11.9 g/dL (119 g/L); mean corpuscularvolume, 76 fL; cholesterol (total), 155mg/dL (4.01 mmol/L); LDL cholesterol,85 mg/dL (2.2 mmol/L); HDL cholesterol,
33 mg/dL (0.85 mmol/L); bilirubin (total),0.5 mg/dL (8.55 mol/L); aspartateaminotransferase, 25 U/L; alanineaminotransferase, 58 U/L; alkalinephosphatase, 110 U/L. Serologic tests forhepatitis virus infection are normal.
Which of the following is the mostappropriate diagnostic test for thispatient?
A. Antitissue transglutaminase antibody
B. 1-Antitrypsin concentration
C. Blood alcohol levelD. Liver biopsy
2. A 35-year-old woman is evaluated for a6-month history of fatigue. She reportsno abdominal pain or diarrhea. Thepatient has a history of unexplainedosteopenia and hypothyroidism due toHashimoto disease; the hypothyroidism istreated with levothyroxine. Her dosagehas steadily increased over the past 2years to her current level of 0.3 mg/dwithout normalization of her serumthyroid hormone levels; she takes thelevothyroxine on awakening. Othermedications include a daily calcium
tablet and multivitamin, both taken atnoon. She is adherent to her medicalprogram.
On physical examination, blood pressureis 126/90 mm Hg, pulse rate is 60/min,respiration rate is 14/min, and body massindex (BMI) is 24.5; weight is 59.1 kg
(130 lb). Neck examination reveals asmall firm goiter. Laboratory studiesshow the following: hemoglobin,11.0 g/dL (110 g/L); mean corpuscularvolume, 75 fL; albumin, 3.7 g/dL (37 g/L);thyroid-stimulating hormone, 13.6 U/mL(13.6 mU/L); thyroxine (T
4), free ,
1.0 ng/dL (12.9 pmol/L).
Which of the following is the mostappropriate next step in management?
A. Add liothyronineB. Change to a different brand of
levothyroxine
C. Move the calcium tablet and vitamindosing to bedtime
D. Screen for celiac disease
3. A 53-year-old woman has a 6-monthhistory of increasing diarrhea withoutbleeding or a sense of urgency. She has 3or 4 bowel movements daily comparedwith her previous pattern of 2 or 3 bowelmovements each day. The patient has lost2.7 kg (6 lb) during this time. Medicalhistory is significant for hypothyroidism,managed with thyroid replacement
therapy. The patient is postmenopausaland has had no abnormal vaginalbleeding. She has maintained a lifelongmilk-free diet. Physical examination isnormal. BMI is 21.
Laboratory studies show the following:hemoglobin, 9.8 g/dL (98 g/L) (was 13.5g/dL [135 g/L] 1 year ago); leukocytecount, 6500/L (6.5 109/L); plateletcount, 250,000/L (250 109/L); meancorpuscular volume, 85 fL; red celldistribution width, 19 (normal:11.514.5) ; serum ferritin, 10 ng/mL(10 mg/L); serum albumin, 4.5 g/dL(45 g/L); liver chemistry studies, normal;serum thyroid-stimulating hormone,normal; serum antitissue, negative;transglutaminase antibody, negative;
stool cultures, no growth of pathogens;stool examination for ova and parasites,negative; stool assay for Clostridiumdifficiletoxin, negative.
Upper gastrointestinal series with small-bowel follow-through is normal.Colonoscopy with random biopsies is alsonormal.
Which of the following diagnostic studiesshould be scheduled next?
A. Serum antiendomysial antibody assayB. Serum calcitonin measurement
C. Upper endoscopy with small bowelbiopsies
D. Serum gastrin measurement
E. Capsule endoscopy
4. A 42-year-old woman is evaluated duringa routine examination. She has beenmarried and monogamous for 21 years.Her history includes celiac sprue, whichwas diagnosed at age 25 years and forwhich she maintains a gluten-free dietthat limits her symptoms. She has mildrosacea and frequent urinary tractinfections. Her mother was recentlydiagnosed with hypothyroidism, but thepatient reports no fatigue or hot or coldintolerance, and she has had no changesin weight, hair, skin, and nails. The
patient exercises regularly. She reports nopolyuria or polydipsia.
On physical examination, the patient isfair-skinned; BMI is 18.9, and weight hasbeen stable. Pulse rate is 68 /min, andblood pressure is 102/66 mm Hg. Theremainder of the physical examination isunremarkable.
Which of the following is mostappropriate for this patient?
A. Thyroid-stimulating hormone
measurementB. Bone-density testC. Chlamydia infection screening
D. Diabetes screeningE. Colon cancer screening