Anatomy of Chest & Neck Final
111
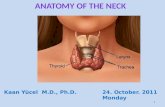
ANATOMY OF CHEST& NECK,
-
Upload
azwarmuslimhasballahamin -
Category
Documents
-
view
14 -
download
1
description
Bedah
Transcript of Anatomy of Chest & Neck Final
-
ANATOMY OF CHEST& NECK,
-
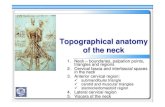
Bifurcation of carotid arteries
C3-C4
-
C.C.I.C.E.C.V.A.B.A.
-
h.p.mas. m.
-
v.a.scmj.v.i.c.ae.c.at
-
p.g
-
th
-
PATHOLOGY
-
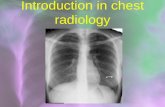
PNEUMONIA
-
PNEUMONIA
-
EMPHYSEMAEmphysema is defined as abnormal permanent enlargement of air spaces distal to the terminal bronchioles, accompanied by the destruction of the walls and without obvious fibrosis. The 3 described morphological types of emphysema are centriacinar, panacinar, and paraseptal
-
EMPHYSEMA
-
PULMONARY EDEMA
-
PNEUMOTHORAX
A collapsed lung, or pneumothorax, occurs when all or part of a lung collapses or caves inward. This occurs when air gets in the area between the lung and chest wall. When this happens the lung cannot fill up with air, breathing becomes hard, and the body gets less oxygen. A collapsed lung can occur spontaneously in a healthy person or in someone who has lungs compromised by trauma, asthma, bronchitis, or emphysema.
-
PNEUMOTHORAX
-
HEMOTHORAX
-
TUBERCULOSISTuberculosis (TB) is a contagious bacterial disease that primarily involves the lungs. Like the common cold, it spreads through the air. Only people who are sick with TB in their lungs are infectious. When infectious people cough, sneeze, talk or spit, they propel TB germs, known as bacilli, into the air. A person needs only to inhale a small number of these to be infected. TB can also affect other parts of the body, such as the brain, the kidneys or the spine.
-
TUBERCULOSIS
-
SARCOIDOSIS
What is sarcoidosis? Sarcoidosis is an inflammatory disease that affects multiple organs in the body, but mostly the lungs and lymph glands. In patients with sarcoidosis, abnormal masses or nodules (called granulomas) consisting of inflamed tissues form in certain organs of the body. These granulomas may alter the normal structure and possibly the function of the affected organ(s).
-
SARCOIDOSIS
-
PULMONARY FIBROSIS
Pulmonary fibrosis is a disease where scar tissue develops in the lungs following many infections and swelling. The scar tissue causes the lungs to become more stiff than normal. This means that the lungs cannot expand like normal, and therefore less air can get in and out of the lungs.
-
BRONCHOGENIC CARCINOMA
-
CALCIFIED B. C.
-
GRANULOMAThe human immune system, which protects us from disease, is made up of a complex network of highly specialized cells and organs. When any part of this network is faulty, it interrupts the smooth functioning of the immune response and can result in an immulogic disorder. Chronic granulomatous disease (CGD) is actually a group of rare, inherited disorders of the immune system that are caused by defects in the immune system cells called phagocytes. These defects leave patients vulnerable to severe recurrent bacterial and fungal infections and chronic inflammatory conditions such as gingivitis (swollen inflamed gums), enlarged lymph glands, or tumor-like masses called granulomas. While not malignant, granulomas can cause serious problems by obstructing passage of food through the esophagus, stomach, and intestines as well as blocking urine flow from the kidneys and bladder
-
GRANULOMA
-
INTERSTITIAL LUNG DISEASE
-
What is interstitial lung disease (ILD) / pulmonary fibrosis?Interstitial lung disease (ILD) is a broad category of lung diseases that includes more than 130 disorders characterized by scarring (i.e. fibrosis) and / or inflammation of the lungs. Some of the disorders included under the heading of ILD are:
Idiopathic pulmonary fibrosis
Hypersensitivity pneumonitis
Sarcoidosis
Eosinophilic granuloma
Chronic eosinophilic pneumonia
Bronchiolitis obliterans Lymphangioleiomyomatosis
-
ASBESTOSIS
-
ASBESTOSIS
A chronic, progressive condition of scar tissue build-up in the lungs resulting from the inhalation of asbestos fibers. Shortness of breath, increased risk of lung infection and permanent lung damage are common symptoms of asbestosis.
-
PAROTID GLAND TUMOR
-
THYROID CANCER
-
CAROTID ANEURYSM
-
NECK ABCESS
-
PROTOCOLSNECKCHEST
-
NECK-STANDARDSCOUT: LATERAL
SCANNING MODE: SPIRAL
LANDMARK: OML
SLICE PLANE: AXIAL
I.V. CONTRAST: 100-150 ml
BREATH HOLD: BREATH HOLD: HOLD ON INSPIRATION
SLICE THICKNESS: 5 MM
START LOCATION: SUPERIOR TO BASE OF TONGUE
END LOCATION: LUNG APICES
FILMING: SOFT TISSUE
-
NECK:VOCAL CORD PARALYSISSCOUT: LATERAL
SCANNING MODE: SPIRAL
LANDMARK: OML
SLICE PLANE: AXIAL
I.V. CONTRAST: 1-2 ML/SEC. 125 ML
BREATH HOLD: HOLD ON INSPIRATION
SLICE THICKNESS: 5 MM, 1MM THROUGH VOCAL CORDS
LETTER E PHONATION TO ASSESS MOBILITY OF VOCAL CORDS
START LOCATION: SUPERIOR TO BASE OF TONGUE
END LOCATION: BELOW CARINA ( T4-T5)
FILMING: SOFT TISSUE
-
AVOIDANCE OF METALLIC ARTIFACTS
-
NECK AND LARYNX+NASOPHARYNXSCOUT: LATERAL
SCAN MODE: SPIRAL
LANDMARK: OML
SLICE PLANE: AXIAL- NECK HYPEREXTENDED
I.V. CONTRAST: 100ml, 1MML/SEC.
BREATH HOLD: QUIET RESPIRATION
SLICE THICKNESS: 3-5 MM, 1MM THROUGH VOCAL CORDS
START LOCATION: SUPERIOR NASOPHARYNX
END LOCATION: CRICOID CARTILAGE
FILMING: SOFT TISSUE
-
CHEST ROUTINESCOUT: AP- AZIMUTH 0 DEG.
LANDMARK: STERNAL NOTCH
SLICE PLANE: AXIAL OR SPIRAL
I.V. CONTRAST: 80-150 ml, 1.5-2 MML/SEC., DELAY 60 SEC
BREATH HOLD: SUSPENDED INSPIRATION
SLICE THICKNESS: 8-10 MM OR 5 MM THROUGH HILUM
START LOCATION: STERNAL NOTCH
END LOCATION: TOP OF KIDNEYS (THROUGH ADRENALS)
FILMING: SOFT TISSUE + SHARP LUNG
-
CT OF CHEST END LOCATIONKIDNEYS-THROUGH ADRENALSBRONCHOGENIC CARCINOMAADRENAL MASS
-
DISPLAY OF CHEST CT400/401500/ -500
-
CHEST PESCOUT: AP
SCANNING MODE: SPIRAL
LANDMARK: STERNAL NOTCH
SLICE PLANE: AXIAL
I.V. CONTRAST: 100-150 ml, 3 ML-4 ML/SEC., DELAY 15-20 SEC
SCANNING IN CAUDOCRANIAL ORIENTATION IF MOTION SUSPECTED- TO PASS DIPHRAGM FAST
BREATH HOLD: SUSPENDED INSPIRATION
SLICE THICKNESS: 3 MM
START LOCATION: STERNAL NOTCH
END LOCATION: LUNG BASES
FILMING: SOFT TISSUE + SHARP LUNG
3D + MPR RECONSTRUCTION
-
PE
-
CHEST HIGH RESOLUTIONSCOUT: AP
SCANNING MODE: AXIAL/ SPIRAL
LANDMARK: STERNAL NOTCH
SLICE PLANE: AXIAL
I.V. CONTRAST: NONE
BREATH HOLD: SUSPENDED INSPIRATION
SLICE THICKNESS: 1-1.5 MM
INDEX: 10 MM
START LOCATION: STERNAL NOTCH
END LOCATION: THROUGH LUNG BASES
FILMING: SHARP LUNG
-
DISPLAY & FILMING1500/ -500
-
CHEST HIGH RESOLUTION-ASBESTOSIS (MESOTHELIOMA)SCOUT: AP
PATIENT SCANNED IN SUPINE AND PRONE POSITION FOR INFLATION OF THE LUNG BASES (POSTERIOR ASPECT)
SCANNING MODE: AXIAL/ SPIRAL
LANDMARK: STERNAL NOTCH
SLICE PLANE: AXIAL
I.V. CONTRAST: NONE
BREATH HOLD: SUSPENDED INSPIRATION
SLICE THICKNESS: 1-1.5 MM
INDEX: 10 MM
START LOCATION: STERNAL NOTCH
END LOCATION: THROUGH LUNG BASES
FILMING: SHARP LUNG + MEDIASTINUM
-
CHEST HIGH RESOLUTIONAIR TRAPPINGSCOUT: AP
SCANNING MODE: AXIAL
LANDMARK: STERNAL NOTCH
SLICE PLANE: AXIAL
I.V. CONTRAST: NONE
BREATH HOLD: SUSPENDED INSPIRATION + EXPIRATION
SLICE THICKNESS: 1-1.5 MM
INDEX: 10 MM
START LOCATION: STERNAL NOTCH
END LOCATION: THROUGH LUNG BASES
FILMING: SHARP LUNG ONLY
-
INSPIRATION AND EXPIRATION SCAN TO EVALUATE AIR ENTRAPMENTDETECTION OF:EMPHYSEMAASTHMASARCOIDOSISINHALATION OF FOREIGN PARTICLES