Surgical anatomy of neck
95
SURGICAL ANATOMY OF NECK DR SATINDER PAL SINGH
-
Upload
satinder-pal-singh -
Category
Health & Medicine
-
view
4.620 -
download
7
Transcript of Surgical anatomy of neck
SURGICAL ANATOMY OF NECK
SURGICAL ANATOMY OF NECKDR SATINDER PAL SINGH
2
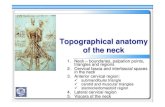
SURFACE ANATOMY OF NECK
The neck is a biomechanical wonder!Connects the head to the trunkConduit for blood vessels, nerves, and hollow organsAll of these complicated structures are packed in a very narrow area that allows for a great deal of mobility for the head as it moves relative to the ground
6
FASCIAThe neck is divided into anatomical compartments by strong fascia, which is arranged in layers and tends to align neck structures in bundles. These are real and important anatomical divisions and have great relevance clinically. The superficial fascia in the neck contains a thin sheet of muscle (the platysma).
Deep Cervical FasciaForm the boundaries of compartmentsFascial spaces can communicate infection or fluid to other regions of the bodyUsed as a guide to surgical dissectionAllow the neck structures to glide past one anotherSupports the thyroid, lymph nodes and blood vessels
10
Deep Fasciaan investing layer, which surrounds all structures in the neck;the prevertebral layer, which surrounds the vertebral column and the deep muscles associated with the back;the pretracheal layer, which encloses the viscera of the neck; and the carotid sheaths, which receive a contribution from the other three fascial layers and surround the two major neurovascular bundles on either side of the neck.
Deep Cervical Fascia
13
Deep Cervical Fascia
14
Deep Cervical Fascial SpacesRetropharyngeal - b/n prevertebral and buccopharyngealPretracheal - b/n infrahyoids and tracheaLateral pharyngeal - lat to pharynx and communicate with RP and SM spacesSubmandibular - below tonguedeep portion above mylohyoidsuperficial portion below mylohyoid
17
PlatysmaMuscle of Facial ExpressionInnervated by the cervical branch of the facial nerve
26
Sternocleidomastoid
The sternomastoid muscle divides the neck into twoanatomical triangles.Flexes and rotates the headInnervation is by CN XI
27
TrapeziusMoves and stabilizes the scapula, extends the headInnervation is by CNXI
29
Deep Cervical (Prevertebral) Muscles
30
Submental Triangle
34
Submandibular Triangle
36
Submandibular Abscess in a person with Diabetes
37
Patient with submandibular space abscess orLudwigs angina who required a tracheostomy.
Carotid Triangle
39
Muscular Triangle
42
SUPRAHYOID MUSCLES
Suprahyoid Muscles
44
Suprahyoid Muscles(geniohyoid)
45
Infrahyoid (Strap) Muscles
46
Actions of Suprahyoid and Infrahyoid Muscles
48
Branches of the external carotid arterysuperior thyroid arteryascending pharyngeal artery lingual arteryfacial arteryoccipital arteryposterior auricular arterysuperficial temporal arterymaxillary artery
VeinsCollecting blood from the skull, brain, superficial face, and parts of the neck, the internal jugular vein.The paired internal jugular veins join with the subclavian veins posterior to the sternal end of the clavicle to form the right and left brachiocephalic veins.Tributaries to each internal jugular vein include the inferior petrosal sinus, and the facial, lingual, pharyngeal, occipital, superior thyroid, and middle thyroid veins.
Innervation and Venous Drainage of the Neck
58
PHARYNXThe is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck.The pharyngeal cavity is a common pathway for air and food.
PHARYNGEAL WALLThe pharyngeal wall is formed by skeletal muscles and by fascia. Gaps between the muscles are reinforced by the fascia and provide routes for structures to pass through the wall.
Superficial lymphatics of the neck. sme, submental; sma, submandibular; f, facial; ej, external jugular; aj, anterior jugular; o, occipital; m, mastoid; p, parotid.
Deep lymphatics of the neck. IJ, internal jugular chain; SA, spinal accessory chain; TC, transverse cervical chain; dn, Delphian node.
Cervical levels according to Robbins
Classification of Neck Dissections Classic radical neck dissectionremove cervical lymph nodes from levels I to V. Extended radical neck dissection L.N. I-V +SAN+SCM+IJVL.N VIII reteropharyngealHypoglossal N.Carotid A.Skin of neck Modified radical neck dissection type I (MRND-I)selectively preserves the spinal accessory nerve (SAN)MRND-IIPreserves SAN + SCMMRND-IIIpreserves SAN+ SCM+ IJV
Comprehensive Neck Dissection
71
Selective Neck DissectionSupraomohyoid neck dissection,lymph nodes at levels I, II, and III for primary tumors of the oral cavityJugular node dissectionlevels II, III, and IV for primary tumors of the hypopharynx and larynxAnterolateral neck dissection,lymph nodes at levels I, II, III, and IV for primary tumors of the oral cavity and oropharynxPosterolateral neck dissectionLymph nodes in the suboccipital triangle, posterior triangle of theneck, level V,Central compartment neck dissection,lymph nodes at level VI in the central compartment of the neck adjacent to the thyroid gland and in thetracheoesophageal groove for thyroid cancer
Cervical lymph node groups removed in various types of neck dissection.
The most commonly used incisions for various types of neck dissections. A, Supraomohyoid neck dissection. B, Supraomohyoid neck dissection with a parotidectomy. C, Supraomohyoid neck dissection with extension for submental dissection.
D, Jugular node dissection.E, Comprehensive neck dissection. F, Comprehensive neck dissection with a thyroidectomy.
SELECTIVE NECK DISSECTION LEVELS I-III.
SELECTIVE NECK DISSECTION LEVELS II-IV
SELECTIVE NECK DISSECTION II-V, POSTAURICULAR, SUBOCCIPITAL, OR POSTEROLATERAL NECK DISSECTION
SELECTIVE NECK DISSECTION VI, OR ANTERIOR NECK DISSECTION
Pattern of lymphatic flow as demonstrated by Fisch.
PATTERNS OF NECK METASTASISPrimary siteFirst echelonlymph nodesOral cavity Submandibular glandSublingual gland Level I Level II Level IIIParotid Preauricular Periparotid & intraparotid Level II Level III Upper accessory chainLarynxPharynx Level II Level III Level IVThyroid Perithyroid nodes Tracheoesophageal groove Level VI
INCISION AND FLAPS OF NECKAllow adequate exposure of the surgical field. Assure adequate vascularization of the skin flaps. Protect the carotid artery if the sternocleidomastoid muscle has to be sacrificed. Include scars from previous procedures (e.g., surgery, biopsy, etc.). Consider the location of the primary tumor. Facilitate the use of reconstructive techniques. Contemplate the potential need of postoperative radiotherapy. Produce acceptable cosmetic results.
Some popular skin incisions for functional and selective neck dissection.(A) Gluck incisionfor unilateral and bilateral neck dissection.B) Double-Y incision of Martin.(C) Single-Y incision (D) Schobinger incision.
E) Conley incision.F) Mac Fee incision. The Mac Fee incision has excellent cosmetic results.(G) H incision.
The double-Y incision of Martin is also popular for functional and selective neck dissection.
The single-Y incision avoids one of the crossings of the double-Y incision but makes the dissection of the supraclavicular fossa difficult.
A popular incision in our practice is the classic Gluck incisionFor a bilateral functional neck dissection the incision extends between both mastoid tips, crossing the midline at the level of the cricoid arch. This incision allows good exposure when the neck dissection is to be combined with total or partial laryngectomy.
Cutaneous line of incision1 = manubrium sterni2 = clavicle3 = acromioclavicular joint4 = anterior margin of trapezius muscle5 = mastoid
Anaplastic thyroid cancer presents as a rapidly enlarging neck mass (A). Establishing a surgical airway can be challenging due to signifi cant tracheal deviation
Low Kochers incision for Thyroidectomy A skin incision is made in, or closely paralleling, a low anterior neck skin crease (Kochers incision)
Incision for parotidectomy.
A patient with enlargement of the right submandibular salivary gland. The surface markings indicate the angle of the mandible and the proposed line of incision.
Right branchial cyst.
Right cervical tuberculous adenitis with central necrosis (scrofula).
Dermoid cyst.Infected thyroglossal duct cyst.