ANATOMY AND BIOMECHANICS EPIDEMIOLOGY · Bones and joints of the pelvis. 6/11/2019 2/ 24 FIGURE...
24
6/11/2019 1/24 Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e Chapter 272: Pelvis Injuries Melissa A. Barton; H. Scott Derstine; Ciara J. Barclay-Buchanan EPIDEMIOLOGY Most pelvic fractures are secondary to automobile passenger or pedestrian accidents but are also the result of minor falls in older persons and from major falls or crush injuries. The mortality rate from all pelvic fractures is approximately 5%. However, with complex pelvic fractures, the mortality rate is about 20%. 1 Isolated fractures of the pubic rami are likely in the elderly who sustain a low-energy mechanism of injury, such as falling o a chair, and are due to underlying fragility and osteopenia. 2 ANATOMY AND BIOMECHANICS The major functions of the pelvis are protection, support, and hematopoiesis. The pelvis consists of the sacrum and coccyx as well as the bilateral "innominate bones," which are comprised of three separate bones: the ischium, ilium, and pubis. These bones provide pelvic stability that is further supported by the strong posterior sacroiliac (SI), sacrotuberous, and sacrospinous ligaments ( Figures 272-1 and 272-2). A small amount of pelvic stability is also provided by the pubic symphysis. The bladder lies in close proximity to the symphysis, as does the rectum to the sacrum, putting each of the structures at risk for injury in a trauma patient. FIGURE 272-1. Bones and joints of the pelvis.
Transcript of ANATOMY AND BIOMECHANICS EPIDEMIOLOGY · Bones and joints of the pelvis. 6/11/2019 2/ 24 FIGURE...

6/11/2019
1/24
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 272: Pelvis Injuries Melissa A. Barton; H. Scott Derstine; Ciara J. Barclay-Buchanan
EPIDEMIOLOGY
Most pelvic fractures are secondary to automobile passenger or pedestrian accidents but are also the resultof minor falls in older persons and from major falls or crush injuries. The mortality rate from all pelvic
fractures is approximately 5%. However, with complex pelvic fractures, the mortality rate is about 20%.1
Isolated fractures of the pubic rami are likely in the elderly who sustain a low-energy mechanism of injury,
such as falling o� a chair, and are due to underlying fragility and osteopenia.2
ANATOMY AND BIOMECHANICS
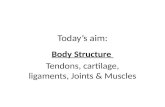
The major functions of the pelvis are protection, support, and hematopoiesis. The pelvis consists of thesacrum and coccyx as well as the bilateral "innominate bones," which are comprised of three separate bones:the ischium, ilium, and pubis. These bones provide pelvic stability that is further supported by the strongposterior sacroiliac (SI), sacrotuberous, and sacrospinous ligaments (Figures 272-1 and 272-2). A smallamount of pelvic stability is also provided by the pubic symphysis. The bladder lies in close proximity to thesymphysis, as does the rectum to the sacrum, putting each of the structures at risk for injury in a traumapatient.
FIGURE 272-1.
Bones and joints of the pelvis.

6/11/2019
2/24
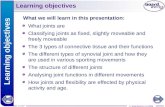
FIGURE 272-2.
Pelvic ligaments.
Incorporated in the pelvic structure are five joints that allow some movement in the bony ring. Thelumbosacral, sacroiliac, and sacrococcygeal joints, as well as the symphysis pubis, allow little movement.The acetabulum is a ball-and-socket joint that is divided into three portions: the iliac portion, or superiordome, is the chief weight-bearing surface; the inner wall consists of the pubis and is thin and easily fractured;and the posterior acetabulum is derived from the thick ischium. Any single break in the ring will yield a stableinjury without significant risk of displacement, whereas the occurrence of two breaks in the ring isconsidered an unstable pelvis.
The pelvis is extremely vascular. The iliac artery and venous trunks pass near the sacroiliac joints bilaterally.The nerve supply through the pelvis is derived from the lumbar and sacral plexuses. Injury to the pelvis mayproduce deficits at any level from the nerve root to small peripheral branches (Figure 272-3). The lower

6/11/2019
3/24
urinary tract is contained in the pelvis (Figure 272-4). In the adult, the bladder lies behind the symphysis andpubic bones, and the peritoneum covers the dome and base posteriorly. The location of the bladder and thedegree of peritoneal reflection are determined by urine content. The lower GI tract housed in the pelvisincludes a small portion of the descending colon, the sigmoid colon, the rectum, and the anus. In women,the uterus and vagina are also housed in the bony pelvis.
FIGURE 272-3.
Arterial and nerve supply of the pelvis. a. = artery; aa. = arteries; Ext. = exterior; Inf. = inferior; Int. = interior;Lat. = lateral; sup. = superior. [Reproduced with permission from Pansky B: Review of Gross Anatomy, 6th ed.Copyright © 1995, McGraw-Hill, New York.]
FIGURE 272-4.
Sagittal section of the male pelvis showing the relation of the full bladder.

6/11/2019
4/24
CLINICAL FEATURES
HISTORY
Consider the possibility of pelvic fracture in every patient with serious blunt trauma (e.g., falls from a height,pedestrian hit by a motor vehicle, crush injury, individuals ejected from a vehicle). Determine the mechanismof injury and the prehospital evaluation and treatment. Ask the patient about areas of pain, last urination ordefecation, present bladder sensation, and last solid and fluid intake. In addition, determine the time of thelast menses or the presence of pregnancy, brief past medical history, current medications, and allergies.
PHYSICAL EXAMINATION
In patients who are awake and alert, a careful physical examination is likely very sensitive (93% in one study)
for the diagnosis of a pelvic fracture.3 Symptoms and signs of pelvic injuries vary from local pain andtenderness, or inability to bear weight, to pelvic instability and severe shock. Unexplained hypotension maybe the only sign of a major pelvic disruption.
Serious Injury
For a patient with a serious or high-energy mechanism of injury, examine for abdominal tenderness, perinealand pelvic ecchymoses, lacerations, and deformities. Scrotal hematoma (Destot's sign) indicates a pelvicfracture. Leg length discrepancy or rotational deformity of the lower extremity without an obvious fracturesuggests a pelvic fracture. Evidence of blood at the urethral meatus suggests a urethral injury.

6/11/2019
5/24
Perform focused abdominal sonogram for trauma (FAST) examination as an adjunct to the physicalexamination during the primary trauma survey in any unstable patient or when the mechanism of injurycould suggest a pelvic fracture. Fluid in the peritoneum can suggest solid organ injury, but fluid in the pelviscan also lead the clinician to suspect a pelvic fracture prior to radiologic confirmation.
Do not perform compressive pelvic maneuvers in a patient with shock or an obvious pelvis fracture becausemovement of unstable fractures could produce further injury and blood loss.
However, some type of assessment for pelvic instability should be done on every trauma patient, whichcould include only visual inspection in patients with obvious pelvic fractures, physical examination by pelvicrim compression, or radiologic survey. Gentle downward and medial manual compression of the pelvis overthe iliac wings should be performed only once during the trauma survey. Repeated manipulation of thepelvic ring on any patient with a suspected pelvic fracture can increase the severity of injury, resulting ingreater blood loss. Rectal examination may detect superior or posterior displacement of the prostate, rectalinjury, or an abnormal bony prominence or large hematoma or tenderness along the suspected fracture line.Proctoscopic and/or bimanual pelvic examination may be required to fully assess mucosal tears in order to
properly diagnosis open fractures. Such injuries increase the risk of infection at the fracture site and sepsis.4
Decrease in anal sphincter tone may suggest neurologic injury. Carefully evaluate lower extremity pulses andsensation. If a pelvic fracture is found, assume intra-abdominal, retroperitoneal, gynecologic, and urologicinjuries until proven otherwise.
Stable Patient and Low Mechanism of Injury
In stable patients and those with a low-energy mechanism of injury, such as in the elderly patient who fallsfrom a seated position, examine the entire spine and the abdomen. Palpate for tenderness along the pelvicbony structures—the iliac crests, pubic rami, sacrum, and coccyx. Compress the pelvis, lateral to medial,through the iliac crests as well as through the greater trochanters. Additionally, compress the pelvic ring fromanterior to posterior through the symphysis pubis and iliac crests. Evaluate lower extremity pulses, motorfunction, and sensation.
IMAGING
The initial stabilization of the patient takes priority over obtaining radiographs. If not already done, perform aFAST scan to identify intraperitoneal bleeding.
In patients with suspected hip fracture, a standard anteroposterior pelvis radiograph is o�en used toevaluate for bony injury. If there is no tenderness to palpation in an otherwise stable, alert patient, then a
plain pelvic radiograph is not indicated.5,6 Indications for a pelvis radiograph include a hemodynamicallyunstable blunt trauma patient, pelvic tenderness, or other finding on physical examination concerning forpelvic fracture. With an unstable blunt trauma patient, a pelvic radiograph can be used to identify a pelvicfracture quickly, allow early stabilization maneuvers, and mobilize resources for emergent angiography.

6/11/2019
6/24
Routine pelvic radiographs are not needed in stable patients who will undergo an emergency CT scan of the
abdomen and pelvis anyway.7,8,9,10
CT is the gold standard for evaluating pelvic injuries. CT is more sensitive than plain radiographs for thedetection of pelvic fractures; plain radiographs rarely change the management plan in stable patients.Compared with CT, pelvic radiographs have a sensitivity of ≤85% for identifying pelvic fractures in blunt
trauma patients.2 CT is also superior to radiography in evaluating pelvic ring instability.7,8,9,11 Therefore,indications for CT include a high clinical suspicion for pelvic fracture but negative pelvic radiographs, orpelvic fractures on plain films with need to evaluate for additional pelvic fractures and instability. Contrast-enhanced CT provides useful information about posterior pelvic ring ligamentous injuries, contrastextravasation, pelvic hematoma, and retroperitoneal bleeding. Contrast extravasation on CT scan is 80% to
90% sensitive for the identification of arterial bleeding.12,13
If additional radiograph views are needed for stable patients, obtain lateral views, anteroposterior views ofeither hemipelvis, internal and external oblique views of the hemipelvis, or inlet and outlet views of thepelvis. An inlet view shows anterior-posterior displacement of ring fractures. An outlet view shows superior-inferior displacement. Oblique views of the hemipelvis are true anteroposterior and lateral views of theacetabulum. Sacral fractures may be di�icult to visualize on plain films, so obtain CT or three-dimensional
reconstruction of CT images when there is concern.14
Extremes of age require di�erent approaches for pelvic imaging. Up to half of elderly patients with a low-energy mechanism and pubic ramus fracture may have an associated posterior pelvic ring disruption
demonstrated on CT scan.15 Pain on sacral palpation may suggest posterior ring disruption and indicate theneed for pelvic CT scan. This o�en overlooked finding may contribute to the fact that one third of the elderlywith isolated rami fractures do not return to their previous living independence or may fail conservative
treatment for pain management.15 Most children with a low-energy mechanism and normal examination donot usually require even plain radiographs, because pelvic fractures are rare in young children. Avulsion/iliac
wing fractures from sports injuries are reportedly the most common pelvic injuries in children.16 Clinicalscenarios that have been associated with a pelvic fracture in children include a high-risk mechanism (e.g.,motor vehicle collision with/without ejection or rollover; automobile versus pedestrian or bicycle) combined
with either a Glasgow coma scale score <14 or pelvic tenderness.17 Other associations with serious pelvicfractures in children include medically complex children, preexisting bone disease, or developmental
delay.16
PELVIC FRACTURE PATTERNS
Pelvic fractures include those that involve a break in the pelvic ring, fractures of a single bone without abreak in the pelvic ring, and acetabular fractures. Pelvic fractures involving a break in the pelvic ring can becomplex and di�icult to classify.

6/11/2019
7/24
Abbreviations: AP = anteroposterior; LC = lateral compression; SI = sacroiliac; VS = vertical shear.
The most clinically useful classification, the Young-Burgess Pelvis Fracture Classification System, is presentedin a simplified version in Table 272-1. This system di�erentiates fracture patterns based on mechanism ofinjury and direction of causative force. Incidence of complications (i.e., urogenital and vascular) is correlatedwith the fracture pattern, making identification of the type more clinically significant and useful.
TABLE 272-1
Abbreviated Young-Burgess Classification System and Potential Incidence of Complications
Category Characteristics
Severe
Hemorrhage
(%)
Bladder
Rupture
(%)
Urethral
Injury
(%)
Lateral
compression
fractures
Transverse fracture of pubic rami, ipsilateral or
contralateral to posterior injury
60 20 20
Anterior-
posterior
fractures
(open-book)
Symphyseal diastasis and/or longitudinal rami
fractures Secondarily injured structures vary based
on severity of AP pelvic fracture
Minimal widening of SI joint with intact
posterior ligaments
Complete SI joint widening with disruption of
posterior ligaments
1
53
8
14
12
36
Vertical shear
fractures
Separation of symphysis and/or SI joint with
vertical displacement anteriorly or posteriorly,
occasionally through iliac wing and/or sacrum
75 15 25
Mixed patterns Combination of other injury patterns, LC/VS being
the most common
58 16 21
There are three main types of pelvic fracture patterns: lateral compression, anterior-posterior compression(open-book), and vertical shear. The di�erent injury types may be suggested by history but may o�en bedi�erentiated radiographically. The alignment of pubic rami fractures is a clue to the mechanism anddirection of force. In general, horizontal fractures suggest lateral compression injury, whereas verticalfractures point to vertical shear force. Open-book fractures point to an anteroposterior injury. Based on therecognition of the fracture pattern, one can then predict the likelihood of severe hemorrhage or urogenitalinjury (Table 272-1).

6/11/2019
8/24
LATERAL COMPRESSION FRACTURE
Lateral compression fractures are the most common mechanism, accounting for 60% to 70% of pelvic
fractures with an overall mortality rate of 8%.18 Motor vehicle crashes in which a car is broadsided or apedestrian is struck from the side are examples. At a minimum, a pubic ramus will be fractured. As the pelvisis further compressed and the degree of injury progresses, the sacroiliac joint is crushed, leading todisruption of the posterior ligaments, fracture of the sacrum, and rotation of the contralateral hemipelvis.(Figure 272-5).
FIGURE 272-5.
Lateral compression fracture (arrows 1 and 2) with rupture of posterior sacroiliac ligaments (R),sacrospinous/sacrotuberous complex (T), and rupture of pubic ramus (B).
ANTERIOR-POSTERIOR COMPRESSION OR OPEN-BOOK FRACTURE
Anterior-posterior compression, or open-book fracture, accounts for about 25% of severe injuries. A head-onmotor vehicle crash is the classic example. The force is delivered in an anteroposterior direction (arrow inFigure 272-6), tending to "open" the pelvis. This splays the pubic symphysis and ruptures the sacralligaments (Figure 272-6). Finally, total disruption of the sacroiliac joint will occur because of the wide"opening" of the pelvis. All supporting ligament groups, including the posterior sacroiliac ligaments, can bedisrupted.
FIGURE 272-6.
Open-book fracture, with opening of the anterior pelvis (arrow) and rupture of the sacral ligaments.

6/11/2019
9/24
VERTICAL SHEAR FRACTURE
The least common mechanism is vertical shear fractures, which are typified by a fall or jump from a height,accounting for approximately 5% of fractures. Combinations of injury patterns can make up the other 20% to25% of injuries. In vertical shear injury, the injury force vector is delivered in a vertical plane (Figure 272-7).Fractures of the pubic rami are usually seen anteriorly, whereas fractures of the sacrum, sacroiliac joint, oriliac wing are usually seen posteriorly. Any of the pelvic ligaments may be disrupted.
FIGURE 272-7.
Vertical shear fracture. Injury vector is delivered in a vertical plane (arrow). There is injury to the posterior (R)and anterior (A) sacroiliac ligaments and sacrospinous/sacrotuberous (T) ligaments.
AVULSION AND SINGLE-BONE PELVIC FRACTURES

6/11/2019
10/24
Isolated, closed avulsion fractures of the pelvis or single-bone, closed pelvic fractures are more commonlyencountered in the ED than pelvic ring disruptions. It is important to know which of these subsets offractures require further diagnostic testing, orthopedic consultation, or admission.
Isolated fractures of the anterior superior iliac spine, anterior inferior iliac spine, ischial tuberosity, pubicramus, body of the ischium, iliac wing, sacrum, or coccyx typically do not disrupt the pelvic ring and, as aresult, typically do not require surgical repair (Figure 272-8 and Table 272-2). Most of these fractures requireonly appropriate analgesia, crutches, either bed rest or non–weight-bearing status, and orthopedic follow-upon an outpatient basis.

6/11/2019
11/24
TABLE 272-2
Avulsion and Single Bone Fractures
FractureDescription/Mechanism
of Injury
Clinical
Findings/Associated
Injuries
TreatmentDisposition and
Follow-Up
Iliac wing
(Duverney)
fracture
Direct trauma, usually
lateral to medial
Swelling, tenderness
over iliac wing;
abdominal pain; ileus;
acetabular fractures;
serious injury
infrequent
Analgesics,
non–weight-
bearing until
hip abductors
pain-free,
usually
nonoperative
Discharge with
orthopedic follow-up
in 1–2 wk; admit for
open fracture or
concerning
abdominal
examination
Single
ramus of
pubis or
ischium
Fall or direct trauma in
elderly; exercise-
induced stress fracture
in young or in pregnant
women
Local pain and
tenderness; may have
inability to ambulate
Analgesics,
crutches
Discharge with PCP
or orthopedic follow-
up in 1–2 wk
Ischium
body
External trauma or from
fall in sitting position;
least common pelvic
fracture
Local pain and
tenderness; pain with
hamstring movement
Analgesics, bed
rest, donut-
ring cushion,
crutches
Discharge with
orthopedic follow-up
in 1–2 wk
Sacral
fracture
Transverse fractures
from direct
anteroposterior
trauma; upper
transverse fractures
from fall in flexed
position
Pain on rectal
examination; sacral
root injury with upper
transverse fractures;
vertical fractures may
transect the pelvic
ring
Analgesics, bed
rest, surgery
may be needed
for displaced
fractures or
neurologic
injury
Discharge with
orthopedic follow-up
in 1–2 wk; orthopedic
consultation for
displaced fractures or
neurologic deficits
Coccyx
fracture
Fall in sitting position;
more common in
women
Pain, tenderness over
sacral region; pain on
compression during
rectal examination
Analgesics, bed
rest, stool
so�eners, sitz
baths, donut-
ring cushion
PCP or orthopedic
follow-up in 2–3 wk;
surgical excision of
fracture fragment if
chronic pain

6/11/2019
12/24
Abbreviation: PCP = primary care physician.
FractureDescription/Mechanism
of Injury
Clinical
Findings/Associated
Injuries
TreatmentDisposition and
Follow-Up
Anterior-
superior
iliac spine
Forceful sartorius
muscle contraction
(e.g., adolescent
sprinters)
Pain with hip flexion
and abduction
Analgesics, bed
rest for 3–4 wk
with hip flexed
and abducted,
crutches
Discharge with
orthopedic follow-up
in 1–2 wk
Anterior-
inferior
iliac spine
Forceful rectus femoris
muscle contraction
(e.g., adolescent soccer
players)
Pain in groin; pain
with hip flexion
Analgesics, bed
rest for 3–4 wk
with hip flexed,
crutches
Discharge with
orthopedic follow-up
in 1–2 wk
Ischial
tuberosity
Forceful contraction of
hamstrings
Pain with sitting or
flexing the thigh
Analgesics, bed
rest for 3–4 wk
in extension,
external
rotation,
crutches
Discharge with
orthopedic follow-up
in 1–2 wk
FIGURE 272-8.
Avulsion fractures of the pelvis. (1) Iliac wing fracture (Duverney fracture). (2) Superior pubic ramus fracture.(3) Inferior pubic ramus fracture. (4) Transverse sacral fracture. (5) Coccyx fracture. (6) Anterior superior iliacspine avulsion. (7) Anterior inferior iliac spine avulsion. (8) Ischial tuberosity avulsion.

6/11/2019
13/24
Simple fractures in the elderly may not be as benign as at first glance. If indicated by physical exam ormechanism of injury, obtain a CT scan of the pelvis with bone windows to detect occult posterior pelvic ring
disruption that will alter management (Figures 272-9 and 272-10).15 Although isolated pelvic ramus fracturesare frequently due to low-impact trauma (e.g., fall from standing) in the elderly, isolated pelvic fractures stillresult in an increased rates of hospital admission, morbidity, need for living assistance a�er hospital
discharge, and overall mortality at 1 year.19
FIGURE 272-9.
Fracture of superior ramus (top arrow) as the result of fall from standing. Healed fracture of the inferiorramus is noted as well (bottom arrow). [Photo used with permission of Patrick Studer, MD.]

6/11/2019
14/24
FIGURE 272-10.
Same patient with fracture of le� lateral sacral body discovered on CT scan. [Photo used with permission ofPatrick Studer, MD.]

6/11/2019
15/24
Pay special attention to isolated fractures of either the sacrum or iliac wing due to the tremendous amount offorce that has occurred. If there is concern for associated injuries, then a more extensive evaluation ismandated with admission for observation.
ACETABULAR FRACTURES
Acetabular fractures are usually secondary to motor vehicle crashes. The fracture force is either transmittedlaterally through the hip or posteriorly through the femur as with a knee-versus-dashboard mechanism.Acetabular fractures are seen commonly with other injuries, including pelvic, femur, and hip fractures anddislocations (Figure 272-11A), and knee injuries. However, these fractures may be subtle and, as a result,necessitate careful inspection on x-ray (Figure 272-11B). If an acetabular fracture is suspected, it can beevaluated with an anteroposterior film, a 45-degree iliac oblique, and a 45-degree obturator oblique view—
together known as Judet views. CT is more sensitive than radiography in detecting acetabular injury.20 Also,CT is able to give more detailed information about the displacement of fracture fragments, degree ofcomminution, and other information that is useful in preoperative planning.
FIGURE 272-11.
A. Le� posterior hip dislocation with avulsed fracture fragments of the posterior acetabular rim. B. Multiplecurvilinear lucencies demonstrating nondisplaced fractures (arrows) of the right acetabulum and rightischium. Pubic symphysis is also slightly widened.

6/11/2019
16/24
Patients with acetabular fractures require hospital admission and orthopedic consultation. Look forassociated visceral, neurovascular, and orthopedic injuries. Sciatic nerve injury is a common complication.
TREATMENT

6/11/2019
17/24
Prevent movement of fracture segments, particularly in the hemodynamically unstable patient. The pelviscan be temporarily yet quickly stabilized with a bed sheet or other pelvic binding device to reduce pelvic
volume and stabilize fracture ends.21,22,23 The simplest technique is the application of either a folded bedsheet secured with towel clips or a commercially manufactured binder that is tightly wrapped around thepelvis at the level of the greater trochanters. A pelvic binder can decrease the volume of the pelvis and, inturn, help diminish blood loss for both open-book and vertical shear fractures. Lateral compression pelvicfractures would not benefit from the application of a pelvic binder because they are already rotated
internally; in fact, these patients may be harmed from further lateral compression.24
Provide resuscitation as needed with crystalloid, blood, and blood products. Retroperitoneal bleeding maycomplicate pelvic fractures. Up to 4 L of blood can be accommodated in the pelvis, until vascular pressure isovercome and tamponade occurs. Most bleeding is due to low-pressure venous bleeding and bleeding frommobile bone edges. Predictors for the need for either a transfusion or a therapeutic intervention due tohemorrhage include: (1) initial hematocrit less than 30%, (2) presence of pelvic hematoma on CT scan, or (3)
a systolic blood pressure of less than 90 mm Hg upon arrival.25 Presence of any of these factors mandates
close observation of the patient in an intensive care setting.25 Moreover, a recent prospective study showedthat base deficit <6 mmol/L or worsening base deficit >2 mmol/L while in the ED also significantly correlated
with the need for either angiography or laparotomy.26
FAST, CT, AND PELVIC FRACTURE
In hemodynamically unstable trauma patients with pelvic fractures, carefully evaluate for other sources ofblood loss. Patients who have sustained a pelvic fracture from a significant mechanism of injury shouldundergo a thoraco-abdomino-pelvic CT scan even if the FAST is negative. In the presence of pelvic fractureand serious mechanism blunt trauma, FAST-negative patients are still very likely to have concomitant visceral
injury.27
If the FAST examination reveals free intraperitoneal fluid (Figure 272-12), then CT scan is also needed todetermine the next treatment step. The FAST false-positive rate for intraperitoneal hemorrhage in patients
with pelvic ring disruption can be up to 30%.28,29 Distortion of the anatomy from fractures, retroperitonealbleeding, urine from ruptured bladder, or pelvic hematomas may result in fluid collections that mimic freeintraperitoneal fluid. The sensitivity and specificity of FAST for free peritoneal blood in major pelvic injury
appear to be related to the severity of the pelvic fracture.28,29
FIGURE 272-12.
Suggested algorithm for pelvic fracture treatment. FAST = focused abdominal sonogram for trauma; OR =operating room.

6/11/2019
18/24
One study reported the overall sensitivity and specificity of FAST to detect free peritoneal fluid in major
pelvic injury to be 81% and 87%, respectively.29 The fluid was blood in 76% and urine in 19%.29 Moderate tolarge free fluid as evidenced by fluid noted in two or more regions of the FAST exam is reported to be
associated with the need for hemorrhage control, either by laparotomy or angiography.30
ANGIOGRAPHY, EMBOLIZATION, AND EXTERNAL FIXATION
If a patient with a pelvic fracture is hemodynamically unstable and other sources of bleeding (e.g., splenic orliver laceration) have been excluded through CT scan or laparotomy, treatment options include angiographywith embolization, with or without external fixation of the pelvic fracture. Angiographic embolization ise�ective at controlling arterial bleeding, and external fixation is thought to be e�ective at controlling venous
bleeding.31,32 Both may be needed to control hemorrhage.
Shock and death are generally due to arterial rather than venous bleeding.12,13,33,34 Arterial bleeding can
occur in all types of pelvic fractures yet does so in only 10% to 15% of cases.31 The arteries involved aretypically branches of the internal iliac system, with the superior gluteal artery and the obturator artery beingthe most common (Figure 272-2). Hemorrhage from pelvic fractures refractory to resuscitation is more likelyarterial than venous in origin; angiography and embolization can control arterial hemorrhage in most
patients.31,32,33 Consider angiography early in a hemodynamically unstable patient with a pelvic fracture,a�er other sources of bleeding have been excluded.
Contrast extravasation on CT is considered by many to be an indication for angiography to evaluate for an
arterial source of bleeding that may be amenable to embolization.12,13,32,35 Some protocols advocate

6/11/2019
19/24
angiography based on hemodynamic status, the need for ongoing blood transfusion, or in patients who meet
certain blood transfusion amounts.13,31 No intervention is needed for nearly half of all patients who
demonstrate a pelvic blush on CT scan without clinical signs of ongoing bleeding.36 The need for arterialembolization has a positive predictive value of 39% for death in open pelvis fractures, as noted in one recent
study.4
Another hemorrhage control method used in the treatment of pelvic fractures is extraperitoneal packing.This technique involves surgically placing packing in the pelvis to reduce the potential space needed totamponade bleeding. Consider this treatment option for an unstable patient who is bleeding secondary to asignificant pelvis fracture in a hospital where angiography is not readily available, when a laparotomy isneeded prior to angiography, or the patient is in extremis and needs quick stabilization prior to
angiography.25
The definitive treatment of pelvic fractures occurs once the patient has been stabilized and a�er otherassociated injuries have been addressed. All pelvic fractures require orthopedic consultation and admission,even in the most stable of patients. Elderly patients with simple pubic ramus fractures typically requireadmission for pain control, observation for complications, and physical therapy for ambulation. The exacttreatment of pelvic fractures is guided by fracture location and pelvic stability. Fractures that disrupt the
pelvic ring need open reduction and internal fixation within 5 to 14 days of injury.37 The decision as to whichservice to which to admit the patient will vary between hospitals and depend on multiple factors includingthe presence of a trauma surgery service, volume of orthopedic cases, comorbidities of the patient, and
absence of other significant injuries.38
COMPLICATIONS OF PELVIC FRACTURES
Acute complications and associated injuries of pelvic fractures include urogynecologic injury, rectal injury,ruptured diaphragm, and nerve root injury. Pelvic fractures can also have long-term e�ects, including chronicpain, sexual dysfunction, and persistent functional disability.
UROGYNECOLOGIC INJURY
If a urethral injury is suspected clinically, perform retrograde urethrography before placing a Foley catheter.Urinary tract injuries are discussed in greater detail in chapter 265, "Genitourinary Trauma." Gynecologicinjuries are uncommon with pelvic trauma. Vaginal laceration can occur with anterior pelvic fractures.Perform a bimanual pelvic examination on women with pelvic fractures. If blood is detected, a speculumexamination is needed to identify vaginal hematoma, laceration, or urethral bleeding.
RECTAL INJURY
Rectal injuries are uncommon and are usually associated with urinary injuries and ischial fractures. Diagnosisis by careful rectal examination or by proctoscopy, during which gross blood is found in the rectum.

6/11/2019
20/24
1.
2.
3.
4.
5.
6.
7.
Treatment includes early diverting colostomy with washout of the distal colon and presacral space drainage.Antibiotics that cover gram-negative organisms should be administered as soon as the injury is discovered.
NERVE ROOT INJURY
Nerve root or peripheral nerve injuries can occur because of traction, pressure from hemorrhage, callus orfibrous tissue, and impingement laceration by bone fragments. The onset of symptoms and signs may bedelayed, but deficits usually follow a nerve root pattern. Lumbar nerve root injuries are associated with
sacroiliac joint dislocation or fracture and longitudinal displacement of the fracture.14 Sacral root injuries areassociated with transverse fractures of S1 and S2 as can be seen secondary to trauma from a suicidal jump
(Figure 272-4).14
REFERENCES
Hauschild O, Strohm PC, Culemann U et al.: Mortality in patients with pelvic fractures: results from theGerman pelvic injury register. J Trauma 64: 449, 2008.
[PubMed: 18301214]
Clement ND, Court-Brown CM: Elderly pelvic fractures: the incidence is increasing and patientdemographics can be used to predict the outcome. Eur J Orthop Surg Traumatol March 25, 2014. [Epubahead of print]
Gonzalez RP, Fried PQ, Bukhalo M: The utility of clinical examination in screening for pelvic fractures inblunt trauma. J Am Coll Surg 194: 121, 2002.
[PubMed: 11848627]
Cannada LK, Taylor RM, Reddix R et al.: The Jones-Powell classification of open pelvis fractures: amulticenter study evaluating mortality rates. J Trauma Acute Care Surg 74: 3, 2013.
[PubMed: 23425755]
Duane TM, Cole FJ, Weireter LJ et al.: Blunt trauma and the role of routine pelvic radiographs. Am Surg67: 849, 2007.
[PubMed: 11565762]
Civil ID, Ross SE, Botehlo G et al.: Routine pelvic radiography in severe blunt trauma: is it necessary? AnnEmerg Med 17: 488, 1998
[PubMed: 3364830]
Obaid AK, Barleben A, Porral D et al.: Utility of plain film pelvic radiographs in blunt trauma patients inthe emergency department. Am Surg 72: 951, 2006.
[PubMed: 17058743]

6/11/2019
21/24
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
Hilty MP, Behrendt I, Benneker LM et al.: Pelvic radiography in ATLS algorithms: a diminishing role? WorldJ Emerg Surg 3: 11, 2008.
[PubMed: 18318904]
Kessel B, Sevi R, Jeroukhimov I et al.: Is routine portable pelvic x-ray in stable multiple trauma patientsalways justified in a high technology era? Injury 38: 559, 2007.
[PubMed: 17303137]
Holmes JF, Wisner DH: Indications and performance of pelvic radiography in patients with blunt trauma.Am J Emerg Med 30: 1129, 2012.
[PubMed: 22920605]
Berg EE, Chebuhar C, Bell RM: Pelvic trauma imaging: a blinded comparison of computed tomographyand roentgenogram. J Trauma 41: 994, 1996.
[PubMed: 8970552]
Stephen DJ, Kreder HJ, Day AC et al.: Early detection of arterial bleeding in acute pelvic trauma. JTrauma 47: 638, 1999.
[PubMed: 10528596]
Brasel KJ, Pham K, Yant J et al.: Significance of contrast extravasation in patients with pelvic fracture. JTrauma 62: 1149, 2007.
[PubMed: 17495715]
Sugimoto Y, Ito Y, Tomioka M et al.: Risk factors for lumbosacral plexus palsy related to pelvic fracture.Spine 35: 9, 2010.
[PubMed: 20150832]
Studer P, Suhm N, Zappe B et al.: Pubic rami fractures in the elderly: a neglected injury? Swiss Med Wkly143: w13859, 2013.
[PubMed: 24089312]
Ortega HW, Reid S, Velden HV et al.: Patterns of injury and management of children with pelvic fracturesat a non-trauma center. J Emerg Med 47: 140, 2014.
[PubMed: 24928540]
Lagisetty J, Slovis T, Thomas R et al.: Are routine pelvic radiographs in major pediatric blunt traumanecessary? Pediatr Radiol 42: 853, 2012.
[PubMed: 22246414]

6/11/2019
22/24
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Manson T, O'Toole RV, Whitney A et al.: Young-Burgess classification of pelvic ring fractures: does itpredict mortality, transfusion requirements and non-orthopedic injuries? J Orthop Trauma 24: 603, 2010.
[PubMed: 20871246]
Dodge G, Brison R: Low-impact pelvic fractures in the emergency department. CJEM 12: 509, 2010. [PubMed: 21073777]
Geijer M, El-Khoury GY: Imaging of the acetabulum in the era of multi-detector computed tomography.Emerg Radiol 14: 271, 2007
[PubMed: 17588182]
Ghaemmaghami W, Sperry J, Gunst M et al.: E�ects of early use of external pelvic compression ontransfusion requirements and mortality in pelvic fractures. Am J Surg 194: 720, 2007.
[PubMed: 18005760]
Krieg JC, Mohr M, Ellis TJ et al.: Emergency stabilization of pelvic ring injuries by controlledcircumferential compression: a clinical trial. J Trauma 59: 659, 2005.
[PubMed: 16361909]
Routt ML, Falicov A, Woodhouse E et al.: Circumferential pelvic antishock sheeting: a temporaryresuscitation aid. J Orthop Trauma 20: S3, 2006.
[PubMed: 16385204]
Toth L, King KL, McGrath B et al.: E�icacy and safety of emergency non-invasive pelvic ring stabilization.Injury 43: 1330, 2012.
[PubMed: 22677220]
Bramos A, Velmahos GC, Umar MB et al.: Predictors of bleeding from stable pelvic fractures. Arch Surg146: 4, 2011.
[PubMed: 21173284]
Toth L, King KL, McGrath B et al.: Factors associated with pelvic fracture-related arterial bleeding duringtrauma resuscitation: a prospective clinical study. J Ortho Trauma December 26, 2013. [Epub ahead of print]
Ho�man L, Pierce D, Puumala S: Clinical predictors of injuries not identified by focused abdominalsonogram for trauma (FAST) examinations. J Emer Med 36: 3, 2009.
[PubMed: 18375089]
Charbit J, Millet I, Martinez O et al.: Does the size of the hemoperitoneum help to discriminate thebleeding source and guide therapeutic decisions in blunt trauma patients with pelvic ring fracture? J Trauma

6/11/2019
23/24
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
Acute Care Surg 73: 117, 2012. [PubMed: 22743381]
Tayal VS, Nielsen A, Jones AE et al.: Accuracy of trauma ultrasound in major pelvic injury. J Trauma 61:1453, 2006.
[PubMed: 17159690]
Verbeek DO, Zijlstra IA, Van Der Leij C et al.: Predicting the need for abdominal hemorrhage control inmajor pelvic fracture patients: the importance of quantifying the amount of free fluid. J Trauma Acute CareSurg 76: 5, 2014.
[PubMed: 24747457]
Totterman A, Dormagen JB, Madsen JE et al.: A protocol for angiographic embolization inexsanguinating pelvic trauma. Acta Orthop 77: 462, 2006.
[PubMed: 16819686]
Miller PR, Moore PS, Mansell E et al.: External fixation or arteriogram in bleeding pelvic fracture: initialtherapy guided by markers of arterial hemorrhage. J Trauma 54: 437, 2003.
[PubMed: 12634521]
Huittenen VM, Slattis P: Post mortem angiography and dissection of the hypogastric artery in pelvisfractures. Surgery 73: 454, 1973.
[PubMed: 4687804]
Gourlay D, Ho�er E, Routt M et al.: Pelvic angiography for recurrent traumatic pelvic arterialhemorrhage. J Trauma 59: 1168, 2005.
[PubMed: 16385296]
Durkin A, Sagi HC, Durham R et al.: Contemporary management of pelvic fractures. Am J Surg 192: 211,2006.
[PubMed: 16860634]
Verbeek DO, Zijlstra IA, Van Der Leij C et al.: Management of pelvic ring fracture patients with a pelvic"blush" on early computed tomography. J Trauma Acute Care Surg 76: 2, 2014.
[PubMed: 24368351]
Jones AL, Burgess AR: Fractures of the pelvic ring, in Bucholz RW, Heckman JD (eds): Rockwood andGreen's Fractures in Adults, 5th ed. Philadelphia: JB Lippincott, 2001.
Bugaev N, Arabian S, Rabinovici R: Admission patterns of stable patients with isolated orthopedic orneurosurgical injuries. J Trauma Acute Care Surg 74: 1151, 2013.
[PubMed: 23511159]

6/11/2019
24/24
McGraw HillCopyright © McGraw-Hill Education
All rights reserved. Your IP address is 75.148.241.33
Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair