Anal Fissure- A Real Pain In The… - tbms.ca · intrinsic non-adrenergic, non-cholinergic pathway...
58
Anal Fissure- A Real Pain In The…
Transcript of Anal Fissure- A Real Pain In The… - tbms.ca · intrinsic non-adrenergic, non-cholinergic pathway...

Anal Fissure- A Real Pain In The…

Conflict of Interest Declaration: Nothing to Disclose
Presenter: Harshad Telang
Title of Presentation: Anal Fissure- A Real Pain In The …
I have no financial or personal relationships to disclose

Rectal Pain
• Character of pain
• Intensity
• Duration
• Constant or intermittent
• Associated symptoms- ie bleeding, constipation

Rectal Pain
• Physical Examination
• Presence of mass
• Deep tissue bulging
• Tight sphincter
• Severe pain with rectal exam


Anal Fissure
• Small linear tear in anal mucosa
• Majority occur in posterior midline
• In women 10% found in anterior midline; less than 1% in males


Diagnosis
• History alone usually renders dx. w/ symptoms of tearing, knife-like pain w/ or w/o bleeding, usually associated with forceful hard stool or diarrhea.
• Pain starting w/ defecation lasts minutes to hours
• Fear of symptoms often causes pt. to withhold stooling, exacerbating constipation, impaction and pain.

Examination
• Gentle retraction of buttocks; pain is noted as fissure is exposed.
• Edematous sentinel tag may be present
• White fibers of internal sphincter may be seen in base of fissure or may be covered by thin epithelium which may hide the fissure
• Digital exam may be attempted with very well lubricated finger pushing away from fissure.
• Overhanging edges suggest chronicity


Etiology
• The initiating factor is trauma, typically overstretching of the anoderm by a large hard stool
• Linear tear along the longitudinal axis of overlying epithelium covering internal sphincter.
• Higher resting internal sphincter pressures are found in people with fissures
• Possible decrease in blood flow as cause of fissures, accounting for the pain
• Because increased resting anal pressure is associated with decreased mucosal blood flow- two may be related

Non-Operative Treatment
• Warm baths and a diet sufficiently high in fibre to achieve soft bulky stools allows approximately 50% of acute anal fissures to heal within three weeks.
• Stool softeners and fibre supplements are reasonable additions
• Recurrence is common, in the range of 30 - 70%, but can be reduced to 15 - 20% by maintaining a high fibre diet

Non-Operative Treatment- Acute Fissure
• Nitric oxide has been identified as the chemical messenger of the intrinsic non-adrenergic, non-cholinergic pathway mediating relaxation of the internal anal sphincter.
• Topical application of nitroglycerin, a nitric oxide donor, causes a transient lowering of resting anal pressure and an increase in anodermal blood flow.
• A 92% healing rate within two weeks for acute fissures treated with application of 0.2% glyceryl trinitrate ointment t.i.d.

Non-Operative Treatment
• Hydrocortisone creams and local anesthetic ointments such as lidocaine may help
• Topical nitroglycerin ointment ranging fr. 0.15% to 0.8% three to four times a day; concentration greater than 0.2% required to decrease MRAP by 25% but headaches increase accordingly
• Diltiazem used as means of “chemical sphincterotomy”. Best used as 2% topical preparation. Side effects generally less frequent vs. nitroglycerin

Non-Operative Treatment- Acute Fissure
• Topical calcium channel blockers (2% diltiazem, 0.3% nifedipine) .
• Heal 65-95% of fissures .
• The most common side effects are
headache, flushing, and symptomatic
hypotension.

Non-Operative Treatment- Chronic Fissure
• Topical Nitroglycerin: At eight weeks healing was observed in 68% of the GTN
• Botulinum Toxin: Botulinum toxin has been injected into the external and internal sphincters and, with short term follow up, healing rates of 80% have been achieved. Botulinum toxin injected into external anal sphincter on both sides of fissure

Operative Treatment
• Most sphincterotomies done as outpatient procedures with sedation and IV anesthesia.
• Intersphincteric groove palpated laterally. Incision made in the groove with division of internal anal sphincter
• the open technique involves making an incision across the intersphincteric groove, separating the internal sphincter from the anal mucosa by blunt dissection, and dividing the internal sphincter using scissors.
• the closed technique or subcutaneous technique involves making a small incision at the intersphincteric groove, inserting a scalpelwith the blade parallel to the internal sphincter and advancing it along the intersphincteric groove, and then rotating the scalpel towards the internal sphincter and dividing it.



Complications of Sphincterotomy
• Minor fecal incontinence and difficulty controlling flatulence are common side effects following surgery. Persistent minor fecal incontinence has been reported in 1.2% to 3.5% of patients; however, this does not appear to be significantly different to the rate of minor fecal incontinence experienced by patients treated with topical GTN.
• Hemmorhage can occur, more often with the open technique, and may require suture ligation.
• Perianal absess occurs in about 1% of closed sphincterotomies, generally in association with anal fistula caused by a breach of the anal mucosa by the scalpel. Incision and drainage of the abscess and fistulotomy are required


Fistula-in-ano and Perianal Abscesses
• Can be considered on a continuum
• Abscess can lead to fistula
• The cryptoglandular hypothesis states that infection of the anal glands associated with the anal crypts is the primary cause of perianal abscesses
• Perianal abscesses can then progress to fistula- an abnormal connection between two epithelialized surfaces, the anorectal mucosa and the skin

Other causes of fistula
Crohn’s
TB
Actinomycosis
Carcinoma
Trauma
Radiation
Foreign body
Lymphoma
Pelvic inflammation
Leukemia



Treatment
• Incision and drainage
• Packing not necessary for longer than a couple of days
• Antibiotics not necessary unless immunocompromised or systemic manifestations
• After I&D may develop into fistula- no way to predict or avoid
• Risk of abscess becoming fistula 26- 38%

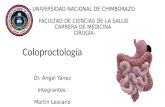
Goodsall’s Rule

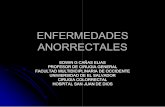
Park’s Classification of Fistula-in-ano

Imaging Studies
• Fistulogram
• Endoanal ultrasound
• CT
• MRI

Management
• No good nonsurgical management except for Crohn’s fistulae- infliximab
• Operative management- fistulotomy, Seton suture, mucosal advancement flap, fistula plug, ligation of intersphincteric fistula tract (LIFT procedure)

Fistulotomy

Seton Suture

Fistula Plug

Mucosal Advancement Flap


Prognosis
• Standard fistulotomy - The reported rate of recurrence is 0-18%, and the rate of any stool incontinence is 3-7%.
• Seton use - The reported rate of recurrence is 0-17%, and the rate of any incontinence of stool is 0-17%.
• Mucosal advancement flap - The reported rate of recurrence is 1-17%, and the rate of any incontinence of stool is 6-8%


Hemorrhoids
• represent engorgement or enlargement of the normal fibrovascular cushions lining the anal canal.
• chronic straining secondary to constipation or occasionally diarrhea
• fibrovascular cushions lose their attachment to the underlying rectal wall.

Hemorrhoids
• right anterior, right posterior and left lateral positions
• those originating above the dentate line which are termed internal
• those originating below the dentate line which are termed external.



Classification
• Grade I - bleeding without prolapse.
• Grade II - prolapse with spontaneous reduction.
• Grade III - prolapse with manual reduction.
• Grade IV - incarcerated, irreducible prolapse.

Evaluation
• rule out rectal cancer.
• young individual with bleeding associated with hemorrhoidal disease and no other systemic symptoms, and no family history, perhaps anoscopy and rigid sigmoidoscopy
• older individual, with either a family history of colorectal cancer, or change in bowel habits, a complete colonoscopy should be performed to rule out proximal neoplasia.

Treatment
• varies from simple reassurance to operative hemorrhoidectomy.
• Treatments are classified into three categories:
1) Dietary and lifestyle modification.
2) Non operative/office procedures.
3) Operative hemorrhoidectomy.

Rubber Band Ligation
• Grade I or Grade II hemorrhoids and, in some circumstances, Grade III hemorrhoids.
• Complications include bleeding, pain, thrombosis and life threatening perineal sepsis.
• successful in two thirds to three quarters of all individuals with first and second degree hemorrhoids.

Infrared Coagulation
• generates infrared radiation which coagulates tissue protein and evaporates water from cells.
• is most beneficial in Grade I and small Grade II hemorrhoids.

Electrocoagulation
• It works, in theory, similar to photocoagulation or to rubber banding.
• the probe must be left in place for ten minutes.
• poor patient tolerance minimized the effect of this procedure.

• Sclerotherapy
• Cryotherapy

Surgical Hemorrhoidectomy
• The triangular shaped hemorrhoid is excised down to the underlying sphincter muscle.
• Wound can be closed or left open
• stapled hemorrhoidectomy has been developed as an alternative to standard hemorrhoidectomy





Levator Ani Syndrome
• Pain, pressure and ache in anorectal area
• Occurs sporadically
• Lasts up to an hour
• Can be fairly severe
• Proctalgia Fugax variant- occurs mainly at night and ususally severe pain

Levator Ani Syndrome
• Spasms of levator ani, and particularily pubococcygeus
• Etiology unknown
•

Pelvic Floor

Levator Ani Syndrome Treatment
• No good treatment available
• Massage of perineum and warm baths
• Biofeedback- relaxation training
• Electrogalvanic stimulation