
Region X SOP Review - Advocate Health Care · lead EKG. –– Identify when Aspirin,...
108
Region X SOP Review Region X SOP Review June 2009 CE June 2009 CE Condell Medical Center Condell Medical Center Condell Medical Center Condell Medical Center EMS System EMS System Site code #107200E Site code #107200E-1209 1209 Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Transcript of Region X SOP Review - Advocate Health Care · lead EKG. –– Identify when Aspirin,...

Region X SOP ReviewRegion X SOP Review
June 2009 CEJune 2009 CE
Condell Medical Center Condell Medical Center Condell Medical Center Condell Medical Center EMS System EMS System
Site code #107200ESite code #107200E--12091209Prepared by: Sharon Hopkins, RN, BSN, EMT-P

ObjectivesObjectives
�� Upon successful completion of this Upon successful completion of this module, the EMS provider will be able to module, the EMS provider will be able to accomplish the following:accomplish the following:–– Identify the location for V1Identify the location for V1--V6 chest lead V6 chest lead
placement when obtaining a 12 lead EKG.placement when obtaining a 12 lead EKG.placement when obtaining a 12 lead EKG.placement when obtaining a 12 lead EKG.
–– Identify ST elevation when presented with a 12 Identify ST elevation when presented with a 12 lead EKG.lead EKG.
–– Identify when Aspirin, Nitroglycerin, and Identify when Aspirin, Nitroglycerin, and Morphine should be administered for an acute Morphine should be administered for an acute coronary syndrome & recognize ST elevation.coronary syndrome & recognize ST elevation.
–– Identify the Region X SOP criteria for treating Identify the Region X SOP criteria for treating asystole/PEA, bradycardia, and ventricular asystole/PEA, bradycardia, and ventricular fibrillation/pulseless ventricular tachycardia.fibrillation/pulseless ventricular tachycardia.

Objectives cont’dObjectives cont’d–– List the 6 H’s and 5 T’s that could be causative List the 6 H’s and 5 T’s that could be causative
factors for cardiac events & understand factors for cardiac events & understand appropriate interventions.appropriate interventions.
–– Identify pad placement for transcutaneous Identify pad placement for transcutaneous pacing.pacing.
–– Identify indications and dosing for Lidocaine, Identify indications and dosing for Lidocaine, Versed, Morphine, and Benzocaine for Conscious Versed, Morphine, and Benzocaine for Conscious Versed, Morphine, and Benzocaine for Conscious Versed, Morphine, and Benzocaine for Conscious Sedation SOP.Sedation SOP.
–– Identify criteria for a Category I and Category II Identify criteria for a Category I and Category II trauma patient.trauma patient.
–– Identify transport decisions for a Category I and Identify transport decisions for a Category I and Category II trauma patient.Category II trauma patient.
–– Actively participate in scenario Actively participate in scenario practice/discussion.practice/discussion.

Interpreting the SOP’sInterpreting the SOP’s
��System members are to begin using System members are to begin using the SOP’s to initiate treatment the SOP’s to initiate treatment without delay in patient carewithout delay in patient care
��Medical Control is to be contacted as Medical Control is to be contacted as ��Medical Control is to be contacted as Medical Control is to be contacted as soon as feasiblesoon as feasible
��An alternate order of listed An alternate order of listed interventions may be appropriate interventions may be appropriate based upon patient assessmentbased upon patient assessment–– ie: based upon assessment, Narcan may ie: based upon assessment, Narcan may
be administered before Dextrosebe administered before Dextrose

Cardiac Patient Cardiac Patient -- ACSACS
�� Use critical thinking skills to consider a Use critical thinking skills to consider a variety of patient complaints as possibly variety of patient complaints as possibly linked to an acute coronary eventlinked to an acute coronary event
–– Women (who often present with weakness and Women (who often present with weakness and unusual fatigue, shortness of breath, dizziness, unusual fatigue, shortness of breath, dizziness, unusual fatigue, shortness of breath, dizziness, unusual fatigue, shortness of breath, dizziness, nausea and vomiting)nausea and vomiting)
–– Elderly Elderly –– (who often present with fatigue and (who often present with fatigue and weakness, shortness of breath and epigastric weakness, shortness of breath and epigastric discomfort)discomfort)
–– Patients in second degree type II or complete Patients in second degree type II or complete heart blockheart block
��An acute MI is present until proven otherwiseAn acute MI is present until proven otherwise

Routine Medical CareRoutine Medical Care
�� Provide routine medical careProvide routine medical care
–– Perform initial assessmentPerform initial assessment
��ABC’sABC’s
��Disability (neuro evaluation)Disability (neuro evaluation)
––AVPUAVPU––AVPUAVPU
��Awake, responds to verbal, responds to Awake, responds to verbal, responds to pain, unresponsivepain, unresponsive
––GCSGCS
��Best response to eye opening, verbal Best response to eye opening, verbal response, and motor (scores 3response, and motor (scores 3--15)15)
–– Identify a priority patient and make a transport Identify a priority patient and make a transport decisiondecision
��Based on patient complaint and your general Based on patient complaint and your general impressionimpression

Routine Medical Care cont’dRoutine Medical Care cont’d
��Additional assessmentAdditional assessment––Vital signs, pain scale (0Vital signs, pain scale (0--10)10)
––Determine weightDetermine weight
––Determine need for and method of Determine need for and method of ––Determine need for and method of Determine need for and method of oxygen delivery (ie: n/c, NRB)oxygen delivery (ie: n/c, NRB)
––Evaluate cardiac rhythm; obtain 12 lead Evaluate cardiac rhythm; obtain 12 lead EKG if applicableEKG if applicable
––Establish IV as indicatedEstablish IV as indicated
––Determine blood glucose if indicatedDetermine blood glucose if indicated
––Reassess, reassess, reassessReassess, reassess, reassess

Routine Medical Care cont’dRoutine Medical Care cont’d
��Contact Medical ControlContact Medical Control––Who do you have (ie: 52 yearWho do you have (ie: 52 year--old male)old male)
––What (ie: with chief complaint of…)What (ie: with chief complaint of…)
––Where (ie: center of their chest Where (ie: center of their chest ––Where (ie: center of their chest Where (ie: center of their chest radiating down the left arm)radiating down the left arm)
––When (ie: for the past 2 hours)When (ie: for the past 2 hours)
––Why (ie: pain began while mowing the Why (ie: pain began while mowing the grass)grass)
–– Interventions performed and patient Interventions performed and patient responseresponse
––ETA ETA

Obtaining 12 Lead EKG’sObtaining 12 Lead EKG’s
��Be as accurate as possible when Be as accurate as possible when attaching the 6 chest leadsattaching the 6 chest leads––All EKG’s are evaluated and compared All EKG’s are evaluated and compared
to each other and measurements taken to each other and measurements taken from the same anatomical lead from the same anatomical lead from the same anatomical lead from the same anatomical lead placementplacement
��Remember: the limb leads really are Remember: the limb leads really are for the limbsfor the limbs––We in medicine have migrated the leads We in medicine have migrated the leads
to place them on the torsoto place them on the torso

12 lead 12 lead
EKG EKG
Chest Chest
LeadsLeads
Placement Placement Placement Placement starts in starts in the 4the 4thth
ICS to ICS to the right the right of the of the sternumsternum

12 Lead EKG Interpretation12 Lead EKG Interpretation
��Get in the habit of reviewing the 12 Get in the habit of reviewing the 12 lead by looking at contiguous leadslead by looking at contiguous leads
––Leads that face the same area of the Leads that face the same area of the heartheartheartheart
�� If ST elevation is seen in one of a If ST elevation is seen in one of a group, closely inspect the other sites group, closely inspect the other sites of that same groupof that same group

Groups of Anatomical Regions on Groups of Anatomical Regions on
EKG EKG –– Contiguous LeadsContiguous Leads
��Lateral wall Lateral wall –– I, aVL, V5, V6I, aVL, V5, V6
�� Inferior wall Inferior wall –– II, III, aVFII, III, aVFInferior wall Inferior wall –– II, III, aVFII, III, aVF
��Septal wall Septal wall –– V1 and V2V1 and V2
��Anterior wall Anterior wall –– V3 and V4V3 and V4

ST Elevation ST Elevation
��MeasurementMeasurement
––Look 0.04 seconds after the J point Look 0.04 seconds after the J point
��J point is where the QRS complex and ST J point is where the QRS complex and ST segment meetsegment meetsegment meetsegment meet
––ST elevation significant if:ST elevation significant if:
��> 1 mm (one small box) above the baseline > 1 mm (one small box) above the baseline is noted in 2 or more leads looking at the is noted in 2 or more leads looking at the same anatomical region (contiguous leads)same anatomical region (contiguous leads)
��> 1 mm in 2 or more anatomically > 1 mm in 2 or more anatomically contiguous chest leads (V1 through V6)contiguous chest leads (V1 through V6)
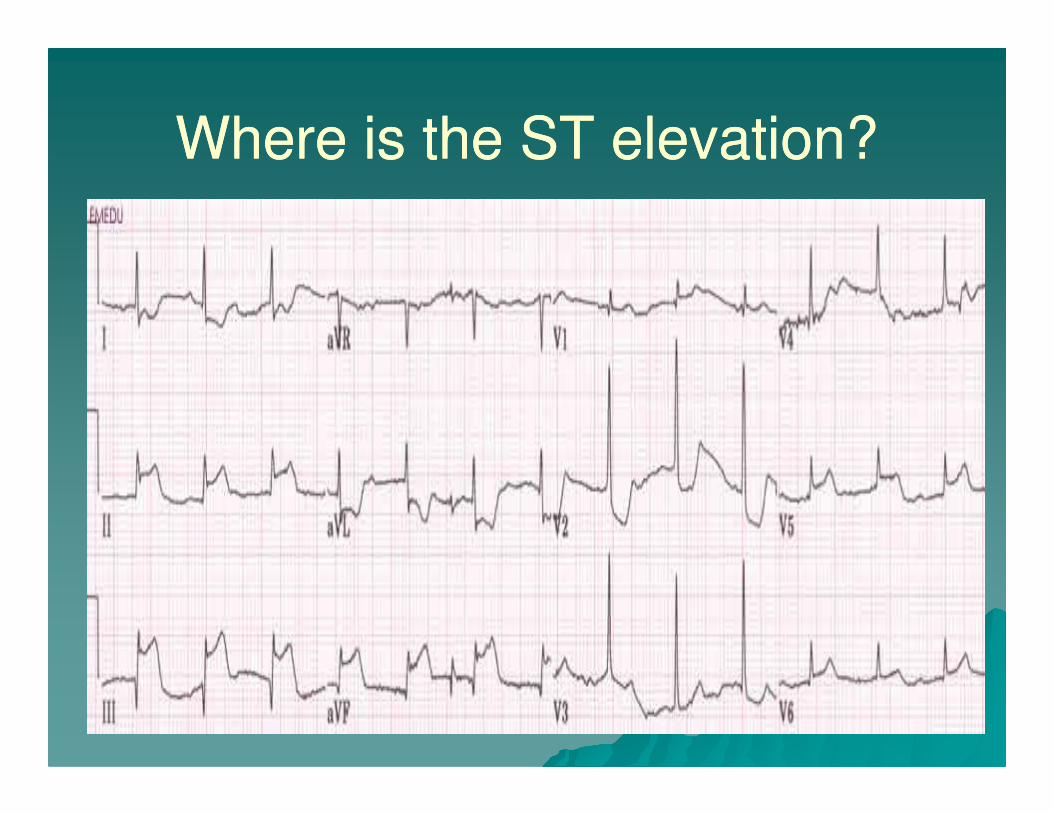
Where is the ST elevation?Where is the ST elevation?

ST Elevation II, III, aVF, V5, V6 ST Elevation II, III, aVF, V5, V6
(Inferiolateral Wall)(Inferiolateral Wall)
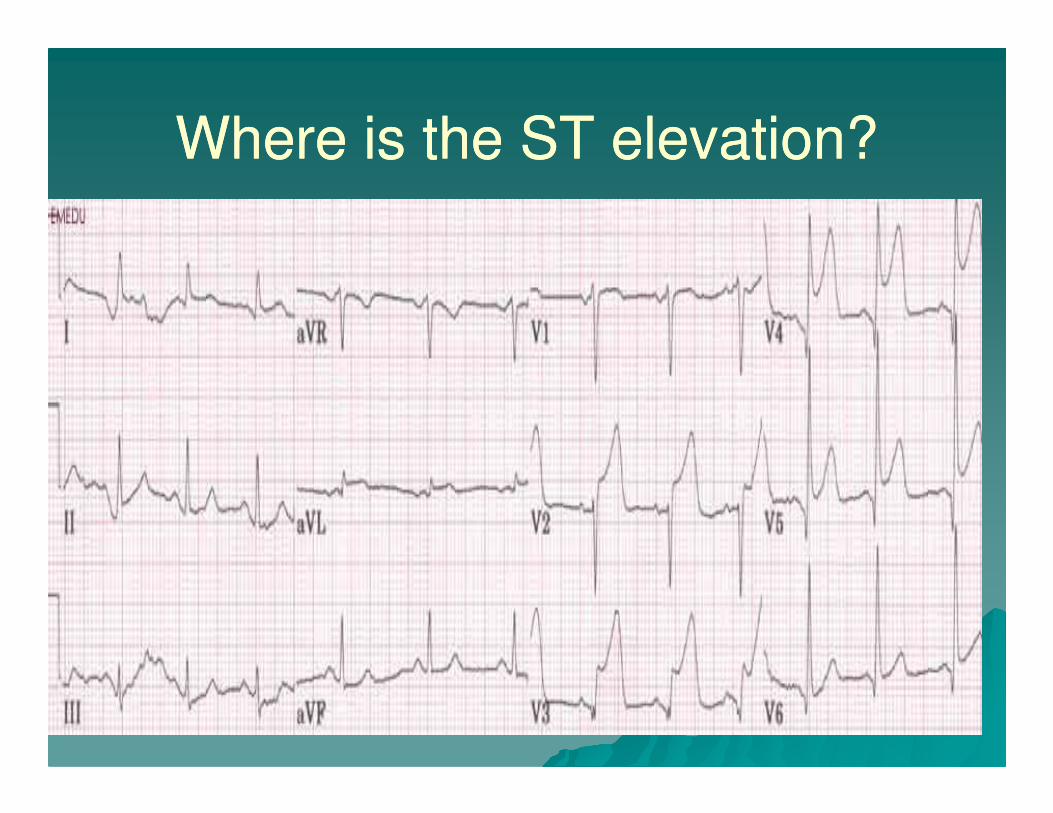
Where is the ST elevation?Where is the ST elevation?

ST Elevation V2 ST Elevation V2 -- 55

Where is the ST elevation?Where is the ST elevation?

ST Elevation II, III, aVF ST Elevation II, III, aVF –– Inf WallInf Wall
Reciprocal ST depression

Where is the ST elevation?Where is the ST elevation?

ST Elevation V2 ST Elevation V2 –– 3 (Septal wall)3 (Septal wall)
Reciprocal ST depression

Routine Medical Care cont’dRoutine Medical Care cont’d
��Transport to closest appropriate Transport to closest appropriate hospitalhospital
––Hospital of patient’s choice (when Hospital of patient’s choice (when possible)possible)possible)possible)
––Nearest hospital in cases of life Nearest hospital in cases of life threatening emergenciesthreatening emergencies

ACSACS
��Determine stability of the patientDetermine stability of the patient
��StableStable
––Alert indicating adequate perfusionAlert indicating adequate perfusion
––Skin warm and dry indicating adequate Skin warm and dry indicating adequate perfusionperfusionperfusionperfusion
––Systolic B/P Systolic B/P >>100 mmHg100 mmHg
��UnstableUnstable
––Altered level of consciousnessAltered level of consciousness
––Systolic B/P <100 mmHgSystolic B/P <100 mmHg

Stable ACSStable ACS
��Medication administrationMedication administration
––Aspirin 324 mg by mouth, chewedAspirin 324 mg by mouth, chewed
––Nitroglycerin 0.4 mg slNitroglycerin 0.4 mg sl
��May be repeated every 5 minutesMay be repeated every 5 minutes��May be repeated every 5 minutesMay be repeated every 5 minutes
��If pain persists after 2 doses, begin If pain persists after 2 doses, begin MorphineMorphine
––Morphine 2 mg IVP slowly over 2 Morphine 2 mg IVP slowly over 2 minutesminutes
��May repeat every 2 minutes as May repeat every 2 minutes as needed to a maximum of 10 mgneeded to a maximum of 10 mg

AspirinAspirin
��Used to prevent platelet aggregation Used to prevent platelet aggregation in the setting of an acute MIin the setting of an acute MI
��Avoid in the patient with an allergy Avoid in the patient with an allergy to aspirin or active GI bleedto aspirin or active GI bleedto aspirin or active GI bleedto aspirin or active GI bleed
��Dose is to chew 4 baby aspirin (total Dose is to chew 4 baby aspirin (total 324 mg)324 mg)
––Chewing breaks down the tablet and Chewing breaks down the tablet and hastens absorption hastens absorption

AspirinAspirin
��What if the patient takes aspirin but What if the patient takes aspirin but can’t remember if he took it todaycan’t remember if he took it today
––Give the dose of 4 baby aspirinGive the dose of 4 baby aspirin
��What if the patient responds that What if the patient responds that they took their aspirin dose today?they took their aspirin dose today?
–– (See next slide)(See next slide)
AspirinAspirin
�� Ask what the dose was (how many tablets Ask what the dose was (how many tablets and what strength)and what strength)
�� If the patient is reliable, document the If the patient is reliable, document the dose the patient took and inform Medical dose the patient took and inform Medical Control during reportControl during reportControl during reportControl during report
�� If patient is reliability is questionable, give If patient is reliability is questionable, give full EMS dosefull EMS dose
––Better to have the loading dose given Better to have the loading dose given than to not have any Aspirin in the than to not have any Aspirin in the system system

NitroglycerinNitroglycerin
�� Potent vasodilatorPotent vasodilator
�� When administered, pools blood away When administered, pools blood away from the heart reducing the amount of from the heart reducing the amount of blood returning to the heart (preload) and blood returning to the heart (preload) and therefore the workload of the heart is therefore the workload of the heart is reducedreducedreducedreduced
�� Onset is 1Onset is 1--3 minutes3 minutes
�� After 2 doses given 5 minutes apart, if After 2 doses given 5 minutes apart, if chest pain persists, begin Morphinechest pain persists, begin Morphine
�� Warn patient of common side effects after Warn patient of common side effects after administration of this drug (ie: headache, administration of this drug (ie: headache, lightheadedness)lightheadedness)

NitroglycerinNitroglycerin
�� Before administering Nitroglycerin, all Before administering Nitroglycerin, all patients must be screened for a B/P patients must be screened for a B/P >>100 100 systolic and use in the past 24systolic and use in the past 24--36 hours of 36 hours of Viagra or Viagra type of drugsViagra or Viagra type of drugs––Concomitant use of nitroglycerin with Concomitant use of nitroglycerin with
these drugs may cause an irreversible these drugs may cause an irreversible ––Concomitant use of nitroglycerin with Concomitant use of nitroglycerin with
these drugs may cause an irreversible these drugs may cause an irreversible hypotension leading to shock and deathhypotension leading to shock and death
��Establish an IV before administering Establish an IV before administering NitroglycerinNitroglycerin––Dilation of blood vessels will make IV Dilation of blood vessels will make IV
attempt a greater challenge after attempt a greater challenge after Nitroglycerin has been givenNitroglycerin has been given
––No IV site = no IV fluids infused if needed No IV site = no IV fluids infused if needed

Morphine SulfateMorphine Sulfate
��An opioid analgesic used for painAn opioid analgesic used for pain
��As a secondary effect, it also causes As a secondary effect, it also causes venous pooling and can pool blood venous pooling and can pool blood away from the heart reducing away from the heart reducing away from the heart reducing away from the heart reducing preload and therefore the workload preload and therefore the workload of the heartof the heart
��Always screen the patient’s B/P Always screen the patient’s B/P before and after administrationbefore and after administration––B/P to remain B/P to remain >>100 systolic100 systolic

Morphine SulfateMorphine Sulfate
��2mg slow IVP (over 2 minutes)2mg slow IVP (over 2 minutes)
��May repeat every 2 minutes as May repeat every 2 minutes as neededneeded
��Maximum dose is 10mgMaximum dose is 10mg��Maximum dose is 10mgMaximum dose is 10mg
��Pain levels often do not decrease to Pain levels often do not decrease to “0” until an intervention is provided “0” until an intervention is provided that opens up the blocked coronary that opens up the blocked coronary arteryartery

Unstable ACSUnstable ACS
�� Aspirin 324 mg by mouth if patient can Aspirin 324 mg by mouth if patient can toleratetolerate
�� Contact Medical ControlContact Medical Control
�� Monitor and transportMonitor and transport
�� If the patient takes a daily aspirin, If the patient takes a daily aspirin, regardless of the dose, and are reliable, regardless of the dose, and are reliable, no further aspirin needs to be no further aspirin needs to be administered in the fieldadministered in the field
�� Watch for hypotension especially in an Watch for hypotension especially in an inferior wall MI (II, III, aVF)inferior wall MI (II, III, aVF)

AsystoleAsystole
��Total absence of ventricular electrical Total absence of ventricular electrical activityactivity
��No pulse, no cardiac output, no blood No pulse, no cardiac output, no blood pressurepressurepressurepressure
��Occasionally may view some attempt Occasionally may view some attempt at minimal atrial electrical activityat minimal atrial electrical activity
��Begin CPR and secure airway with Begin CPR and secure airway with minimal interruption of compressionsminimal interruption of compressions
��Search for possible causes of the Search for possible causes of the arrestarrest

Possible Causes Possible Causes -- 6 H’s6 H’s
�� Hypovolemia Hypovolemia –– administer fluid challenges administer fluid challenges in 200 ml incrementsin 200 ml increments–– First evaluate breath sounds and reevaluateFirst evaluate breath sounds and reevaluate
�� Hypoxia Hypoxia –– connect to Oconnect to O22 sourcesource
Acidosis Acidosis –– ventilate to blow off retained ventilate to blow off retained �� Acidosis Acidosis –– ventilate to blow off retained ventilate to blow off retained COCO22 (an acid)(an acid)
�� HyperHyper--hypokalemia hypokalemia –– be suspicious if pt be suspicious if pt on renal dialysis or in DKAon renal dialysis or in DKA
�� Hypothermia Hypothermia –– check body temperature if check body temperature if coldcold
�� Hypoglycemia Hypoglycemia –– obtain a blood sugar levelobtain a blood sugar level

Possible Causes Possible Causes –– 5 T’s5 T’s
��Toxins Toxins –– consider all possibilities of consider all possibilities of drug overdosesdrug overdoses
��Tamponade, cardiac Tamponade, cardiac –– what is the what is the history? JVD present?history? JVD present?history? JVD present?history? JVD present?
��Tension pneumothorax Tension pneumothorax –– difficulty difficulty bagging? Breath sounds present?bagging? Breath sounds present?
��Thrombosis Thrombosis –– coronary or pulmonary coronary or pulmonary –– What is the history?What is the history?
��Trauma Trauma –– What is the history?What is the history?

AsystoleAsystole
�� Establish a drug route Establish a drug route –– IV or IOIV or IO
�� Medications:Medications:
–– Epinephrine 1:10,000 1 mg IVP/IO every 3Epinephrine 1:10,000 1 mg IVP/IO every 3--5 5 minutesminutes
–– Alternated with Atropine 1 mg IVP/IO every 3Alternated with Atropine 1 mg IVP/IO every 3--5 minutes 5 minutes
��Maximum total dose of 3 mgMaximum total dose of 3 mg
�� Remember for Atropine: when they’re Remember for Atropine: when they’re done (ie: dead), give them one (ie: 1 mg) done (ie: dead), give them one (ie: 1 mg)

Epinephrine 1:10,000Epinephrine 1:10,000
�� A vasopressor drug that mimics the A vasopressor drug that mimics the sympathetic nervous systemsympathetic nervous system
�� Increases heart rate, automaticity, and Increases heart rate, automaticity, and contraction strengthcontraction strengthcontraction strengthcontraction strength
�� At this strength and route, this drug is At this strength and route, this drug is used on patients that require extensive used on patients that require extensive and aggressive resuscitative effortsand aggressive resuscitative efforts
�� This drug may increase myocardial oxygen This drug may increase myocardial oxygen demand by making the heart work harderdemand by making the heart work harder
Epinephrine 1:10,000Epinephrine 1:10,000
��Vasopressors are important medications Vasopressors are important medications to give at the onset of the arrestto give at the onset of the arrest
��The use of vasopressors (ie: Epinephrine) The use of vasopressors (ie: Epinephrine) help to improve blood flow especially to help to improve blood flow especially to help to improve blood flow especially to help to improve blood flow especially to the heart and brainthe heart and brain
��The cardiac arrested patient does not The cardiac arrested patient does not need the strain on the heart that need the strain on the heart that Epinephrine also causes, it just comes as Epinephrine also causes, it just comes as part of the package of administration part of the package of administration with this drugwith this drug

Atropine Atropine
��Opposes the effects of the Opposes the effects of the parasympathetic nervous systemparasympathetic nervous system
�� Increases the heart rate by Increases the heart rate by increasing the rate of discharge at increasing the rate of discharge at increasing the rate of discharge at increasing the rate of discharge at the SA node (and, in the case of the SA node (and, in the case of heart block and bradycardia, heart block and bradycardia, decreasing the blockage at the AV decreasing the blockage at the AV node)node)
��Stimulates pupillary dilation after Stimulates pupillary dilation after administrationadministration

PEAPEA
��A clinical condition of the absence of A clinical condition of the absence of breathing and absence of a pulse in a breathing and absence of a pulse in a patient who exhibits organized patient who exhibits organized electrical activity on the cardiac electrical activity on the cardiac monitor.monitor.monitor.monitor.
��These patients need CPR and a These patients need CPR and a search for the causesearch for the cause––6 H’s6 H’s
––5 T’s5 T’s

PEA PEA
��Begin CPR 30:2Begin CPR 30:2
��Secure airwaySecure airway
��Search for causesSearch for causes��Search for causesSearch for causes
��Establish IV/IOEstablish IV/IO
��Determine if the heart rate is over Determine if the heart rate is over or under 60 beats per minuteor under 60 beats per minute
��Administer medicationsAdminister medications

PEA Rate < 60PEA Rate < 60
��Epinephrine 1:10,000 1 mg IVP/IOEpinephrine 1:10,000 1 mg IVP/IO
––Repeat every 3 Repeat every 3 –– 5 minutes 5 minutes
alternated withalternated withalternated withalternated with
��Atropine 1 mg IVP/IO Atropine 1 mg IVP/IO
––Repeat every 3 Repeat every 3 –– 5 minutes5 minutes
––Maximum total dose is 3 mgMaximum total dose is 3 mg

PEA Rate > 60 PEA Rate > 60
�� Administer Epinephrine 1 mg IVP/IO every Administer Epinephrine 1 mg IVP/IO every 3 3 -- 5 minutes5 minutes
�� A time keeper needs to monitor when it is A time keeper needs to monitor when it is time to readminister successive doses of time to readminister successive doses of time to readminister successive doses of time to readminister successive doses of EpinephrineEpinephrine
�� Continue to search for possible causes and Continue to search for possible causes and treat the most likely (6 H’s and 5 T’s)treat the most likely (6 H’s and 5 T’s)
–– Administer fluid challenge if lungs clearAdminister fluid challenge if lungs clear
–– Provide supplemental O2 while ventilatingProvide supplemental O2 while ventilating
–– Obtain blood glucose levelObtain blood glucose level

BradycardiaBradycardia
��This rhythm is defined by a heart This rhythm is defined by a heart rate <60rate <60
��Determine if the patient is Determine if the patient is symptomatic or notsymptomatic or not––What is the level of consciousness?What is the level of consciousness?––What is the level of consciousness?What is the level of consciousness?
��This is the first parameter to be This is the first parameter to be affected with altered perfusionaffected with altered perfusion
––What is the quality of the peripheral What is the quality of the peripheral pulse?pulse?
��B/P is the last parameter to be B/P is the last parameter to be affected by a state of decreased affected by a state of decreased perfusionperfusion

First Degree Heart BlockFirst Degree Heart Block
�� This is a This is a conditioncondition of a rhythm, not a true of a rhythm, not a true rhythmrhythm
�� Impulses from the SA node are delayed at Impulses from the SA node are delayed at the AV node and not truly blockedthe AV node and not truly blockedthe AV node and not truly blockedthe AV node and not truly blocked
�� The PR interval is greater than 0.20 The PR interval is greater than 0.20 seconds (5 small boxes)seconds (5 small boxes)
�� Most patients are not symptomatic and Most patients are not symptomatic and treatment is not requiredtreatment is not required
�� Always evaluate the underlying rhythm Always evaluate the underlying rhythm withwith the first degree heart blockthe first degree heart block

11stst Degree Heart BlockDegree Heart Block
Sinus rhythm with

Differentiating Heart Blocks

22ndnd Degree Type I Degree Type I -- WenckebachWenckebach
��SA node is generating impulses in a SA node is generating impulses in a normal fashion so P to P will march normal fashion so P to P will march out (ie: atrial rate is regular)out (ie: atrial rate is regular)
��Ventricular rate is irregularVentricular rate is irregular��Ventricular rate is irregularVentricular rate is irregular
��PR interval gets progressively longer PR interval gets progressively longer until there is a dropped QRSuntil there is a dropped QRS
��This patient is usually asymptomatic This patient is usually asymptomatic and cardiac output is not affected and cardiac output is not affected significantlysignificantly

Second Degree Heart block Type I Second Degree Heart block Type I
-- WenckebachWenckebach
��P to P is regular; PR getting longerP to P is regular; PR getting longer
P P P P P P PPP

Second Degree Heart block Second Degree Heart block –– Type Type
II II -- ClassicalClassical
��The conduction delay occurs below The conduction delay occurs below the AV nodethe AV node––Either at the bundle of His or at the Either at the bundle of His or at the
bundle branchesbundle branches
This block is more serious and can This block is more serious and can ��This block is more serious and can This block is more serious and can deteriorate to third degreedeteriorate to third degree
��Ventricular rhythm can be regular or Ventricular rhythm can be regular or irregularirregular
��There are more P waves than QRS’sThere are more P waves than QRS’s

22ndnd Degree Type II Degree Type II -- ClassicalClassical
�� P to P marches out; PR interval consistentP to P marches out; PR interval consistent
P

Third Degree Heart Block Third Degree Heart Block --
CompleteComplete
�� Impulses generated by the SA node Impulses generated by the SA node are blocked before reaching the are blocked before reaching the ventricles so no P waves are ventricles so no P waves are conductedconducted
��Atria and ventricles beat Atria and ventricles beat independently of each otherindependently of each other
��The QRS may be wide or narrow, The QRS may be wide or narrow, depending on the location of the depending on the location of the escape pacemaker siteescape pacemaker site

Complete Heart Block and Acute Complete Heart Block and Acute
MI MI –– Inferior WallInferior Wall
��33rdrd degree with an inferior wall MI degree with an inferior wall MI (II, III, aVF) is usually a result of a (II, III, aVF) is usually a result of a block above the bundle of Hisblock above the bundle of His
��The escape pacemaker site is often The escape pacemaker site is often ��The escape pacemaker site is often The escape pacemaker site is often junctionaljunctional
��The QRS will be narrow The QRS will be narrow
��Therefore the ventricular rate is Therefore the ventricular rate is often more than 40often more than 40

Complete Heart Block and Acute Complete Heart Block and Acute
MI MI –– Anterior WallAnterior Wall
�� 33rdrd degree with an anterior wall MI (V3 degree with an anterior wall MI (V3 ––4) is usually from an escape pacemaker 4) is usually from an escape pacemaker site in the ventriclessite in the ventricles
�� This 3This 3rdrd degree is often preceded by 2degree is often preceded by 2ndndThis 3This 3 degree is often preceded by 2degree is often preceded by 2degree block Type II or a bundle branch degree block Type II or a bundle branch blockblock
�� The ventricular rate is often < 40The ventricular rate is often < 40
�� The patient will most likely be The patient will most likely be symptomatic related to poor perfusionsymptomatic related to poor perfusion

33rdrd Degree Heart BlockDegree Heart Block
Remember: P to P marches out in all heart Remember: P to P marches out in all heart blocksblocks
P P P P P PP
AtropineAtropine
��Remember: “When they’re alive, Remember: “When they’re alive, give them 0.5” (mg)give them 0.5” (mg)
��Atropine is for symptomatic Atropine is for symptomatic bradycardia (sinus bradycardia and bradycardia (sinus bradycardia and bradycardia (sinus bradycardia and bradycardia (sinus bradycardia and second degree type I/Wenckebach)second degree type I/Wenckebach)
��Type II and 3Type II and 3rdrd degree are more degree are more lethal rhythms and need to be lethal rhythms and need to be aggressively cared for when aggressively cared for when symptomaticsymptomatic––These rhythms treated with TCPThese rhythms treated with TCP

Electrical Therapy Electrical Therapy --
Transcutaneous PacemakerTranscutaneous Pacemaker
��Apply (Apply (--) chest pad in the apical area) chest pad in the apical area––Over the apex (lower portion) of the Over the apex (lower portion) of the
heartheart
��Apply (+) pad in midApply (+) pad in mid--upper back upper back area between the spine and scapulaarea between the spine and scapula
��Apply (+) pad in midApply (+) pad in mid--upper back upper back area between the spine and scapulaarea between the spine and scapula
��Set rate at 80/minuteSet rate at 80/minute
��Sensitivity set for auto (demand)Sensitivity set for auto (demand)
��mA turned to lowest setting to mA turned to lowest setting to deliver consistent capturedeliver consistent capture––Pacer spike followed by wide QRSPacer spike followed by wide QRS

TCPTCP
��For patient discomfort (and there will For patient discomfort (and there will be some with electrical stimulation at be some with electrical stimulation at a rate of 80/minute)a rate of 80/minute)
––Valium 2 mg slow IVPValium 2 mg slow IVP––Valium 2 mg slow IVPValium 2 mg slow IVP
––Repeated every 2 minutes for chest wall Repeated every 2 minutes for chest wall discomfortdiscomfort
––Maximum of 10 mgMaximum of 10 mg
��You may touch the patient to provide You may touch the patient to provide care; you will care; you will notnot feel electric shocksfeel electric shocks

TCP Pad PlacementTCP Pad Placement

Ventricular Fibrillation/Pulseless Ventricular Fibrillation/Pulseless
Ventricular TachycardiaVentricular Tachycardia
��VF is a chaotic rhythm that begins in VF is a chaotic rhythm that begins in the ventriclesthe ventricles
��Absence of any organized activityAbsence of any organized activity
��No effective myocardial contraction No effective myocardial contraction ��No effective myocardial contraction No effective myocardial contraction and no pulseand no pulse
��Wave forms over 3 mm high (3 small Wave forms over 3 mm high (3 small boxes) termed coarse VFboxes) termed coarse VF
��Priorities of care are CPR and Priorities of care are CPR and defibrillationdefibrillation

VFVF

Pulseless Ventricular TachycardiaPulseless Ventricular Tachycardia
��When the QRS complexes of VT are When the QRS complexes of VT are of the same shape and amplitude, of the same shape and amplitude, the rhythm is called monomorphic VTthe rhythm is called monomorphic VT––Complexes are such that they can be Complexes are such that they can be
stacked upon each other and fitstacked upon each other and fit––Complexes are such that they can be Complexes are such that they can be
stacked upon each other and fitstacked upon each other and fit
��When the QRS complexes of VT vary When the QRS complexes of VT vary in shape and amplitude, the rhythm in shape and amplitude, the rhythm is polymorphic VT (ie: Torsades de is polymorphic VT (ie: Torsades de Pointes)Pointes)––May be caused by long QT syndromeMay be caused by long QT syndrome

Pulseless VT (Monomorphic)Pulseless VT (Monomorphic)

Long QT SyndromeLong QT Syndrome
�� An abnormality of the electrical systemAn abnormality of the electrical system
�� May be acquired or inheritedMay be acquired or inherited
�� Consider long QT syndromeConsider long QT syndrome
–– Recurrent syncope during physical exertion or Recurrent syncope during physical exertion or –– Recurrent syncope during physical exertion or Recurrent syncope during physical exertion or emotional stressemotional stress
–– Sudden & unexplained loss of consciousness Sudden & unexplained loss of consciousness during childhood and teenage yearsduring childhood and teenage years
–– Any young person with unexplained cardiac Any young person with unexplained cardiac arrestarrest
–– In the presence of family history of In the presence of family history of unexplained syncope and history of sudden, unexplained syncope and history of sudden, unexpected deathunexpected death

TorsadesTorsades

Electrical Therapy Electrical Therapy -- DefibrillationDefibrillation
�� Safety; safety; safetySafety; safety; safety
�� Always call and look for “all clear”Always call and look for “all clear”
�� Older defibrillators use 360 joules to shock Older defibrillators use 360 joules to shock and stay at 360and stay at 360and stay at 360and stay at 360
�� Newer biphasic units follow the specific Newer biphasic units follow the specific manufacturer’s recommendationsmanufacturer’s recommendations
–– Usually set at lower watt settingsUsually set at lower watt settings
�� Immediately after each defibrillation Immediately after each defibrillation attempt, resume 2 minutes of CPR before attempt, resume 2 minutes of CPR before stopping to evaluate the rhythm stripstopping to evaluate the rhythm strip

EpinephrineEpinephrine
��Start with a vasopressor drugStart with a vasopressor drug––Supports the tone of blood vessels and Supports the tone of blood vessels and
tries to improve circulation to the heart tries to improve circulation to the heart and brainand brain
Administer Epinephrine 1;10,000 Administer Epinephrine 1;10,000 ��Administer Epinephrine 1;10,000 Administer Epinephrine 1;10,000 1 mg every 3 1 mg every 3 --5 minutes5 minutes
��Alternate vasopressor with Alternate vasopressor with antidysrhythmicantidysrhythmic
��Administer medications during 2 Administer medications during 2 minute cycles of CPRminute cycles of CPR

AmiodaroneAmiodarone
��AntidysrhythmicAntidysrhythmic
��Administered at 300 mg IVP/IO for Administered at 300 mg IVP/IO for 11stst dosedose
Alternate with vasopressor drug Alternate with vasopressor drug ��Alternate with vasopressor drug Alternate with vasopressor drug (Epinephrine)(Epinephrine)
��After 5 minutes may repeat After 5 minutes may repeat Amiodarone at 150 mg IVP/IOAmiodarone at 150 mg IVP/IO
��Do not mix antidysrhythmics Do not mix antidysrhythmics ––makes the heart more irritablemakes the heart more irritable

LidocaineLidocaine
��AntidysrhythmicAntidysrhythmic
��First dose, if chosen, is 1.5 mg/kgFirst dose, if chosen, is 1.5 mg/kg
��Alternate with vasopressor drug Alternate with vasopressor drug (Epinephrine)(Epinephrine)(Epinephrine)(Epinephrine)
��After 5 minutes may repeat at After 5 minutes may repeat at 0.75 mg/kg IVP/IO0.75 mg/kg IVP/IO
��Do not mix antidysrhythmics Do not mix antidysrhythmics ––makes the heart more irritablemakes the heart more irritable

Antidysrhythmic DripsAntidysrhythmic Drips
�� Not started until the patient is resuscitatedNot started until the patient is resuscitated
�� If Amiodarone is given as a bolus, then If Amiodarone is given as a bolus, then the hospital will hang the Amiodarone dripthe hospital will hang the Amiodarone drip
�� If Lidocaine was used and the last dose If Lidocaine was used and the last dose �� If Lidocaine was used and the last dose If Lidocaine was used and the last dose was < 10 minutes ago, start Lidocaine was < 10 minutes ago, start Lidocaine drip at 2 mg/minute (30 minidrips)drip at 2 mg/minute (30 minidrips)
�� If >10 minutes from last dose, administer If >10 minutes from last dose, administer Lidocaine 0.75 mg/kg and start dripLidocaine 0.75 mg/kg and start drip
�� If no Lidocaine was given, contact Medical If no Lidocaine was given, contact Medical Control for directionControl for direction

Conscious SedationConscious Sedation
��What is the intent of this SOP?What is the intent of this SOP?
––To allow the EMS provider to sedate and To allow the EMS provider to sedate and relax the patient when advanced airway relax the patient when advanced airway maneuvers must be undertaken to maneuvers must be undertaken to maneuvers must be undertaken to maneuvers must be undertaken to protect the airway in a patient with protect the airway in a patient with reflexes. reflexes.
––These medications are not intended to These medications are not intended to paralyze the patient and should not paralyze the patient and should not make the patient apneicmake the patient apneic

Conscious SedationConscious Sedation
�� IndicationsIndications
–– Failure to maintain an adequate airway or Failure to maintain an adequate airway or aspiration riskaspiration risk
–– Actual or impending respiratory failure (severe Actual or impending respiratory failure (severe CHF, pulmonary edema, COPD, asthma, CHF, pulmonary edema, COPD, asthma, CHF, pulmonary edema, COPD, asthma, CHF, pulmonary edema, COPD, asthma, anaphylaxis with RR, 10 or >40, anaphylaxis with RR, 10 or >40, shallow/labored effort, or SpO2 shallow/labored effort, or SpO2 <<92)92)
–– GCS 8 or less due to head injuryGCS 8 or less due to head injury
–– Inability to ventilate/oxygenate adequately Inability to ventilate/oxygenate adequately after insertion of oral/nasal airway and/or BVMafter insertion of oral/nasal airway and/or BVM
–– Anticipated patient deterioration due to airway Anticipated patient deterioration due to airway in imminent risk of closurein imminent risk of closure

Conscious SedationConscious Sedation
��ContraindicationsContraindications
––Age less than 16 (15 and under)Age less than 16 (15 and under)
––Systolic B/P <100 mmHgSystolic B/P <100 mmHg
––Known hypersensitivity to any of the Known hypersensitivity to any of the ––Known hypersensitivity to any of the Known hypersensitivity to any of the drugsdrugs

Lidocaine for Head InjuriesLidocaine for Head Injuries
�� Intent Intent –– to suppress the cough reflexto suppress the cough reflex
��Probing into a patient’s mouth will Probing into a patient’s mouth will stimulate coughingstimulate coughing
Coughing raises intrathoracic Coughing raises intrathoracic ��Coughing raises intrathoracic Coughing raises intrathoracic pressures which increase intracranial pressures which increase intracranial pressures (ICP)pressures (ICP)
��Do not want to raise ICP when the Do not want to raise ICP when the patient has a head injury (ie: patient has a head injury (ie: trauma, stroke)trauma, stroke)

Lidocaine for Head InjuriesLidocaine for Head Injuries
�� 1.5 mg/kg IVP/IO as one time bolus1.5 mg/kg IVP/IO as one time bolus
�� Effect lasts approximately 5 minutesEffect lasts approximately 5 minutes
�� No need to hang a dripNo need to hang a drip
–– Don’t need a continuous drug levelDon’t need a continuous drug level–– Don’t need a continuous drug levelDon’t need a continuous drug level
�� In the cardiac setting, avoid Lidocaine if In the cardiac setting, avoid Lidocaine if the patient is in bradycardiathe patient is in bradycardia
�� In the setting of head injury, any In the setting of head injury, any bradycardia is likely a reflex reaction from bradycardia is likely a reflex reaction from the head injury the head injury -- Lidocaine Lidocaine cancan be givenbe given

VersedVersed
�� Intent Intent –– to relax the patient; serve as an to relax the patient; serve as an amnesicamnesic
�� Onset of action 1 Onset of action 1 –– 3 minutes3 minutes
�� Short actingShort acting
Initial dose 5 mg IVP/IOInitial dose 5 mg IVP/IO�� Initial dose 5 mg IVP/IOInitial dose 5 mg IVP/IO
�� If necessary, may repeat 2mg every If necessary, may repeat 2mg every minute until sedatedminute until sedated
�� After intubation, may continue 1mg every After intubation, may continue 1mg every 5 minutes for agitation5 minutes for agitation
�� Maximum dosage total is 15 mgMaximum dosage total is 15 mg

MorphineMorphine
�� Intent Intent –– to relax the patient, reduce to relax the patient, reduce anxiety, and relieve painanxiety, and relieve pain
�� Versed does not affect pain receptors at Versed does not affect pain receptors at allallallall
�� If the doses of Versed and Morphine are If the doses of Versed and Morphine are alternated, the total effect will be more alternated, the total effect will be more therapeutic than giving either drug alonetherapeutic than giving either drug alone
�� Dose: 2 mg IVP/IO slow over 2 minutesDose: 2 mg IVP/IO slow over 2 minutes
�� May repeat every 3 minutesMay repeat every 3 minutes
�� Max dosage of 10 mgMax dosage of 10 mg

BenzocaineBenzocaine
�� Intent Intent –– to suppress the gag reflexto suppress the gag reflex
�� If the patient is unconscious, check for a If the patient is unconscious, check for a blink reflex to check for the presence of a blink reflex to check for the presence of a gag reflex gag reflex gag reflex gag reflex
–– Stroke the eyelashes looking for movement of Stroke the eyelashes looking for movement of the eyelidthe eyelid
�� If possible, ask the patient to open their If possible, ask the patient to open their mouth to spray Benzocainemouth to spray Benzocaine
�� If the patient cannot open their mouth, If the patient cannot open their mouth, open their mouth and use the extender open their mouth and use the extender straw to spray the back of the throatstraw to spray the back of the throat

BenzocaineBenzocaine
��DoseDose
––Short 1 second spray delivered to the Short 1 second spray delivered to the posterior aspect of the mouthposterior aspect of the mouth
��Extended exposure to Benzocaine Extended exposure to Benzocaine ��Extended exposure to Benzocaine Extended exposure to Benzocaine may produce methemoglobinemiamay produce methemoglobinemia
––Patient presents cyanotic and needs an Patient presents cyanotic and needs an antidote administered at the hospitalantidote administered at the hospital
––Keep the spray to 1 second and deliver Keep the spray to 1 second and deliver no more than 2 sprays, if neededno more than 2 sprays, if needed

Region X Field Triage CriteriaRegion X Field Triage Criteria
��Base criteria created by IDPH and Base criteria created by IDPH and augmented by Region X membersaugmented by Region X members
��Assists in decision making regarding Assists in decision making regarding patient transportpatient transportpatient transportpatient transport
��Give as much of a heads up as Give as much of a heads up as possible to allow the facility to possible to allow the facility to prepare for the patientprepare for the patient
��Be sure to include mechanism of Be sure to include mechanism of injury and body region injuredinjury and body region injured

Unstable PatientUnstable Patient
��Systolic B/P Systolic B/P <<90 on 2 readings90 on 2 readings
OROR
��For the pediatric patient, For the pediatric patient, <<80 on 80 on 2 readings2 readings2 readings2 readings
��Transport to the Transport to the highest Level highest Level Trauma Center within 25 minutesTrauma Center within 25 minutes

Category I Trauma PatientCategory I Trauma Patient
��Unstable vital signsUnstable vital signs
––GCS GCS <<10 or deteriorating 10 or deteriorating mental statusmental statusmental statusmental status
––Respiratory rate <10 or >29Respiratory rate <10 or >29
––Revised trauma score <11Revised trauma score <11

Category I Trauma PatientCategory I Trauma Patient
�� Anatomy of injuryAnatomy of injury
–– Penetrating injuries to head, neck, torso, groinPenetrating injuries to head, neck, torso, groin
–– Combination trauma with burns Combination trauma with burns >>20%20%
–– 2 or more proximal long bone fractures2 or more proximal long bone fractures
–– Unstable pelvisUnstable pelvis
–– Flail chestFlail chest
–– Limb paralysis &/or sensory deficits above the Limb paralysis &/or sensory deficits above the wrist or anklewrist or ankle
–– Open & depressed skull fractureOpen & depressed skull fracture
–– Amputation proximal to wrist or ankleAmputation proximal to wrist or ankle

Transport Decision Transport Decision –– Category ICategory I
��Patients with unstable vital signs and Patients with unstable vital signs and meeting any criteria of Category I meeting any criteria of Category I must be transported to the must be transported to the highest highest level trauma center within 25 level trauma center within 25 minutesminutesminutesminutes
��This may mean passing up a Level II This may mean passing up a Level II Trauma Center if you can get to a Trauma Center if you can get to a Level I Center within 25 minutesLevel I Center within 25 minutes
��The clock starts from time of insultThe clock starts from time of insult

Category II Trauma PatientCategory II Trauma Patient
��Mechanism of injury Mechanism of injury ––Puts patient at high risk for injury Puts patient at high risk for injury
potential but right now the patient is potential but right now the patient is stablestable
Consider coConsider co--morbid factors that morbid factors that ��Consider coConsider co--morbid factors that morbid factors that increase the riskincrease the risk––Age Age <<5 without booster/car seat5 without booster/car seat
––Bleeding disorders or on anticoagulantsBleeding disorders or on anticoagulants
––Pregnancy Pregnancy >>24 weeks24 weeks

Category II Trauma PatientCategory II Trauma Patient
��Mechanism of injuryMechanism of injury
––Ejection from automobileEjection from automobile
––Death in same vehicleDeath in same vehicle
––Motorcycle crash >20mph or with Motorcycle crash >20mph or with ––Motorcycle crash >20mph or with Motorcycle crash >20mph or with separation of rider from bikeseparation of rider from bike
––Rollover Rollover –– unrestrainedunrestrained
––Falls Falls >>20 feet or Peds falls 20 feet or Peds falls >>3x their 3x their body lengthbody length
––Pedestrian thrown or run overPedestrian thrown or run over

Category II Trauma PatientCategory II Trauma Patient
��Mechanism of injury continuedMechanism of injury continued
––Auto vs pedestrian/bicyclist with >5mph Auto vs pedestrian/bicyclist with >5mph impactimpact
––Extrication > 20 minutesExtrication > 20 minutes––Extrication > 20 minutesExtrication > 20 minutes
––High speed MVCHigh speed MVC
��Speed Speed >> 40 mph40 mph
��Intrusion Intrusion >> 12 inches12 inches
��Major deformity Major deformity >> 20 inches20 inches

Transport Decision Transport Decision –– Category IICategory II
��Transport to the Transport to the closestclosestTrauma CenterTrauma CenterTrauma CenterTrauma Center

Category III Trauma PatientCategory III Trauma Patient
��All other patients receiving traumatic All other patients receiving traumatic injuries and do not fit/meet criteria injuries and do not fit/meet criteria for a Category I (unstable) or for a Category I (unstable) or Category II (stable and lucky) Category II (stable and lucky) patient automatically are deemed a patient automatically are deemed a patient automatically are deemed a patient automatically are deemed a Category III trauma patientCategory III trauma patient
��Transport to the Transport to the closest closest trauma trauma centercenter

Practice ScenariosPractice Scenarios
��Review the clinical vignetteReview the clinical vignette
��Discuss the assessment performed Discuss the assessment performed
�� Interpret the lead II rhythm strip or Interpret the lead II rhythm strip or identify ST elevation on the 12 lead identify ST elevation on the 12 lead identify ST elevation on the 12 lead identify ST elevation on the 12 lead EKGEKG
��Determine a clinical impressionDetermine a clinical impression
��Decide on intervention(s) requiredDecide on intervention(s) required

Scenario #1Scenario #1
��A 25 yearA 25 year--old female working in a old female working in a lumberyard was struck in the chest lumberyard was struck in the chest with lumber begin loaded by a with lumber begin loaded by a forklift.forklift.forklift.forklift.
��Upon your arrival, the scene is safe, Upon your arrival, the scene is safe, the patient is unresponsive, apneic, the patient is unresponsive, apneic, and found to be pulseless. There is a and found to be pulseless. There is a large bruise on the center of her large bruise on the center of her chestchest
��CPR is initiatedCPR is initiated

Scenario #1 RhythmScenario #1 Rhythm
There is no pulse
��What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #1Scenario #1
��With PEA, determine the underlying With PEA, determine the underlying raterate
––Rate will influence the use of Rate will influence the use of Atropine or notAtropine or notAtropine or notAtropine or not
��As you are performing CPR, start As you are performing CPR, start considering the causesconsidering the causes
––6 H’s and 5 T’s6 H’s and 5 T’s
��Add treatment to the likely causesAdd treatment to the likely causes

Scenario #1Scenario #1
��What medications are indicated?What medications are indicated?
––Epinephrine as a vasopressor is always Epinephrine as a vasopressor is always the first drug administeredthe first drug administered
––Atropine is indicated only if the heart Atropine is indicated only if the heart ––Atropine is indicated only if the heart Atropine is indicated only if the heart rate is below 60rate is below 60
��Whoever is reading the monitor needs to Whoever is reading the monitor needs to convey to their team members what the convey to their team members what the rate is when PEA is discovered rate is when PEA is discovered
��Allows the team leader and medication Allows the team leader and medication person to plan the appropriate interventionperson to plan the appropriate intervention

Scenario #2Scenario #2
��You have arrived on the scene to You have arrived on the scene to initially find your 72 yearinitially find your 72 year--old male old male patient complaining of pain radiating patient complaining of pain radiating to his neck for the past hour with a to his neck for the past hour with a heavy weight on his chest.heavy weight on his chest.heavy weight on his chest.heavy weight on his chest.
��Patient is slightly short of breath, Patient is slightly short of breath, denies nausea or vomiting.denies nausea or vomiting.
��Awake, skin pale and clammyAwake, skin pale and clammy
��VS: B/P 102/58; P VS: B/P 102/58; P –– 220; RR 220; RR –– 2424
��As you connect the monitor, the As you connect the monitor, the patient becomes unresponsivepatient becomes unresponsive

Scenario #2 RhythmScenario #2 Rhythm
The patient has lost consciousness and now has no pulse
��What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #2 Rhythm ChangeScenario #2 Rhythm Change
��What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #2 Rhythm ChangeScenario #2 Rhythm Change
��Rhythm observed during a 10 second Rhythm observed during a 10 second pause in CPR pause in CPR –– what do you do now?what do you do now?

Scenario #2 12 Lead EKGScenario #2 12 Lead EKG
�� If you have time and opportunity, If you have time and opportunity, obtain a 12 lead EKG.obtain a 12 lead EKG.

Scenario #3Scenario #3
��You have a 72 yearYou have a 72 year--old male who old male who complains of slight chest pressure complains of slight chest pressure but believes it is related to the cold but believes it is related to the cold he has had for the past few days.he has had for the past few days.
��Patient is awake, cooperative, dizzy.Patient is awake, cooperative, dizzy.
��Lungs clear but breath sounds are Lungs clear but breath sounds are decreased, skin pale, cool, and decreased, skin pale, cool, and clammy with slight lip cyanosis.clammy with slight lip cyanosis.
��VS: B/P 92/60; P VS: B/P 92/60; P –– 30; RR 30; RR -- 2424

Scenario #3 RhythmScenario #3 Rhythm
��What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #3 Rhythm ChangeScenario #3 Rhythm Change
�� You observe 1:1 capture on the monitorYou observe 1:1 capture on the monitor
�� Document rate (80) and what mA setting Document rate (80) and what mA setting you turned up toyou turned up to
�� Monitor patient’s tolerance and need for Monitor patient’s tolerance and need for ValiumValium

Scenario #4Scenario #4
��Your 72 yearYour 72 year--old patient has been ill old patient has been ill for the past 4 days with flufor the past 4 days with flu--like like symptoms. She has mild shortness of symptoms. She has mild shortness of breath and has nausea, vomiting, breath and has nausea, vomiting, and diarrhea. and diarrhea. and diarrhea. and diarrhea.
��Alert & oriented; skin pale, cool and Alert & oriented; skin pale, cool and dry with signs of dehydrationdry with signs of dehydration
��VS: B/P 90/60; P VS: B/P 90/60; P –– 56; RR 56; RR –– 26; 26; SpOSpO22 93%93%

Scenario #4 RhythmScenario #4 Rhythm
�� What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #5Scenario #5
��Your patient is a 67 yearYour patient is a 67 year--old female old female with complaints of confusion, nausea, with complaints of confusion, nausea, abdominal cramps, weakness, and abdominal cramps, weakness, and dizziness. They appear apathetic. They dizziness. They appear apathetic. They deny chest pain or shortness of deny chest pain or shortness of deny chest pain or shortness of deny chest pain or shortness of breath.breath.
��Hx: MI 4 years ago, CHF, COPD, Hx: MI 4 years ago, CHF, COPD, �� B/PB/P
��VS: 100/48; P VS: 100/48; P –– 60; RR 60; RR –– 2020
��Skin pink, cool, dry. Lungs clearSkin pink, cool, dry. Lungs clear

Scenario #5 RhythmScenario #5 Rhythm
��What is this rhythm and what is the What is this rhythm and what is the clinical significance for this patient?clinical significance for this patient?

Scenario #5Scenario #5
��Prepare for the TCPPrepare for the TCP–– In the demand/automatic mode the TCP In the demand/automatic mode the TCP
will function when the patient’s heart will function when the patient’s heart rate drops and will go into the standby rate drops and will go into the standby mode when their heart rate picks upmode when their heart rate picks upmode when their heart rate picks upmode when their heart rate picks up
��Consider Valium for the chest wall Consider Valium for the chest wall discomfortdiscomfort
��Obtain and transmit a 12 lead EKGObtain and transmit a 12 lead EKG––All EKG’s are to be interpreted by EMS All EKG’s are to be interpreted by EMS
for ST elevation whether they are for ST elevation whether they are transmitted or nottransmitted or not

BibliographyBibliography
�� Aehlert, B. ECG’s Made Easy. 3Aehlert, B. ECG’s Made Easy. 3rdrd Edition. Edition. Elsevier. 2006.Elsevier. 2006.
�� CMC EMS System February 2009 CE. CMC EMS System February 2009 CE. 12 12 Lead EKG’sLead EKG’s..
Region X SOP’s March 2007, Amended Region X SOP’s March 2007, Amended �� Region X SOP’s March 2007, Amended Region X SOP’s March 2007, Amended January 1, 2008January 1, 2008
�� www.ambulancetechnicianstudy.co.ukwww.ambulancetechnicianstudy.co.uk
�� www.davidge2.umaryland.edu/~emig/gif/www.davidge2.umaryland.edu/~emig/gif/pared2.gifpared2.gif
�� www.emedu.org/ecg/images/ami2b_ia.jpg www.emedu.org/ecg/images/ami2b_ia.jpg


















