An orthopaedic overview. Characteristic Hip Pains: ◦ Dull ache- OA, degenerative, tendinitis/...
41
An orthopaedic overview
-
Upload
philomena-stafford -
Category
Documents
-
view
222 -
download
0
Transcript of An orthopaedic overview. Characteristic Hip Pains: ◦ Dull ache- OA, degenerative, tendinitis/...

An orthopaedic overview

Characteristic Hip Pains: ◦ Dull ache- OA, degenerative, tendinitis/
bursitis◦ Sharp – Impingement, acute sprain, labrum
tear, subluxation/dislocation, fracture Pain frequently noted in groin and
medial thigh Symptoms: pain, weakness,
numbness, clicking, giving way Referred Pain from: Back, Abdomen,
Pubic symphysis Refers Pain to: knee





Mechanism: High energy:◦ Motor vehicle crash (50-60%) ◦ Motorcycle crash (10-20%) ◦ Pedestrian versus car (10-20%) ◦ Falls (8-10%) ◦ Crush (3-6%)
Physical examination is specific for pelvic instability, but it has a low sensitivity: high level of suspicion
Pain, swelling, WB/NWB, deformity, crepitus, Consider Blood loss and signs of shock GU exam: rectal tone, bladder control,
perineum, boggy prostate, scrotal hematoma, hematuria
digital rectal examination has a very low sensitivity for diagnosing pelvic fractures

Management: pelvic binder (T-pod), IV, analgesia, Blood,
Evacuation for surgical assessment X-ray: pelvic ring- usually disrupted
in 2 places Tile classification: based on the
integrity of the posterior sacroiliac complex
Young classification system is based on mechanism of injury
Death most commonly due to hemorrhage or multiple injuries


Mechanism: high velocity trauma, MVA, falls from height
Multiple fracture patterns: MOI Pain, non WB, presentations of
hip, Neurovascular exam, abdominal
exam, LLD, position of lower limb Stabilize, IV, analgesic, Evacuation for X-ray, surgical
assessment 20% concomitant pelvic fracture

“People come into this world under the brim of the pelvis and leave it by the neck of the femur.”


MOI: Young- MVA, fall from height◦ Older: simple fall, Osteoporosis: abrupt
step, Runners: stress fractures Acute onset hip pain, unable to
WB O/E: shortened leg, external
rotation, painful ROM, crepitus Neurovascular exam Stabilize, IV, analgesia Evacuation for X-ray and surgical
assessment


Garden Classification: 1-4
Treatment: ◦ Young: internal
fixation (+/- reduction)
◦ Older: internal fixation non displaced, hemi-arthroplasty

Extra-capsular fracture including the greater and lesser trochanter (b/w neck and shaft)
Traumatic force to trochanteric area
Acute pain, unable to WB, shortened, ER
Stabilize, IV, analgesic Evacuation for X-ray, surgical
assessment Treatment: Dynamic Hip Screw
fixation

Mechanism: high energy trauma Pain, deformity, Non WB Neurovascular status: urgent
reduction? Procedural sedation, blood loss into fracture site…1000mL
Reduction, immobilize, IV, analgesia, Blood products, +/- antibiotics
Evacuation to surgical capability Surgery: internal fixation- IM nail/
plate

Complications: ◦Haemorrhage requiring transfusion◦Fat embolism – ARDS◦Increased risk of open fracture◦Nerve injury◦Infection

Supracondylar: above condyles Condylar, Inter-condylar= intra-
articular involvement Mechanism: high energy force,
axial load Pain, hemarthrosis, non WB, ER,
shortened Immobilize, IV, analgesia Evacuation for surgical fixation Complication: femoral artery tear
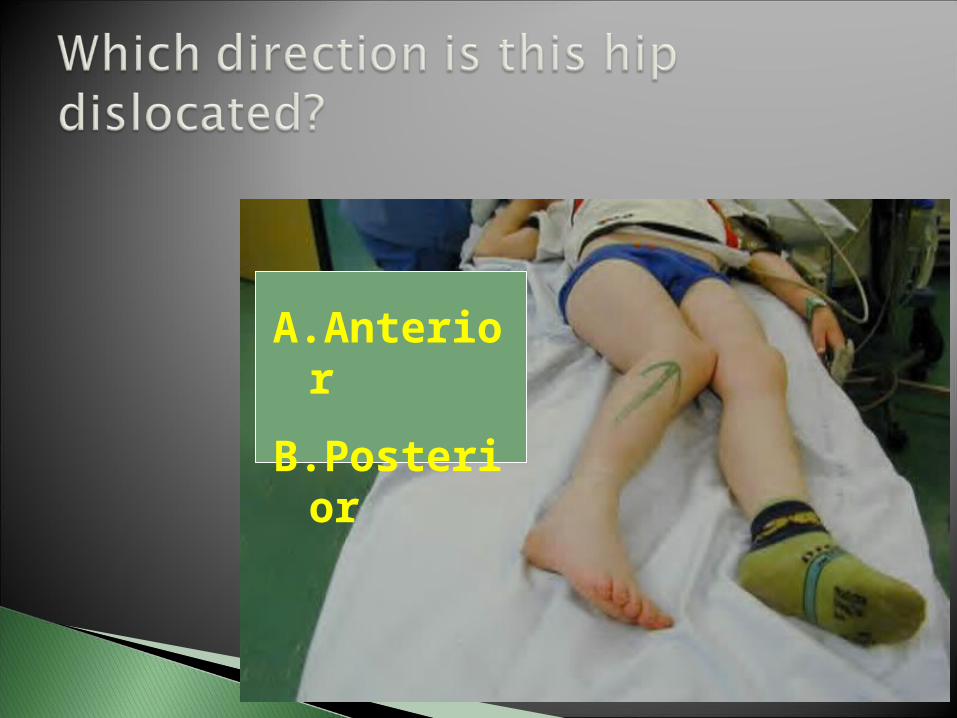
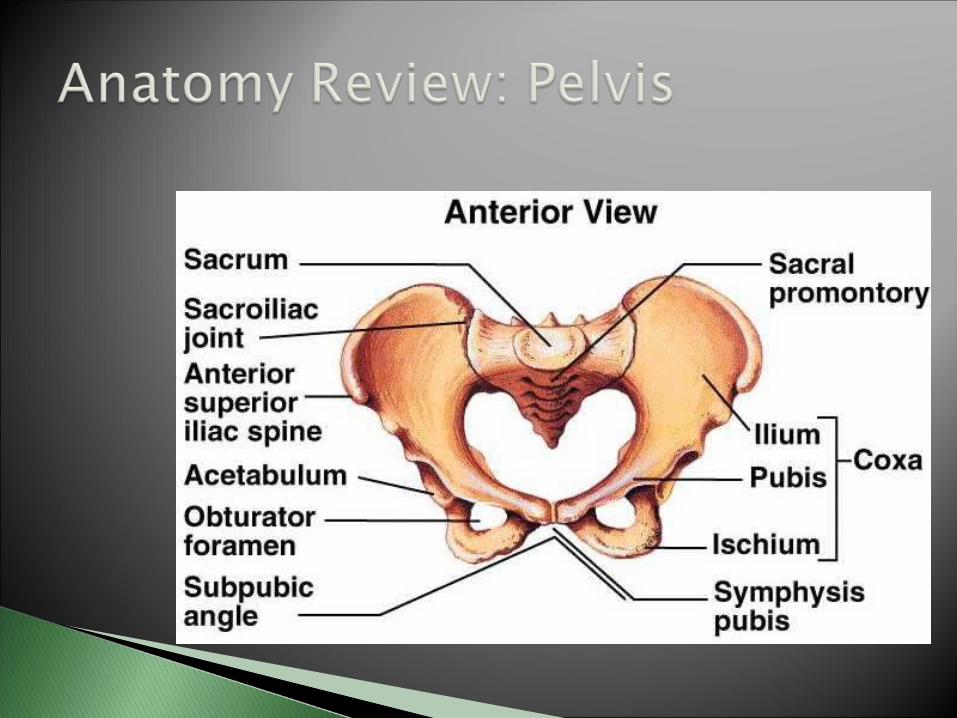
A.Anterior
B.Posterior



***Orthopaedic Emergency
Mechanism: blow to knee in hip abduction
Shortened, abducted, ER limb Neurovascular exam Stabilize, IV, analgesia, Urgent Evacuation for X-ray,
reduction under sedation/GA Complications: as per posterior

***Orthopaedic Emergency Mechanism: high force through
femur with hip in flexion and adduction (dashboard )
Pain, Shortened, Add and IR of hip

Stabilize, IV, analgesia, Urgent Evacuation for X-ray- r/o
fracture, reduction under sedation/ GA, ORIF
risk of AVN with delayed reduction (>6 hrs)

Slow onset degenerative change often following injury or prolonged exposure to impact, poor biomechanics, congenital hip disorder
Pain into groin and medial thigh worse with activity, intermittent flares
with acute pain and swelling
O/E: trendelenberg gait, decreased ROM, strength deficit, ligament laxity
X-ray: decreased joint space, osteophyte formation, sclerosis of femoral head, subchondral cysts
Treatment: NSAIDS for acute flare, Tylenol/NSAID for long-term analgesia
Physiotherapy: ROM, strengthening, gait aids
Partial/Total hip replacement

Etiology: Loss of vascular supply to femoral head
Primarily distal to proximal intra-osseous blood supply
Predisposing factors: systemic steroid, dislocation of femur, fracture of femoral neck, chronic alcohol use, sickle cell, septic arthritis, “the Bends”

Symptoms: Pain in groin, worse with WB O/E: abnormal range of motion if collapse of
cartilage on femoral head Normal strength on manual muscle testing Pain on compression testing X-ray may show crescent sign Treatment: Non WB until new bone
formation
Etiology: trauma to hip, abnormal gait mechanics, muscle tightness, over-training
Rule out cellulitis or infection Pain at lateral aspect of hip, worse with
weight bearing/ walking/ direct pressure O/E: pain on palpation over greater
trochanter, +/- tight ilio-tibial band, muscle imbalance, pain on single leg stance

Treatment: Rest, Ice, NSAIDS Physiotherapy for stretching, muscle
imbalance Consider corticosteroid injection for
refractive conditions

Abnormal contact between the acetabulum and femoral head-neck junction
Primarily an impingement issue Groin pain with activity or extreme ROM Usually younger active people Can lead to labral tears




A. Rectus femoris
B. Vastus lateralis


Adductors: groin pull Hip flexors: Rectus femoris strain Snapping hip: iliopsoas Piriformis syndrome Iliotibial band syndrome Gluteal strain

Let’s take a break.