An introduction to haematological malignancies
29
HAEMATOLOGICAL MALIGNANCY Benjamin Smeeton (Year 4) An introduction to PART ONE
-
Upload
meducationdotnet -
Category
Documents
-
view
2.525 -
download
1
Transcript of An introduction to haematological malignancies

HAEMATOLOGICAL MALIGNANCY
Benjamin Smeeton (Year 4)
An introduction to PART ONE
What are we going to cover?
(1) The Basicsi)Haematopoiesis
ii)Extra-medullary haematopoiesis
(1) Common malignanciesi)Leukaemias
ii)Myeloproliferative disorders
iii)Multiple myeloma
(2) Questions
}An integrated approachFor each disease we will explore the basic pathological concepts underpinning the clinical manifestations.
Don’t worry
we’ll all go
over them
together!

A quick quiz to test your existing knowledge!
(1)A 63 year old female presents to her GP with general fatigue and lethargy of 6 months duration. She suffers from HTN, but is otherwise well. A FBC reveals WBCs and Hb ↑ ↓(iron, B12 and folate are normal). The doctor orders a blood film.
Examination of the blood film reveals large reticulocytes and damaged red cells. The presence of characteristic smear cells is also noted.
What is the most likely diagnosis?
• Acute myeloid leukaemia
• Multiple myeloma
• Iron deficiency anaemia
• Chronic lymphocytic leukaemia
• Essential thrombocythaemia

(2)A 4 year old boy presents with his mother. His mother explains he has had a widespread rash for 7 days and that he has been ‘somewhat lethargic’ for the last 2 weeks. O/E: he is pale, with a widespread purpuric rash but there is no fever or meningism; generalised non-tender lymphadenopathy and splenomegaly are also noted. A FBC reveals WCC, ↓
Hb, Plts and a blood film is ordered.↓ ↓
Examination of the blood film reveals blast cells.
What is the most likely diagnosis?
• Bacterial meningitis
• Acute myeloid leukaemia
• Acute lymphoblastic leukaemia
• Chronic lymphocytic leukaemia
• Essential thrombocythaemia
A quick quiz to test your existing knowledge!
(3)A 65 year old man presents to his GP with intermittent headache and dizziness of 6 months duration. He has also noted an unpleasant burning sensation in his hands and feet, especially when he is in the shower. O/E: both his big and first toes of his right foot are dusky in colour and tender to touch.
What single pathological process is most likely to account for his symptoms?
• Bone marrow failure
• Plasma cell proliferation
• Chronic haemolysis
• Chronic lymphocytic leukaemia
• Myeloproliferation
A quick quiz to test your existing knowledge!
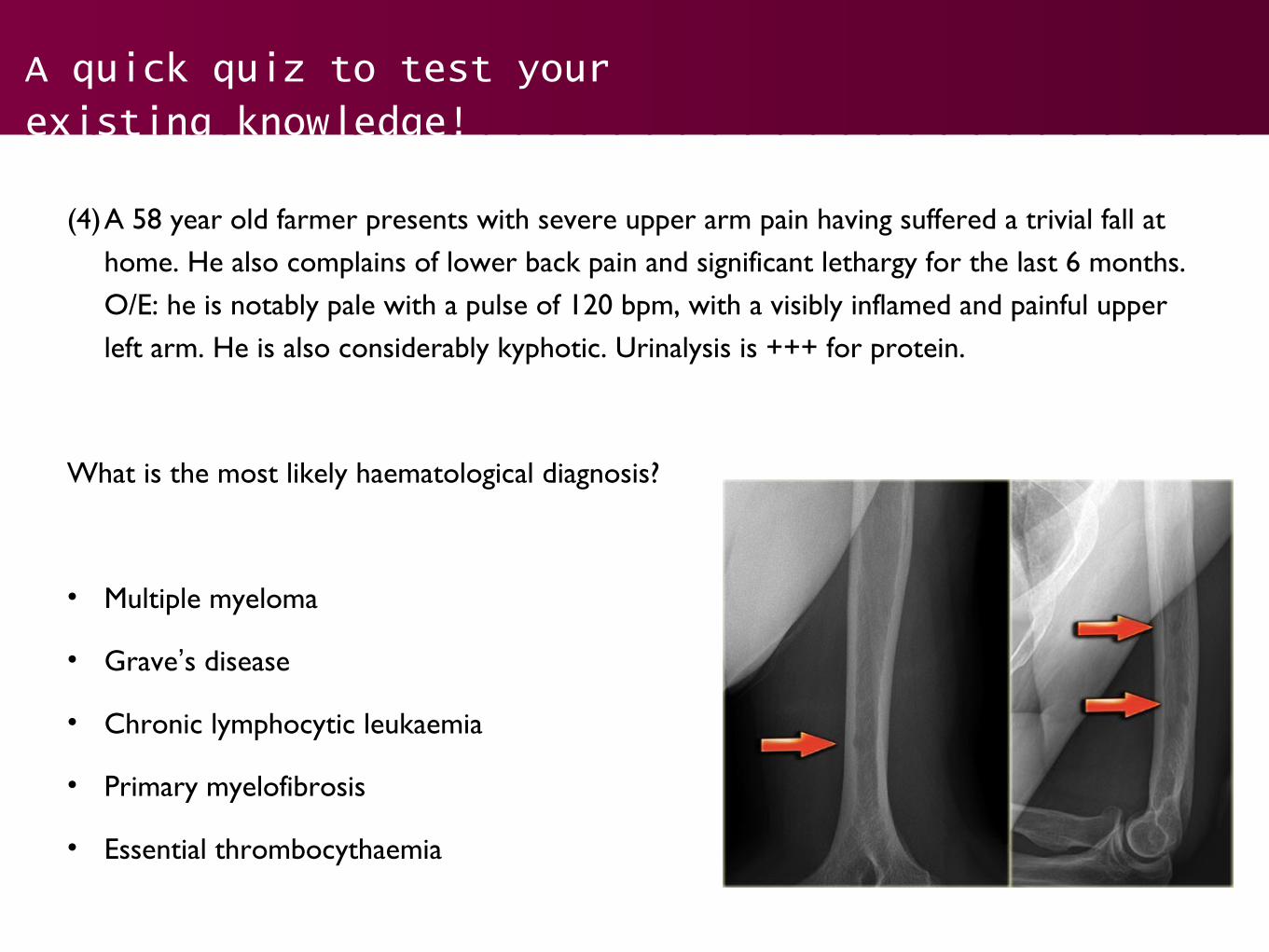
(4)A 58 year old farmer presents with severe upper arm pain having suffered a trivial fall at home. He also complains of lower back pain and significant lethargy for the last 6 months. O/E: he is notably pale with a pulse of 120 bpm, with a visibly inflamed and painful upper left arm. He is also considerably kyphotic. Urinalysis is +++ for protein.
What is the most likely haematological diagnosis?
• Multiple myeloma
• Grave’s disease
• Chronic lymphocytic leukaemia
• Primary myelofibrosis
• Essential thrombocythaemia
A quick quiz to test your existing knowledge!

The Basics: Haematopoiesis
Pluripoten
t
haematopoi
etic stem
cell
Myeloid
stem
cell
Lymphoid stem cell
Megakaryocyte
Platelets RBC Monocyte Neutrophil
Basophil Eosinophil
B-lymphocyt
e
T-lymphocyt
e
Plasma cell

The Basics: Haematopoiesis
• In an adult, all blood cells are produced in the red marrow. Restricted to the bones of the axial skeleton (vertebrae, ribs, sternum, skull, sacrum, pelvis and femur).
• In fetal life, the major haemopoietic tissues are:
• Yolk sac (before 6 weeks).
• Liver and spleen (6 weeks to 6-7 months). In disease, the liver and spleen can again become haemopoietic, even in adult life (extramedullary haemopoiesis).

Common malignancies: introduction
• The same basic pathological mechanism underpins a large number of haematological malignancies.Essentially, a haemopoietic stem cell in the BM acquires genetic mutations which disrupt the normal differentiation and maturation of its progeny.
• The resulting disease depends on how these mutations affect the differentiation pathway.
MUTATED
Pluripoten
t
haematopoi
etic stem
cell

Common malignancies: overview
More indolent
UndifferentiatedAcute
leukaemias
(ALL /
AML)
Chronic lymphocytic leukaemia
(CLL)
Chronic myeloid leukaemia
(CML)
Differentiated
Normal differentiation
Abnormal differentiation
Myeloid
cell
line
Lymphoid cell line
Myeloproliferative disorder
Myelodysplastic disorder
Lymphomas
Dealt with as a
slightly
separate entity!
More aggressive

Common malignancies: what we will be covering!
(1) Leukaemiasi) Acute lymphoblastic (ALL)ii) Acute myeloid (AML)iii) Chronic lymphocytic (CLL)
• Myeloproliferative
• Chronic myeloid leukaemia*• Polycythaemia vera• Essential thrombocythaemia• Primary myelofibrosis
(3) Othersi) Multiple myelomaii) Myelodysplastic disorders
i)Lymphomas(4)Hodgkin(5)Non-Hodgkin
Although it is
a
leukaemia it i
s
also considere
d a
myeloprolifera
tiv
e disorder!
These will be covered in detail in Part II
Acute leukaemias: ALL & AML
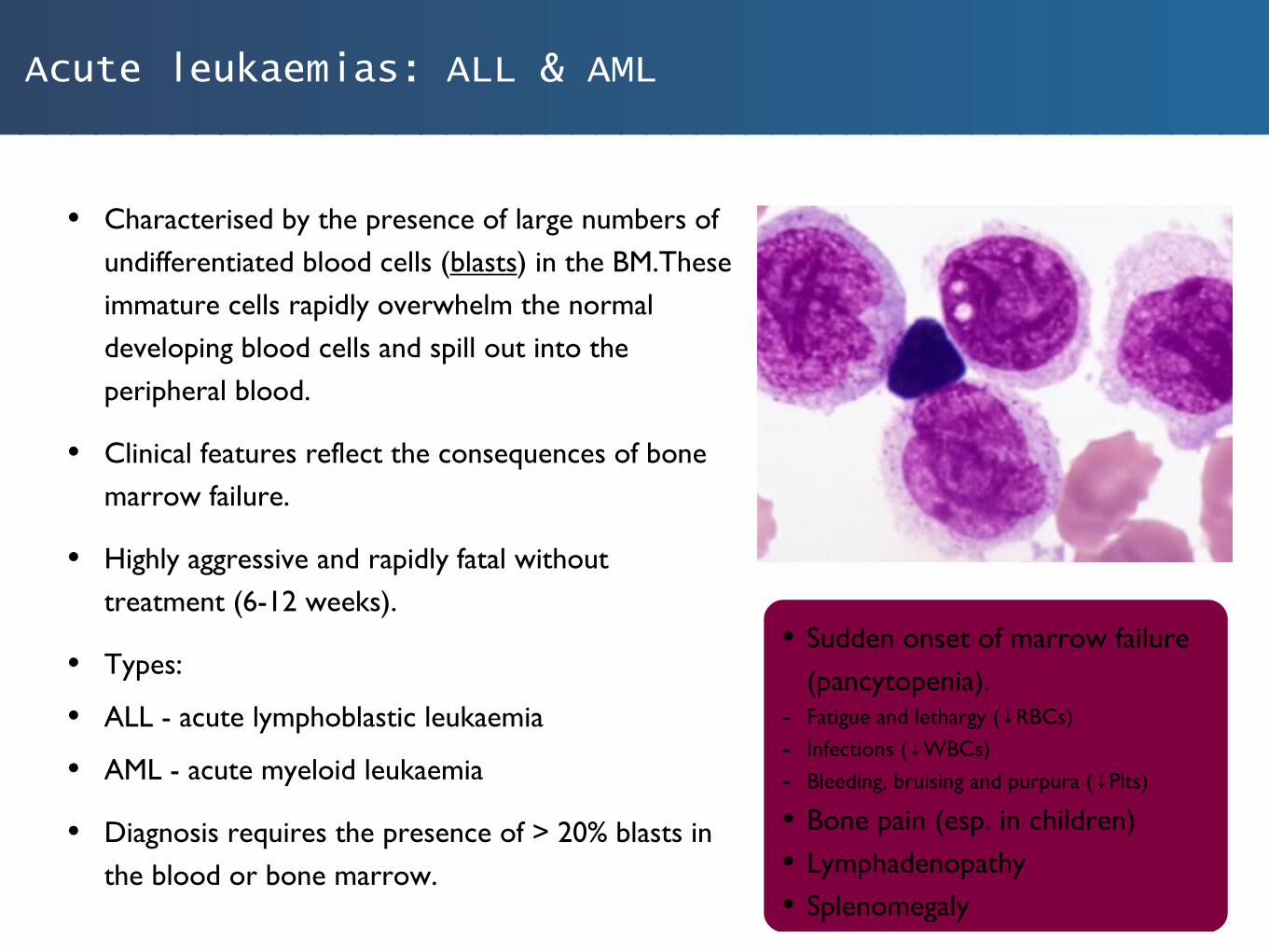
• Characterised by the presence of large numbers of undifferentiated blood cells (blasts) in the BM.These immature cells rapidly overwhelm the normal developing blood cells and spill out into the peripheral blood.
• Clinical features reflect the consequences of bone marrow failure.
• Highly aggressive and rapidly fatal without treatment (6-12 weeks).
• Types:
• ALL - acute lymphoblastic leukaemia
• AML - acute myeloid leukaemia
• Diagnosis requires the presence of > 20% blasts in the blood or bone marrow.
• Sudden onset of marrow failure (pancytopenia).
- Fatigue and lethargy ( RBCs)↓- Infections ( WBCs)↓- Bleeding, bruising and purpura ( Plts)↓
• Bone pain (esp. in children)• Lymphadenopathy• Splenomegaly

Acute leukaemias: ALL & AML
• ALL (acute lymphoblastic leukaemia):
• Commonest childhood cancer (peak incidence at age 2-4 years)
• Modern treatment has improved prognosis significantly (4 stages - induction, consolidation, CNS prophylaxis, and maintenance)
• Male gender and age > 10 years represent negative prognostic factors.
• AML (acute myeloid leukaemia):
• May occur at any age, but becomes increasingly common in older people.
• Down’s syndrome = 400x greater incidence.
• Poor prognosis, patients over the age of 70 rarely survive beyond 1 year.
• Sudden onset of marrow failure (pancytopenia).
- Fatigue and lethargy ( RBCs)↓- Infections ( WBCs)↓- Bleeding, bruising and purpura ( Plts)↓
• Bone pain (esp. in children)• Lymphadenopathy• Splenomegaly
Chronic leukaemias: Chronic Lymphocytic Leukaemia
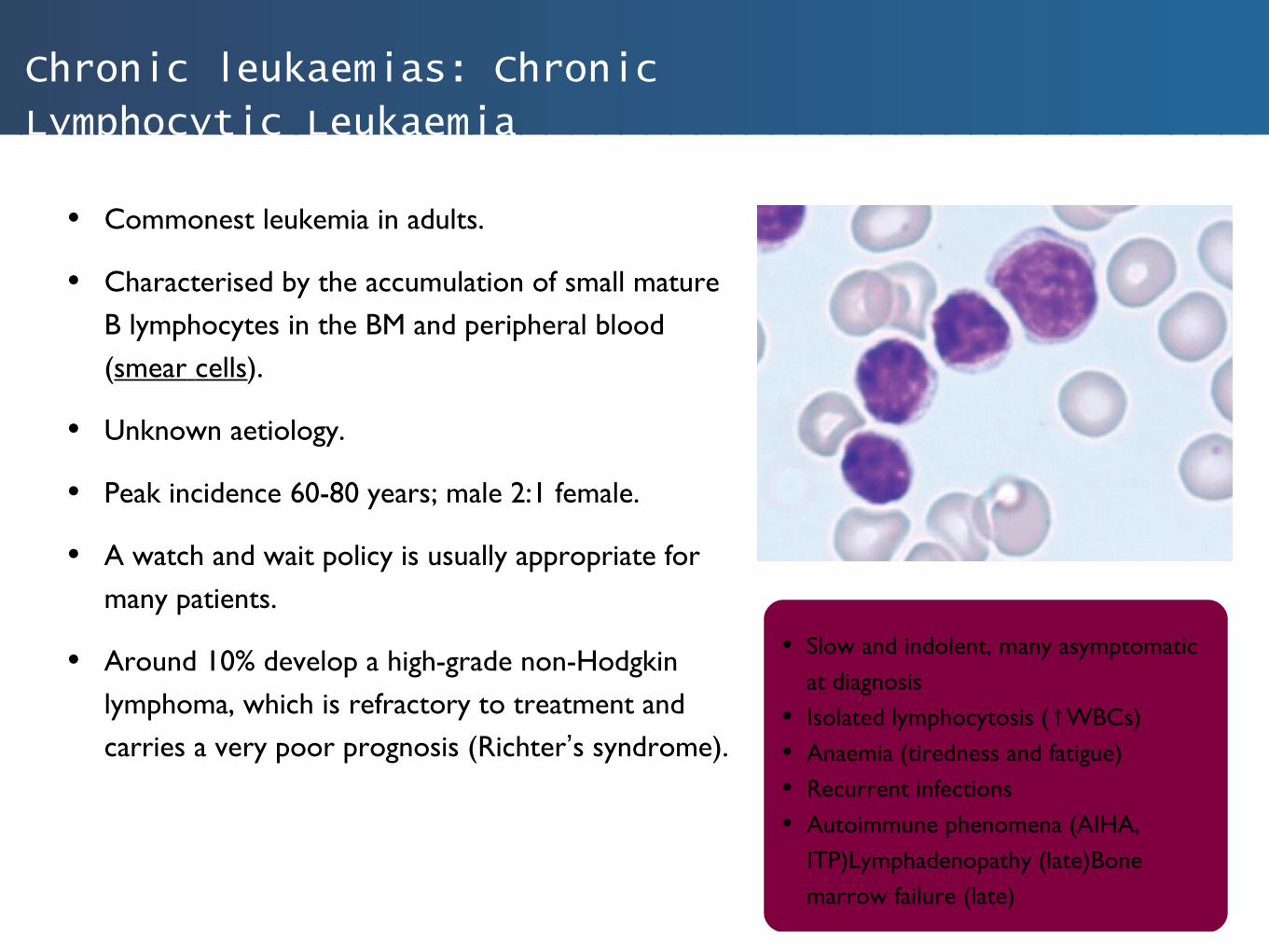
• Commonest leukemia in adults.
• Characterised by the accumulation of small mature B lymphocytes in the BM and peripheral blood (smear cells).
• Unknown aetiology.
• Peak incidence 60-80 years; male 2:1 female.
• A watch and wait policy is usually appropriate for many patients.
• Around 10% develop a high-grade non-Hodgkin lymphoma, which is refractory to treatment and carries a very poor prognosis (Richter’s syndrome).
• Slow and indolent, many asymptomatic at diagnosis
• Isolated lymphocytosis ( WBCs)↑• Anaemia (tiredness and fatigue)• Recurrent infections• Autoimmune phenomena (AIHA,
ITP)Lymphadenopathy (late)Bone marrow failure (late)

Myeloproliferative disorders: overview
• A group of neoplastic disorders characterised by the overproduction of normal myeloid cells.
• Occur mostly in the elderly.
• Caused by a genetic abnormality which bestows a proliferation advantage to one or more myeloid cell lineages.
• Types:
• Chronic myeloid leukaemia ( neutrophils)↑
• Polycythaemia vera ( RBCs)↑
• Essential thrombocythaemia ( Plts)↑
• Primary myelofibrosis ( Megakaryocytes)↑
• Diagnosis is difficult as blood cell overproduction can often be a normal physiological response.
Chronic myeloid leukaemia
(CML)Polycythaemi
a vera
Essential thrombocytha
emia
PlateletsRBCNeutrophil
MUTATED
Myeloid
stem cell

Myeloproliferative disorders: Chronic Myeloid Leukaemia
• CML is the most common myeloproliferative disorder.
• Very rare in children; incidence increases with age.
• Examination of the peripheral blood reveals large numbers of neutrophils and neutrophil precursors.
• Associated with the Philadelphia chromosome.
• 95% possess the t(9;22) translocation.
• The translocation produces an abnormal fusion gene, BCR-ABL, which generates a protein with excessive tyrosine kinase growth signaling properties.
• Tx. imatinib (tyrosine kinase inhibitor - not curative).
• Pallor• Night sweats• Fatigue, weight loss and anorexia.• Massive splenomegaly• Begins with a ‘chronic’ phase (5
years) which then spontaneously transforms into a ‘blast’ crisis with fulminant bone marrow failure.

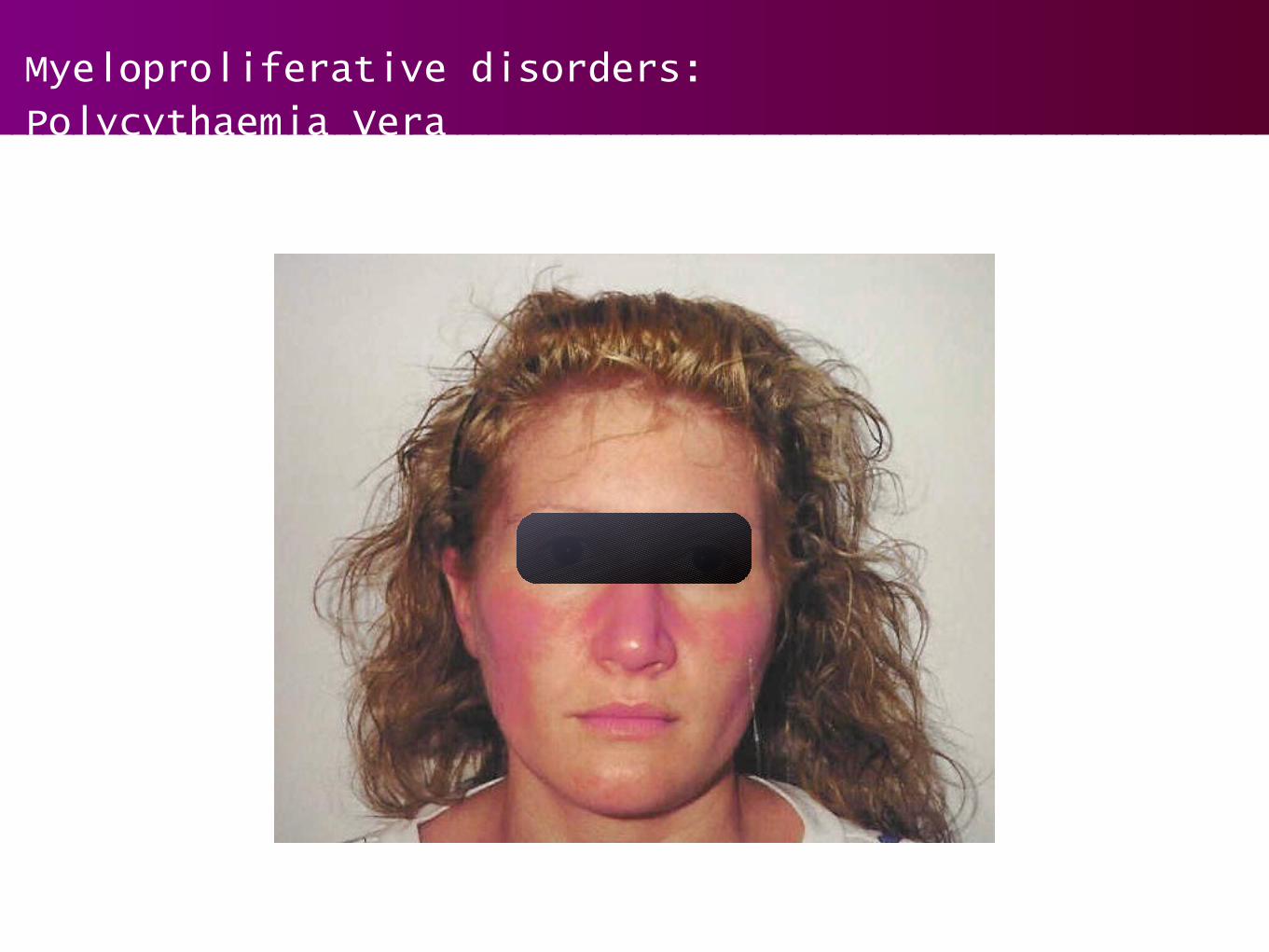
Myeloproliferative disorders: Polycythaemia Vera
• Increased production of RBCs.
• Excess proliferation of other myeloid lineages is usually seen ( neu plts).↑ ↑
• Rarely presents before age 40.
• 90% of cases associated with a mutation in the erythropoietin signaling pathway (JAK-2).
• The key to diagnosis is the exclusion of a secondary physiological erythrocytosis.
• Chronic hypoxia (e.g. lung disease)
• ↑EPO secretion (e.g. RCC, PCKD)
• Thrombosis is a serious risk.
• With treatment (venesection), patients often survive 10 years; most die from thrombosis / haemorrhage.
• Plethora (red face)• Erythromelalgia (burning red skin)• Pruritus (particularly after hot
baths)• Hepatosplenomegaly• Headache, dizziness and stroke ( ↑
blood viscosity).• Mesenteric, portal or splenic vein
thrombosis.
Myeloproliferative disorders: Polycythaemia Vera

Myeloproliferative disorders: Essential Thrombocythaemia
• Increased production of platelets (megakaryocyte cell line).
• Platelet count > 600 x 109/L (normal = 150-400)
• Difficult to differentiate from reactive causes of thrombocytosis (e.g. infection, malignancy).
• 50% possess JAK-2 mutation.
• Usually affects older patients; presents with thrombotic or bleeding complications.
• An indolent condition with a median survival of 12-15 years.
• Rarely transforms into an acute leukaemia.
• Many asymptomatic (25%)• Erythromelalgia and digital ischaemia
(intense burning and pain)• Stroke• Recurrent abortions and fetal
growth retardation• Hepatic and portal vein thrombosis
(e.g. Budd-Chiari syndrome)
Myeloproliferative disorders: Primary Myelofibrosis
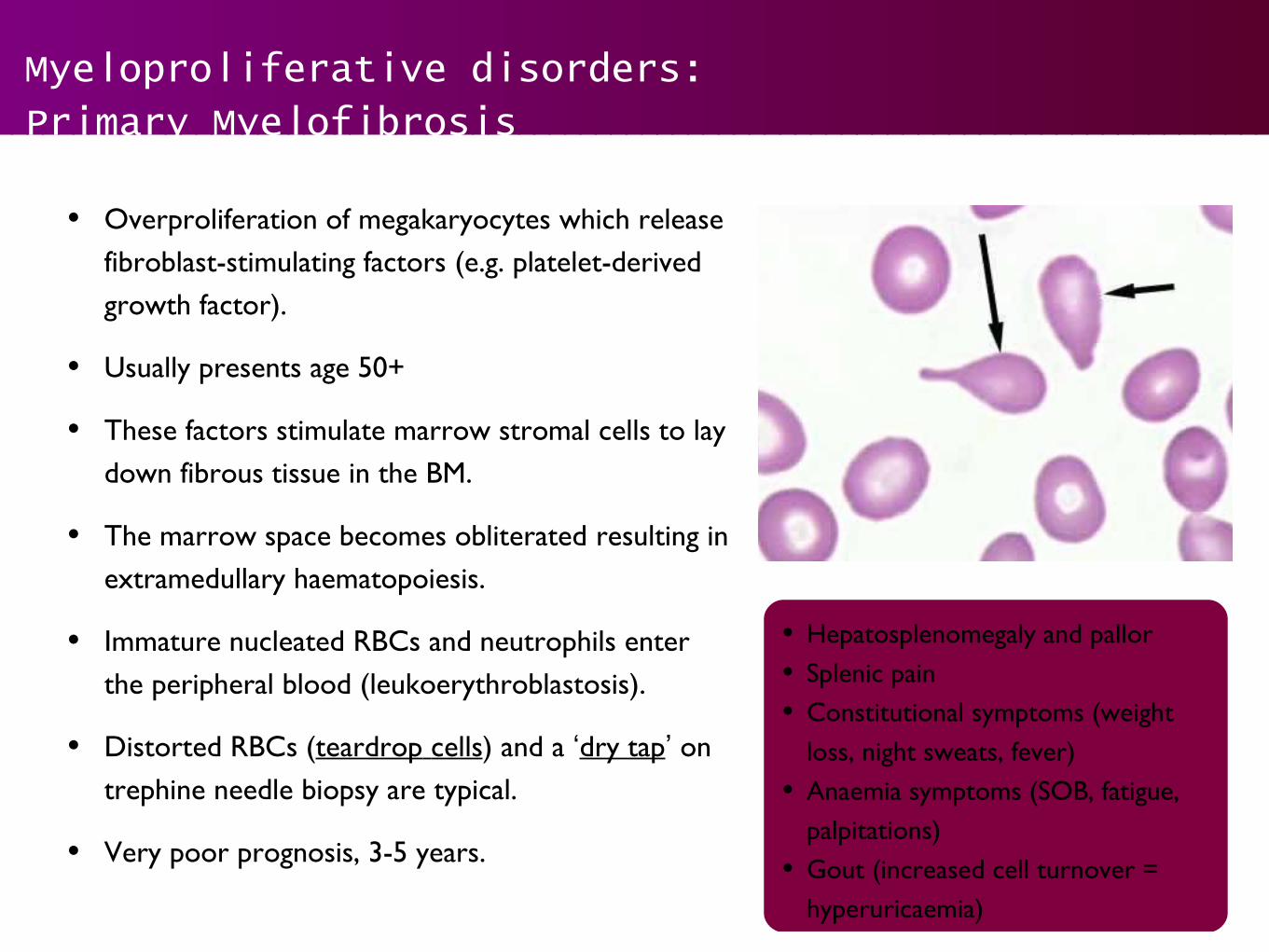
• Overproliferation of megakaryocytes which release fibroblast-stimulating factors (e.g. platelet-derived growth factor).
• Usually presents age 50+
• These factors stimulate marrow stromal cells to lay down fibrous tissue in the BM.
• The marrow space becomes obliterated resulting in extramedullary haematopoiesis.
• Immature nucleated RBCs and neutrophils enter the peripheral blood (leukoerythroblastosis).
• Distorted RBCs (teardrop cells) and a ‘dry tap’ on trephine needle biopsy are typical.
• Very poor prognosis, 3-5 years.
• Hepatosplenomegaly and pallor• Splenic pain• Constitutional symptoms (weight
loss, night sweats, fever)• Anaemia symptoms (SOB, fatigue,
palpitations)• Gout (increased cell turnover =
hyperuricaemia)

Others: Multiple Myeloma
• A malignant disease of plasma cells in the BM.
• Unknown aetiology.
• Generalised BM involvement; although areas of greatest haematopoietic activity (vertebrae, ribs and skull) are predominantly affected.
• Malignant plasma cells produce a single non-functioning monoclonal immunoglobulin (paraprotein) in large quantities.
• The abnormal plasma cells also produce free immunoglobulin light chains, which are readily filtered and excreted by the kidneys (Bence-Jones protein).
Plasma cell
YYY YY
Y
Y
Y
YYY YY
Y
Y
YYY
YY
Y
Y
YYYYY
Y YY
YY
Y
Y

Others: Multiple Myeloma
• Clinical features:
• Bony destruction: proliferating plasma cells stimulate osteoclast activity (lytic lesions).
• Immunosuppression: production of normal immunoglobulins is impaired, leading to immune paresis (recurrent infections).
• Renal failure: free light chains produced by the malignant cells become trapped in the renal tubules resulting in kidney damage.
• Diagnosis:
• Serum electrophoresis (serum paraprotein)
• Urine electrophoresis (Bence-Jones protein)
• Bone marrow aspirate (demonstrates plasma cell infiltration).
• Peak age 50-60 years.Bone destruction / pain
• Renal failure• Bone marrow failure• Immunodeficiency• Hypercalcaemia• Amyloidosis (peripheral neuropathy,
cardiomyopathy etc)

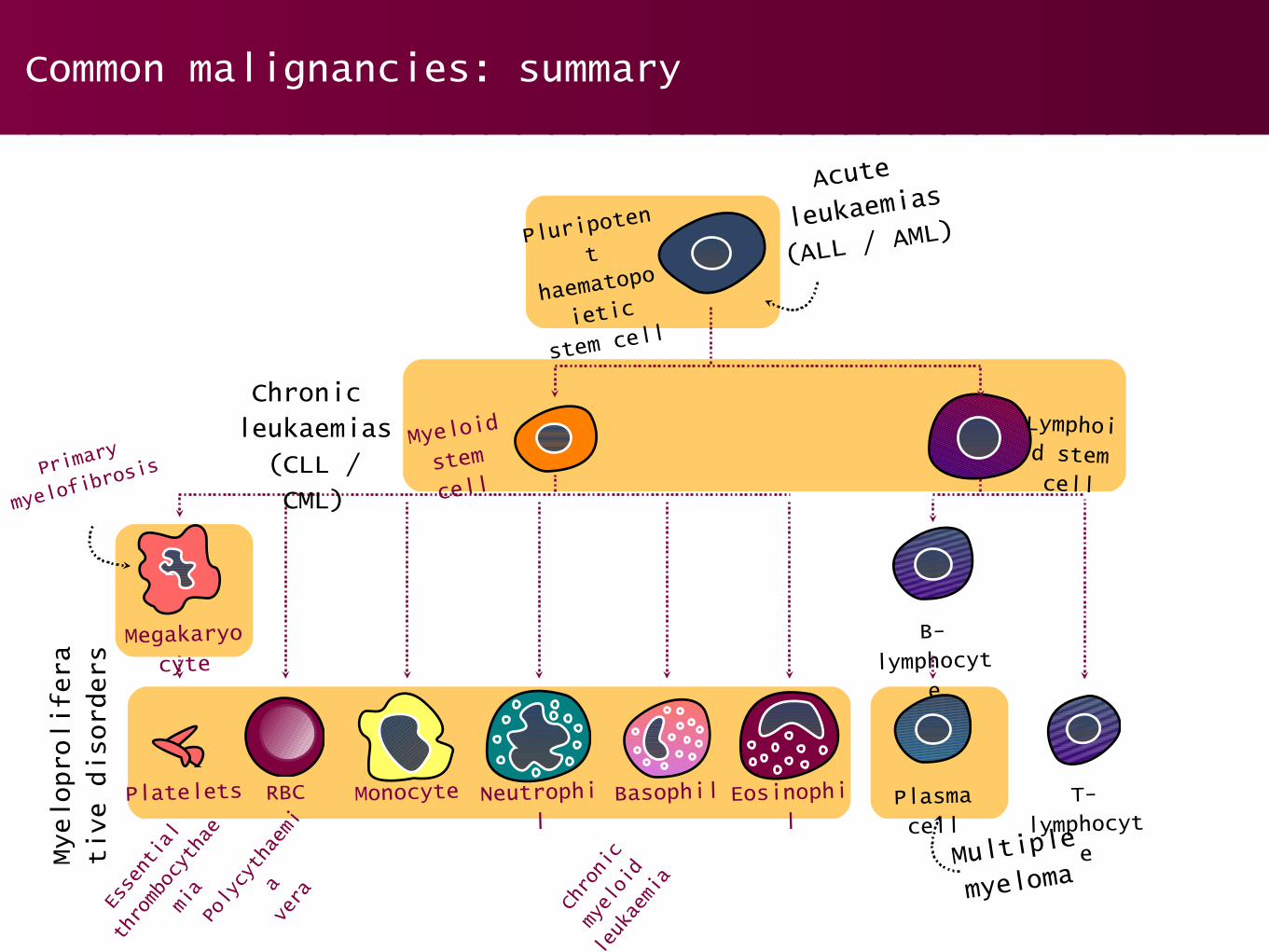
Common malignancies: summary
• The same basic pathological mechanism underpins a large number of haematological malignancies.Using knowledge of haematopoiesis, the haematological malignancies can be categorised into:
• Acute leukaemias
• Chronic leukaemias
• Myeloproliferative disorders
• Others (e.g. myeloma)
• In part two of this series, we will be covering the topic of lymphoma.
Common malignancies: summary
Pluripoten
t
haematopo
ietic
stem cell
Myeloid
stem
cell
Lymphoid stem cell
Megakaryocyte
Platelets RBC Monocyte Neutrophil
Basophil Eosinophil
B-lymphocyt
e
T-lymphocyt
e
Plasma cell
Acute
leukaemias
(ALL / AML)
Chronic leukaemias(CLL / CML)
Myelop
rolifera
tive d
isor
ders
Essential
thrombocythae
mia
Polycythaemi
avera Chronic
myeloid
leukaemia
Primary
myelofibro
sis
Multiple
myeloma

SBA questions: haematology quiz
(1)A 63 year old female presents to her GP with general fatigue and lethargy of 6 months duration. She suffers from HTN, but is otherwise well. A FBC reveals WBCs and Hb ↑ ↓(iron, B12 and folate are normal). The doctor orders a blood film.
Examination of the blood film reveals large reticulocytes and damaged red cells. The presence of characteristic smear cells is also noted.
What is the most likely diagnosis?
• Acute myeloid leukaemia
• Multiple myeloma
• Iron deficiency anaemia
• Chronic lymphocytic leukaemia
• Essential thrombocythaemia

SBA questions: haematology quiz
(2)A 4 year old boy presents with his mother. His mother explains he has had a widespread rash for 7 days and that he has been ‘somewhat lethargic’ for the last 2 weeks. O/E: he is pale, with a widespread purpuric rash but there is no fever or meningism; generalised non-tender lymphadenopathy and splenomegaly are also noted. A FBC reveals WCC, ↓
Hb, Plts and a blood film is ordered.↓ ↓
Examination of the blood film reveals blast cells.
What is the most likely diagnosis?
• Bacterial meningitis
• Acute myeloid leukaemia
• Acute lymphoblastic leukaemia
• Chronic lymphocytic leukaemia
• Essential thrombocythaemia

SBA questions: haematology quiz
(3)A 65 year old man presents to his GP with intermittent headache and dizziness of 6 months duration. He has also noted an unpleasant burning sensation in his hands and feet, especially when he is in the shower. O/E: both his big and first toes of his right foot are dusky in colour and tender to touch.
What single pathological process is most likely to account for his symptoms?
• Bone marrow failure
• Plasma cell proliferation
• Chronic haemolysis
• Chronic lymphocytic leukaemia
• Myeloproliferation

SBA questions: haematology quiz
(4)A 58 year old farmer presents with severe upper arm pain having suffered a trivial fall at home. He also complains of lower back pain and significant lethargy for the last 6 months. O/E: he is notably pale with a pulse of 120 bpm, with a visibly inflamed and painful upper left arm. He is also considerably kyphotic. Urinalysis is +++ for protein.
What is the most likely haematological diagnosis?
• Multiple myeloma
• Grave’s disease
• Chronic lymphocytic leukaemia
• Primary myelofibrosis
• Essential thrombocythaemia
An introduction to haematological malignancy: Part one
Thank you for listening!