AMYLOIDOSIS - Journal of Clinical Pathology › content › jclinpath › 9 › 3 ›...
17
J. clin. Path. (1956), 9, 212. AMYLOIDOSIS FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS AND SOME OTHER UNUSUAL CASES BY W. St. C. SYM MERS From the Departtmzenit of Morbid A natomnv, Chlarinlg Cross Hospital anld Medical Schlool, Lonidon A conception of amyloidosis as merely a compli- cation of chronic syphilitic, tuberculous or septic disease of bones and joints or of chronic intra- thoracic sepsis is no longer adequate. This older view has had to be modified as the association of amyloidosis with other diseases came to be recog- nized: the predisposing diseases are now known to include rheumatic and rheumatoid affections, myelomatosis, Hodgkin's disease, ulcerative colitis, pyelonephritis and a variety of other conditions. In addition, the occurrence of generalized amyloid- osis in the absence of any recognized predisposing cause, that is, " primary amyloidosis," has lately attracted increasing attention. The first indisput- able cases of this sort were reported by Soyka (1876) and Wild (1886), but the condition did not begin to be widely known until after Lubarsch (1929) defined certain pathological differences be- tween this atypical form of amyloidosis and ordin- ary secondary amyloidosis. These differences have proved to be neither absolute nor diagnostic, although they characterize a majority of the cases: in fact, it is now known that there is no one feature which occurs exclusively in any form of amyloidosis. How far primary amyloidosis may be considered an entity remains undecided, but the present tendency is to consider all forms of amyloidosis to be closely related. Various aspects of the history, pathology, aetio- logy, and clinical pictures of amyloidosis, with special reference to primary amyloidosis, have been reviewed elsewhere in this issue. In thz present paper five cases of primary amyloidosis are recorded, and some cases illustrating o.her unusual manifestations and associations of amy- loidosis are described briefly. Cases of Primary Generalized Amyloidosis Case 1: Primary Amyloidosis Presenting with Pro- gressive Heart Failure. A previously healthy builders' foreman, aged 61, began to be short of breath on ordinary exertion, such as hurrying about his business, and this symptom became slowly severer. About a year later his feet and ankles began to swell, and during the next nine months he gradually developed widespread oedema and effusions in the serosal cavi- ties. His doctor found mercurial diuretics and full doses of digitalis to be without effect on these symp- toms, even after repeated tapping of the pleural and peritoneal effusions. Two years after the onset of dyspnoea the patient had become so incapacitated that he at last agreed to go to hospital. On admission he was orthopnoeic, cyanotic, and dropsical. The heart was enlarged and gallop rhythm was present. The pulse (86 per minute) was regular; the blood pressure was 130/70 mm. of mercury. There was gross ascites, a large pleural effusion on the right and a small one on the left. The liver was slightly enlarged. Investigations. Urine: protein + + +; occasional hyaline casts. Blood: erythrocytes 4,600,000 per c.mm.; haemoglobin 12.0 g. per 100 ml. Serum albu- min 3.0 g. per 100 ml., globulin 3.2 g. Blood urea 55 mg. per 100 ml. Kahn test negative. Electro- cardiography showed the usual changes associated with digitalis therapy, and also low, voltage in all leads. Progress. A litre of clear straw-coloured fluid was aspirated from the right pleural cavity and 21 litres from the abdomen. Mersalyl was injected daily, and 0.25 mg. of digoxin given by mouth every six hours: there was no diuresis, his pulse rate dropped to 56 per minute within 48 hours and the beats became coupled. Treatment with digoxin was stopped, and within 24 hours auricular fibrillation developed. From this time his condition deteriorated rapidly. Fourteen days after admission he died suddenly. Necropsi .-There was generalized dropsy., with large pleural and peritoneal transudates. The right lung was completely collapsed ; the left lung was partly collapsed, hyperaemic, and oedematous. A long, coiled thrombus was impacted at the bifurcation of the main pulmonary artery. Partly adherent thrombus filled the deep veins of both calves; the thrombus on the left extended up into the external iliac vein, while that on the right had broken off in the poplitea. The heart (610 g.) was uniformly enlarged, with thickening of the myocardium of all parts and dilatation of all chambers. The myocardium was firm, and mottled with irregular, pale, opaque patches. The valves and endocardium were normal. on July 10, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.9.3.212 on 1 August 1956. Downloaded from
Transcript of AMYLOIDOSIS - Journal of Clinical Pathology › content › jclinpath › 9 › 3 ›...

J. clin. Path. (1956), 9, 212.
AMYLOIDOSISFIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS AND SOME OTHER
UNUSUAL CASESBY
W. St. C. SYM MERSFrom the Departtmzenit of Morbid A natomnv, Chlarinlg Cross Hospital anld Medical Schlool, Lonidon
A conception of amyloidosis as merely a compli-cation of chronic syphilitic, tuberculous or septicdisease of bones and joints or of chronic intra-thoracic sepsis is no longer adequate. This olderview has had to be modified as the association ofamyloidosis with other diseases came to be recog-nized: the predisposing diseases are now knownto include rheumatic and rheumatoid affections,myelomatosis, Hodgkin's disease, ulcerative colitis,pyelonephritis and a variety of other conditions.In addition, the occurrence of generalized amyloid-osis in the absence of any recognized predisposingcause, that is, " primary amyloidosis," has latelyattracted increasing attention. The first indisput-able cases of this sort were reported by Soyka(1876) and Wild (1886), but the condition did notbegin to be widely known until after Lubarsch(1929) defined certain pathological differences be-tween this atypical form of amyloidosis and ordin-ary secondary amyloidosis. These differences haveproved to be neither absolute nor diagnostic,although they characterize a majority of thecases: in fact, it is now known that there is noone feature which occurs exclusively in any formof amyloidosis. How far primary amyloidosismay be considered an entity remains undecided,but the present tendency is to consider all formsof amyloidosis to be closely related.Various aspects of the history, pathology, aetio-
logy, and clinical pictures of amyloidosis, withspecial reference to primary amyloidosis, havebeen reviewed elsewhere in this issue. In thzpresent paper five cases of primary amyloidosisare recorded, and some cases illustrating o.herunusual manifestations and associations of amy-loidosis are described briefly.
Cases of Primary Generalized AmyloidosisCase 1: Primary Amyloidosis Presenting with Pro-
gressive Heart Failure. A previously healthy builders'foreman, aged 61, began to be short of breath onordinary exertion, such as hurrying about his business,and this symptom became slowly severer. About ayear later his feet and ankles began to swell, and
during the next nine months he gradually developedwidespread oedema and effusions in the serosal cavi-ties. His doctor found mercurial diuretics and fulldoses of digitalis to be without effect on these symp-toms, even after repeated tapping of the pleural andperitoneal effusions. Two years after the onset ofdyspnoea the patient had become so incapacitated thathe at last agreed to go to hospital.On admission he was orthopnoeic, cyanotic, and
dropsical. The heart was enlarged and gallop rhythmwas present. The pulse (86 per minute) was regular;the blood pressure was 130/70 mm. of mercury. Therewas gross ascites, a large pleural effusion on the rightand a small one on the left. The liver was slightlyenlarged.
Investigations. Urine: protein + + +; occasionalhyaline casts. Blood: erythrocytes 4,600,000 perc.mm.; haemoglobin 12.0 g. per 100 ml. Serum albu-min 3.0 g. per 100 ml., globulin 3.2 g. Blood urea55 mg. per 100 ml. Kahn test negative. Electro-cardiography showed the usual changes associatedwith digitalis therapy, and also low, voltage in allleads.
Progress. A litre of clear straw-coloured fluid wasaspirated from the right pleural cavity and 21 litresfrom the abdomen. Mersalyl was injected daily, and0.25 mg. of digoxin given by mouth every six hours:there was no diuresis, his pulse rate dropped to 56per minute within 48 hours and the beats becamecoupled. Treatment with digoxin was stopped, andwithin 24 hours auricular fibrillation developed. Fromthis time his condition deteriorated rapidly. Fourteendays after admission he died suddenly.
Necropsi .-There was generalized dropsy., withlarge pleural and peritoneal transudates. The rightlung was completely collapsed ; the left lung waspartly collapsed, hyperaemic, and oedematous. Along, coiled thrombus was impacted at the bifurcationof the main pulmonary artery. Partly adherentthrombus filled the deep veins of both calves; thethrombus on the left extended up into the externaliliac vein, while that on the right had broken off inthe poplitea. The heart (610 g.) was uniformlyenlarged, with thickening of the myocardium of allparts and dilatation of all chambers. The myocardiumwas firm, and mottled with irregular, pale, opaquepatches. The valves and endocardium were normal.
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED A]VIYLOIDOSIS 213
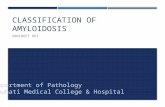
FIG. 1.-Case 1. Perivascular andjuxtavascular amyloidosis, amyloidreplacement of media of arteriole, and(top) amyloidosis of myocardium.Haematoxylin and eosin. x 80.
FIG. 2.-Case l. Large focus ofmyocardialcytolysis. Haematoxylin and eosin.x 150.
FIG. 3.-Case 1. The most heavily in-volved of the very small number ofglomeruli which were found to con-tain amyloid. Haematoxylin andeosin. x 350.
FIo. 1
~.-.-*p _
. ; , .-...
t-S
Z..
r'
d
qr#
-'5
* ... -_*..- _a:
-,~~~~~~~~~~~A
- a 2
.U',,.o -< .-*aaFX.e rr <;;,s . F. z I . .
iv #'s 4N
-o-;' - 'S' ;,.;4.V /; f \~~~~,.
FIG. 2 FIG. 3
I
0 -1 ,
, "A"k Affilh- .I qoll
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
Early fibrinous pericarditis was present. The liver(1,950 g.), spleen (115 g.), and kidneys (200 and 190 g.)showed typical chronic venous congestion only. Therewere no noteworthy changes in other viscera or tissues,including the accessible bones.
Histology.-There was extensive amyloidosis, pre-dominantly affecting the myocardium, but widespreadalso in the walls of blood vessels, particularly smallarteries and arterioles, throughout many organs (Fig.1). Extravascular deposits of amyloid were also foundin the musculature of the tongue, stomach, and smallintestine. and in scanty small clumps beneath the endo-cardium. The amyloid showed little or no affinity forCongo red, but usually gave a metachromatic reactionwith methyl violet. There was no granulomatousreaction around any of the amyloid deposits. Noplasma-cell proliferation was found.
The arteries most heavily affected were those in theheart and liver. There was widespread focal myo-cardial cytolysis (Fig. 2) and patchy interstitial myo-cardial fibrosis. Renal amyloidosis was limited tosmall deposits in occasional glomeruli (Fig. 3) andheavier involvement of interlobular and largeiarteries; apart from amyloidosis there was focal cor-tical atrophy, with basal glomerular hyalinization andinterstitial fibrosis in these areas. In the spleenamyloid was found only in some trabecular vessels:some follicles showed interstitial hyalinization thehyaline tissue resembled amyloid when stained witheosin, but was coloured intensely red by Van Gieson'sfluid. Slight to moderate amyloidosis of blood vesselswas found in the tongue, stomach, intestines, thyroid,adrenals, reproductive organs and skeletal muscle;none was found in the lungs or in adipose tissue. orin the thrombosed veins in the legs.
The main clinical feature of this case was theprogressive development of cardiac failure, charac-teristically showing the lack of response to treat-ment which is a feature of amyloid heart disease.Gunnar, Dillon, Wallyn, and Elisberg (1955) foundthat cardiac catheterization studies confirmed theclinical observation of a similarity between thecardiovascular disturbances of myocardial amy-loidosis and constrictive pericarditis; they attri-buted the resemblance to the lowered elasticity ofthe amyloid myocardium. The later stages ofheart failure in the case described here were asso-ciated with massive accumulations of fluid in theserosal cavities, more suggestive of a nephroticstate than of cardiac dropsy, particularly as therewas persistently heavy proteinuria necropsyshowed that there was in fact only slight renaldamage. The nephrotic syndrome, which may goon to uraemic renal failure, has been observed inprimary amyloidosis (Muehrcke, Pirani, Pollack,and Kark, 1955). Fatal pulmonary embolism isthe only unusual feature of the present case.
Primary amyloidosis itself does not appear to pre-dispose to thrombosis.
Case 2: Primary Amyloidosis Presenting withHeart Failure and Peripheral Neuropathy.--A dairystoreman, aged 47, was admitted to hospital with threemonths' history of rapidly progressive breathlessness,associated with pins-and-needles and numbness in thehands and feet. There was no history of serious ill-health previously.On admission he was orthopnoeic and somewhat
cyanotic. and his legs were oedematous. There wererales at the lung bases. Auricular fibrillation waspresent (heart rate about 90 per minute), and the heartwas considerably enlarged. Blood pressure about110 60 mm. of mercury. The peripheral arteries werenot thickened ; the retinal vessels were normal. Therewas slight loss of pain and touch sensation in thehands and feet, with some wasting of the thenar andhypothenar muscles and weakness of the grip theankle reflexes were absent and there was weakness ofplantar flexion; neurological examination was other-wise normal. The liver was slightly enlarged andtender. No other clinical abnormalities were found.
Inivestigations.-Urine: protein, a trace. Blood:erythrocytes 4,400,000 per c.mm.; haemoglobin 10.8 g.per 100 ml.; leucocytes 8.200 per c.mm. (normaldifferential count). Erythrocyte sedimentation rate 110mm. in one hour (Westergren). Serum albumin 3.5 g.per 100 ml., globulin 7.7 g. Blood urea 40 mg. per100 ml. Kahn test negative. Cerebrospinal fluid:total protein 70 mg. per 100 ml.: excess globulinpresent (Pandy) ; Wassermann reaction negative; noincrease in cells. Electrocardiography showed auri-cular fibrillation; changes indicative of previousmyocardial infarction were present. although there wasno history of symptoms suggesting myocardialischaemia at any time. Radiographs of the skull,chest, spine, and pelvis were normal.
Progress.-His condition did not respond to fulldoses of digitalis and vitamin-B complex. He died inhis sleep 10 days after admission.
Necropsy. The tissues were waterlogged, and therewere small effusions in the body cavities. The heart(640 g.) was enlarged, mainly by thickening of the ven-
tricular walls and dilatation much of the posteriorwall of the left ventricle was replaced by the fibrousscar of an old infarct; there was a large pale recentinfarct in the apical part of the left ventricle. The restof the myocardium was firm, and was irregularlymottled by pale areas. The endocardium, particularlyof the atria and the ventricular aspect of the tricuspidand mitral valve cusps, was studded here and therewith firm, translucent nodules, about 0.2 cm. in dia-meter. The pericardium was normal apart fromadhesions over the old infarct. Organizing thrombusoccluded the anterior interventricular coronary arteryto within about 1 cm. of its origin; fresh thrombusextended proximally from this level and occluded theleft coronary artery at its bifurcation. The distal halfof the posterior interventricular artery was represented
214
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOlDOSIS
by a fibrous cord. The coronary arteries were other-wise normal. The aorta was slightly atheromatous.The lungs showed chronic venous congestion, withconsiderable basal oedema. The liver (2,150 g.),stomach and intestines, spleen (200 g.), kidneys (each240 g.), and adrenals showed typical chronic venouscongestion. The brain, spinal cord, and main peri-pheral nerves were macroscopically normal. Thecranium, spine, thoracic cage, pelvis, scapulae,clavicles, one humerus, and one femur were searchedfor evidence of myeloma: none was found.
Histology.-Apart from chronic venous congestionof the viscera and the myocardial infarcts, the signi-ficant histological findings were those of amyloidosis.The kidneys and bones in particular showed no otherabnormalities; there was no evidence of myeloma orof plasma-cell proliferation. Amyloid was present inmost of the tissues sectioned, and, apart from the sub-endocardial nodules, was virtually confined to thewalls of the blood vessels. It stained metachromatic-ally with methyl violet and showed strong affinity forCongo red. The vascular involvement took twoforms. In one form, the commoner, the entire mediaof arteries and arterioles, and, less often, of veins, invarious organs and tissues was replaced by amyloid,with more or less encroachment upon the lumen;there was no cellular reaction of any sort around theselesions. In the other form irregular clumps of amyl-oid were present in the connective tissue immediatelysurrounding the media of the vessels: macrophagesand foreign-body giant cells were closely applied tomany of these clumps, some of which were stippledwith calcium.
Affected vessels were oftenest seen in the heart andin the adventitia of the aorta. There was less frequentinvolvement of vessels in the submucosa of thestomach and intestines, in bone marrow and aroundthe adrenals, and rare involvement in hepatic portaltracts, pancreas, lungs, kidneys, spleen, lymph nodes,and thyroid. No amyloid was found in the repro-ductive organs, skeletal muscle, tongue, or skin, or inthe meninges, brain, cranial nerves, or spinal cord.The spinal nerves were involved sparsely, but sectionsat different levels between their roots and peripheraldistribution clearly indicated the likelihood of a cumu-lative injury through the effects of a series of amyloidvascular lesions scattered along their length.The occluded stretches of the coronary arteries
were particularly heavily affected by amyloidosis, butthe amyloid was mainly in the adventitia, with onlyscattered deposits in the media and intima. Therecent thrombosis had occurred on typical athero-matous plaques.
Heart failure in this case could be explainedwholly on the basis of myocardial ischaemiacaused by coronary atheroma and thrombosis,although it is likely that the widespread vascularamyloidosis played some part. It is noteworthythat atheroma was confined to the sites of actualocclusion, and that amyloidosis was particularly
severe in these parts. The absence of anginal painor of any clinical evidence of an acute infarctiveepisode is remarkable.There is no reason to doubt that amyloidosis
of the vasculature of the spinal nerves accountedfor the neurological manifestations. Amyloidneuropathy has been reviewed by Ritama and afBjorkesten (1954); Mathews (1954) cited addi-tional cases.The uncommonly high serum globulin level is
interesting in relation to the possible pathogeneticsignificance of hyperglobulinaemia in amyloidosis:its cause is obscure.Case 3: Primary Amyloidosis Presenting with
Goitre and Congestive Heart Failure.--A man, aged35, was admitted to hospital complaining of enlarge-ment of the neck and breathlessness. His health hadbeen good until a year earlier, when he noticed thathis collars were becoming tight. Three months laterhe went on an annual walking holiday and found hiscapacity for this exercise greatly lessened by short-ness of breath. His neck continued to enlarge,breathlessness became slowly severer, and his feetbegan to swell in the evenings. There were no othersymptoms.On admission, examination showed a large, smooth,
firm, symmetrical goitre; there was no evidence ofhyperthyroidism or hypothyroidsm. His legs wereoedematous and there were rales at the base of eachlung. The veins of the neck were engorged, the heartwas slightly enlarged and there was an apical systolicmurmur. The pulse was regular (90 per minute).Blood pressure 135/65 mm. of mercury. The edge ofthe liver was palpable just below the costal margin.The spleen reached halfway from the costal marginto the umbilicus. His tongue was uncommonly large,although otherwise normal in appearance; its mobilitywas decreased.
In view of the macroglossia, and heart failure with-out obvious cause, the diagnosis of amyloidosis wasmade. The patient collapsed and died suddenly onthe day after admission. The only investigationswhich had been completed were: Urine: protein +.Blood: erythrocytes 5,500,000 per c.mm.; haemo-globin 15.1 g. per 100 ml.; leucocytes 6,800 per c.mm.Serum albumin 3.3 g. per 100 ml., globulin 3.8 g.Erythrocyte sedimentation rate 58 mm. in one hour(Westergren). Wassermann and Kahn tests negative.Necropsy.-The pericardial sac was distended with
fresh blood clot (about 400 ml.). The heart (500 g.)was enlarged; there was an irregular rent, about 2 cm.long, in the wall of the left ventricle adjacent to theseptum. The myocardium was extensively replaced byamyloid: the rupture had occurred between a largeamyloid plaque in the anterior wall of the ventricleand an area of apparently healthy muscle. Minuteamyloid nodules were scattered in the endocardium ofall chambers: the valves were normal and the pericardium was free from obvious amyloid. The thyroid(250 g.) was symmetrically enlarged, smooth, and waxy-
215
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
At
*8 r~~A
'S.>;/... .,,
/ ~~~~~~~ 4
-a !.
v9
* r t;t7 Mi
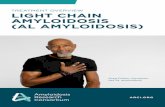
FIG. 4.-Case 3. Large amyloid deposits separating and compr
looking. The tongue was also heavily infiltrated withamyloid. The lungs, liver (1,800 g.), stomach, intes-tines, kidneys (combined weight, 370 g.), and adrenalsshowed chronic venous congestion; a fibroma, 0.6 cm.in diameter, was present in a pyramid in one kidney.The spleen (700 g.) was practically completely replacedby amyloid. Lymph nodes in various situations weremoderately enlarged.
Histology.- Widespreadamyloidosis of blood ves-sels was found in all or-gans. Confluent interstitialamyloid was abundant in , 7the myocardium, tongue \(Fig. 4), thyroid, spleen,lymph nodes, and haemo-poietic marrow. Pericellu-lar amyloid was seen inadipose tissue from varioussites and in the muscula-ture of the gastrointestinal P'.7--and urinary tracts, seminalivesicles, and prostate, aswell as in the less heavilyaffected parts of the myo- 4cardium (Fig. 5) andtongue. In the myo-cardium there were ap- * Jpearances suggesting amy-loid transformation of ,ermuscle cells as well as the 74<pericellular and interstitial iG 5.-Case 3. Pericelluldeposition. The liver and Congo red and ha4
0.-
*.:.
larLem
F $ ',.
>47
-Er'
A
I
I
ftI.v*...."I
Ares ucl ire f oge.Mthlvolt x15
reasing muscle fibres of tongue. Methyl violet. x 155.
kidneys were free from amyloid, apart from involve-ment of the walls of some arteries and arterioles, andextensive interstitial deposits in the renal fibroma. Thelungs contained nodular masses of amyloid alongsideheavily affected vessels; amyloid was also present insome alveolar septa, and there was considerableinvolvement of the bronchi, where amyloid in placesmerged into the cartilage and elsewhere formed
nodules which jutted intoC-} t the airway.
& 4 iq ''' The amyloid had littleor no affinity for Congo
t-K#F *+! ~red, but for the most partstained metachromatically
r-* tJPwith methyl violet. Agiant-cell reaction was pre-
w. 8' * x sent around the amyloid in.1t*Xf-* e ithe spleen and some lymph
nodes, but not elsewhere.I * ." $Rupture of the myo-
Si) gIS lwfcardium has not been>IiJ 4a j;"a recorded previously inb; ,>, ;t ;> any case of amyloidosis.
-. % ##t-;tSpontaneous rupture ofwsA the spleen has been re-
-4 Sw ^ 4 ft ported on three occasions(King and Oppenheimer,1948; Wiley, Teeter, and
'N KSchnabel, 1951; Dra-~- -. > Wpiewski, Sternlieb, and
amyloidosis of myocardium Jiatoxylin. x 375. Jones, 1955), and patho-
216
.i
A.;
tAA....p 1.
4e
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
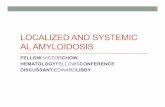
i''sFIG. 6.-Case 4. Pericellular amyloidosis and irregular masses of amyloid in myocardium. Haematoxylin and eosin. x 125.
logical fracture associated with osseous amyloidosishas been described (Koletsky and Stecher, 1939).Amyloid goitre is quite well known (Walker, 1942),usually occurring in association with chronicbronchopulmonary sepsis; the thyroid is com-
monly affected in primary amyloidosis, but thedegree of involvement is rarely sufficient to beapparent macroscopically, and frank goitrousenlargement must be very rare.
Case 4: Primary Amyloidosis with Obscure Symp-toms and Haemorrnagic Manifestations.-A scaffolder,aged 44, complained of headaches and depression: noabnormality was found. The Wassermann and Kahntests were negative. Six months later he was seenagain, complaining of hoarseness of three months'duration and of pain in the right side of the chest,aggravated by exertion and of three weeks' duration.He had some upper abdominal pain and complainedof breathlessness. Chest radiography, an opaquemeal, and electrocardiography showed no abnormality. After a further six months he was admittedto hospital complaining of persistence of the pain inthe abdomen and chest, hoarseness, and loss ofappetite. He had had melaena for two months andhad coughed up a little blood-stained sputum.On admission he was pale and had clearly lost much
weight. The edge of the liver was about 5 cm. belowthe costal margin. Haemoglobin 32%. Leucocytes20,000 per c.mm. (polymorphonuclear leucocytosis).Opaque meal normal. Chest radiograph: enlargement
of heart; opacity of base of right lung. He was given2 pints (1,100 ml.) of blood soon after admission.Three days after admission his leucocyte count was10,000 per c.mm., platelet count 145,000 per c.mm.,and bleeding time normal. His condition deterioratedquickly, crepitations developed at the base of thelungs, and he died five days after admission.Necropsy.-There were a few petechiae on the side
of the neck and on the palate. The heart (470 g.)showed hypertrophy of both ventricles; the myo-cardium was pale. The endocardium of the atria andof the atrioventricular valves was rough; in appear-ance and feel it resembled the pericardium in fibrinouspericarditis. Thrombus was present in several smallpulmonary arteries and there were a few small infarctsin the lungs. The lower lobe of the right lung wasconsolidated. Multiple submucosal haemorrhageswere found in the small intestine. The liver and spleenwere enlarged and congested. Nothing else of notewas found.
Histology.-There was extensive and severe amy-loidosis of the walls of arteries, arterioles, and veinsin the myocardium and small intestine, and lessinvolvement in the lungs, liver, and elsewhere. Peri-cellular amyloidosis was present in the heart (Fig. 6)and parallel striae of amyloid traversed practically theentire thickness of the atnial wall. There were exten-sive subendocardial and subepicardial deposits. In theintestine parts of the muscularis mucosae were whollyreplaced by amyloid; large fresh haemorrhages hadoccurred around heavily involved submucosal vessels.
217
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
Amyloid was present in some interalveolar septa in thelungs, but pulmonary involvement was predominantlyseen in arteries, and affected both bronchial and pul-monary vessels; lobar pneumonia was present in theright lower lobe, and therc were haemorrhagicinfarcts elsewhere, the cause of which was notapparent in the sections. The liver, kidneys, andspleen were congested; amyloid was scanty, and con-fined to arteriole walls.
This case illustrates the vague symptoms whichmay for long be the only manifestations ofprimary amyloidosis. The eventual occurrence ofhaemorrhagic manifestations is not uncommon inprimary amyloidosis, and was observed also in thefollowing case.Case 5: Primary Amyloidosis with Predominant
Haemorrhagic and Pulmonary Manifestations.-Aman, aged 47, was admitted to hospital with a historyof coryza and productive cough 18 days earlier, fol-lowed by feverishness and gradually worsening painin the left sidc of the chest. The sputum was blood-stained, and there was bleeding from the nose. On theday of admission he vomited a little blood.For as long as he could remember he had been sub-
ject to a local purpuric eruption whenever his skin wasfirmly stroked or pinched. During the years beforeadmission his exercise tolerance had been restricted bybreathlessness. He had been told that a chest radio-graph taken three years after the dyspnoea beganshowed " healed miliarv tuberculosis." and furtherradiographs during the following years were said tohave shown no change. He was known to have acardiac murmur: this had been described as a non-organic pulmonary systolic murmur.On admission his temperature was 99.4' F. (37.4c
C.). There was widespread purpura, particularly onthe trunk. Scratching the skin was promptly followedby a crop of purpuric spots along the scratch line. Afew haemorrhagic herpetic vesicles were present onthe upper lip and there were petechiae in the oralmucosa. The heart was enlarged (apex beat in sixthinterspace just outside the mid-clavicular line). Aharsh systolic murmur was audible over the wholeprecordium, and loudest in the fourth left interspacebeside the sternum. Pulse regular (100 per minute).Blood pressure 130 o70 mm. of mercury. There werescattered rales in the lungs. The edge of the liver waspalpable 2.5 cm. below the costal margin, and thespleen could just be felt.
Investigations.-Chest radiograph: uniform, closestippling of lungs with " hard " miliary shadows.Electrocardiography : left ventricular preponderance.Blood erythrocytes 3,750,000 per c.mm.; hacmo-globin 64 '', ; leucocytes 18,700 per c.mm. (neutro-phils 15,300, eosinophils 100, lymphocytes 1,400,monocytes 1,800, Turk cells 100); platelets 363.000per c.mm.; 'target cells " present. Urine: protein +hyaline casts and occasional leucocytes and erythro-cytes.
Progress.-Eight hours after admission the patienthad severe melaena, followed by haematemesis. Inspite of immediate blood transfusion he quickly died.
Necropsvy.-The stomach contained about 600 ml.of freshly clotted blood, and there was a large amountof fresh blood in the lumen of the small intestine.The gastric and intestinal mucosa was severely auto-lysed and stained by blood and bile : no ulceration andno indisputable purpura or other source of haemor-rhage was visible to the naked eye. The peritoneumwas normal; there was no ascites. The liver (1,800g.), pancreas (400 g.), and spleen (250 g.), a splenun-culus (20 g.), and the kidneys (combined weight 450 g.)and adrenals (combined weight 45 g.) showedthe typical appearances of severe diffuse amyl-oidosis. The iodine test gave no clear result, but onapplying sulphuric acid some of the amyloid devel-oped a muddy bluish-olive colour. The tongue wasmoderately enlarged ; there were deep, clean foldsbetween amyloid deposits in the mucosa of its posteriorthird, and its musculature was widely affected byamyloidosis. The mouth otherwise, and the salivaryglands, pharynx, and oesophagus were normal. Thenose, nasal sinuses, larynx, trachea and bronchi.and thyroid were normal. Small effusions werepresent in the pleural cavities, which were partlyobliterated by old fibrous adhesions; adhesions boundthe pleurae to the pericardium. The lungs were ofnormal size, but hyperaemic; they were studdedthroughout with firm, black nodules, uniformly about0.35 cm. in diameter, and most numerous in the hilarand central parts of each lobe. The pulmonaryvessels were normal. The heart (500 g.) was hyper-trophied, particularly the left ventricle ; the myo-cardium looked otherwise healthy and no amyloid wasevident ; there was no septal defect. The valves,endocardium, and coronary vessels were normal; thepericardial sac contained a small excess of fluid butotherwise was normal. There was slight aorticatheroma. The urinary tract, prostate, seminalvesicles, and testicles were normal. The brain wasnormal. The skull, spine, thoracic cage, and pelvicbones, and the accessible skeletal muscles were normal.The tissues in general were dry ; there was no oedema.There was widespread purpura of the skin, withecchymoses in some areas, particularly around theeyes and in the neck.The lymph nodes throughout the body were grossly
abnormal. The mesenteric nodes were enlarged, thebiggest measuring 5 by 3 by 1.5 cm.; their cut surfacewas finely spongy, showing yellow or orange, opaque.soft material separated by fine, interlaced trabeculae.Similar appearances were seen in the juxta-aortic andiliac lymph nodes and in those of the mediastinum andneck ; the superior vena cava was compressed bygroups of greatly enlarged nodes. Extensive freshhaemorrhage was present in many of these mediastinalnodes. in some instances virtually destroying them.
Histology.-The distribution and appearance of theamyloid deposits in the most heavily involved organs,
218
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
W.~~~~~~~~~~.--49.'v -1 '~~~~~~~~~ '*. '
..~~~~~~~~~;~n
;".tiix46
FIG. 7.-Case 5. Amyloidosis in alveolar septa of lang, at margin of a calcified amyloid nodule. Haematoxylinand eosin. x 125.
which included the lymph nodes, were typical of thatseen in classical cases of severe secondary amyloidosisand require no further description. The amyloid hadstrong affinity for Congo red, and for the most partgave a clearly metachromatic reaction with methylviolet. It gave a positive but not very intense periodic-acid-Schiff reaction. In frozen sections abundantSudanophil lipid was present in the amyloid in thespleen and to a less extent in the liver and a mesentericlymph node, but not in other situations: only inter-stitial and pericapillary amyloid contained fat, that inthe walls of larger blood vessels being free of demon-strable fat. In most tissues sectioned there was heavyamyloidosis of the walls of blood vessels, particularlysmall arteries and arterioles.
Sections of the stomach and small intestine showedwidespread and severe amyloidosis in the mucosa andin submucosal blood vessels, with scanty pericellularamyloid in the muscle coats. In spite of severe auto-lysis it was clear that there was extensive recenthaemorrhage in the mucosa, particularly in the imme-diate vicinity of arterioles showing heavy amyloidinvolvement. The source of bleeding in the haemor-rhagic lymph nodes could not be determined, so severe
y
was the destruction caused; there was well-advancedorganization of the haematomas in some nodes.The tongue was heavily affected, with amyloid
deposits separating and destroying the muscle cells.No other skeletal musculature was found to beinvolved. Amyloid in the heart was confined to vesselwalls; the myocardium was hypertrophic: occasionalsmall foci of advanced cytolysis were present. Thenodules noted in the lungs macroscopically were areasof heavy amyloidosis of interalveolar septa (Fig. 7),with carbon pigmentation and focal calcification; inaddition there was patchy amyloidosis of the largerblood vessels and in the walls of bronchi and somebronchioles, occasionally with small local haemor-rhages.The parenchyma of the brain and the vessels in it
were free from amyloid, although some meningealvessels and the choroid plexuses were heavily affected.The blood vessels of the skin showed severe amyloid-osis, particularly the arterioles, and there were freshhaemorrhages around some vessels. Interstitial amyl-oidosis was present sparsely in the superficial zone ofthe dermis. Subcutaneous fat, and adipose tissue else-where in the body, was almost free from amyloidosis,
219.
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
although in some sections pericellular amyloid ringswere found.
This case illustrates well that amyloidosis mayoccur without a recognizable predisposing causeand yet present the gross distribution of amyloidwhich is usually associated with secondaryamyloidosis. The presence of macroglossia hascommonly been stressed in the literature as avaluable diagnostic feature of primary amyloid-osis: its presence should indeed draw attentionto the possibility of amyloidosis, but one mustremember that it is absent oftener than present inprimary amyloidosis, and that it occurs, althoughrarely, in secondary amyloidosis.The haemorrhagic manifestations are a puzzling
feature of this case. The sudden onset and rapidlyfatal outcome of the final gastro-intestinal haemor-rhage suggested that the bleeding would prove tohave come from a major, localized source: buta very thorough search failed to show any suchsource, and histological examination showed wide-spread gastrointestinal purpura in relation tosevere amyloidosis of many small vessels. Whilea major lesion may indeed have been overlooked,the available evidence suggests that the fatalhaemorrhage was purpuric in nature: if this iscorrect it remains to be explained how suchsudden widespread haemorrhage could occur moreor less synchronously from so many vesselsaffected by this essentially chronic alteration oftheir substance. Moreover, it is difficult to under-stand why the haemorrhage should be so muchseverer and more widespread in the alimentarytract than in other tissues with vascular amyloid-osis of comparable degree, e.g., the bronchi. Theextensive recent and fresh haemorrhages in someof the amyloid lymph nodes is a further remark-able and unexplained feature of this case. Finally.how is one to relate the terminal haemorrhagicstate and its underlying vascular amyloidosis tothe apparently very long history of purpura asso-ciated with trivial pressure on or stretching of theskin ? The clinical history and the radiologicaland post-mortem findings together suggest thatpulmonary amyloidosis had been present for atleast 10 years, seemingly without detectable altera-tion in its extent if this is the true interpretationof the observations, does it imply that amyloidosishad been present for considerably longer, andeven for as long as the haemorrhagic tendency ?Unfortunately, the onset of the latter cannot bedated from the available records. Most cases ofgeneralized amyloidosis run their course withinone to three years of the first symptom : on'y afew cases have been reported in which the course
was considerably longer, and the longest survivalon record is 14 years (Koletsky and Stecher, 1939).
Eisen (1946) and Mathews (1954) cited a smallnumber of recorded cases of primary amyloidosiswith severe gastrointestinal haemorrhage; suchhaemorrhage has usually been traced to erosive orfrankly ulcerative lesions, which were not ob-served in the present cases (Cases 4 and 5) butmight have been obscured by the severe autolysisin Case 5. Propp, Scharfman, Beebe, and Wright(1954) have discussed the association betweenprimary amyloidosis and athrombocytopenic pur-pura, which they considered to be vascular inorigin.
Amyloidosis Associated with Disturbance ofEndocrine Balance
Case 6: Amyloidosis Associated with ExophthalmicOphthalmoplegia and Pretibial Myxoedema afterThyroidectomy for Hyperthyroidism. A woman, aged67. was admitted to hospital with myxoederna. Four-teen years earlier, after an attack of pneumonia, shebegan to lose weight. became breathless on exertion,nervous. and easily tired, and developed progressivebilateral staring exophthalmos. The menopause hadbeen a year before the onset of these symptoms. Herfamily doctor gave her a course of thyroid extract,which greatly aggravated her condition. Eventually.four years after the onset of thyrotoxic symptoms. sub-total thyroideztomy was performed. Shortly after thisshe was told by her doctor that the surgeon hadremoved too much of the thyroid; he prescribednothing. After the operation her right eye becamenormal, and it remained so : progressive protrusion ofthe left eye led within a few months to severe exoph-thalmos, with paralysis of the external ocular muscles.At about the same time she began to have severe painin the hips. lumbar region. knees, and wrists thiscontinued to trouble her considerably throughout therest of her life. Her energy and strength failed : thehair of her scalp and eyebrows became thin. Twomonths before admission to hospital she developeddiarrhoea, and this persisted, with several fluid motionsdaily. Dried thyroid extract was given soon after thediarrhoea began : she had not had thyroid since thethyroidectomy; only half a grain (0.03 g.) daily wasprescribed, and this had no apparent effect. She wastherefore referred to hospital. where she was admittedimmediately.On admission she presented the typical picture of
severe myxoedema, together with left-sided exoph-thalmic ophthalmoplegia and severe pretibial myx-oedema. In addition there was a palpable tumour inthe left hypochondrium, and severe osteoarthritis ofthe hips and knees. There was no evidence of heartfailure. Blood pressure 140 90 mm. of mercury. Theliver and spleen were not palpable.
Investigations. Urine: protein +. Blood: ersthro-cytes 3,110,000 per c.mm.: haemoglobin 9.4 g. per 100
220
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
ml.; leucocytes 7,100 per c.mm. (myelocytes 35, meta-myelocytes 180, neutrophils 4,685, eosinophils 35,lymphocytes 1,280, monocytes 815, plasma cells 35,Turk cells 35). Erythrocyte sedimentation rate 70mm. in one hour (Westergren). Blood urea 43 mg. per100 ml. Basal metabolic rate minus 35 %.Progress.-Thyroid extract was given by mouth,
half a grain (0.03 g.) three times a day. Five daysafter admission the patient collapsed suddenly; sheremained semiconscious from then until her deaththree days later. During this time there was gross anduncontrollable disturbance of serum electrolytes.The serum potassium concentration ranged between
21.4 mg. and 13 mg. per 100 ml., the lowest figurebeing found on the day of death, in spite of parenteraland oral administration of potassium salts.Necropsy.-The pretibial tissues had the classical
appearances of myxoedema. Similar myxoedematousmaterial filled the left orbit, pushing the bulb forward.The thyroid was represented by three rounded nodulesof fibrotic tissue, each about 0.5 cm. in diameter. Theheart (530 g.) was enlarged by hypertrophy and dila-tation of the ventricles. The hypertrophic myocar-dium looked healthy and the valves, endocardium, andpericardium were normal. The coronary vessels werenormal. There was atheromatous ulceration of theabdominal aorta. The main bronchi of the lower lobeof each lung showed fusiform dilatation, with somechronic suppuration and peribronchial fibrosis. Therest of the lungs, the pleurae, and the upper respira-tory tract were normal. The mouth, salivary glands,and tonsils were normal; the tongue was not enlarged.The oesophagus, stomach, intestines, liver (1,450 g.),biliary tract, pancreas, and spleen (110 g.) appearedhealthy. There was no lymphadenopathy. Theadrenals (combined weight 10.5 g.) were small andpale.
Both kidneys (right, 165 g.; left, 385 g.) showednarrowing of the cortex and fine granularity of theirouter surface. A typical, infiltrating Grawitz tumour(8 by 7 by 6 cm.) occupied the middle third of the leftkidney; no metastases were found anywhere in thebody. The urinary tract and reproductive organs werenormal. The brain and the accessible parts of theskeleton were normal; the hip joints and knees werenot opened, but there was external evidence of osteo-arthritis.Histology.-Patchy or severe amyloidosis affected
small arteries, arterioles, and venules, and occasionallycapillaries, in all the tissues sectioned, except the brain,which was histologically normal. The spinal cord wasnot examined. The degree of vascular involvementdiffered from organ to organ: it was particularly wide-spread and severe in the myocardium and gastro-intestinal tract and around the adrenals, and wasscanty in the liver, kidneys, and spleen. The par-enchyma of the solid organs was not affected. Peri-cellular amyloid was most abundant in the adiposetissues, but was present also in many small areas ofmyocardium and in the muscularis mucosae of the
stomach and intestines and, to a less extent, in theirmain muscle coats. Amyloid deposits were present inthe interstices of the connective tissue of the gastro-intestinal mucosa and of the tongue between its surfaceepithelium and its musculature. Skeletal muscle,including that of the tongue, was scarcely involved,and virtually no amyloid was found in skin or bonemarrow. The haemopoietic marrow showed erythroidand myeloid hyperplasia; there was no evidence ofleukaemia. The pretibial myxoedema was histo-logically typical: similar myxoedematous infiltrate waspresent in the left orbital tissues. There was no cel-lular infiltration of any sort in the orbital tissues,including the ocular muscles. No myxoedematousinfiltrate was found elsewhere. Minimal mucoiddegeneration of myocardial fibres was seen.The thyroid remnants were fibrotic; the surviving
acini were lined by tall epithelium, often with muchpapillary ingrowth, and only a little, poorly stainedcolloid was present. The pituitary showed a frankreduction in the proportion of acidophil and baso-phil cells. Many chromophobe cells were uncom-monly large; their cytoplasm sometimes containedone or two large vacuoles; in places they formedrosette-like groups, and in these they assumed acolumnar or wedge shape. Calcified, concentricallylaminated spherules were scattered through theanterior lobe. There were areas of hyaline thickeningof the connective-tissue framework of the gland;amyloid was found only in arteriole walls, and wassparse there. The adrenal cortex was narrow andthe zona glomerulosa was ill-defined or lacking;amyloid was confined to the walls of arterioles and ofthe central veins. The histological findings in thepituitary and adrenals corresponded very closely tothose described by Brewer (1951) in his case of un-complicated myxoedema.
Histochemical Findings.-The pretibial and orbitalmyxoedema infiltrate gave a positive reaction withperiodic-acid-Schiff, stained metachromatically withtoluidine blue and was mucicarminophil. It wasstrongly acid, taking up methylene blue at pH 3. Insections which had been incubated with hyaluronidasethere was no appreciable difference in the reactionwith periodic-acid-Schiff but metachromasia withtoluidine blue was considerably less apparent; in-cubation with diastase had no effect. These resultscorrespond to those found by Brewer (1951) on investi-gating the mucoid infiltration in the tongue in hiscase of myxoedema, and they were obtained by themethods which he described: they suggest that themyxoedema infiltrate may be a mixture of hyaluronicacid and a strongly acid polysaccharide, possibly ofthe nature of chondroitin sulphuric acid.The amyloid deposits in this case had considerable
affinity for Congo red and stained metachromaticallywith rosanilin dyes. It was noticed that in parts ofthe heart small clumps of interstitial amyloid gave astrong positive reaction with periodic-acid-Schiff,appeared to stain metachromatically with toluidineblue and were mucicarminophil, while most of the
221
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
amyloid elsewhere gave only a weak reaction withperiodic-acid-Schiff and did not stain with muci-carmine or metachromatically with toluidine blue. Inthe strongly reacting areas there was abundant, butnot pathologically excessive, connective-tissue groundsubstance, which stained metachromatically withtoluidine blue and was mucicarminophil and unusuallyacid, taking up methylene blue at pH3. Incubationwith hyaluronidase greatly diminished the toluidine-blue metachromasia, the mucicarminophilia and thereaction with periodic-acid-Schiff, in both the groundsubstance and the amyloid. Neither hyaluronidasenor diastase had any effect on the staining of theamyloid with rosanilin dyes or with Congo red. Theseobservations suggest that the anomalous staining ofthe amyloid was due to its being bathed in the appar-
ently somewhat abnormal connective-tissue mucoid:they do not, of course, prove any derivation of theone substance from the other.
Of the four conditions which were associatedwith amyloidosis in this case-osteo-arthritis, renalcarcinoma, bronchiectasis, and the post-thyroid-ectomy state-it seems reasonable to exclude thefirst two from consideration as possible predis-posing causes. Amyloidosis has not been observedto occur with unusual frequency in cases of osteo-arthritis, in contrast to the known predispositionto amyloidosis in cases of rheumatoid arthritis(Reece and Reynolds, 1954). The presence of therenal carcinoma may be considered incidental.Amyloidosis may occur as a complication ofcancers, but ordinarily this association is only seen
with slowly progressive growths with ulcerationand chronic infection (Dahlin, 1949); there is no
known predisposition to amyloidosis in cases ofother neoplasms, with the exception of myeloma-tosis, which is in a special category in this respectas amyloidosis occurs in 10% or more cases
(Snapper, Turner, and Moscovitz, 1953). Althoughplasma cells were found in the peripheral bloodin this case, and there was a sparse accumulationof plasma cells in the haemopoietic marrow and
in the bronchiectatic lesions, nothing suggestingmyeloma was found anywhere.
Bronchiectasis is one of the recognized predis-posing causes of amyloidosis. The resultingamyloidosis usually has the distribution of classi-cal secondary amyloidosis; occasionally, however,the distribution is that which is more character-istically seen in amyloidosis without a recognizedcause. Bronchiectasis certainly cannot be excludedas a cause, and possibly the sole predisposingcause, of amyloidosis in this case.
In addition, this patient was at an age whenprimary senile amyloidosis begins to appear.Husselmann (1955) found that about 15% of menand 10% of women over 70 have amyloidosis:
this senile amyloidosis is similar in Its manifesta-tions to primary amyloidosis of younger people,particularly in its predilection for the cardiovascu-lar tissues, and it has a special tendency to affectthe heart predominantly.The relation between the post-thyroidectomy
state in this case, with its disturbance of pituitary-thyroid function, and the amyloidosis is debatable.It is possible that hypothyroidism enhanced amy-loid formation. There seems to be little doubt fromthe patient's history that she had previously hadhyperthyroidism. Attempts to get informationabout her condition from the hospital where thethyroidectomy was performed were unsuccessful,and requests for access to sections of the surgicalspecimen were refused, so that it has been im-possible to discover whether there was histologicalevidence of amyloidosis at that time. This is par-ticularly unfortunate in view of the possibilitythat there might have been evidence of amyloidosisantedating the hypothyroidism. The associationof amyloidosis and hypothyroidism was observedalso in the case described next in this paper, butappears to have been described only once beforein the literature (Case Records of the Massa-chusetts General Hospital, 1956). As in the presentcase, the Massachusetts General Hospital patientwas a woman who had what was in effect a totalthyroidectomy for hyperthyroidism. Six yearslater, when aged 30, she was found to haveamyloidosis: necropsy showed involvement oflymph nodes, salivary glands, skeletal muscle,intestines, and lungs, and no cause for amyloidosiswas found. Exophthalmos was never present andmyxoedematous deposits were not noted in theMassachusetts case ; the patient had receivedsome maintenance treatment with thyroid.There is experimental evidence that hormones
can influence amyloid formation. Perasalo andLatvalahti (1954) found that corticotrophin and,to a less extent, cortisone enhanced amyloid pro-duction in mice receiving caseinate injections;castration had a similar effect, while testosteronewas without obvious influence; thyroidectomyalso encouraged the development of amyloidosis,while thyroid extract appeared to have some in-hibitory effect upon it. Uotila, Perasalo, andVapaavuori (1955) found that growth hormonehad no effect on the development of experimentalamyloidosis, whereas thyrotrophin accelerated it.Confirmation of these findings would be a con-
siderable advance in knowledge of the factors con-
cerned in amyloid formation, particularly in rela-tion to cases such as this one and the next. Mean-time, it is interesting to speculate about the
222
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
possible role of thyrotrophin, diverted from itsproper sphere of activity by the absence of thyroidtissue, in the development of exophthalmos, pre-tibial myxoedema, and amyloidosis in this case.Amyloid is an atypical and predominantly pro-
tein substance probably containing a small pro-portion of polysaccharide, which is usually saidto be chondroitin sulphuric acid. Chondroitinsulphuric acids, hyaluronic acids, and protein areconstituents of the mucoid material of myxoedemainfiltrates (Brewer, 1951 ; Bruns, 1955). Thepossibility of a relationship between amyloid andmyxoedema mucoid might repay study. It isinteresting to observe the similar distributionof the amyloid deposits in some cases andof myxoedema infiltrates. This is reflected,for instance, in the diagnostically important ob-servation that the two commonest causes ofmacroglossia are amyloidosis and myxoedema.Brewer (1951) showed that the " basophilic de-generation" of the myocardial cells, which is par-ticularly frequent and extensive in myxoedema, isdue to deposition of a mucoprotein distinctfrom that of the interstitial myxoedema infiltrates.The presence of this myocardial mucoiddegeneration and of the chemically distinctmyxoedema infiltrate in other tissues indicates theoccurrence in hypothroidism of two pathologicalalterations in the utilization of polysaccharides:a third alteration, resulting in the formation ofamyloid, might be mediated similarly, or amyloidmight even result by transformation of myxoedemainfiltrate.As only the Massachusetts General Hospital
case and the two cases in this paper have beenrecorded, so far, it must be very rare for clinicalevidence of endocrine dysfunction to be a featureof the antecedent history of cases of amyloidosis.It is clear that neither hypothyroidism nor anyother endocrine disorder can be held responsible,on the evidence available, for any considerableproportion of cases of amyloidosis in which noobvious predisposing cause is found. The mostthat can be said is that these three cases illustratea state of affairs which resembles that observedexperimentally by the Finnish workers, and thatthey are an encouragement to further investigationalong these lines. Further research, however,should be directed as much to investigatingchanges in polysaccharide and protein metabolismand the role of hyperglobulinaemia, plasma-cellproliferation and immunological disturbances asto the study of hormonal influences. The problemof amyloidosis is clearly a complex one, in whichmany factors are concerned.
Haemmerli (1954), on the basis of clinical andpost-mortem observations, suggested that hypo-thyroidism due to amyloid deposition in thethyroid might contribute to the picture of primaryamyloidosis, and he advised considering the useof thyroid extract in treatment. While there is infact only rarely any considerable degree of thyroidamyloidosis in these cases, Haemmerli's suggestionwould seem to be worth following up, in view ofthe experimental findings already referred to andof the clinical observations in the next case. Carewould obviously be necessary in giving thyroidextract to patients with serious cardiac disability,and the need for thorough investigation beforeand during treatment is self-evident.To summarize the case described above, it can
be said that the development of amyloidosis mayhave been determined primarily by chronic sup-purative bronchiectasis, by the patient's age (senileamyloidosis), or by the pituitary-thyroid disturb-ance, or by the combination of any of these. Thedistribution of the amyloid deposits, with pre-dominant involvement of tissues which are charac-teristically involved in cases of amyloidosis with-out recognized cause (" primary amyloidosis "), isof no differential significance, for the same dis-tribution is found in a proportion of cases ofamyloidosis occurring as a complication of theclassical predisposing causes (see Cases 11 and 12,below).Case 7: Amyloidosis Associated with Myxoedema
after Treatment of Hyperthyroidism with RadioactiveIodine.-A man, aged 27, developed severe hyper-thyroidism, with a large goitre and exophthalmos. Herefused surgical treatment and failed to co-operate intreatment with thiouracil. He was advised to havetreatment with radioactive iodine and this was carriedout. Inadvertently, he received three times the calcu-lated dose. No lymphadenopathy, hepatospleno-megaly, or macroglossia was present at that time. Hewas next seen two years later, when he presented thepicture of severe hypothyroidism. His basal metabolicrate was minus 32%. In addition, the liver and spleenwere hard, and palpable 2 cm. below the costal margin;he had generalized enlargement of superficial lymphnodes, and macroglossia of such degree that he couldnot close his jaws.
Investigations.-Slight proteinuria. Serum albumin2.8 g. per 100 ml.; globulin 2.2 g. Erythrocytes4,100,000 per c.mm.; haemoglobin 10.2 g. per 100 ml.Chest radiograph: slight increase of transverse dimen-sion of heart; otherwise normal. Electrocardio-graphy: low voltage in all leads.Biopsy of an axillary lymph node (Fig. 8) and of
the tongue showed widespread amyloid deposits. Theamyloid stained metachromatically with methyl violetand had considerable affinity for Congo red.
223
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
Al.~ ~ ~
'i. A;P,I~~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~~~~~~C
-V~~~~~~~
J,
FI 8.-Case 7. Amyloidcsis of a lymph node. Haematoxylin and eosin. 15.
Progress.-The patient was treated with thyroid about 1.5 cmextract by mouth, and a maintenance dose of 4 grains defined at its(10.26 g.) daily kept his basal metabolic rate within areola. Theanormal limits. During the following six months the their skin apgeneral mental and physical stigmata of myxoedema movably toregressed satisfactorily. The tongue decreased in size resilient tissuuntil it was not obviously larger than normal. The which coinciliver and spleen ceased to be palpable. and the super- reddened ZOrficial lymph nodes became smaller although they re- deep underImained palpable and firm. The size of the heart about 5 mm.On radiography and the electrocardiograph returned to on compressinormal. When last seen, 12 months after starting the rubber s,
treatment with thyroid extract, he felt very well. The to its previourine still contained a trace of protein ; the serum were normalalbumin concentration was 3.8 g. per 100 ml. and perineum wa,
globulin 2.3 g. The lymph nodes continued to) than the are(decrease in size. oped, but nc
No cause for amyloidosis was found in this tained ase.vercase, unless it was a result of the gross destruction Ithe lacrosmof the thyroid by radio-active iodine. The de- amelanotic, r
velopment of amvyloidcosis and myxoedemapaoridainately over
passu is itself suggestive of a rela-tion between the two, and a rela-tionship is supported by the regres-sion of the amyloidosis when thehypothyroidism was brought undercontrol by substitution therapy. Itis obviously impossible to determinehow far the manifestations observedduring the phase of uncorrectedinyxoedema were due to hypo-thyroidism per se and how far toamyloidosis; equally, it is impos-sible to determine how far the dis-appearance of these manifestationswas the result simply of recoveryfrom the usual effects of hypo-thyroidism and how far it repre-sented regression of amyloidosis.
Localized AmyloidosisCase 8: Amyloidosis of Unknown
Cause Apparently Confined to theMammary Areolae and the Vulva.-A medical woman, aged 24, who hadnever had any serious or chronic ill-ness, volunteered to take part in aninvestigation in normal people of thehaemostatic activity of Congo red andof the uptake and excretion of thedye. She was given an intravenousinjection of 10 ml. of 1'l solution ofCongo red: the usual calculationshowed 65% of the dye still to bepresent in the blood stream 60 mi-nutes after the injection. Nextmorning she noticed a red circlearound the areola of each breast.Examination showed a vivid red zone.
i. wide, in the skin of each breast, sharplys periphery and merging centrally with theireolae were black and completely smooth;)peared healthy, but was fixed almost im-an underlying disc of tough, remarkablyLe. This disc had a thin but distinct edgeided precisely with the outer edge of thene: it was possible to press one's fingersthe disc, which seemed to be uniformly. in thickness, except at its tapered edge;3ing it from side to side it bent up likesole of a slipper, springing back at onceDUS shape when released. The nipples1. The skin of the axillae, vulva, ands melanotic, although considerably less soolae. The labia minora were well devel-ot abnormally large or thick; each con-ral irregular, indurated plaques, up tois, which occupied the full thickness ofand were adherent to its skin on themedial side of the labium the skin imme-the plaques showed the same peculiar red
224
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
colour as was seen on the breasts, and the hymenwas similarly coloured. Clinical examination showedno other abnormality; no unusual pigmentations or
other lesions were found elsewhere in the skin.The patient said that the indurated plaques had
been present ever since her breasts developed atpuberty, about 11 years before, and that the areolarskin had always been smooth, relatively firmlyattached to the plaques, and uncontractile, whereasthe nipples were erectile. She herself attributed theintense melanosis of the areolae, axillae, and vulva toa former habit of occasionally taking large doses ofhexoestrol by mouth in order to delay menstruation.At the time of the Congo red injection she had nottried to interfere with menstrual function for almosttwo years, and her cycle was perfectly normal.
Ins estigations.-Urine, blood picture, erythrocytesedimentation rate, plasma proteins, serum electrolytes,and chest radiographs were normal. A biopsy of thered zone on one breast showed that the underlyingplaque consisted of amyloid, intensely stained in situby Congo red. Microscopically, the amyloid formeda dense, homogeneous mass, sharply demarcated fromthe normal underlying adipose tissue; only a shallowzone of the superficial part of the dermis was un-affected. No muscle was seen in the sections, otherthan that of the blood vessels, which were normal;epidermal appendages were also absent, although theepidermis itself appeared to be normal apart fromintense pigmentation with melanin at the edge of theareola. The amyloid stained metachromatically withmethyl violet ; there was no cellular reaction of any
sort around it.
Progress.-The Congo red staining of the areolaefaded gradually, but traces were still visible for morethan five months. The patienit has kept perfectly wellduring the five years which have passed since theamyloid nature of the plaques was discovered. Shehas been married for three years, and has two children,both of whom were breast-fed without difficulty. Inview of the introital induration hymenectomy was
performed before marriage; the presence of amyloidin the hymen was confirmed microscopically, andvery faint traces of the original Congo red stainingwere recognizable although almost two years hadpassed since the injection. The patient has noticedno difference in the amyloid plaques in the breasts,although those in the labia are no longer palpable.
This case appears to be unique, not only in theway in which it came to light but in the distribu-tion of the deposits also. The manifestations donot correspond to any recognized form ofcutaneous amyloidosis (Andrews, 1954), whetherlocalized or as a manifestation of generalizedamyloidosis. There is clearly no evidence of any
generalized disease in this patient. It is note-worthy that the subareolar discs were known byher to be present before she took oestrogens : a
causal relation betweeen this self-medication and
the amyloidosis can be set aside. Other varietiesof localized amyloidosis have been mentionedbriefly elsewhere (Symmers, 1956).
Amyloidosis Associated with Rheumatic HeartDisease
Case 9: Amyloidosis and Recurrent RheumaticPancarditis. A woman, aged 43, was admitted tohospital with acute polyarthritis. She had had rheu-matic fever at the ages of 16, 20, 32, and 36, andsevere mitral and aortic valvular lesions were present.Acute heart failure developed, and she died five daysafter admission.Necropsy showed acute rheumatic pericarditis and
endocarditis, with old rheumatic disease of all fourvalves, and generalized chronic venous congestion.Histological examination showed acute rheumaticlesions in all parts of the heart. There was amyloidmacroglossia, widespread amyloidosis of blood vesselsthroughout the body, and pericellular amyloidosis inthe musculature of the alimentary tract and to aslight degree in the myocardium. The amyloiddeposits in the myocardium appeared to be indepen-dent of the Aschoff bodies, and of the old interstitialscars. Except for involvement of their larger bloodvessels the kidneys, liver, spleen, and adrenals werefree from amyloid.Case 10: Amyloidosis and Recurrent Rheumatic
Carditis and Polyarthritis. A woman, aged 53, wasadmitted to hospital because of fever, polyarthritis,and anaemia. Her only previous illness was rheumaticfever at the age of 20, and this had left her withaortic-valve incompetence. A year before admission,and just after the menopause, she began to haverecurrent attacks of painful swelling of the knees.ankles, wrists, and hands, and her health steadilyfailed. Aspirin regularly relieved the pain. Onadmission, examination showed painful swelling, red-ness, and effusion in the knee, wrist, and finger joints;there was no deformity. Gross aortic-valve incom-petence was present; there was no evidence of heartfailure. Temperature 100° F. (37.80 C.). Urine:protein + +. Blood: erythrocytes 2,500,000 perc.mm., haemoglobin 7.7 g. per 100 ml., leucocytes13,100 (80°,0 neutrophil polymorphs). Blood culturessterile. Wassermann and gonococcal complement-fixation tests negative. Serum antistreptolysin titre20 units per ml. Four days after admission she diedsuddenly.Necropsy showed gross scarring with calcification
of the aortic valve, which was stenotic and incompe-tent; the mitral valve showed less severe old rheum-atic disease. The left ventricle was much hyper-trophied and dilated. There were old pericardialadhesions and severe coronary atheroma. Widespreadamyloidosis was present, affecting predominantly theparenchyma of the kidneys, liver (Fig. 9), and spleen.Occasional Aschoff bodies (Fig. 10) and extensive oldinterstitial fibrosis were found in the myocardium.These two cases illustrate the association of
rheumatic fever and amyloidosis; in one case the
225
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

226 W. St. C. SYMMERS
!i AC-0' ;oe
* * *,* *** r,'wa.¢4 ~
'.tsS '', ' S;W tWg ;'t:w; ' ? {;~~~~~~~~~~~~~~~~~~~~~~!
-0. ~ ~ ~ ~ FG 9
FIG 10b:'
FIG .9.-Casel10. Amyloidosis of hepatic portaltracts. Haematoxylin and eosin. x 130.
FIc,. IO.--Case 10. Aschoffbody. Haematoxylinand eosin. -,180.
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

FIVE CASES OF PRIMARY GENERALIZED AMYLOIDOSIS
distribution of the amyloid deposits was that com-monly seen in primary amyloidosis and in theother the picture was that of classical secondaryamyloidosis. Amyloidosis is seldom found inassociation with rheumatic fever or its sequelae,but such cases have been described from time totime, for instance, by Wilks (1856), Beattie (1906),Dillon and Evans (1942), and Jackson (1954).Amyloidosis is much oftener seen as a complica-tion of rheumatoid arthritis (Reece and Reynolds,1954). The arthritis in the second of these twocases was considered on clinical grounds to berheumatic in type rather than rheumatoid.The association of amyloidosis with rheumatic
fever has been said to suggest a relationship be-tween amyloidosis and the so-called collagendiseases (Jackson, 1954) ; this scarcely seems towarrant describing any form of amyloidosis as a
" collagen disease," and the relationship may proveto be tenuous or even illusory.
Two Unusual Cases of Amyloidosis Associated withChronic Infection
Case 11: Predominantly Cardiovascular and Lin-gual Amyloidosis Associated with Chronic Suppura-tive Osteomyelitis. A man, aged 36, was admitted tohospital in the last stages of congestive heart failure;he died two days later. He had had chronic suppura-tive osteomyelitis of the left femur for 14 years, withconstant purulent discharge from two sinuses: the con-
dition had caused him little inconvenience and he haddeclined to have any treatment, except occasionally toallow removal of small protruding sequestra. A yearbefore his death he began to develop symptoms ofcongestive heart failure and his tongue was noted tobe enlarging. No cause for the cardiac conditioncould be found clinically, and it proved to be refrac-tory to all forms of treatment. A series of electro-cardiographs showed a progressive fall in voltage in allleads during the last 10 months of his life. TheWassermann and Kahn tests were negative.Necropsy showed severe chronic suppurative osteo-
myelitis of the femur, with large sequestra and severalramifying sinuses. There was no evidence of tuber-culosis. The heart was enlarged and showed wide-spread amyloidosis. Lingual amyloidosis and amyloidplaques in the intestines were present. Histologically,there was extensive amyloidosis of blood vessels andof the musculature of the heart, tongue, alimentarytract, and abdominal wall. There was minimal amyl-oidosis of the liver, spleen, kidneys, and lungs. Theamyloid stained metachromatically with methyl violetand showed a moderate affinity for Congo red.
Case 12: Predominantly Cardiovascular Amyloid-osis Associated with Chronic Actinomycosis.-Awoman, aged 27, had appendicectomy in 1939 foracute suppurative appendicitis. The laparotomywound did not heal fully, and a faecal fistula devel-
oped. Five months later the fistula was excised andright-sided colectomy was performed. This was fol-lowed by the development of multiple abscesses, withsinuses and fistulae in the abdominal wall. A yearafter the appendicectomy an abscess formed in theright lung and was followed by pleural empyema andbronchopleural fistula. Actinomyces (israeli) wasrepeatedly isolated from pus from the abdominal andthoracic lesions. The patient became grossly emaciatedand cachectic, and 19 months after the appendicectomyshe died of actinomycotic meningitis. There was noclinical evidence of amyloidosis.
Necropsy showed extensive abdominal and thoracicactinomycosis, with terminal pyaemia and meningitis.There was no macroscopical evidence of amyloidosis,but sections showed very extensive pericellular amyl-oidosis of the myocardium, in the musculature of thestomach and intestines, in the myometrium and in theabdominal muscles. There was heavy involvement ofthe walls of arteries, arterioles, and veins in all thetissues sectioned, but no amyloid deposits were foundin the parenchyma of the liver, kidneys, or spleen.The amyloid had little affinity for Congo red, and itshowed metachromasia with methyl violet only insome areas.
These two cases illustrate that amyloidosisoccurring with such a well-known predisposingcondition as chronic suppuration can present thedistribution which is usually associated with prim-ary amyloidosis: the converse was illustrated byCase 5. While such observations do not provethe identity of all forms of amyloidosis, they in-dicate that the distribution of the deposits is nota sufficient criterion by which to attempt to dis-tinguish different varieties.
SummaryTwelve cases of amyloidosis are described.Five are cases of generalized amyloidosis with-
out apparent predisposing cause (" primary amy-loidosis"): heart failure, peripheral neuropathy,goitre, haemorrhage, and pulmonary lesions wereamong the presenting manifestations.Two cases of amyloidosis associated with severe
hypothyroidism following treatment for hyper-thyroidism are reported, and the possible signi-ficance of the hormonal disturbance is discussed.
Amyloidosis, confined to the mammary areolaeand vulva, was found unexpectedly in an other-wise healthy young woman.Two cases of amyloidosis associated with recur-
rent rheumatic carditis are described. In one thedistribution of the amyloid was that usually seenin primary amyloidosis; in the other it was thatseen in classical cases of secondary amyloidosis.Two cases of amyloidosis in patients with
227
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from

W. St. C. SYMMERS
chronic septic lesions (osteomyelitis; widespreadactinomycosis) are reported in which the amyloidwas predominantly deposited in the cardiovascularsystem, almost completely sparing the organsusually affected in secondary amyloidosis.
Amyloidosis occurring without an apparent pre-disposing cause, that is, primary amyloidosis, in-cluding the predominantly cardiovascular senileamyloidosis, is probably commoner than secondaryamyloidosis, particularly now that the incidenceof the latter has been so much reduced by ad-vances in the treatment of the diseases whichformerly were its most frequent predisposingcauses. Many more cases will have to be recog-nized during life if the nature of amyloidosis andthe possibilities of developing methods of treatingit are to be adequately investigated.
I am indebted to many colleagues for permisisonto include accounts of their cases in this paper. Inparticular, I should like to thank Dr. A. P. Barter,Dr. P. B. S. Fowler, Dr. D. R. Humphreys, Dr.A. C. F. Ogilvie, Dr. N. S. Plummer. Dr. W. H.Russell Rees, Dr. J. H. Shore. and Dr. C. B. I. Willeyfor their help.My thanks are also due to Mr. Allan Ayres and
Mr. Frank Humberstone for technical assistance, andto Mr. K. W. Iles for help in preparing the photo-micrographs.
REFERENCESAndrews, G. C. (1954). Diseases of the Skin for Practitioners and
Students, 4th ed., pp. 579-583. Saunders, Philadelphia andLondon.
Beattie, J. M. (1906). Brit. med. J., 2, 1444.Brewer, D. B. (1951). J. Path. Bact., 63, 503.Bruns, G. (1955). Zbl. allg. Path. path. Anat., 93, 246.Case Records of the Massachusetts General Hospital (1956). New>
Engl. J. Med., 254, 226.Dahlin, D. C. (1949). Ann. intern. Med., 31, 105.Dillon, J. A., and Evans, L. R. (1942). Ibid., 17, 722.Drapiewski, J. F., Sternlieb, S. B., and Jones, R. (1955). Ibid., 43,
406.Eisen, H. N. (1946). Amer. J. Med., 1, 144.Gunnar, R. M., Dillon, R. F., Wallyn. R. J., and Elisberg, E. I.
(1955). Circulation (N.Y.), 12, 827.Haemmerli, A. (1954). Schweiz. med. Wschr., 84, 1262.Husselmann. H. (1955). Virchows Arch. path. Anat., 327, 607.Jackson, A. (1954). Arch. intern. Med., 93, 494.King, F. H., and Oppenheimer, G. D. (1948). Ann. intern. Med., 29,
374.Koletsky, S., and Stecher, R. M. (1939). Arch. Path. (Chicago), 27.
267.Lubarsch, 0. (1929). Virchows Arch. path. Anat., 271, 867.Mathews, W. H. (1954). Amer. J. med. Sci., 228, 317.Muehrcke, R. C., Pirani, C. L., Pollack, V. E., and Kark, R. M.
(1955). Guy's Hosp. Rep., 104, 295.Perasalo, O.. and Latvalahti, J. (1954). Acta path. microbiol. scand.,
34, 208.Propp, S., Scharfman, W. B., Beebe, R. T., and Wright, A. W.
(1954). Blood, 9, 397.Reece, J. M., and Reynolds, T. B. (1954). Amer. J. nied. Sci., 228.
554.Ritama, V., and Bjorkesten, G. af (1954). Ann. AMed. intern. Fetin.,
43, 152.Snapper, I., Turner, L. B., and Moscovitz, H. L. (1953). Multiple
Myeloma, pp. 85-94. Grune and Stratton, New York.Soyka, J. (1876). Prag. med. Wschr., 1, 165.Symmers, W. St. C. (1956). Journal of Clinical Pathology. 9, 187.Uotila, U., Perasalo, O., and Vapaavuori, M. (1955). Acta path.
microbiol. scand., 37, 322.Walker, G. A. (1942). Surg. Gynec. Obstet., 75. 374.Wild, C. (1886). Beitr. path. Anat., 1, 175.Wiley, A. T., Teeter, R. R., and Schnabel, T. G. (1951). Med. Clini.
N. Amer., 35, 1841.Wilks, S. (1856). Guy's Hosp. Rep., 17, (Series 3, 2) 103.
228
on July 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.9.3.212 on 1 A
ugust 1956. Dow
nloaded from