ALCOHOLIC LIVER DISEASE
62
ALCOHOLIC LIVER DISEASE
-
Upload
karl-daniel-md -
Category
Documents
-
view
3.504 -
download
0
description
Transcript of ALCOHOLIC LIVER DISEASE

ALCOHOLIC LIVER DISEASE

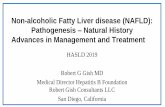
Колебания смертности в России 1984-1994 г.г.
Сердечно-сосудистые Сердечно-сосудистые заболеваниязаболевания
1987-1994
1984-1987
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
Общая смертностьОбщая смертность
Онкологические заболеванияОнкологические заболевания
ПневмонииПневмонии
0,5
0,1
10
5
2
1
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
Алкоголь- Алкоголь-
обусловленные обусловленные
заболевания заболевания
0,5
0,1
10
5
2
1
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
0,5
0,1
10
5
2
1
1- 4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80 ЛЕТ
НесчастныеНесчастныеслучаи и случаи и
насильственнаянасильственная смерть смерть
0,5
0,1
10
5
2
1
0,5
0,1
10
5
2
1
0,5
0,1
10
5
2
1
Leo
n D
., Ш
коль
нико
в В
., За
харо
в С
. и д
р. L
ance
t, 19
97

Principal alcohol-induced hepatic lesions
• alcoholic fatty liver (steatosis)• alcoholic hepatitis (steatohepatitis)• alcoholic cirrhosis• hepatocellular carcinoma• These morphologic categories are rarely
found in a pure form• Features of each may be present to varying
degrees in an individual patient.


Alcohol-induced hepatic lesions: 1
• only a minority of consistently heavy drinkers with hepatic
steatosis (15 to 20 %) ever have clinically important liver disease (LD)• Other host or environmental factors have a role in determining the evolution of alcohol-related liver disease (ARLD)
•Risk factors for serious liver damage in habitual alcohol drinkers include certain polymorphisms in alcohol-metabolizing enzymes, obesity, exposure to other hepatotoxins (e.g., acetaminophen), and infection with hepatitis C
•In many patients, a specific RF is never identified.

Alcohol-induced hepatic lesions: 2
• Numerous reports point to an association between episodes of gastrointestinal bleeding or sepsis and an acute, clinical
decompensation of ARLD suggesting that endotoxemia potentiates the progression of the disease.
• The appearance of steatohepatitis is an important rate-limiting step in the development of progressive ARLD
•One-month mortality rates of 40 to 50 % have been reported
among pts hospitalized with acutely decompensated liver
disease due to alcohol-induced steatohepatitis.
•Furthermore, cirrhosis develops in almost half the survivors within five years.


Pathogenesis• Acetaldehyde has been shown to stimulate collagen
production in cultured lipocytes and myofibroblasts and fibroblasts
• At the earliest stages (simple or uncomplicated fatty liver), collagen is detectable by chemical means only
• Hereditary predisposition may play a role
• For the transition of the more benign to the more severe stages of the disease, autoimmune mechanisms have been postulated and cytotoxicity of lymphocytes documented
• It is unclear how alcoholic hepatitis eventually develops into cirrhosis

Cytokines and liver damage
• Cytokines are pleiotropic regulatory peptides that can be produced by virtually every nucleated cell in the body, including most types of liver cells.
• The cytokine family consists of several subfamilies•: the interleukins •the tumor necrosis factor (TNF) family• interleukin-6 and related cytokines• interferons• chemokines such as interleukin-8• transforming growth factor ß• colony-stimulating factors• others

Cytokines and liver damage
• In most tissues, including the liver, constitutive production of cytokines is absent or minimal.
• However, as physiologic and pathologic stimuli activate cells, the production of these autocrine, paracrine, and endocrine effector molecules increases
• They, in turn, orchestrate the tissue's response to the stimulus.
• There is increasing evidence that several cytokines mediate
hepatic inflammation, apoptosis and necrosis of liver cells,
cholestasis, and fibrosis, but paradoxically, they also mediate the regeneration of liver tissue after injury

Cytokines and liver damage
• Among the various cytokines, the proinflammatory cytokine TNF- has emerged as a key factor in various aspects of liver disease.
• Some of the most definitive data on the importance of TNF- in the pathogenesis of liver disease come from studies of alcoholic and nonalcoholic steatohepatitis in animals
• In combination with data from clinical studies, these findings indicate that TNF- mediates not only the early stages of FLD but also the transition to more advanced stages of liver damage.

Biomedical and cellular pathogenesis of liver injury secondary to chronic
ethanol ingestion
• MAA, malondialdehyde-acetaldehyde
• TNF-, tumor necrosis factor • TGF-, transforming growth factor ; IL,
interleukin


Pathophysiologic Relevance of Cytokines (C) in Chronic Liver Disease (CLD): 1
•Most types of cells in the liver, including Kupffer cells, hepatocytes, and stellate cells, either synthesize or respond to C
•In the early phase of CLD, specific agents (viruses, ethanol, toxins) may stimulate the production of C
•In the late phase, endotoxin may be the key agent stimulating C production.
• Clinical features of CLD mediated by C include cachexia, cholestasis, fibrosis, synthesis of acute-phase proteins, and hypergammaglobulinemia.

Pathophysiologic Relevance of Cytokines (C) in Chronic Liver Disease (CLD): 2
•Proinflammatory C (TNF, IL-6) are mainly involved in cholestasis and the synthesis of acute-phase proteins, transforming growth factor ß (TGF-ß) released by activated Kupffer cells and hepatocytes may be one of the critical C involved in fibrosis.
• In pts with progressive LD, the balance between proinflammatory and antiinflammatory C may be shifted toward the proinflammatory axis, thus the counteracting antiinflammatory C are unable to control inflammation and fibrosis.

Pathophysiologic Relevance of Cytokines in Chronic Liver Disease.

The production of TNF- is one of the earliest events in many types of liver injury, triggering the production of other cytokines
that together recruit inflammatory cells, kill hepatocytes, and initiate a healing response that includes fibrogenesis

. Hepatocyte Responses to Tumor Necrosis Factor (TNF-).

Эквиваленты абсолютного алкоголя
• Водка 28 мл 10 г
• Вино 85 мл 10 г
• Пиво 230 мл 10 г
• Минимальные повреждения печени -
начиная с 30 г/сут ?• 210 г этанола еженедельно-БЕЗОПАСНО

Маркеры хронической алкогольной интоксикации
• Ожирение Дефицит веса• Транзиторная гипертония Тремор• Полинейропатия Мышечная атрофия• Гипергидроз Гинекомастия• Паротит Обложенный язык• Татуировка Гепатомегалия• Контрактура Дюпюитрена• Телеангиэктазии Следы травм• Макроцитоз Гаммаглютаматтранспептидаза


Этиологические факторы паротита
• Алкоголизм
• Диабет
• Подагра
• Синдром Шегрена
• Саркоидоз
• Лимфома



Этиологические факторы контрактуры Дюпюитрена
• Алкоголизм
• Ручной труд
• Старая травма кисти
• Диабет
• Эпилепсия (лекарства?)
• Пожилой возраст

Этиологические факторы гинекомастии
• Хронические гепатиты и циррозы печени
• Алкоголизм
• Лекарства
• Гипертироз
• Уремия - гемодиализ
• Первичный гипогонадизм







polyneuropathia

Лабораторные признакиХАИ
Повышение в крови активности гамма-глютамилтранспептидазы
Повышение среднего объема эритроцитов
Повышение уровня трансферина
Сочетание 6 и более клинических илабораторных признаковсвидетельствует о регулярномупотреблении алкоголя.


Alcoholic fatty liver
• Clinical manifestations are often minimal or entirely absent
• the disorder may not be recognized unless another illness (frequently alcohol-related) brings the patient to medical attention
• Hepatomegaly, at times accompanied by tenderness, may be the only finding
• Jaundice, ascites, and edema are seen only with more serious liver injury.

Two-Hit Model of the Progression of Fatty Liver Disease

Two-Hit Model of the Progression of Fatty Liver Disease. • The earliest stages of FLD involve exposure of hepatocytes to TNF-
• TNF- initiates various intracellular signals mitochondrial
permeability and the release of reactive oxygen species (ROS).
• Left unchecked, these responses promote hepatocyte apoptosis.
• Most healthy hepatocytes use some of the potentially lethal signals
(e.g.,ROS) to activate a multifaceted response that permits
the hepatocytes to survive.
• Secondary insults (second hits) that inhibit this adaptation also result
in apoptosis
• Even when adaptation is successful and hepatocytes remain viable,
they become extremely vulnerable to other insults that partially
depolarize the mitochondrial inner membrane, dying by necrosis
when the mitochondrial membrane potential collapses.

Alcoholic fatty liver
• Fatty liver invariably develops after heavy alcohol intake
• It can progress to alcoholic hepatitis and cirrhosis
• In some patients, alcoholic hepatitis is a necessary step in the development of alcohol-induced cirrhosis
• However, in some other patients alcohol may stimulate the production of fibrosis and cirrhosis without requiring alcoholic hepatitis as an intermediate lesion.



Similarities between Alcoholic and Nonalcoholic Fatty Liver Diseases
• Obesity (OB) and alcohol abuse (AA) are associated with the same spectrum of liver diseases.
• The time course for the progression of disease and the RR of cirrhosis are also similar in obesity-related liver disease (ORLD)and ARLD
• Distinct, but mutually enhancing, mechanisms may also be involved
• The similar pathologic features and natural histories of the two types of FLD suggest that common pathogenic mechanisms may be involved.
• A fatty liver is more common in pts with OB and AA than in those with either alone.
• Moreover, OB is an independent RF for cirrhosis in pts who AA Thus,
elucidation of the mechanisms that cause ORLD is liikely to clarify the role of pluripotent cytokines, such as TNF- , in promoting alcohol-induced liver damage.

Alcoholic hepatitis
• The clinical features AH resemble those of viral or toxic liver injury
– anorexia, nausea and vomiting, malaise, weight loss, abdominal distress, and jaundice
– Fever is seen in about half of cases.
• On physical examination– tender hepatomegaly is common– splenomegaly is found in about one-third of patients– the patient may have cutaneous arterial "spider" angiomas and jaundice
More severe cases may be complicated by ascites, edema, bleeding, and encephalopathy.



This figure depicts a laparoscopic view of a patient
with chronic active hepatitis and early cirrhosis


Острый алкогольный гепатит
• Гепатомегалия 87%
• Желтуха 60% Боли в животе 18%
• Асцит 50% Панкреатит 11%
• Анорексия 50% Полинейропатия10%
• Энцефалопатия 45% Гипертония 10%
• Спленомегалия 25%
• Лихорадка 23%

Percutaneous liver biopsy with or without ultrasonic guidance
• standard diagnostic approach for establishing the presence of chronic hepatitis
• Laparoscopic liver biopsy, which is used in large referral centers, has the advantage of minimizing the sample error by facilitating gross inspection of the liver and thus ensuring an adequate biopsy sample size.

Alcoholic hepatitis: liver biopsy
• Major features found include – marked variation in cell size– evidence of cell necrosis and variable inflammation with a
mixture of polymorphonuclear and mononuclear cell– there is evidence of variable sinusoidal compression– pericellular fibrosis is an important feature
– In many pts eosinophilic inclusions (Mallory bodies) are found
– Often the most intense alcoholic-induced injury is in Zone III (centrilobular)




• In the alcohol-fed baboon model, fibrosis and cirrhosis developes in the absence of alcoholic hepatitis
• Only a minority of heavy drinkers develop cirrhosis and, experimentally, only one third of baboons fed a high dose of alcohol developed lesions more severe than those of fatty liver
• The reason for this individual susceptibility to the development of these more severe complications is not known.
• Markers of HBV 46%• Markers of HCV 80%

Treatment of severe alcoholic hepatitis
• Administration of prednisolone in moderately large doses may be helpful in patients with encephalopathy
• However, the use of glucocorticoids in acute alcoholic hepatitis remains controversial and should probably be reserved
• Maintenance therapy with colchicine (0.6 mg PO bid) has been shown to slow disease progression and increase longevity of the patient with alcoholic liver disease in one long-term study.

Причины смерти при алкогольном гепатите
• Печеночная недостаточность (кома) 56%
• Кровотечение 31%
• Гепаторенальный синдром 28%
• Инфекция 15%

TNF- and Progression from Steatohepatitis to Cirrhosis
•Transient reconfiguration of the extracellular matrix of the injured liver, which permits the infiltration of inflammatory cells, facilitates the local accumulation of growth factors, and accommodates regenerating hepatocytes, is a critical component of healing after liver injury (LI).
•After acute LI from various insults ( toxins, viral infections, or surgical trauma the resorption and deposition of the components of the matrix are balanced, and therefore there is no accumulation of fibrous tissue
• However, chronic inflammatory conditions, such as alcoholic and nonalcoholic steatohepatitis, alter the composition of the matrix and upset the balance between the synthesis and degradation of the matrix.
• Consequently, fibrosis occurs, compromising portal venous blood flow, which in turn both compromises hepatic regeneration and promotes the portosystemic shunting of blood that leads to some of the clinical manifestations of advanced LD

Alcoholic cirrhosis
• The typical alcoholic patient with cirrhosis has had a daily consumption of a pint or more of whiskey, several quarts of wine, or an equivalent amount of beer for at least 10 years.
• The amount and duration of ethanol ingestion, rather than the type of alcoholic beverage or the pattern of ingestion, appear to be the important determinants

Alcoholic cirrhosis
• historically referred to as Laennec's cirrhosis
• is the most common type of cirrhosis in North and South America and in western Europe
• It is characterized by diffuse fine scarring, fairly uniform loss of liver cells, and small regenerative nodules
• may be clinically silent and 10 to 40% cases are discovered incidentally at laparotomy or autopsy
• In many cases symptoms are insidious in onset, occurring usually after 10 or more years of excessive alcohol use and progressing slowly over subsequent weeks and months

Alcoholic cirrhosis: clinical manifestations
• Easy bruising• Increasing weakness and fatigue• Hepatocellular dysfunction and portal hypertension• Anorexia and malnutrition lead to weight loss and a
reduction in skeletal muscle mass • Progressive jaundice• Bleeding from gastroesophageal varices, ascites• Encephalopathy• Progressive renal dysfunction often complicates
the terminal phase of the illness.