
Aktuelles zur adjuvantenAktuelles zur adjuvanten ... · Aktuelles zur adjuvantenAktuelles zur...
21
Aktuelles zur adjuvanten Aktuelles zur adjuvanten Systemtherapie Systemtherapie Daniel Sattler Praxis Gynäkologie Arabella 21 Oktober 2017 21. Oktober 2017
Transcript of Aktuelles zur adjuvantenAktuelles zur adjuvanten ... · Aktuelles zur adjuvantenAktuelles zur...

Aktuelles zur adjuvantenAktuelles zur adjuvanten SystemtherapieSystemtherapie
Daniel SattlerPraxis Gynäkologie Arabella
21 Oktober 201721. Oktober 2017
Adjuvante Systemtherapie
- Endokrine TherapieChemotherapie- Chemotherapie
- AK: Trastuzumab (Herceptin®)- AK: Trastuzumab (Herceptin )Pertuzumab (Perjeta®)Pertuzumab (Perjeta )
- Bisphosphonate

Adj t d k i Th iAdjuvante endokrine Therapie
Nur falls rezeptorpositiv:Nur falls rezeptorpositiv: >=1% der Zellen!
Fast immer indiziertFast immer indiziert, aber: Nutzen-Risiko-Abwägung!
D 5 10 J h (ATLAS TT MA 17)Dauer: 5-10 Jahre (ATLAS, aTTom, MA.17)

Adjuvante endokrine TherapieAdjuvante endokrine Therapiein der Prämenopause
Standard: Tamoxifen 5 10 JahreStandard: Tamoxifen 5-10 Jahre
B i höh Ri ik d/ d <35 J h ltBei höherem Risiko und/ oder <35 Jahre altern.:GnRH 2-5 Jahre + Tamoxifen 5-10 Jahre oderGnRH 5 Jahre + Aromataseinhibitor 5 Jahre
Kein Aromataseinhibitor ohne GnRH!

Adjuvante endokrine TherapieAdjuvante endokrine Therapiein der Postmenopause
Switch: Tam →→ AIoder AI →→ Tamoder AI →→ Tam
Upfront AI: bei N+, inv. lobulärem Ca.Tamoxifen: niedriges Risiko, Osteoporose,
NW AI> 5 Jahre: bei höherem Risiko, z.B. N+
/ äund/ oder guter Verträglichkeit

Adjuvante Chemotherapie
Indikation zur Chemotherapie:Indikation zur Chemotherapie: G3, hohes Ki 67, niedrige Rezeptoren, HER2 pos., triple negativ, >3 bef. Lk
Chemo mit Antrazyklin + Taxan Standard bei:Chemo mit Antrazyklin Taxan Standard bei: HER2+, triple negativ, Luminal B, neoadjuvantneoadjuvant
Chemo dosisdicht: insbes. bei hohem LK-Befall oder triple negativ
Adjuvante ChemotherapieAdjuvante ChemotherapiePrognosetests
Oncotype DX ® (21 Gene) Endopredict ® (8 Gene)Mammaprint ® (70 Gene)Mammaprint ® (70 Gene)Prosigna ® (50 Gene) alle AGO +
- Nur bei grenzwertiger Chemotherapieindikation!
- bei N0 und N1 (≤ 3LK) ER pos HER2 negativbei N0 und N1 (≤ 3LK), ER pos., HER2 negativ und endokriner Therapie

Adjuvante Chemotherapie
E 1199 (Sparano 2008 2015):E 1199 (Sparano 2008, 2015):4954 Patientinnen:
4 x Paclitaxel (3-wöchentlich)12 x Paclitaxel (wöchentlich)12 x Paclitaxel (wöchentlich)
4 x AC4 x Docetaxel (3-wöchentlich)12 x Docetaxel (wöchentlich)12 x Docetaxel (wöchentlich)

Adjuvante Chemotherapie
aktuelles Follow-up 12,1 Jahre (2015) Hazard ratioHazard ratio
DFS OS4 x Paclitaxel 1 112 x Paclitaxel 0 84 0 87 n s12 x Paclitaxel 0,84 0,87 n.s.
4 x Docetaxel 0,79 0,86 n.s.
12 x Docetaxel n.s. n.s.explorat: TNBC: nur 12 x Pacli dtl. signif. p g
HR pos., HER2 neg.: nur 4 x Doce signif.

Adjuvante Chemotherapie:Adjuvante Chemotherapie:anthrazyklinfrei?
WSG PlanB-Studie (Harbeck et al ASCO 2017):WSG PlanB-Studie (Harbeck et al. ASCO 2017):- 2449 Patientinnen- HER2-negativ - Rezeptor-positiv und –negativ- Rezeptor-positiv und –negativ- N+: 41% (≥4 LK: < 10%)
Random: 6 x TC vs. 4 x EC→4 x Doc

Adjuvante Chemotherapie:Adjuvante Chemotherapie:anthrazyklinfrei?
WSG PlanB-Studie (Harbeck et al ASCO 2017):WSG PlanB-Studie (Harbeck et al. ASCO 2017):- Medianes Follow-up 5,1 Jahre- DFS 89,9 vs. 90,2%
OAS 94 7 vs 94 6%- OAS 94,7 vs. 94,6%
6 TC 4 EC 4 D !6 x TC = 4 x EC→4 x Doc!

Adjuvante Chemotherapie:Adjuvante Chemotherapie:anthrazyklinfrei?
ABC Trials (Blum et al. JCO 2017)( )- 4242 Patientinnen in 3 amerik. Studien- HER2 negativ- Rezeptor-positiv und -negativRezeptor positiv und negativ- Non-Inferiority-Trial
Random: 6 x TC vs. 6 x TAC oder A-T-Sequenz

Adjuvante Chemotherapie:Adjuvante Chemotherapie:anthrazyklinfrei?
ABC Trials (Blum et al. JCO 2017)( )- 334 IDFS-Events (50%)
M di F ll 3 3 J h- Medianes Follow-up 3,3 Jahre- HR 1,202 (> 1,18), ( , )- IDFS 88,2 vs 90,7%
G ößt B fit b i ≥4 LK d t i l ti- Größter Benefit bei ≥4 LK und triple negativ
AT-Kombination oder Sequenz > 6xTC!

TNBCTNBC(Triple negatives Mammakarzinom)
- Chemotherapie besser präop.!Chemotherapie besser präop.!- Cis-/ Carbo-Platin, insbes. bei BRCA-Mutation- CMF ist Option: Wang et al 2012
CMF vs. Anthrazyklin und/ oder TaxanCMF vs. Anthrazyklin und/ oder Taxan (retrosp.): HR 0,66! B i CR dj t C it bi 6 8 Z kl- Bei non-pCR adjuvant Capecitabine 6-8 Zyklen mit Benefit (Masuda et al NEJM 2017)
Adjuvante Chemotherapie
Chemotherapieschemata mit AGO ++:Chemotherapieschemata mit AGO ++:
4 x A/EC 12 x Paclitaxel wöchentlich4 x A/EC, 12 x Paclitaxel wöchentlich4 x A/EC, 4 x Docetaxel6 x TACETC dosisintensiv (2 wöchentlich)ETC dosisintensiv (2-wöchentlich)

Adjuvant TrastuzumabAdjuvant Trastuzumab (Herceptin®)
Voraussetzung: HER2-positiver Tumorg pICH 3+ , ICH 2+ und FISH/ CISH positivE f hl dj t b T1b (T ößEmpfehlung: adjuvant ab pT1b (Tumorgröße
> 5 mm)Chemo-AK-Therapie besser präop.!
Therapiedauer: 1 JahrTherapiedauer: 1 JahrApplikation: 3-wöchentlich oder wöchentlich,
i.v. oder 3-wöchentlich s.c.
Adjuvant TrastuzumabAdjuvant Trastuzumab (Herceptin®)
Empfohlene Chemotherapieschemata:
4 x EC/AC, 12 x Paclitaxel + Herceptin: ++4 EC/AC 4 D t l H ti4 x EC/AC, 4 x Docetaxel + Herceptin: ++6 x TCH: +

Adjuvant TrastuzumabAdjuvant Trastuzumab APT-Trial
12 x Paclitaxel + Herceptin 1 Jahr12 x Paclitaxel + Herceptin 1 Jahrbei low risk (T< 3cm, N0, 410 Pat.):( , , )
7-J-DFS: 94 6% (rezeptorpositiv)7-J-DFS: 94,6% (rezeptorpositiv)90,7% (rezeptornegativ)
T l t l ASCO 2017Tolaney et al ASCO 2017
Adjuvant Trastuzumab + PertuzumabAdjuvant Trastuzumab + Pertuzumab APHINITY-Studie
4805 Pat., HER2 positivp63% N+36% t ti36% rezeptor-negativStandard-Chemotherapie p
+ 1 Jahr Trastuzumab P t b Pl b+ Pertuzumab vs. Placebo
Von Minckwitz et al NEJM 2017
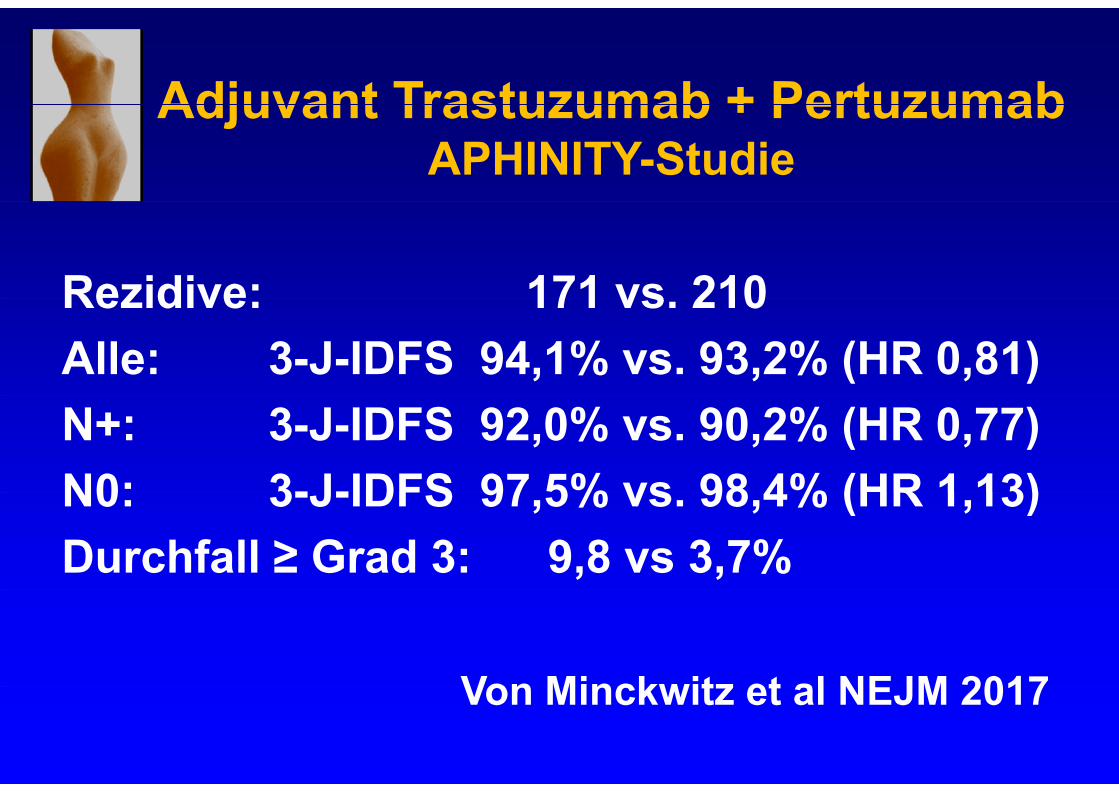
Adjuvant Trastuzumab + PertuzumabAdjuvant Trastuzumab + Pertuzumab APHINITY-Studie
Rezidive: 171 vs 210Rezidive: 171 vs. 210Alle: 3-J-IDFS 94,1% vs. 93,2% (HR 0,81)N+: 3-J-IDFS 92,0% vs. 90,2% (HR 0,77)N0: 3-J-IDFS 97 5% vs 98 4% (HR 1 13)N0: 3-J-IDFS 97,5% vs. 98,4% (HR 1,13) Durchfall ≥ Grad 3: 9,8 vs 3,7%
Von Minckwitz et al NEJM 2017Von Minckwitz et al NEJM 2017

Adjuvant Bisphosphonate
ABCSG 12: prämenopausal Zoledron (6 x alleABCSG 12: prämenopausal Zoledron (6 x alle 6 Monate) bei GnRH+Tam/ GnRH+AI
Metaanalyse EBCTCG 2015 positiv nur bei postmenopausalen Pat.p p
Zoledronat i.v. oder Clodronat oral K i Z l !Keine Zulassung! Denosumab: bisher keine adjuvanten Datenj
![Hypoallergene orthomolekulare Therapie hoT zur adjuvanten ... · die adjuvante Prüftherapie (Ablauf und Präparate-Kombinationen vgl. Tabelle 1 in Teil I [25]) nach Herstellerangaben](https://static.fdocuments.net/doc/165x107/6062fd624ee7fa5d3f7bffd0/hypoallergene-orthomolekulare-therapie-hot-zur-adjuvanten-die-adjuvante-prftherapie.jpg)

















