Age- and sex-specific estimation of dose to a normal ...
39
3 445b 0064330 0
Transcript of Age- and sex-specific estimation of dose to a normal ...

3 4 4 5 b 0064330 0


NUREC/CR-3955 ORNL/TM-9800 Dist. Category RH
Health and Safety Research Division
A G E AND SEX-SPECIFIC ESTIMATION OF DOSE TO A NORMAL THYROID FROM CLINICAL
ADMINISTRATION OF IODINE-131
George 6. Killough Keith F. Eckerman
Metabolism and Dosimetry Research Group
NOTICE This document contains information of a preliminary nature. It is subject to revision or wrrection and therefore does not represent a final report.
Manuscript Completed - July 1986 Date Published - September 1986
Prepared for the Office of Nuclear Regulatory Research
Division of Radiation Programs and Earth Sciences U.S. Nuclear Regulatory Commission
Washington, DC 20555 Research contracted through
Center for Devices and Radiological Health U.S. Food and Drug Administration
5600 Fishers Lane Rockville, MD 20857
Under Interagency Agreement FDA 224-84-6014
NRC FIN No. B5771
Prepared by the OAK RIDGE NATIONAL LABORATORY
Oak Ridge, Tennessee 37831 operated by
MARTIN MARIETTA ENERGY SYSTEMS, IPJC.
3 4 4 5 6 0067330 0


CONTENTS
Page Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
List of Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v List of Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v Abstract, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 PATIENT DATA FILE . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 DESCRIPTION OF THE MQDEL . . . . . . . . . . . . . . . . . . . . . . . 4
The retention function . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 The dosimetric S-factor . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 Calculation with the model . . . . . . . . . . . . . . . . . . . . . . . . . 12
SENSITIVITY OF THE DOSE MODEL TO UNCERTAINTIES IN THE MODEL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
DISTRIBUTION OF DOSE AMONG PATIENTS IN THE FDA DRH DATA FILE . . . . . . . . . . . . . . . . . . . . . . 14
SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . 16 ACKNOWLEDGMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . 16 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Appendix A - COMPUTATIONAL PROCEDURE FOR THE THYROID UPTAKE
AND RETENTION FUNCTION . . . . . . . . . . . . . . . . . . . . . . 18 First constraint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 Second constraint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 Third constraint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 Summary of the computational procedure . . . . . . . . . . . . . . . . . . 19
. . . 20 OTHER RADIONUCLIDES . . . . . . . . . . . . . . . . . . . . . . . . 23 The retention function . . . . . . . . . . . . . . . . . . . . . . . . . . . 23 TheS.factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 Radioactive progeny . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 Use of the dose conversion factors . . . . . . . . . . . . . . . . . . . . . . 27 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
...
Appendix B - COMPUTER IMPLEMENTATION OF THE DOSE MODEL Appendix C - ADDENDUM: DOSE CONVERSION FACTORS FOR
... u1


List of Figures
Page l a . The Riggs/ICRP metabolic model for iodine . . . . . . . . . . . . . . . . . 5 lb . Two-box metabolic model for iodine . . . . . . . . . . . . . . . . . . . . . 5
3 . Mass of the thyroid as a function of age . . . . . . . . . . . . . . . . . . 11 4 . Distributions of thyroid dose corresponding to uncertainties in biological half-time T*
and mass Mth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 25
2 . Biological half-time of iodine in the thyroid as a function of age . . . . . . . . . 9
C1 . Fractional uptake of iodine to the thyroid as a function of age . . . . . . . . .
List of Tables
Page . . . . . . . . . . . . . . . 2
. . . . . . . . . . 6 3 . Photon Specific Absorbed Fraction for the Thyroid as a Function of Thyroid Mass 10
. . . . . . . . . . . . . 10 . . . . . . . . . . 11
. . . . . . . . . 12 7 . Joint Frequency of Thyroid Dose and Age for Subjects in the FDA DRH Data File 15
24 23
C3 . Iodine S-Factor Parameters by Isotope . . . . . . . . . . . . . . . . . . . 26 C4 . Absorption Fractions (%) for Radioiodines Based on ICRP Models for the Lung and
GITract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
1 . Organization of Records in the Patient Data File 2 . Age-Dependent Retention Parameters for 1311 in the Thyroid
4 . Iodine-131 S-Factor as a Function of Thyroid Mass 5 . Sex- and Age-Dependent S-Factors for 1311 in the Thyroid 6 . Iodine-131 Dose to the Thyroid by Age and Sex (rad pCi")
C1 . Dose to the Thyroid (rad L1Ci-l) for Various Radioiodine Isotopes . . . . . . . C2 . Age-Dependent Retention Coefficients for Iodine in the Thyroid . . . . . . . .
V


ABSTRACT
This report describes the derivation of an age- and sex-dependent model of radioiodine dosimetry in the thyroid and the application of the model to estimating the thyroid dose for each of 4,215 patients who were exposed to 13’1 in diagnostic and therapeutic procedures. In most cases, the data available consisted of the patient’s age at the time of administration, the patient’s sex, the quantity of activity administered] the clinically determined uptake of radioiodine by the thyroid, and the time after administration at which the uptake was determined. The model was made to conform to these data requirements by the use of age-specific estimates of the biological half-time of iodine in the thyroid and an age- and sex-dependent representation of the mass of the thyroid. Also, it was assumed that the thyroid burden was maximum at 24 hours after administration (the lS1I dose is not critically sensitive to this assumption). The metabolic model is of the form
A ( t ) = K . (exp(-plt) - exp(-pZt)) pCi
where pi = A, + Aib (i = 1, 2), A, is the radiological decay-rate coefficient, and the Aib are biological removal-rate coefficients. The values of A i b are determined by solving a nonlinear equation that depends on assumptions about the time of maximum uptake and the eventual biological loss rate (through which age dependence enters). The value of K may then be calculated from knowledge of the uptake at a particular time. The dosimetric S-factor (rad/pCi-day) is based on specific absorbed fractions for photons of energy ranging from 0.01 to 4.0 MeV for thyroid masses from 1.29 to 19.6 g; the functional form of the S-factor also involves the thyroid mass explicitly, through which (,he dependence on age and sex enters. An analysis of sensitivity of the model to uncertainties in the thyroid mass and the biological removal rate for several age groups is reported. This model could prove useful in the dosimetry of very short-lived radionuclides. Tables of age- and sex-dependent coefficients axe provided to enable readers to make their own calculations. An addendum (Appendix C) extends the method to other radioiodines and gives age- and sex-dependent dose conversion factors for most isotopes.
V i i


INTRODUCTION
This report describes work performed at Oak Ridge National Laboratory (QRNL) for the National Center for Devices and Radiological Wealth (DRH) of the Food and Drug Admin- istration (FDA) in support of the Diagnostic '"1 Study conducted by DRH and funded by the U.S. Nuclear Regulatory Commission.* The task of ORNL was to examine a computer file consisting of records of administration of '"1 to 4,216 patients for completeness of data needed to estimate the radiation dose to the thyroid gland, and to compute the thyroid dose for each administration for which the data were sufficient.
The file to which ORNL was given access contained 5,382 records, with most records corresponding to single administrations of IsrI. A few records, however, represented follow- up observations for previously-recorded administrations. And some records were duplicates. Many records were incomplete in the data needed to estimate the thyroid dose. In some cases, these records could reasonably be completed by using information from other records on the same patient; in other cases they could not, and no dose estimate was possible.
The data file was revised and supplemented at ORNL in the following respects:
0 Duplicate records were deleted.
Incomplete records were supplemented from other records for the same patient when such supplementation appeared reasonable.
0 Dose to the thyroid was computed for each administration for which the record was complete or could be supplemented as indicated above. The computed dose was added to the record.
The dosimetric model was constructed specifically for the information contained in this file. The model requires the patient's age and sex, the quantity of radioactivity administered, the fractional uptake of "'1 by the thyroid, and the time interval from the administration to the determination of fractional uptake.
This report discusses the revised data file and details of the dosimetric model for 1311. It is intended as a reference for the use of DRH in carrying out the Diagnostic 1311 Study, as well as documentation of the model for possible use in other applications. The contents of the data file are not listed in this report.
THE PATIENT DATA FILE
The data file furnished to ORNL by DRH (which we shall call "the original file") consisted of 5,382 records of 50 characters each and represented a population of 4,216 patients. Each record corresponded to a particular administration of lS1I to a patient and determination of the fractional uptake of the radioiodine by the patient's thyroid. In some cases, multiple records existed for a single administration. In some of these instances, fractional uptake of the 1311 had been measured at two or more times after administration, but in others the multiplicity appeared redundant. Each record consisted of 16 fields, with definitions and formats as shown in Table 1.
Some of the records were incomplete in one or more fields. Approximately 11 percent of the records lacked data in one or more of the fields giving the exposure, the fractional uptake, and the time at which the uptake was determined. At the time the file was received
* Office of Nuclear Regulatory Research, Division of Rzdiation Programs and Earth Sci- ences, FIN B5771.
1

1-6
7-13 14
15-16 17-18 19--20 21-22 23-24 25-26 23-31 32-35 36-37
38
39-43 44-48 49-50
5 1-59
Patient identification The first two digits are the code for the institution w5ere the iotoye was administered. Age of patient (months) at the time of the administration. Sex of patieat (1 -:: male, 2 = female, 3 = unstated) Birth month Birth day Birth year Month of administration Day of administration Year of administration Amount cf I3lI administered ( j~Ci ) Fractional uptake of radioiodine by the patient's thyroid 6%) Time i n t e n d (bonrs) after administration when fraction31 uptake was de- termined Region of coimtry in which the institution is located:
1 - Northeast: New Ymk8 Massnchusette 2 - North Central: Ohio, Iowa, Illinois 3 - South Ccntral: Kansas, Missouri 4 - Western: California, Colorado
First diagnosis at the time of the procedure (ICDA8 code) Second diagnosis at the time of the procedure (IGDA8 code) Institution code:
04 - University of Kansas Medical Center 05 -- University of Iowa Hospital 06 - Ds. John Sinkey, Toledo, Ohio
11 -- University of Cincinnati Hospital 19 - Cleveland C h i c 24 - St. Louis University 25 - Washington University Hospital 27 - University of Illiliais Hospital 28 - Sutter Genera.1 Hospital, Sacramento, California 39 - Callinnbus Childrens Hospital, CoAumbiis, Ohio 54 - Miami Valley Hczpital, Dayton, Ohio 56 - Alta Bates Hospital, Dayton, Ohio 62 - Silver Cross Hospital, Johiet, Illinois 64 - University of California Hospital, San Francisco, California 71 - Coluiiibia Presbyt~riau Hospital, New York, New York 73 - Strong Medical Center, Rochester, New York 74 - Sheltow Clinic, Los Amgeles, California 77 - University of Colorado Medical. Center, Denver, Colorado 81 - Menorah Medical Center, K a m a City, Missouri 92 - Childrens Hospital, Boston, lilassachnsetts
10 - Stanford LJBiversity Hospital
xxxxx.xx[*] Model-cakiilated dose to the thyroid (rad). The asterisk, when it k present, indicates that measured uptake i s incompatible with model assumptions. In such cases, the dose corresponds to the assumption that removal of iodine from the thyroid prior to the time of maximum burden occurs only by radioactive decay (refer to the discussion of the retention function A' I t ) ) .
2
by ORNL, a similar number of records had missing or erroneous birth dates, or in some cases, an age field that was inconsistent with other records for the same patient. The latter inconsistencies were attributed by DRH to an incorrect computer algorithm, and corrections were furnished by DRH staff. At the same time, the DRH staff provided missing sex data and a number of miscellaneous corrections to records in the file.
In dose computations performed at ORNL, the corrected age field was used rather than the computed interval between the date of birth and the date of administration.
In some cases, missing uptake data could reasonably be estimated from another record for the same patient. A recurring pattern in the file consisted of a pair of records €or a patient, indicating two administrations of 131X= The first record would be complete with respect to uptake data. The second record would portray a somewhat larger administration 1 to 5 days later, for a diagnostic scan, and would lack uptake data. At the request of DRH, such cases were identified, and the uptake data from the earlier record were copied to the later record for dose computation. Approxiniately 90 patients had records that fell into this pattern.
We have alluded to multiple records corresponding to the same administration. For example, the last three records for patient #190370 corresponded to a single administration of 7pCi on January 7, 1958; uptakes of 21%, 24%, and 25% were measured 5 , 6, and ?hours after administration, respectively. In situations of this kind, only the last record has been used to estimate the dose to the thyroid.
Other multiple records were apparently the result of redundant replication, and each was restored to a single record.
The file resulting from the corrections and revisions described above includes a 17th field, which gives the computed dose to the thyroid (rad) in each record for which the computation of dose is possible. We shall call this file "the revised file."
While ORNL will have no role in the epidemiological study that will be supported by the data in the revised file, we wish to make two observations about these data that we believe may bear upon the work.
First, the variability of the fractional uptake suggests the presence of subjects with abnormal thyroid conditions. The model that was derived for estimating the dose is based on euthyroid patients and may give biased estimates when it is applied to an abnormal population. The revised file presents dose numbers for all patients whose records contain sufficient data, whether the model may have been appropriately applied or not.
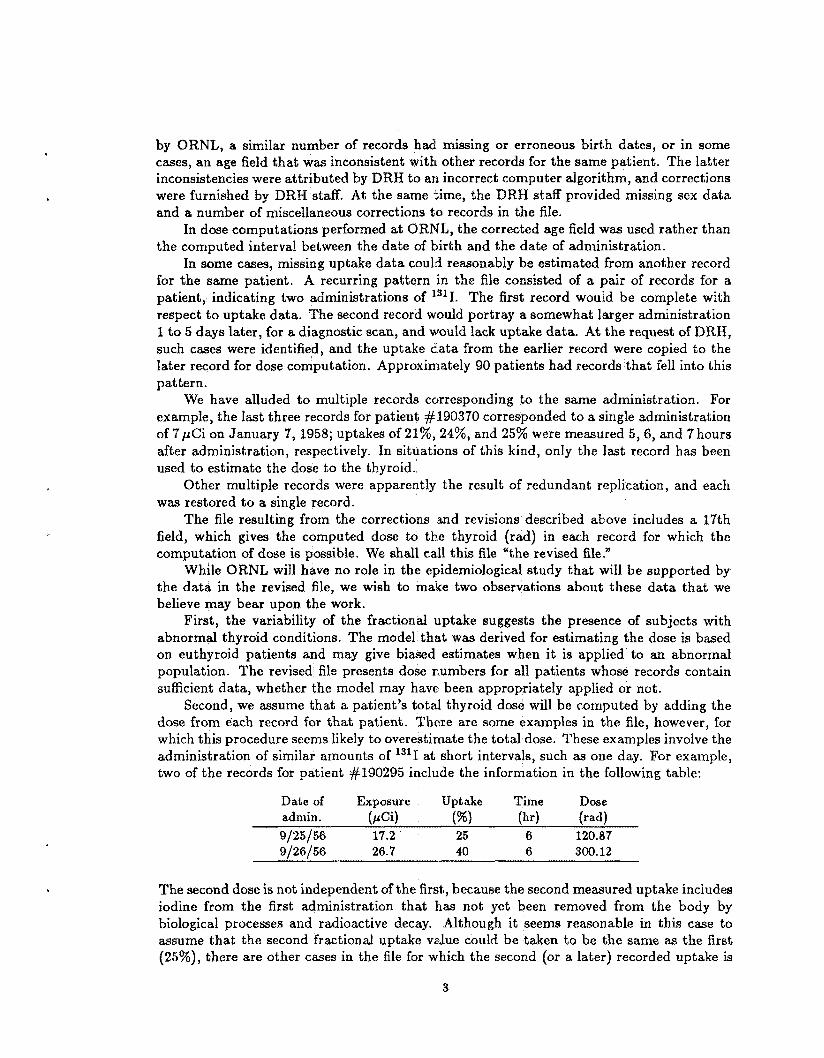
Second, we assume that a patient's total thyroid dose will be computed by adding the dose from each record for that patient. There are some examples in the file, however, for which this procedure seems likely to overestimate the total dose. These examples involve the administration of similar amounts of 1311 at short intervals, such as one day. For example, two of the records for patient Jf190295 include the information in the following table:
Date of Exposure Uptake Time Dose
9 / 25 /56 17.2 25 6 120.87 9/26/56 26.7 40 6 300.12
admin. (PCi) (%I (hr) (rad)
The second dose is not independent of the first, because the second measured uptake includes iodine from the first administration that has not yet been removed from the body by biological processes and radioactive decay. Although it seems reasonable in this case to assume that the second fractional uptake vdue could be taken to be the same as the first (25%), there are other cases in the file for which the second (or a later) recorded uptake is
3

less than the earlier one (e.g., the first two records for patient :/#O'E67). Thus a consistent policy for adjusting the uptake values does not immediately suggest itself. The investigators in the Diagnostic lS1I Study need to be aware of the existence of such effects and take them into account in using this data base.
DESCRIPTIO
The model that we have applied to the age, sex, m d uptake data in the revised file estimates absorbed dose (rad) to the thyroid resulting from a known fractional uptake by the thyroid at a specified time after a clinical administration of '''I. To an extent that we believe i s consistent with observations, the model distinguishes age differences md to a lesser degree, those related to sex. W e emphasize that the model i s based on data from etathyroid subjects; i t s elaboration t o abnormal thyroid conditions has n o t been ~ ~ ~ e r t Q ~ ~ ~ "
The mode! consists of two components, corresponding to the two factors in the right- hand side of the dose equation
b(t) = S(thyroid +-- thyroid) - A(t) (1)
where b(t) = absorbed dose rate (rad day-') to the thyroid at time t, S(thyroid +- thyroid) -= dosimetric ( L S - f ~ ~ t ~ ~ 7 ' (rad (pCi-day)--') €or 1311 in the thyroid, and A( t ) = activity burden (pCi) of 1311 in the thyroid at time t . In our model, S depends an age and sex, and A(t ) depends on age at the time of administration of the 1311.
The 1311 activity in the thyroid, A ( t ) , is based on a metabolic model of iodine in the body. Several levels of detail have been incorporated into existing models. Multicompart- mcwt models aim at providing mechanistic representations of iodine kinetics (e.g., Berman, 19726, but the numerous parameters of such models are not readily expresaed as fumtions of age. The International Commission OB Radiological Protection (ICRP, 1979) has adapted a model of Riggs (1952) for its purposes of rad.iation protection far occupationally exposed adults. The Riggs/llCRP model (Pig. la) consists of three compartments. The first is a "transfer compartment," into which the radioiodine is originally introduced and from which the iodine is removed with biological half-time 025 days; 78% i s excreted through the urinel and the remaining 30% i s available for uptake by the thyroid. Iodine i~ cleared from the thy- roid compartment with a half-time of 88 days into an organic iodine: pool, which lasee iodine through excretion and feedback to the transfer compartment of iodine from delhalogenatiori of thyroxine and triiodothyronine.
The transfer compartment has proved useful in avoiding overestimation of dose to the thyroid by short-lived radioiodines, which decay significantly before reaching the thyroid, and we wished to retain this feature in the model implicitly. The feedback pathway, om the other hand, makes little contribution to the time integral of activity in the thyroid for 1311. To support this assertion, we have performed calculations with the three-box model of Fig. Pa and a two-box caunterpa.r& that lacks the organic-iodine compartment (Fig. Ib). When PpCi of 1311 is introduced into the transfer compartment at time t - 0, the two models agree in the following respects:
gn Both model thyroids have their maximum activity between 1.2 and 1.3 days after ad-
8 Both maximum uptakes by the thyroid are 26% of the administered activity.
m For both models, the time integral of activity in the thyroid is 3.1 yci-days pea pCi
ministration.
taken into the body.
4

ORNL-DWG 85-13113 ORNL-OWG 85-13112
COMPARTMENT
OTHER ORGANS (Organic Iodine)
Figure la . The Riggs/ICRP metabolic model for iodine. Times in the boxes are biological removal half-times. The connecting arrows are labeled with the corresponding pathway frac- tions.
Figure lb. Two-box metabolic model for io- dine, which predicts, for 1311, the same time- integrated radioactivity in the thyroid as the three-box model of Fig. la.
For our purposes, the model of Fig. l b is essentially the functional equivalent of that of Fig. la and offers the advantage of fewer parameters.
But the formulation of the two-box model represented by Fig. l b was not yet ideal for application to the FDA DRH computer file. We needed to be able to specify directly the fractional uptake of the administered isotope by the thyroid. The coefficient 0.3 (in the presence of the other parametric values) gives a maximum uptake of 26% and thus corresponds roughly to the maximum fractional uptake. But some patients’ records con- tained measured uptakes only a t times that were unlikely to correspond to the maximum. A model that would accommodate such a pattern of data was needed. To construct one, we proceeded along the following lines of reasoning.
The retention function When the differential equations that describe the two-box model of Fig. l b are solved explicitly, the representation of the thyroid compartment has the form
A(t ) = K - (eXP(-Pd) - exP(-Pzt)) 9 (2)
where = Aib + A, (i = 1, 2) are effective decay-rate coefficients, Aib = (ln2)/Tib are biological decay-rate coefficients (the xb are biological removal half-times), and A, is the radiological decay-rate coefficient for the radioiodine of interest.
Please note: Throughout this discussion, we assume that A(t ) is normalized to the intake of 1pCi of radioactive iodine into the body. Consequently, in applications, A( t ) must be multiplied by the actual number of pCi administered. Note also that A(0) = 0, because the initial intake is in the transfer compartment.
We take K , AI, and A2 as unknown parameters and impose three constraints to deter- mine their values:
5

1. A( t ) is required to have its maximum at a specified time, t = tmm. Normally we will take t,= = 1 day, corresponding to the clinical assumption that maximum uptake oc(3iirs in approximately 24 hours. or 1311 we tested the sensitivity of the time integral of A(t) to the choice of t,,,, by varying ithis parameter over a range from 8.5 to 2days. The maximum deviation of the time integral of A(t ) from its reference vdue was 11%.
2. The function yb(t) = exp(-Xit) - exp(-Azt) is required t s have a specified %qqxwent" biological half-time, T", with respect to a given interval, tl 5 t L t 2 ( t l 1 tmm). We normdly set tl = t,, and t 2 = 15days, in accordance with the common experimen- tal practice of reporting a single clearance-rate parameter based on the first P5days' observations. We express this requirement by the equation
3. Finally, we require that at a specified time, %, the fractional uptake, u, of iodine ta the thyroid can he .zssigned: A(T) = u. The time T at which the fractional uptake is actually determined often does not coincide with tmax; for example, the file contains a number of observations at T = 6 hours.
Within the parameter range of interest in this work, the requirements 1-3 given above determine the parameters K, XI, and A2 M functions of t,,, t l , t 2 , T u , T, and ue The numerical calculation of K, X I , and A2 in a given case involves sollvin a nonlinear equation. We give the details of the procedure in Appendix A, and Appendix B lists a FORTRAN77 subroutine far carrying out the calculation.
0 1 2 3 4 5 6
8 9
I
Table 2. Age-Dependent Retention Pwameters for '''1 in the Thyroid
Rate cacf$lciexats
0.1324 0.1403 0.1328 0.1243. 0.1182 0.1 140 0.1 I08 0.1083 0.1062 0.1046
3.3691 3.2977 3.3654 3.4491 3.5089 3.5540 3.5891 3.6172 3.6403 3.6596
0,1032 0.1020 0.1010 0.0997 0.0988 0.0980 0.0973 0.0967 0.0962
3.6759 3.6WO 3.7021 3.7187 3.730% 3.7398 3.71684 5.7559 3.7626
Table 2 displays the rate coefficients p1 and p~ o€ Eq. 2 vs. age. The tabulation is based on the parameter values t p = tmaw = 1 day and t z = 15 days. The following example illustrates how the retention function corresponding to a particular uptake observation i s determined. Suppose that 25pCi of 1311 is administered to a ten-year-old male, and after 6hours it is determined that the thyroid has taken up 9%. Let us calculate the fractional retentiori function. From Table 2 we have the effective rate coeficients pl = 0.1032, p2 = 3,6759day-I, and we are given that for E = G hours = 0.25day,
K - (e~p(---0.1032 x 0.25) - exp(-3,6753 x 0.25)) = 0.09
6

so that K = 0.09/0.5756 = 0.1564. Since the maximum value occurs at t,, = lday, we may compute it as follows:
urn, = 0.1564 x (exp(-0.1032 x 1) - exp(-3.6759 x 1)) --7 0.1371
or 13.7% (3.4 pCi). For some combinations of input parameters, however, the formulation just described
and illustrated gives misleading results. Such an occurrence results from an estimate of the fractional uptake u at time T that predicts a maximum uptake = A(&=) that exceeds any amount that the thyroid could possibly take up by time tmax7 given the structural assumptions of the model and the values of the remaining input parameters. A necessary constraint may be expressed by the inequality
A(trnim) < exp(-&tmax) 7 ( 4 )
because the value exp(X,tmm) is an upper bound €or the fraction of the administered ra- dioactivity that survives radioactive decay and is available for uptake by the thyroid at time itmax. This upper bound is conservative, because some of the radioiodine would also be removed from the body by biological processes during the interval [0, tmax]. But the constraint of Eq. 4 is not built into the model as we have formulated it so far. Our remedy for physically impossible cases is to replace the retention function A(t) by A*(E), which is computed in the same way, but with T = t m , and u = urn, = exp(-Xrtma). This use of the conservative upper bound for insures that A* will not underestimate the uptake, given the model's structure and the other parameter values. But; the use of A* also has the advantage of avoiding dose estimates that are grossly in excess of what is physically possible. The choice, of course, is not consistent with the original input value of u.
We illustrate the handling of such exceptions with the case of a six-year-old who was given 20 pCi of 1311 and was reported to have taken up 41.4% after 2 hours = 0.083 day. For age six years, pl = 0.1108 and pz = 3.5891 day-l (Table 2), and we rue given
K . (exp(-O.1108 x 0.083) - exp(-3.5891 x 0.083)) = 0.414
so that K = 0.414/0.2485 = 1.666. This retention function predicts a maximum fractional uptake, at t,, = lday, of
urn= = 1.666 x (exp(-0.1108 x 1) - exp(-3.5891 x 1)) = 1.45
or 145%, which is impossible. We must conclude that the observation was taken, recorded, or transcribed incorrectly, or that the patient's uptake of the radioiodine was approach- ing its maximum somewhat earlier than the assumed 24 hours. Having no further in- formation about the patient or the procedure, we discard the observation of 41.4% after 2 hours and instead assume that u = u,, = exp(-Art) at t = fmM = lday. With A, = (ln2)/(8.04 days) = 0.0862 day-', this gives um, = 0.917 and
K . (exp(-0.1108 x 1) - exp(-3.5891 x 1)) = 0.917
so that K = 0.917/0.8675 = 1.057. As we nated earlier, the recomputed retention function A*(t) cannot be consistent with the reported 41.4% at 2 hours; instead, the value after 2 hours is
u = A*(0.084) = 1.057 x (exp(-0.1108 x 0.083) - exp(-3.5891 x 0.083))
= 0.263
7

or 26.3%. The interpretation of this d&dt retention function is that during the first 24 hours, radioiodine is lost from the body ody by radioactive decay, whereas after 24 hours it is removed by a combinartian of radioadctivc decay and biological processes. Thus, the default represents an upper bomd for retention curves having; their maximum vdues at t = 1 day anrd having the same vdues of the parameters t l t 2 , and T* .
Whenever the procedure that we have just illustrated h i d to be applied to a cme, the resulting dose estimate was marked with an terisk as it was written into the revised data file (Table 1). The incidence of such O ~ C F I P P B ~ C ~ B was confined to a small fraction of the records.
The biological half-time, T", of iodine in the thyroid has been estimated in numerous studies with different age groups and is m e of the parameters considered by Dunning and Schwarz (1981) in a review of literature for euthyroid patients. Dunroin estimated distributions of T" far each of several age groups ranging from ne Their mean value of 85 days for the adult i s similar t5 the 80-day value used by the TCRP ( lW9) . We will use a function that interpolates the mean values given by Dunning anti Schwarz (1981) as an age-dependent representation of "I"* (Fig. 2).
Thus, Eq. 2, together with constraints 1-3 described previously, defines an age-specific metabolic model of iodine retention in the thyroid. The 111~dg/l can he tied directly to population data through its biological half-time parameter T' and to specific individual clinical data through the uptake parameters T and u, and it depends only marginally on a parameter (tmax) to which we have less direct access.
The dosimetric §-factor The remaining factar in the dose-rate equation (Eg. I ) is the S-factor, which depends on the mass of the thyroid, which in turn depends strongly on age and to a much lesser extent an sex. We outline the considerations used in obtaining the S-factora for the model.
We express the S-factor, which represents absorbed dose rate to (taxget) organ Y per unit radioactivity of the radionuclide of interest in (source) organ X , in the farm
where
Q = mean number of radiations of type i per nuclear transformation = mean energy per radiation of &ype i (MeV)
@i(Y c X) = specific absorbed fraction for radiation type i (g-') k = 2.13 (rad-g)/(~Ci-hr-MeVb.
In the present context, X = Y = thyroid. The absorbed dose rate from non-penetrating radiation as a function of thyroid mass kfth is
2.13 E; a;Ei Snp(thyroid 5- thyroid) =
Mth 9
because 4i, I- 1/M& for such radiations. For 1311, 0.191 MeV of non-penetrating radiation i s emitted per nuclear transformatian (ICRP, 1983). Thus,
2-13 x 0.191 0.406 Snp (thyroid +- thyroid) = II -- ..- robd/pCi-hr.
N t h Mtb
8

ORNL-DWG 85-13114
--------
Points a ipdicate mean values Dashed lines span age groups on which averages are based
5 10 15 20 AGE (years)
Figure 2. Biological half-time of iodine in the thyroid as a function of age, based on estimates of Dunning and Schwarz (1981).
Monte Carlo calculations of the specific absorbed fraction for photons of energy ranging from 0.01 to 4.0 MeV have been performed for thyroid mass values from 1.29 to 19.6 g (Table 3). An S-factor for the penetrating radiations of 1311 was calculated for each specific thyroid mass (Table 4) and fitted to a power function of thyroid mass. The resulting expression is
0.666 &(thyroid t thyroid) = 1.014 x lO-’Mth- . This function fits the data with reasonable accuracy. The total S-factor is the sum of the components for non-penetrating and penetrating radiations:
f 1.014 x 10-2bfbh-o.6GB . 0.406 S(thyroid t thyroid) = -
Mth
It remains for us to express the thyroid mass, Mth, as a function of age and sex. Kay et al. (1966) analyzed the masses at autopsy of thyroids of 537 subjects of both sexes and of ages ranging from pre-natal to 19 years (all but eight were under 15 years of age). Kay
9

photon energy .̂ l.._.ll
@(thyroid +- thyroid) kg-l
( k e v 1.29 g 1.78 3.45 7.93 12.4 19.6
10 15 20 30 50 100 200 500
1,000 2,000 4,000
533. 280. 145. 49.0 15.4 8.73 9.42
9.89 8.26 6.83
10.2
390. 209. 110. 37.0 11.7 6.98 7.72 8.78 8.18 6.86 5.46
215. 123. 67.6 23.9 7.68 4.58 5.09 5.71 5.45 4.57 3.38
100. 62.7 36.4 13.7 4.46 2.62 2.88 3.22 3.02 2.56 2,Q4
66.4 43.5 26.0 10.2 3.43 2.03 2-20 2,43 2.29 1.90 1.49
42.9 29.3 18.1 7.41 2.42 1.44 1.55 1.66 1.54 1.31 1.05
Table 4. Iodine-131 S-Factor as a ction of Thyroid Mass
S (rad/p@i-hr)
Thyroid mass (g) Non-penetrating Penetrating Total
1.29 1.78 3.45 7.93 12*4 19.6
0.314 0.228 0.118 0.0512 0.0327 0.0207
8.32 x 10-3 0.323 6.95 x 10-3 0.235
2.57 x lo-’ 0.0538
1.35 x IO-’ 0.0221
4.56 x 10-3 0.123
1.95 x 10-3 0.0347
et al. fitted the data with the regression line
Mth = 1.48 + 8.64%~ f 1.94 g (7)
where a = age in years and 1.94 g is the residual standard error. Over the range of ages considered, the difference in thyroid m a ~ s between sexes was not found to be significant. To construct our function, we have used the regression line of Eq. (7) for both sexes and ages ranging from newborn to 15 years. For adults, we have adopted the average values 1 7 . 5 f 6 . 5 g (male) and 14.9zk6.7g (female) from a study of New York City cases (Mochizuki et al., 1963; ICRP, 1975). The articulation of the two data sets was accomplished by interpolating linearly, for each sex, between the value of Mth given by Eq. 7 for a = 15 years and the appropriate adult value at a = 25 years. After 25 years, the functions are considered to be constant (Fig. 3). This scheme furnishes, for each age and sex, a value of Mth, which is substituted into Eq. 6 to obtain the S-factor.
Table 5 shows S-factors for males and females and for ages newborn to 25 years. We illustrate the dose computation procedure by referring to an earlier example of a ten-year- old male who was given 25 pCi of 1311 and found to have taken up 9% to the thyroid after 6 hoiirs. The fractional retention function WM found to be
A(t ) = 0.1564 x (exp(--0.1032t) - exp(-3.67532)).
10

ORNL-DWG 85-13115
Mean for All Adult Males (Mochizuki et a i , 1963)
I._._. .-.-.-.= ...-.-.-.-.-.-.-.- ----------
I( 20 - + InterpOlatPd Values +
- m 4 5
- --- ....I----. Mean for All Adult Females
(Mochizuki et al, 1963)
t + Regression Line of Kay el al (1966) +
0
> 1 k
Means for Adult Age Groups
Male _._. _. -. _. Female -------
0. I 1 I 1
AGE (years) 0 10 20 30 40
Figure 3. Mass of the thyroid as a function of age.
Table 5. Sex- and Age-Dependent S-Factors for lSxI in the Thyroid
S-factors (rad /pCi-day )
Age (years) Male Female
0 1 2 3 4 5 6 7 8 9 10 11 12
6.7709 4.7259 3.6332 2.9529 2.4883 2.1509 1.8946 1.6933 1.5309 1.3972 1.2852 1.1899 1.1080
6.7709 4.7259 3.6332 2.9529 2.4883 2.1509 1.8946 1.6933 1.5309 1.3972 1.2852 1.1899 1.1080
I
S-far: tors (rad/pCi-day)
13 14 15 16 17 18 19 20 21 22 23 24
2 25
1.0367 0.9740 0.9187 0.8706 0.8273 0.7882 0.7527 0.7203 0.6906 0.6632 0.6380 0.6146 0.5929
1.0366 0.9740 0.9187 0.8898 0.8627 0.8372 0.8132 0.7906 0.7692 0.7490 0.7298 0.7115 0.6942
Integration gives
0.1564 0.1554 0.1032 3.6759
A(t) dt = - - - - - 1.473 pCi-days per pCi intake.
(The infinite limit of integration, in the case of 1311, gives the same result as an integration time of 50, 70, or 100 years.) The S-factors in Table 5 are in units of rad/pCi-day. Hence the dose to this patient’s thyroid is estimated to be
D = 25 pCi x 1.285 rad/pCi-day x 1.473 pCi-day/pCi = 47.3 rad to the thyroid.
11

Calculation with the model Table 6 gives the results of a calculation performed with this composite d Dose to the thyroid (rad/pCi) ia tabulated by age and sex. For this tabulati maximum uptake waa based on the age-specific mean values from the r and Schwarz (1981). F'm comparison, corresponding estimates of lS1I dos Dunning and Schwarn (19811, Johnson (1981), ICRP (Eekerman et -, 1981), Medical In- ternal Radiation Dosimetry (MIRD) Committee (19751, and the U.K. National Radiological Protection Board (NRPB, 1983) are shown alongside.
3.35 8.5
2.29
Table 6, Iadine-lZ$l. Dose to the Thyroid
n d e l 1981 Schware, 1981 methodologya MIRE), 1975 NRPB, 1983b Age Male Female Male Female (Both sexes) (Both sexes) (Both sexes) (Both sexes)
Age and Sex (sad pCi-') Present Johnson, Dunnhg and ICRP
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
25.1 14.4 11.4 10.0 9.0 8.2 7.5 7.0 6.5 6.1 5.9 5-6 4.8 4.1 3.5 2.9 2.5 2.0 1.6 1.5 1.5 1.4 1.3 1.3 1.2 1.2
25.1 14.4 11.4 10.0 9.0 8.2 7.5 7.0 6.5 6.1 5.9 5.6 4.8 4.1 3.5 2.9 2.5 2.1 1.7 1.7 1.6 1.6 1.5 1.5 1.4 1.4
15.1 10.8 7.95
5.34
3.35
2.29
1.38
15.1 25.3
14.2' 10.8 7.95
5.34
1.66 1.4 8
13.7
4.4
38 1.6
aEckerman et al. (1981). bStather et al. (1983). '0.5-2 years. dBa3ed on maximum uptake to the thyroid of 25% and thyroid mass 20 g.
hi general, the agreement among these estimates of dose per unit intake is good, but the comparison with the factors of Johnson (1981), which for the younger age groups are systematically less than our factors, deserves further comment. In the caqe of our model, the fractional uptake and the biological half-time for iodine in the thyroid are considered
12

to be observables and are furnished from cPinical or experimental data. In the model of Johnson, however, these quantities are not specified directly but are defined implicitly by the model's kinetics. We have estimated their values by solving the differentid equations of the model after following the calibration procedure set forth by Johnson (1981). The following table compares the values of the fractional uptake and the biological half-time with the corresponding parameters from Dunning and Schwarz (1981) for newborn infants and adults:
For newborns, the Johnson model simulates a much lower fractional uptake than the Dun- ning and Schwarz value that was used in our model. This disparity in uptake fractions explains most of the difference in the dose conversion factors; because of the 8-day half-life of 1311, the much slower removal simulated by the Johnson model's kinetics cannot offset the gap in uptakes. In the case of adults, however, the fractional uptakes are reversed, but the difference between them is less. For longer-lived radioiodines ("'1 and 1291, the contrast in the apparent biological half-times between the two models becomes significant, and the dose conversion factors calculated with the Johnson model for the youngest age groups are marginally larger than the corresponding factors calculated with our model.
The discrepancies in the two models' predictions lie almost entirely in their metabolic representations; their S-factors for corresponding age groups differ by at most a few percent.
SENSITIVITY OF THE DQSE MODEL TO UNCERTAINTIES IN ITS PARAMETERS
We have tested the sensitivity of the dose estimate to uncertainties in two of the model parameters by replacing those parameters with probability distributions and estimating the corresponding distribution of the dose. The parameters are the biological half-time of iodine in the thyroid (2'') and the mass of the thyroid (Mth). The calculations, which were performed by pseudorandom sampling from the input probability distributions, were carried out for each of the four age groups considered by Dunning and Schwarz (1981):
0 newborn e children 0.5-2 years 0 adolescents 6-16 years 0 adults 2 18years.
For each age group, the corresponding estimate b y Dunning and Schwarz of the mean value of fractional uptake by the thyroid was used. Substitution of different values ,of fractional uptake-such as clinically determined uptakes-would, of course, lead to different distributions of dose, but the distributions we have computed should give a reasonable impression of variability in the dose estimates for fixed fractional uptake.
Other fixed parameters and their values that were used in the simulations were tmax (1 day), tl (1 day), t 2 (15 days) , and T (1 day).
13

The biological half-time of iodine in the thyroid, T’, md the mass of the thyroid, h’ftth,
were treated, for each age group, as independent random variables OA the assumption that independence would represent an extreme case. The distribution of T* was assumed to be lognormal with values of the logarithmic mean and standard deviation, p and 5 , taken from Dunning and Schwarz (1981). For each nonadult group, Mth was assumed lognormally distributed with logarithmic parameters p and 1~ computed from the mean and standard deviation (a and p ) given by Kay et a:. (1966). Sexes were consolidated in accordance with the conclusion of May et al. that in the nonadult groups the difference in thyroid mass between males and females is not statistically significant. The equations are
These equations were obtained by solving the inverse equations given by Aitchison and Brown (1969; Sect. 2.3). For adults, we followed a similar procedure, but with differentiation by sex, using lognormal distributions with parameters based an autopsies performed in New York City for individuals aged 20 to 30years. These autopsy data were originally reported by Mochizuki et al. (1963) and were reprinted in the Reference Man Report (ICRP, 1975).
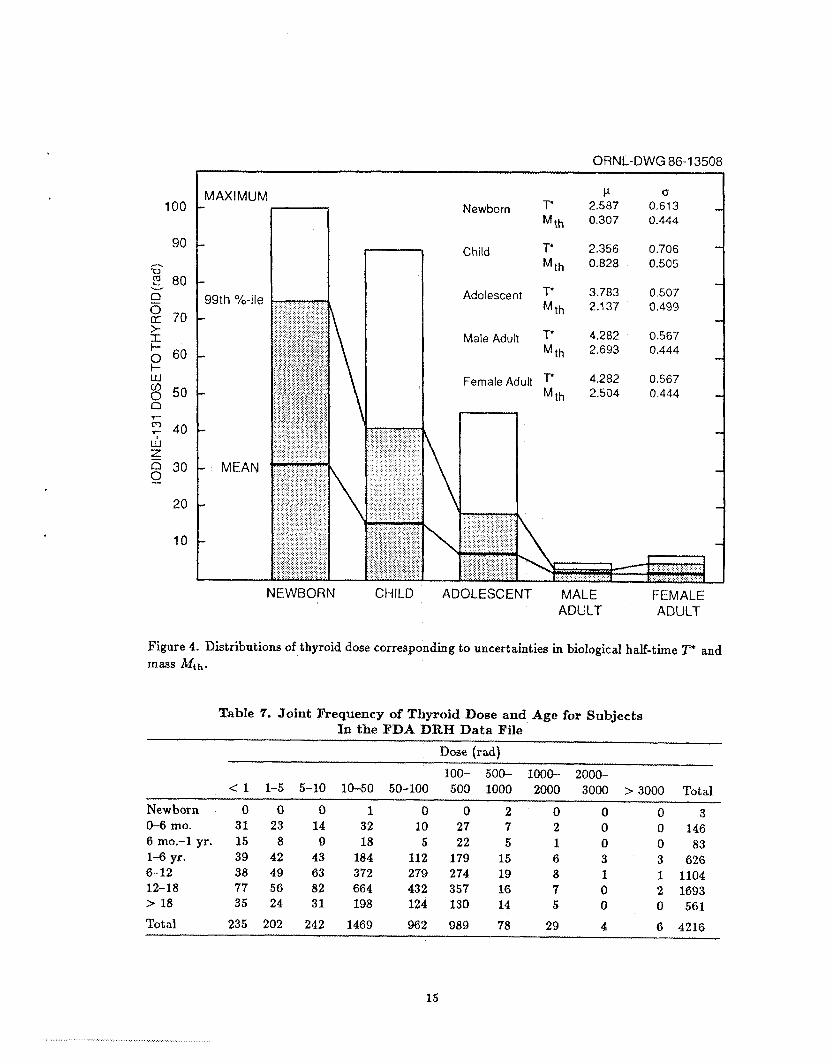
Figure 4 gives an indication of the distribution of dose for each of the age groups. In absolute t e r m , the variability shown in Fig. 4 is large for the newborn and children’s groups (99th percentile = 75 and 41 rad, respectively) and progressively smaller with increasing age. But in relative terms, the variability changes little with age: the coefficients of variation (standard deviation divided by the mean) for all of these groups cluster closely about the value 0.5.
Note: The uncertainty analysis described in this section represents a departure from the procedure reported by Kiliough and Eckerman (1985). The present analysis i s based on variances p2 in thyroid mass that are specific to age, whereas for the previous work it ww assumed that all sub-adult groups had a common variance. We are indebted to F.O. Hoffman, ORNL Environmental Sciences Division, for suggesting that we perform the analysis with thyroid mass variance specific to each age group.
DISTRIBUTION OF DOSE A ONG PATIENTS IN THE FDA DR DATA FILE
A detailed accounting of the information in the FDA DRM file is beyond the scope of this report. For the general reader, however, it may be of interest to see how dose as estimated by the model is distributed within the population of patients represented by the file. Table 7 shows the frequency (i.e., number of patients) within each of seven age groups and 10 levels of radiation dose to the thyroid from administered l3’1[. For inclusion in Table 7, each patient’s total dose was computed by adding the result of each administration. Patients for whom no dose could be computed were represented by zero and were tallied in the column for < 1 rad.
In a few cases, considerable intervals of time elapsed between administrations to a given patient, and there may he a few individuals whose experience spanned more than one age group. In all cases, the age corresponding to the most recent administration was arbitrarily assigned to the individual for the purposes of the table. Such situations are tao rare to have an important effect on the tabulated frequencies.
14
100
90
2 80 0 2 70 >. I I-
A
-0
v
p 60 w $ 50 n
ORNL-DWG 86-1 3508 1
NEWBORN CHILD
\ \
Newborn T" Mth
Child T' M t h
Adolescent T* M t h
Male Adult T* Mth
Female Adult M t h
P 2.587 0.307
2.356 0.828
3.783 2.1 37
4.282 2.693
4.282 2.504
0 0.613 - 0.444
0.706 0.505
0.507 0.499
0.567 0.444
0.567 0.444 -
- - -
-
- I
-
-
ADOLESCENT MALE FEMALE ADULT ADULT
Figure 4. Distributions of thyroid dose corresponding to uncertainties in biological half-time T* and mass Mth.
Table 7. Joint Frequency of Thyroid Dose and Age for Subjects In the FDA DRH Data File
Dose (rad)
< 1 1-5 5-10 10-50 50-100 500 1000 2000 3000 > 3000 Total 100- 500- 1000- 2000-
Newborn 0 0 0 1 0 0 2 0 0 0 3 0 146 0-6 mo. 31 23 14 32 10 27 7 2 0
9 18 5 22 5 1 0 o a3 6 mo.-1 yr. 15 8 1-6 yr. 39 42 43 18.1 112 179 15 6 3 3 626 6-12 38 49 63 372 279 274 19 8 1 1 1104 12-18 77 56 82 664 432 357 16 7 0 2 1693 > 18 35 24 31 198 124 130 14 5 0 0 561
Total 235 202 242 1469 962 989 7a 29 4 6 4216
15
Readers are reminded once again that the doses were estimated in a way appropriate for subjects with normal thyroid function, and the incidence of a.bnormal. thyroid function in the population under study could bias the frequencies presented in Table 7.
We have described the derivation and application of an age- and sex-specific model of 1311 dosimetry for the thyroid. The model was specially formulated for the data base that will support the Diagnostic 13’1 Study conducted by L)XH; in particular, the model accommodates vdues of fractional uptake to the thymid that were determined at various times after administration, including but not restricted to the time of maximum thyroid burden. The model has been applied to all records of the data file for which the uptake and retention data are complete or can be estimated from other records for the same patient, and each computed thyroid dose has been incorporated into the appropriate record.
Tests of sensitivity of the model’s predictions to uncertainties in the biological half- time of iodine in the thyroid and the mass of the organ were performed. These tests showed large absolute variability in the dose for newborns and children, but relative measures of dispersion, such as the coefficient of variation, differ little among age groups. Inasrnuch as there was no clinical determination of thyroid mass nor of biological half-time of iodine in the thyroid for the patients in this study, our estimates of variability in dose due to uncertainty about these variables could be of interest to the investigators in the Diagnostic 1311 Study and also to those who make generic applications of the madel.
ACKNOWLEDGMENT
We wish to acknowledge the aid and suggestions of Wah Lee and Peggy M. Hamilton, Division of Life Sciences, Center for Devices and Radiological Health, FDA, during the course of this work. We also express our thanks to Dr. S.S. Yaniv of the U S . Nuclear Regulatory Commission, Office of Nuclear Regulatory Research, for his technical. advice and support throughout this work.
REFERENCES
Aitchisoa, J., and J .A.C. Brown. 1969. The Lognormal Distribution, Cambridge University
Berman, M. 1972. “Iodine Kinetics,” Chapter 11 in: The Thyroid and Biogenic Amines (J.E. Rall and I.J. Kopin, editors), Vsl. I of Methods in Investigative Endocrinology (S.A. Berson, series editor). North-Hollmd Publishing Company.
Cristy, M., and K.F. Eckerman. Specific Absorbed Fractions of Energy a t Various Ages from Internal Photon Sources. ORNL/TM-8381 Vol. 1 - Vol. 6 (in preparation).
Dunning, D.E., Jr., and G. Schwarz. 1981. “Variability of Human Thyroid Characteristics and Estimates of Dose from Ingested 13’I.” Health Phys. 40(5): 661-675.
Eckerman, K.F., M.R. Ford, and S.B. Watson. 1981. Internal Dosimetry Data and Methods of ICRP-Part 2, Vol. 1: Committed Dose Equivalent and Secondary Limits, NUREG/ CR-1962 Volume 1, ORNL/NUrtEG/TM-433/VI.
Press.
16

Forsythe, G.E., M.A. Malcolm, and C.B. Moler. 1977. Computer Methods for Mathematical Computations. Englewood Cliffs, New Jersey: Prentice-Hall.
International Cornmission on Radiological Protection. 1983. Radionuclide !lIamforma- tions-Energy and Intensity of Emissions, ICRP Publication 38. Oxford: Pergamon Press.
International Commission on Radiological Protection. 1979. Limits for Intakes of Radionu- clides by Workers, ICRP PubIication 30 Part 1, Ann. ICRP 2(3/4): 88-93.
International Commission on Radiological Protection. 1975. Report of the Task Group OR
Reference Man, ICRP Publication 23. Oxford: Pergamon Press.
Johnson, J.R. 1981. “Radioiodine Dosimetry.” J . Radioanal. Chern. 65( 1-2): 223-238.
Kay, C., S. Abrahams, and P. McClain. 1966. “The Weight of Normal Thyroid Glands in Children,” Arch. Path. 82: 349-352.
Killough, G.G., and K.F. Eckerman. 1986. “An Age- and Sex-Dependent Model for Es- timating Dose to a Normal Thyroid.” Proc. Fourth International Radiopharmaceutical Dosimetry Symposium, Oak Ridge, Tennessee, November 5-8, 1985 (in press).
Medical Internal Radiation Dosimetry (MIRD) Committee. 1975. uSummary of Current Radiation Dose Estimates to Humans from 12’1, ”‘1, 12’1, 13*1, ‘”1, and 1321 as Sodium Iodide,” Dose Estimate Report No. 5 , J . Nucl. Med. 16(9): 857-860.
Mochizuki, Y., R. Mowafy, and B. Pasternaek. 1963. “Weights of Human Thyroids in New York City,” Health Pbys. 9: 1299-1301. Data reproduced in ICRP Publication 23 (1975), p. 198.
Riggs, D.S. 1952. “Quantitative Aspects of Iodine Metabolism in Man,’’ Pharmacol. Rev.
Stather, J.W., J.R. Greenhalgh, and N. Adam. 1983. ”The Metabolism of Iodine in Children
4: 284-370.
and Adults,” NRPB Radio]. Prot. Bull. No. 54 [ISSN 0308-4272).
17

Appendix A COMPUTATIONAL PROCEDURE FQR THE THYROID
UPTAKE AND RET NTION FU
This appendix gives details of the determination of the fractional uptake and retention function for '''1 in the thyroid given by Eq. 2. The bask for the determination of the parameters p1, p2, and K i s three constraints, which we recapitulate:
First constraint The fraction A(t ) defined in Eq. 2 must take its maximum value at a specified time, t I= t,,,.
This constraint requires that the derivative of A(T) vanish at t = tmm:
__ d A ~ -K(l l le-- iJlfmax I p2e-Pztrn=) = 0 dt
from which we obtain - PI = e(Fl-iJz)LaT
P2
We introduce the following transformation of 112) ++ ( r , s): r = M / P 2
9 = p2 - p1 (0 L Pl < P2)
with inverse p1 = rs/ (I - r)
p2 = s/(f - r ) (0 5 r < 1, 9 > 0). Using &. A l , we may express s explicitly in terms of r :
This relationship will enable us to eliminate s and obtain a single equation in P.
Second con st raint The biological retention function
9 -- -tmax-l In r I
qb(t) = exr tA( t ) x K(e-'lt - e-'''t)
is to have a specified biological half-time, T ' , with respect to a given interval t l 5 t 5 t 2 , where t l 2 t,,, in the sense that the equation
must be satisfied. The function q b ( t ) , through A1 and A2 and the transformation of Eq. A2, depends on
the paranieters r and s; the latter parameter can be eliminated by Eq. A4, leaving q as a function of t with parameter r . The explicit dependence can be shown to be
qb(t; r) = Kr[r/ ( l -r ) l ( ' / t~ax)~'r~( l - r'/'ma*) . (A71 When Eq. A7 is substituted into Eq. A6, the result is a nonlinear equation in the variable P, which can be solved numerically to obtain the solution P = r*. Then from Eqs. A3 and A4, we may compute
s* = -tmax-l In r*
A 1 = p 1 - A, = r*s*/(I - r * ) - A, A2 = 112 - A, = s*/(1 - r*) - A,
(AB)
and thus the ratio q b ( t ) / K (Eq. A5) is determined.
18

Third constraint For a specified time T and fractional uptake u by the thyroid, we must have
A(T) = u if A(tmax) S exp(-A,t,,).
In the event that A(tmax) > exp(-&tm,), we substitute the function A*(t), which is computed by the requirement
In case the condition of Eq. A9 holds, the determination of the constant K is as follows:
Otherwise
Summary of the computational procedure Substitute Eq. A7 into Eq. A6 and solve for r = t*. Then use Eq. A8 to calculate p1 and p2. Finally, obtain K from %. A l l or Eq. A12, according to whether or not the inequality
e-alflnu - e-X2tm.x
,-hT - c-X2T U * 5 e--
is satisfied.

Appendix B COMPUTER I
The FORTRAN77 subroutine IRET (Iodine REYl'entioxP) goes a bit beyond its name and computes integrated activity and dose, ia9 well as returning the rate constants XI and Xz and the coefficient la'. It is provided to assist the reader who needs to examine the details of the calculation and should be studied primarily in connection with Appendix A. Subroutine IRET invokes the nonlinear equation solver ZEROIN (or more precisely, a double-precision version of it), which was taken from Forsythe et al. (1977; p- 164ff). Other equation solvers might be substituted, but those requiring the evaluation of one or more derivatives will demand additional effort on the part of the user, because no code for calculating derivatives is
C C C C C C C 6 C e C C c c c C C C C e C C C c C
C C c
included in the listings that follow.
SUBROUTINE IRET(LMR,TMM,TCAP,U,T1.T2,AG~,SEX, $ AWIGL, DOSE e K, LMI , LM2)
ESTIMTES PARAMETERS OF A THYROID-IODINE RETENTION FUNCTION OF THE FORM
WHERE LMR = RADIOLOGICAL DECAY CONSTANT (l/DAY) FOR THE PARTICWLAR ISOTOPE OF IODINE, AND K , LMI, AND LM2 ARE: THE ~ ~ ~ K ~ Q W ~ ~ PARAMETERS. THE CRITERIA FOR THEIR DETERMINATION ARE:
(1) THE MAXIMUM VALUE OCCURS AT A SPECIFIED TIME, (2) THE VALUE AT A SPECIFIED TIME, TCAP, IS A GIVEN NUMBER, U. (3) THE APPAENT BIOLOGICAL HALF-TIME IN THE RANGE (TI,T2),
TMAX > 0 .
WHERE TMAX <= Ti < T2, IS A GIVEN VALUE TSTAR.
INPUT PARAMETERS: LMR (l/DAY) , TMAX, TCU (DAYS),
Ti, T2 (DAYS), AGE (YEARS), SEX (l=M, 2=F)
DOSE (RAD), K (MICROCURIE-DAYS) LMl, LM2 (l/DAY)
u (FRACTION) I
RETURNED VALUES: AWIGL (MICROCURIE-DAYS PER MICROCURIE INTAKE),
IMPLICIT REiU*8 (A-H, 0-Z) , INTEGER (I-N)
INTEGER SEX EXTERNAL FCN DIMENSION X(2) ,F(2) ,WA(13) COMMON CVAR(5) QBYA(T ,Xi ,X2)=DEXP (- (XI+LMR) *T) -DE=(- (X2+LMR) *T)
REAL*8 K,LMR,LMI,LMZ,MTH
cawuw. APPARENT BIOLOGICAL HALF TI^ OF IODINE IN THE THYROID AS A FUNCTION OF THE AGE VALUE THAT WAS JUST READ IN. THE PIECEWISE LINEAR
20

C FUNCTION EVALUATED BELOW IS BASED ON THE REVIEW OF DUNNING & SCWARZ. IF (AGE .GE. OD0 .AND. AGE .LT. 1.25DO) THEN
ELSEIF (AGE .GE. 1.25DO .AND. AGE .LT. 13DO) THEN
ELSEIF (AGE .GE. 13DO .AND. AGE .LT. 18DO) THEN
ELSE
ENDIF
TSTAR=16DO-2.4DO*AGE
TSTAR=8.26D0+3.80DO*AGE
TSTAR=-SDO+SDO*AGE
TSTAR==85DO
C SOLVE THE EQUATION§ FOR LM1, LM2, AND A FOR THE METABOLIC MODEL C C MOVE VALUES OF DUMMY PARAMETERS TO COMMON AREA TO MAKE THEM AVAILABLE C TO FCN
CVAR ( 1 =LMR CVAR (2) -TMAX CVAR (3)=Tl CVAR (4)=T2 CVAR(5) -TSTAR AR-. OOlDO BR= .99W TOLslD-6
C INVOKE DOUBLE-PRECISION VERSION OF ZEROIN (FORSYTHE, C 1977) TO SOLVE EQ. A6 FOR R, WERE THE DEPENDENCE OF C BY EQ. AS.
RwZEROIN (AR ,BR, FCN , TOL)
LMl-R*S/ (IDO-R) -LMR LM2=S/ (1DO-R) -LMR K=U/QBYA(TCAP , LM1, LM2)
s=-DLOG (R) /TMAX
MALCOLM, AND MOLER, qB(T) ON R IS GIVEN
C EVALUATE THE INTEGRAL OF THE THYROID BURDEN (Q) FROM 0 TO 50 YEARS AYIGL=K* ((lDO-DEXP(-(LMI+LMR) *1825O.D0) )/(LMl+LMR)
$ -(lDO-DEXP(-(LM2+LMR)*18250.D0))/(LM2+LMR)) C COMPUTE THE S-FACTOR (REM/MICROCURIE-DAY) FOR THE GIVEN AGE AND SEX
IF (AGE .GE. OD0 .AND. AGE .LE. 15M) THEN
ELSEIF (AGE .GT. 15D0 .AND. AGE .LE. 25DO) THEN MTH=l.48D0+0.648DO*AGE
IF (SEX .EQ. 1) THEN
ELSE
ENDIF
IF (SEX .EQ. 1) THEN
ELSE
ENDIF
MTH=1.75D0+0.63DO*AGE
MTH=5.65D0+0.37DO*AGE
ELSE
MTH=1?.5DO
MTH-14.9DO
ENDIF C MTH = AGE- AND SEX-DEPENDENT MASS C THIS APPROACH USES THE REGRESSION C KAY ET AI.. (1966) FOR BOTH SEXES,
OF THE THYROID IN GRAMS CURVE MTH==l.48+.648*AGE FROM AND FROM 15 TO 25 YEARS EXTRAPOLATES
21

C LINEARLY TO OBTAIN T W VALUES 17.6 (MALE) AND 14.9 C FROM NEW YORK CITY DATA C PRESENTED IN REFERENCE MAN (ORIGXNfiLY FROM MOCHIZUKI ET AL., 1983).
C THIS S-FACTOR IS SPECIFIC TO IODINE-131 SFACT-(4.0598n-i/MTH+I.014n-P*MTH*s(-0.6~~~0))~24.DO
DOSE=SFACT*AWICZ RETURN END
FUNCTION IFCN(R)
REAL*€$ LMR,LBI,LB2 LOGICAL FIRST COMMON LMR,TMAX,TI,TZ,TSTAR DATA FIRST/. TRUE. / qB(T)=DEXP (R/ (IDQ-R) *T/TMAX*RLR) *DEXP (LMR*T)
IMPLICIT REAL*$ (A-H,O-Z) , INTEGER (I-N)
$ * (IDO-DEXP (T/TMAX*DLR) 1 c
10
IF (.NOT. FIRST) GOTO 10 FIRST-.FALSE. DL24LOG (2. DO)
CONTINUE DER=DLOG (R) FCN-QB (T2) -QB (TI) *DEXP (-DLZ/TSTAR* (T2-Tl)) RETURN END
22

Appendix C ADDENDU : DOSE CQNVERSION FACTORS
FOR QTHER RADIOIODINES
Age K A 1 A2
0 5.268055(-1) 4.515202(-2) 1.920236 1 4.652511(-1) 5.325276(-2) 1.818654 2 4.445201(-1) 4.555638(-2) 1.914753 3 4.430334(-1) 3.664530(-2) 2.048413 4 4.449618(-1) 3.064626(-2) 2.157817 5 4.487747(-1) 2.633288(-2) 2.250343 6 4.537359(-1) 2.308210(-2) 2.330465 7 4.594484(-1) 2.054477(-2) 2.401078 8 4.656786(-1) 1.8508981-2) 2.464190 9 4.722818(-1) 1.684042(-2) 2.521193
The foregoing portions of this report describe the development of dosimetric information for the Diagnostic l3l1 study conducted by the National Center for Devices and Radiological Health (DRH) and represents a final report for that work. This appendix discusses work that we have performed recently to extend the method to radioxtive isotopes of iodine other than mass number 131. This recent work incorporates certain departures from the method employed for the DRH study, but the resulting doses to the thyroid from 1311 are for all practical purposes the same; hence there is no reason to revise any of the dose estimates that were written into the DRH data file. The following subsections explain the adjustments that were made in order to calculate age- and sex-dependent dose conversion factors (rad pCi-l) for other radioiodines. Dose conversion factors for mast radioactive isotopes of iodine are tabulated (Table C1) as well as the coefficients and parameters of the model (Tables C2 and C3).
Age K A 1 A2
10 4.791605(-1) 1.544690(-2) 2.573194 11 4.862500(-1) 1.426617(-2) 2.620971 12 4.437564(-1) 1.325277(-2) 2.665159 13 4.011307(-1) 1.188835(-2) 2.730168 14 3.591805(-1) 1.096815(-2) 2.778261 15 3.175215(-1) 1.018005(-2) 2.822688 16 2.760936(-1) 9.498037(-3) 2.863931 17 2.348510(--1) 8.900370(-3) 2.902521
218 1.937611(-1) 8.374135(-3) 2.938654
The Retention Function The principal change of approach in deriving the retention function is that we now postulate the time, t,,, at which the biological retention function
takes its maximum value (the earlier method considered the maximum of the function A(t) = e-’rtqb(t>). And we have adopted tmaw = 2 days as being typical of the normal thyroid (Bell, Davidson, and Scarborough, 1968). One may obtain the revised calculation from Appendix A by putting A, = 0 and making the replacements pi t- &? i = 1, 2, and A( ) t- qb( ) in Eqs. A1 through A12.
Table C2 lists the computed quantities K, AI) and A2 for newborn and through age 18 years; the values for adults are the same as those for 18 years. The uptake fraction, u, and biological half-time, T* , are taken from the review of Dunning and Scfiwarz (1981); T* vs. age is plotted in Fig. 2, and uptake vs. age i s shown in Fig. C1.
23

N rp
Table C1. Dose t o the Thyroid (rad psCi-') for Various Radioiodine Isotopes
Male Age l z r ] 1221 1231 1241 lZ.51 1261 1281 1291 1301 1311 1321 1331 1341 1351
0 4.9(-2) 4.7(-4) 2.7(-1) 1.6(+1) 7.7 2.9($1) 1.5(-2) 2.5(+1) 2.4 2.5(+1) 2.7(-1) 6.2 5.6(-2) 1.2 1 2.9(-2) 2.7(-4) 1.6(-1) 9.6 4.3 1.6(+1) 3 4 - 3 ) 1.4(+1j 1.5 1.5(+1) 1.6(-1) 3.7 3.3(-2) 6.8(-1) 2 2.33-2) 2.1(-4) 1.3(-1) 7.4 3.7 1.3(+1) €.8(-3) 1.2(+13 1.1 I.l(+l) 1.2(-1) 2.3 2.6(-2] 5.2{-1)
3 2.0(-2) 1.9(-4) 1.1(-1) 6.4 3.6 1.2(+1] 5.9(-3) 1.2(+1) 9.5(-1) 1.0(+1) 1.0(-1) 2.3 2.21-2) 4.51-1)
4 1.8(-2) 1.7(-4) 9.4(-2) 5.6 3.6 i.l(+1) 5.3(-3) l.2(+1) 8.3(-1) 9.0 9.3(-2) 2.0 2.0(-9) 3.9(-1) 5 1.6(-2) 1.5(-4) 8.4{-2) 5.1 3.5 9.9 4.8(-3) 1.2(+1) 7.4(-1) 8.2 8.4(-2) 1.8 1.8(-2) 3.5(-3)
6 1.5(-2) 1.4(-4) 7.7(-2) 4.6 3.4 9.2 4.4(-3) 1.3(+1) €A(-1) 7.5 7.7(-2) 1.6 1.7(-2) 3.2(-1]
8 1.3(-2) 1.2(-4) 6.6(-2) 4.0 3.3 8.2 3.9(-3) 1.3(+1) 5.8(-1) 6.5 6.7(-2) 1.4 1.5(-2) 2.7(-1) 9 1.3(-2) 1.2(-4) 6.2(-2) 3.7 3.3 7.8 3.6(-3) 1.3(+1) 5.4(-1) 6.2 6.3(-2) 1.3 1.4(-2) 2.6(-3)
10 1.2(-2) 1.1(-4) 5.8(-2) 3.5 3.2 7.4 3.5(-3) 1.4(+1) 5.1(-1) 5.8 6.0(-2) 1.2 1.3( -2) 2.4(-1)
12 9.9(-3) 9.1(-5) 4.8(-2) 2.9 2.9 6.1 2.9(-3) 1.3(+1) 4.2(-1) 4.8 5.0(-2) 9.8(-9) 1.1(-2) 2.0(-13 13 8.6(-3) 7.9(-5) 4.1(-2) 2.5 2.6 5.3 2.5(-3) 1.2(+1) 3.6(-1) 4.1 4.3(-2) 8.4(-1) 9.4(-33 1.7(-1)
14 7.4(-3) 6.7(-5) 3.5(-2) 2.1 2.3 4.5 2.1(-3) 1.1(+1) 3.0(-1) 9.5 3.6(-2) 7.1(-1) 8.0(-3) 1.4(-1) 15 6.2(-3) 5.7(-5) 2.9(-2) 1.7 2.0 3.8 1.8(-3) 9.9 2.6(-1) 2.9 3.1(-2j 5.9<-1) 6.8(-3) 1.2(-1)
46 5.2(-3) 4.8(-5) 2.4(-2) 1.4 1.7 3.2 9.5(-3) 8.7 2.1(-1) 2.4 2.6(-2) 4.9(-1) 5.7(-3) S.O(-l)
18 3.4(-3) 3 4 - 5 ) 1.6(-2) 9.3(-1] 1.1 2.1 9.7(-4) 6.1 1.4(-1) 1.6 P.7(-2) 3. l ( - l f 3.7(-3) 6.5(-2) 19 3.3(-3) 3.0(-5) 1.5(-2) 8.9(-1) 1.1 2.0 9.3(-43 5.9 4.3(-1) 1.5 1.6(-2) 3.0(-1) 3.5(-3) 6.2(-2)
20 3.1(-3) 2.3(-5) 1.41-2) 8.5(-1) 1.0 1.9 B.3(-4) 5.7 1.3(-3) 1.4 1.5(-2) 2.9(-1) 3.4(-3) 6.0(-2)
2 i 3.0(-3) 2.7(-5) 1.4(-2) 3.2(-1) 1.0 1.8 8.5(-4) 5.4 1.2(-1] 9.4 1.5(-2) 2.7(-3) 3.3(-3) 5.71-2) 22 2.9(-3) 2.6(-5) 1.3(-2) 7.9(-1) 9.G(-1) 1.7 8.1(-4) 5.2 1.2(-1) 1.3 1.4(-2) 2.6(-1) 3.1(-3) 5.5(-2)
23 2.8(-3) 2.5(-5) 1.3(-2) 7.6(-1) 9.3(-1) 1.7 7 4 - 4 1 5.0 l.i(-l) 1.3 1.4(-2) 2.5(-1) 3.0(-3) 5.3(-2)
7 i.4(-2) i . q -4 ) 7.1(-2) 4.3 3.4 3.6 4 4 - 3 ) i.3(+1) 6.q-i) 7.0 7.2(-2) 1.5 1 4 - 2 ) a.s(-rj
11 l. l(-2) 1.1(-4) 5.6(-2) 3.3 3.2 7.1 3.3(-3) 1.4(+1) 4.9(-1) 5.6 5.q-2) 1.1 1.3(-2j 2.3(-1j
17 4.3(-3) 3.9(-5) 2.0(-2) 1.2 1.4 2.6 1.2(-3) 7.5 1.7(-1) 2.0 2.1(-4) 4.0(--1) 4.7(-33 824-2 )
24 2.7(-3) 2.4(-5) 1.2(-2) 7.3(-1) 9.q-1) 1.6 7.5(-4) 4.8 1.1(-1) 1.2 1.3(-2) 2.4(-1) 2.9(-3) j . l ( - 2 )
Female
25 2.6(-3) 2.3(-5) 1.2(-2) 7.1(-1) 3.7(-1) 1.6 7.3(-4) 4.7 l . O ( - l j 1.2 1.3(-2j 2 4 - 1 1 2.8(-3) 4.9(-2)
16 5.3(-3) 4.9(-5) 2.5(-2) 1.5 1.7 3.3 1.5(-3) 9.0 2.2(-1) 2.5 2.6(-2) 5.0(-1) 5.8(-3) 1.0(-1)
18 3.6(-3) 3.3(-5) 1.7(-2) 9.9(-1) 1.2 2.2 1.01-3) 6.6 3.4(-1) 1.7 1.8(-2) 3.3(-1) 3.9(-3) B.Q(-f f
19 3.5(-3) 3.2(-5) 1.6(-2) 9.6(-1) 1.2 2.1 1.0(-3) 6.4 i.4(-1) 1.6 1.7(-2) 3.2(-1) 3.8(-3) 6.71-21
20 3.4(-3) 3.1(-5) 1.6(-2) 9.3(-1) 1.1 2.1 9.7(-4) 6.2 1,4(-1) 1.6 1.7(-2) 3.1(-2) 3.7(-3) 6.5(-2] 2.0 9.5(-4) 6.1 1.9(-1) 1.5 1.6(-2) 3.1(-1] 3.6(-3) 6.4(-2) 21 3.3(-3) 3.0(-5) 1.5(-2) Q.l(-1) 1.1
22 3.3(-3) 2.9(-5) 1.5(-2) 8.9(-3) 1.1 2 .o 9.2(-4) 5.9 1.3(-1] 1.5 1.6(-2) 3.0(-1) 3.5(-3) 6.2(-2) 1.5(-2) 2.9(-1) 3.4(-3j 6.G{-2) 2 3 3.2(-3) 2.9(-5) 1.5(-2) 8.6(-1) 1.1 1.9 9.0(-4) 5.8
24 3.1(-3) 2.8(-5) 1.4(-2) 8.4(--1) 1.0 1.9 8.7(-4) 5.6 1.2(-1) 1.4 1.5(-2) 2.8(-2) 3.3(-3) 5.9(-2) 25 3.0(-3) 2.7(-5) 1.4(-2) 8.2(-1) 1.0 1.8 3.51-4) 5.5 1.2(-1) 1.4 1.5(-2) 2.3(-1) 3.3(-3) 5.8(-2)
17 4.5(-3) 4 4 - 5 ) 2 4 - 2 ) 1.2 1.5 2.7 1.31-3) 7.9 1.8(-1] 2.1 2.2(-2) 4.1(-1] 4.9(-3) f 3 . q - q
1.3{-1) 1.5

ORNL-DWG 86-13509 I I
Adolescent 47% ,--. E
B 40 f! - > 1 I- >- a
- Q Points indicate mean values. LL 0 W Y
Child - 0 5 - 2 years Adolescent - 6 - 16 years
20 Adult - 218 years ;I: - a 3 AdUlt1996 J 6 z
I- 10 - CL: LL
9
2
0 5 10 15 20 AGE (years)
Figure C1. fractional uptake of iodine to the thyroid as a function of age. The plotted points are mean values based on estimates reported by Dunning and Schwarz (1981).
For radioiodines with half-lives at most a few days, the dose is calculated by the formula
50 years
D = S(thyroid +-- thyroid) 1 qb(t)e-Xrt dt , ((3
where qb( t ) is given by Eq. C1 and the S-factor is calculated in a manner that is described in the next section. For the longer-lived isotopes, however (1251 and 1291, with half- lives 60.14 days and 5.73 x lo9 days, respectively), the dependence of the biological rate coefficients and the S-factor on age is a potentially significant effect in the integration, and Eq. C2 should be replaced by the more general formulation
where a0 denotes the age a t time t = 0, 8 0 ( u ~ 4- t ) is the age- and sex-dependent S-factor, and the age-dependent level of radioactivity in the thyroid, A(t; q), is obtained by solving
25
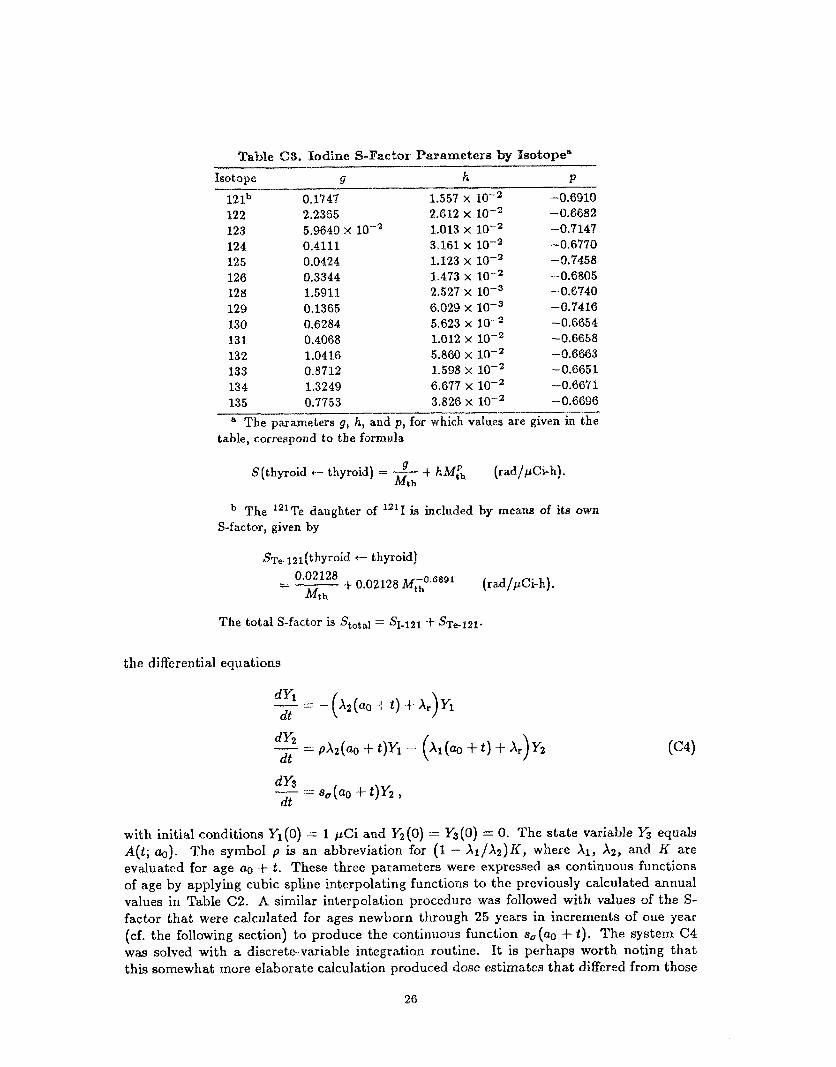
Table C8. Iodine S-Facto~ Parameters by Isotope"
Isotope 9 h P
12 lb 0.1147 1.557 x -0.6910 122 2.2365 2.612 x 10-2 -0.8682 123 5.9640 x 1.013 x 10-2 -0.7147 124 0.4111 3.161 x -0.6770 125 0.0424 1.123 x -0.7458 126 0.3344 1.473 x -0.6805 128 1.5911 2.527 x -0.6740 129 0.1365 6.029 x 10-3 -0.7416 130 0.6284 5.623 x -0.6654 131 0.4068 1.012 x 10-2 -0.6658 132 1.0416 5.860 x lo-' -0.6663 133 0.8712 1.598 x -0.6651 134 1.3249 6.677 x -0.6671 135 0.7753 3.826 x lo-' -0.6696 - " The parameters g, h, and p, for which values are given in the
table, correspond to the formula
9 Mt h
S(thyroid c- thyroid) = ___ -t- hMfh (rad/pCi-h).
The "'Te daughter of 12'X is included by means of its own S-factor, given by
Ser*12l(thyyroid 6- thyroid)
0.02128 Mt h
=- -t- 0.02128 Mt;;0.G8g1 (rad/pCi-h].
the differential equations
-- dY1 = - (X2(ao + t) 4- Ar)Yl dt
s,(ao + t)Y2 , dY3 dt --
with initial conditions Yl(0) = 1 pCi and Yz(0) = Y3(O) = 0. The state variable Y3 equals A(t; a*). The symbol p is an abbreviation for (1 - X ~ / X Z ) K , where XI, X2, and K are evaluated for age a0 + t . These three parameters were expressed as continuous functions of age by applying cubic spline interpolating functions to the previously calculated annual values in Table C2. A similar interpolation procedure was followed with values of the S- factor that were calculated for ages newborn through 25 years in increments of one year (cf. the following section) to produce the continuous function s,(ao + t). The system C4 was solved with a discrete-variable integration routine. It is perhaps worth noting that this somewhat more elaborate calculation produced dose estimates that differed from those
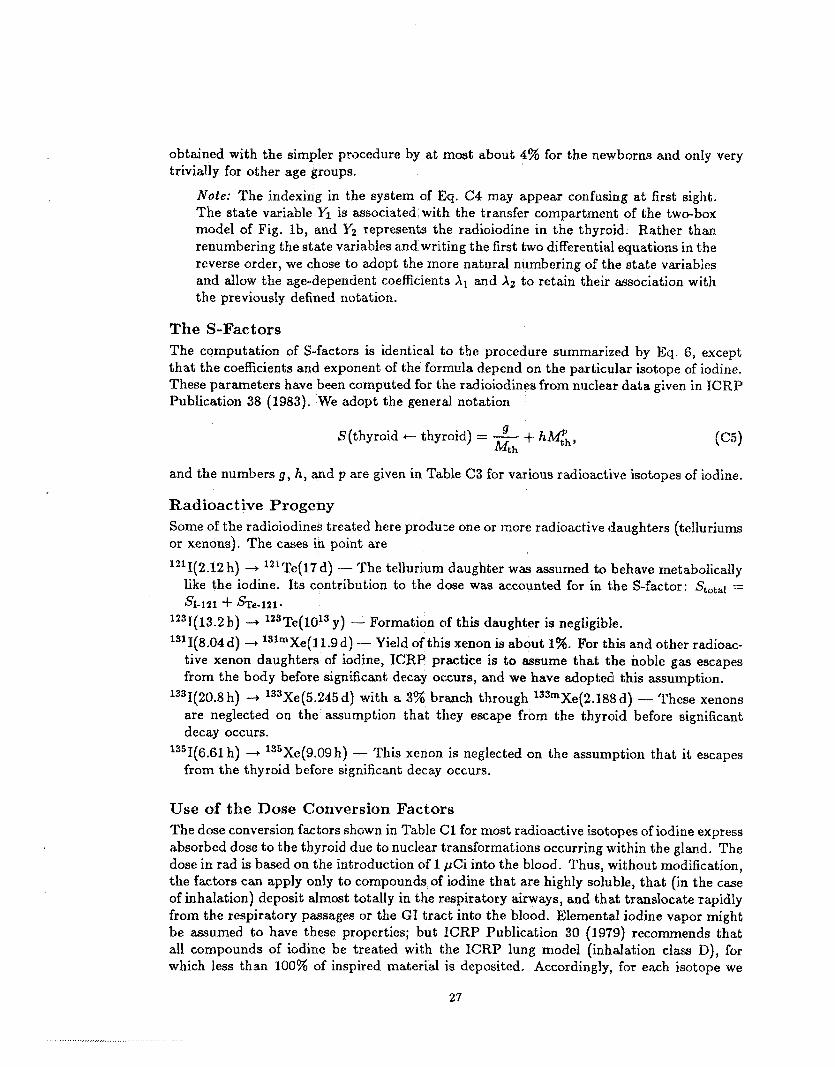
obtained with the simpler procedure by at most about 4% for the newborns and only very trivially for other age groups.
Note: The indexing in the system of Eq. C4 may appear confusing at first sight. The state variable Y1 is associated with the transfer compartment of the two-box model of Fig. lb, and Y2 represents the radioiodine in the thyroid. Rather than renumbering the state variables and writing the first two differential equations in the reverse order, we chose to adopt the more natural numbering of the state variables and allow the age-dependent coefficients XI and A2 to retain their association with the previously defined notation.
The S-Factors The computation of S-factors is identical to the procedure summarized by Eq. 6, except that the coefficients and exponent of the formula depend on the particular isotope of iodine. These parameters have been computed for the radioiodines from nuclear data given in ICRP Publication 38 (1983). We adopt the general notation
9 S(thyroid e thyroid) = - + h l ~ , P , , Mth
and the numbers g, h, and p are given in Table C3 for various radioactive isotopes of iodine.
Radioactive Progeny Some of the radioiodines treated here produce one or more radioactive daughters (telluriums or xenons). The cases in point are
1211(2.12 h) -+ 121Te(17d) - The tellurium daughter was assumed to behave metabolically like the iodine. Its contribution to the dose was accounted for in the S-factor: Statal = SI-121 -k sTe-121-
1231(13.2 h) -+ lZ3Te(lOl3 y) - Formation of this daughter is negligible.
13'I(8.04d) 3 131mXe(11.9d) - Yield of this xenon is about 1%. FOr this and other radioac- tive xenon daughters of iodine, ICRP practice is to assume that the noble gas escapes from the body before significant decay occurs, and we have adopted this assumption.
1331(20.8h) 4 133Xe(5.245d) with a 3% branch through 13SmXe(2.188d) - These xenons are neglected on the assumption that they escape from the thyroid before significant
1351(6.61 h) 3 135Xe(9.09 h) - This xenon is neglected on the assumption that it escapes
decay occurs.
from the thyroid before significant decay occurs.
Use of the Dose Conversion Factors The dose conversion factors shown in Table C1 for most radioactive isotopes of iodine express absorbed dose to the thyroid due to nuclear transformations occurring within the gland. The dose in rad is based on the introduction of 1 pCi into the blood. Thus, without modification, the factors can apply only to compounds of iodine that are highly soluble, that (in the case of inhalation) deposit almost totally in the respiratory airways, and that translocate rapidly from the respiratory passages or the GI tract into the blood. Elemental iodine vapor might be assumed to have these properties; but ICRP Publication 30 (1979) recommends that all compounds of iodine be treated with the ICRP lung model (inhalation class D), for which less than 100% of inspired material is deposited, Accordingly, for each isotope we
27

furnish an absorption fraction for inhalation that is based on the ICRP lung model, with particle diameter (AMAD) 1 p m and solubility class E) assumed. These absorption fractions are isotope-specific, because the fraction of the iodine that reaches the blood from the respiratory tract is dependent on the competition between radioactive decay and biological translocation processes. We remind the reader that neither age nor sex dependence i s built into the ICRP lung model, and any application of the inhalation absorption fractions to the age- and sex-dependent dose conversion factors of Table C1 should be undertaken only with this deficiency in mind. The absorption fractions for inhalation are given in Table 64 .
Table C4. Absorption Fractions @) for Radioiodinesl Based on ICRP Models for the Lung" and GI Tractb
Isotope 121 122 123 124 125 126 128 129 130 131 132 133 134 135 Inhalation 34 5 48 60 63 62 19 63 48 61 34 52 26 43 Ingestion 75 8 95 99 100 100 38 100 95 100 77 97 56 90
a Class D, AMAD = 1pm (ICRP, 1979). Iodine i s removed from the stomach directly to blood with biological rnean-time 1 hour (ICRP,
1979).
For ingestion of radioiodines, ICRP practice is to assume complete absorption of the iodine from the small intestine (ICRP, 1979). We have computed absorption fractions for ingestion by assuming that the iodine being removed from the stomach to the small intestine goes instead directly into the blood (Table C4). These ingestion fractions are significant only for short-lived isotopes and therefore are of little use for environmental studies in which ephemeral isotopes will have decayed away during their transit to the target individual. But for certain other applications, it may be useful to take into account the decay of radioactive iodine in the stomach before it reaches the blood; hence for completeness, the absorption factors for ingestion are included in Table C4. Note also that these fractions are based on a model of the GI tract that is neither age- nor sex-dependent, and that the model involves time constants that vary greatly from one individual to another.
References Note: All references, other than the following, are given in the main report.
Bell, G.H., J.N. Davidson, and H. Scarborough. 1968. Textbook of Physiology and Bio- chemistry. Edinburgh and London: E. & S. Livingstone Ltd.
28

29
IaTUREG/CR-3955 QRNL/TM-9800 Dist. Category Rti
INTERNAL DISTRIBUTION
1. B. A . Berven 2. R. 0. Chester
6. J. L. Davis 7. L. T. Dillman 8. D. E. Dunning, Jr
3-5. M. Cristy
9-13. K. F. Eckerman 14. F. 0 . Hoffman 15. S , V. Kaye
16-18. G. D. Kerr 19-23. G . G . Killough
24. F. F. Knapp 25-27. R. W. Leggett
28. 29. 30. 31. 32.
33-34. 35. 3 6 . 37. 38. 39.
40-41. 42,
C . W. Miller C . R. Richmond J. C . Ryman C . S . Sims P. J. Walsh B . P. Warren L. R. Williams E. A . Zeighamf Central Research Library Document Reference Section Laboratory Records Laboratory Records, ORNL - RC ORNL Patent Office
EXTERNAL DISTRIBUTION
43. Office of the Assistant Manager for Energy Research and Development, Department of Energy, Oak Ridge Operations Office, Oak Ridge, TN 37831
44-45. Technical Information Center, Oak Ridge, TN 37831
46. P. M . Hamilton, Division o f Life Sciences, Center for Devices and Radiological Health, U.S. Food and Drug Administration, Rockville, MD 20857
47. C. M. Luccioni, IPSN/DPS/SEAPS/LBA, Commissariat a’ e‘ Energie Atomique, BP 6, 92260 Fontenay aux Roses, FRANCE
48. Alexander Kaul, Institut fur Strahlenhygiene des Bundesgesundheitsamtes, Ingolstadter Landstrasse 1, D-8042 Neuherberg, Federal Republic of Germany
49. Wah Lee, Division of L i f e Sciences, Center for Devices and Radiological Health, U.S. Food and Drug Administration, Rockville, MD 20857
50. M. G. Stabin, Oak Ridge Associated Universities, NERT (2724F), P . 0. Box 117, Oak Ridge, Tennessee 37831
51. J. E. T i l l , Radiological Assessments Corp., Route 2, Box 122, Neeses, SC 29107
52. E. E. Watson, Oak Ridge Associated Universities, MERT (2714F), P. 0 . Box 117, Oak Ridge, Tennessee 37831
53. S . S . Yaniv, Office of Nuclear Regulatory Research, Division of Radiation Programs and Earth Sciences, U.S. Nuclear Regulatory Commission, Washington, DC 20555
54-223. Given distribution as shown in NUREG-0550 under category RI-I, Health and Safety Research Reports