Aesthetic Surgery Journal Barbed Sutures in Aesthetic...
15
Supplemental Article Aesthetic Surgery Journal 33(3S) 17S–31S © 2013 The American Society for Aesthetic Plastic Surgery, Inc. Reprints and permission: http://www.sagepub.com/ journalsPermissions.nav DOI: 10.1177/1090820X13499343 www.aestheticsurgeryjournal.com Suture suspension techniques have been used in various surgical specialties for decades. Among the more common applications are bladder suspension, uterine suspension, upper lid ptosis correction, treatment of sleep apnea, and a variety of other plastic surgical procedures, both aes- thetic and reconstructive. In the field of aesthetic facial plastic surgery, in particu- lar, much of the popularity of these techniques has focused on minimally invasive approaches—a phenome- non that has been largely patient driven rather than data driven. In fact, there is a dearth of peer-reviewed clinical data based on objective outcome measures from long-term controlled studies in this field. 1,2 To the best of my knowl- edge, no Level 1 or 2 and minimal Level 3 evidence cur- rently exists to support claims about the longevity of patient satisfaction and lower complication rates with these techniques. For the most part, the Level 3 evidence that does exist concerns the Aptos device (Kolster Methods, Inc, Anaheim, California), 1,2 which has been commercially available for the longest duration. This article reviews the evolution of barbed suture tech- nologies and their application to the field of plastic surgery. The features of various modified suture designs used in aesthetic plastic surgery are presented in Table 1. Many of the preferences for the techniques discussed in this article are my opinion, based on more than 30 years of personal experience in private clinical practice. Barbed Sutures in Aesthetic Plastic Surgery: Evolution of Thought and Process Malcolm D. Paul, MD, FACS Abstract The evolution of barbed suture technologies and their application in the field of plastic surgery is now in its third decade. Much has been learned along the way. Initial excitement was often followed by disappointment as we learned more about the limited longevity of minimally invasive procedures and complications arising from various suture designs of the past. Some of the early designs, developed primarily for use in aesthetic facial procedures, included free-floating, bidirectionally barbed, nonabsorbable sutures; unidirectional barbed, nonabsorbable sutures; anchored, bidirectional, nonabsorbable double- threaded sutures; and a technology combining a nonabsorbable knotted thread and absorbable cones. More recently, a new, absorbable, unidirectional barbed suture design has become available. However, it should be noted that very limited data are available for any of the modified suture designs used in this field, and much of what has been published is based on the experience of a single user. The author has used the bidirectionally barbed Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals, Inc, Vancouver, British Columbia, Canada), the most common barbed suture in both facial and other aesthetic plastic surgery procedures, with considerable success in various open aesthetic facial procedures, including suspension of the brow and midface, platysmaplasty, and lateral neck suspension. It is the author’s experience that completion of 1 to 2 cases with this technology is sufficient to achieve competency in the closure techniques discussed in this article and that time savings can be realized using this device in various breast and body contouring procedures, including mastopexy, reduction mammoplasty, abdominoplasty, bodylift, and brachioplasty. Keywords barbed sutures, suture suspension, wound closure, knotless wound closure Accepted for publication January 16, 2012. Dr Paul is Clinical Professor of Surgery in the Aesthetic and Plastic Surgery Institute, University of California, Irvine. Corresponding Author: Dr Malcolm D. Paul, Aesthetic and Plastic Surgery Institute, University of California, 1401 Avocado Ave, Suite 610, Newport Beach, CA 92660, USA. E-mail: [email protected] by guest on July 20, 2016 http://asj.oxfordjournals.org/ Downloaded from
Transcript of Aesthetic Surgery Journal Barbed Sutures in Aesthetic...

Supplemental Article
Aesthetic Surgery Journal33(3S) 17S ndash31Scopy 2013 The American Society for Aesthetic Plastic Surgery IncReprints and permission httpwww sagepubcomjournalsPermissionsnavDOI 1011771090820X13499343wwwaestheticsurgeryjournalcom
Suture suspension techniques have been used in various surgical specialties for decades Among the more common applications are bladder suspension uterine suspension upper lid ptosis correction treatment of sleep apnea and a variety of other plastic surgical procedures both aes-thetic and reconstructive
In the field of aesthetic facial plastic surgery in particu-lar much of the popularity of these techniques has focused on minimally invasive approachesmdasha phenome-non that has been largely patient driven rather than data driven In fact there is a dearth of peer-reviewed clinical data based on objective outcome measures from long-term controlled studies in this field12 To the best of my knowl-edge no Level 1 or 2 and minimal Level 3 evidence cur-rently exists to support claims about the longevity of patient satisfaction and lower complication rates with these techniques For the most part the Level 3 evidence that does exist concerns the Aptos device (Kolster Methods
Inc Anaheim California)12 which has been commercially available for the longest duration
This article reviews the evolution of barbed suture tech-nologies and their application to the field of plastic surgery The features of various modified suture designs used in aesthetic plastic surgery are presented in Table 1 Many of the preferences for the techniques discussed in this article are my opinion based on more than 30 years of personal experience in private clinical practice
Barbed Sutures in Aesthetic Plastic Surgery Evolution of Thought and Process
Malcolm D Paul MD FACS
AbstractThe evolution of barbed suture technologies and their application in the field of plastic surgery is now in its third decade Much has been learned along the way Initial excitement was often followed by disappointment as we learned more about the limited longevity of minimally invasive procedures and complications arising from various suture designs of the past Some of the early designs developed primarily for use in aesthetic facial procedures included free-floating bidirectionally barbed nonabsorbable sutures unidirectional barbed nonabsorbable sutures anchored bidirectional nonabsorbable double-threaded sutures and a technology combining a nonabsorbable knotted thread and absorbable cones More recently a new absorbable unidirectional barbed suture design has become available However it should be noted that very limited data are available for any of the modified suture designs used in this field and much of what has been published is based on the experience of a single user The author has used the bidirectionally barbed Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada) the most common barbed suture in both facial and other aesthetic plastic surgery procedures with considerable success in various open aesthetic facial procedures including suspension of the brow and midface platysmaplasty and lateral neck suspension It is the authorrsquos experience that completion of 1 to 2 cases with this technology is sufficient to achieve competency in the closure techniques discussed in this article and that time savings can be realized using this device in various breast and body contouring procedures including mastopexy reduction mammoplasty abdominoplasty bodylift and brachioplasty
Keywordsbarbed sutures suture suspension wound closure knotless wound closure
Accepted for publication January 16 2012
Dr Paul is Clinical Professor of Surgery in the Aesthetic and Plastic Surgery Institute University of California Irvine
Corresponding AuthorDr Malcolm D Paul Aesthetic and Plastic Surgery Institute University of California 1401 Avocado Ave Suite 610 Newport Beach CA 92660 USA E-mail mpaulmdhotmailcom
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
18S Aesthetic Surgery Journal 33(3S)
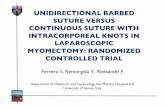
EArly BArBEd SuturE tEchnologyAptos ThreadThe introduction of suture suspension techniques in aes-thetic plastic surgery began in the late 1990s with the presentations and publications of Dr Marlen Sulamanidze who introduced the Aptos threads3 His procedure called the ldquofeatherliftrdquo was performed by inserting bidirectional barbed sutures into the subcutaneous plane of the face These sutures were manufactured with a nonabsorbable polymer (polypropylene) and designed to be used in freely mobile tissue Barbs are cut at an angle in the suture and organized facing toward the midline in a bidirectional fashion (Figure 1) Certainly it was attractive to be able to offer patients a ldquononinvasiverdquo approach to lifting ptotic facial soft tissues As we do with all new technology we
began with ldquoexuberant enthusiasmrdquo (in the words of the former Federal Reserve Chairman Alan Greenspan) However as we witnessed the relapse of ptosis and the possible complications of a nonabsorbable suturemdashwhich included palpation migration extrusion and abnormal facial expression on animationmdashour initial ldquoexuberant enthusiasmrdquo was replaced with unhappiness Reports of these types of complications began to appear in the litera-ture throughout the early 2000s based on large retrospec-tive data sets of more than 100 patients with up to 25 years of follow-up14-7 Modifications have since been made to the Aptos thread needle design and its placement method8 and further experience has allowed the tech-nique and technology to assume a niche in our surgical repertoire However there has never been widespread acceptance in the US market for this type of nonanchored nonabsorbable barbed suture suspension device
This experience with the Aptos device clearly illustrates the 3 phases in the introduction of a new technique andor technology first excitement followed by disappoint-ment then by defined applications This was certainly the case with the ldquofree-floatingrdquo nonabsorbable Aptos barbed suture technology
continuEd Evolution of BArBEd SuturE tEchnology
Stress relaxation occurs when soft tissue particularly skin is held under tension in 2 points The tensile relaxation properties of the dermis will reorganize the collagen elas-tin and ground substances to lengthen the distance between the fixation points As with tissue expansion the bodyrsquos ability to recruit tissue to reduce tension loading will compromise the elevation when the repositioning is supported in only 2 points (Dr Stephen Mulholland oral communication) Multiple-point fixation techniques and technologies such as the Endotine device (Coapt Systems Inc Palo Alto California) or barbed sutures can greatly minimize the stress relaxation and ldquocheese wiringrdquo associ-ated with 2-point fixation9 Without multiple fixation
Table 1 Comparison of Barbed Suture Devices
Suture Name Description Suture Placement
Aptos Thread (Kolster Methods Inc Anaheim California) Bidirectional nonabsorbable barbed suture Free floating
Contour Thread (Surgical Specialties Reading Pennsylvania) Unidirectional nonabsorbable looped or nonlooped barbed suture Anchored proximally
Isse Endo Progressive Facelift Suture (Kolster Methods Inc Anaheim California) Unidirectional nonabsorbable barbed suture Anchored proximally
Silhouette Mid-Face Suture (Kolster Methods Inc Anaheim California) Nonabsorbable suture material with absorbable knots at 10-mm intervals Anchored proximally
Woffles Thread (Kolster Methods Inc Anaheim California) Bidirectional nonabsorbable barbed suture doubled in a sling format Anchored proximally
V-Loc Wound Closure Device (Covidien Mansfield Massachusetts) Unidirectional knotless absorbable barbed suture Anchored or not anchored
Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada)
Absorbable and nonabsorbable knotless bidirectional barbed suture with central nonbarbed segment
Anchored or not anchored
Figure 1 Aptos thread 2G suture with insertion needles From Sulamanidze and Sulamanidze3 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 19S
points pure suture suspension techniques often have lim-ited long-term efficacy1011 An implied benefit of bidirec-tional barbed suture technology which can elevate tissue by compressing the tissues between the barbs in 1 direc-tion without placing tension at the opposite end is that it distributes retention forces along the entire length of the barbed segments12 Any device with an anchoring mecha-nism fixed at one end does not possess this feature
Contour Thread
In a renewed effort to introduce barbed suture technology into the field of aesthetic plastic surgery the Contour Thread device was developed by Dr Gregory Ruff and mar-keted by Surgical Specialties (Reading Pennsylvania) It received US Food and Drug Administration (FDA) clear-ance for midface suspension in 2005 This clear nonab-sorbable polypropylene unidirectional thread was designed with barbs arranged in a helical design similar to DNA The basic advantage of this suture was that it could be fixed at the proximal end to a nonmobile structure such as the deep temporal fascia or mastoid fascia In addition it was thought that having barbs along almost the full length of the suture eliminated cheese wiring reduced stress relaxation and allowed for tension unloading The origi-nal and most widely used design included a long Keith needle at one end and a curved needle at the other end (Figure 2) Another design featured a looped barbed suture with long needles on both ends The looped suture did not require the tying of a knot at the proximal ends of the sutures since the needle from one end of the suture was passed through the fixation point in fascia and then advanced to pierce the target soft tissue The procedure was labeled the ldquoContour Threadliftrdquo and the device was marketed along with numerous teaching courses that taught participants both through didactic lectures and live surgical demonstrations how to utilize the device for brow lifting midface lifting and jawline lifting
Again the initial enthusiasm for the Contour Thread was replaced with disappointment in many cases when the suspension simply did not hold nonundermined soft tissue In a report of 33 patients followed for a mean of 21 months aesthetic improvements noted at 1 month were not maintained in those who had received a threadlift13 In contrast patients who underwent other rejuvenation pro-cedures (eg lipotransfer chemical peels surgical rhytidec-tomies) showed longer-lasting improvements In a second reportmdashthis time of 72 proceduresmdash31 of patients required revision cosmetic surgery after a mean of 87 months14 A third report 45 of 29 subjects who under-went threadlift procedures experienced recurrence of lax-ity within 6 months15 Other problems with the Contour Thread emerged due to the position of the device and the fact that the suture was nonabsorbable Although some including myself were able to achieve some reasonably good results with repositioned soft tissue of the brow midface and neck in well-selected cases the efficacy of
threadlift procedures tended to be unpredictable In addi-tion to the problem of failure to maintain soft tissue eleva-tion complications of the threadlift included palpability of sutures tenderness extrusion of knots fracture of the suture migration and abnormal traction lines in the skin with or without animation1016 While acceptable improve-ments in the position of ptotic soft tissue were achieved in select patient groups surgeons could not consistently pre-dict who would do well and who would not This led for the most part to the abandonment of the use of the Contour Thread to hold nondissected soft tissue Today the device is no longer manufactured Evolving concepts for utilizing fixed-point barbed sutures included minimal and extensive dissection to free the soft tissue attachments
Figure 2 The Contour Thread a 25-cm 2-0 polypropylene suture with barbs cut into the central 10 cm of suture The Contour Thread device was the first contour suture approved by the US Food and Drug Administration From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
20S Aesthetic Surgery Journal 33(3S)
and then use of the barbed sutures to support the soft tis-sues1718 Soft tissue dissection followed by the use of barbed sutures to suspend tissue has been more reliable as a method to correct ptotic soft tissues than simply passing these sutures subcutaneously without first performing the dissection
Other Suture Designs
Dr Nicanor Isse a plastic surgeon in Newport Beach California first developed a unidirectionally barbed non-absorbable polypropylene suture known as the Isse Endo Progressive Face Lift Suture (Kolster Methods Inc) before designing an alternate type of modified suture the Silhouette Mid-Face Suture (Kolster Methods Inc) which received its US FDA approval for midface suspension in November 2006 Instead of having barbs contained within the polypropylene suture the Silhouette suture has knots tied at 10-mm intervals along the distal 10 cm of the suture (Figure 3)19 The knots hold unidirectional absorbable cones of polyglactic acid in place These cones which are actually a copolymer of glycolic acid and lactic acid pro-vide the tension loading for soft tissue elevation The cone anchors the suture and allows in-growth of soft tissue Whereas a barb only grasps the soft tissue at 1 fixed point the cone grasps tissue across 360 degrees This enhances the tensile loading capability which is no longer just across the barbed length of the suture but 360 degrees around the cone and the cone length of the suture The Silhouette suture is used principally for lifting and reposi-tioning the soft tissue of the midface and not for wound closure The initial reports on the Silhouette based on 17 patients who underwent midface repositioning with this suture have been favorable20 Patient satisfaction was 90 at 9 months resuspension of the sutures was neces-sary in only 1 case No larger data sets for this device are yet available
Still another barbed suture developed for facial soft tissue suspension is the Woffles thread (Kolster Methods) (Figure 4)721 With the Woffles lift a bidirectional non-absorbable polypropylene thread is introduced using an 18-gauge spinal needle placed in the temporal region The thread is doubled to form a sling suspending sag-ging tissues of the face from the stable temporal scalp Data published in 2004 from 112 patients indicated that approximately 30 of the aesthetic benefit of the Woffles lift was lost at 3 months but was otherwise maintained at 1 year7 Knot palpabilityexposure occurred in 9 of cases
Although the bidirectional Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada) described below is by far the most commonly used barbed suture in aesthetic plastic surgery at this time a unidirectional absorbable barbed suture device (V-Loc Wound Closure Device Covidien
Figure 3 Silhouette Midface Suture From Kress33 Reprinted with permission from Springer-Verlag
Figure 4 Woffles thread version 30 X From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 21S
Mansfield Massachusetts) has also been developed for knotless soft tissue approximation with the goal of reduc-ing operating times and knot-related complications The V-Loc is armed with a surgical needle attached to one suture end and a loop end effector at the other end I have had no experience with this device and at the time of writing there have been few publications of its use in plastic surgery applications
Quill Device
Since the development of the early barbed suture devices described above barbed suture technology has progressed to the development of both absorbable and nonabsorbable bidirectionally barbed sutures with barbs arranged in opposing directions on either side of an unbarbed segment (ie the Quill device)22 This device is armed with a surgi-cal needle on each end Absorbable materials for the device include polydioxanone (PDO) and Monoderm (Angiotech Pharmaceuticals Inc) a polyglycolide-poly-e-caprolactone copolymer (Figure 5) Nonabsorbable mate-rials include nylon and polypropylene A novel helical design in the placement of the barbs supports the concept of better tissue adherence to the barbs (Figure 6) As with prior barbed suture configurations the goal of this new design was to avoid knot tying which has on occasion resulted in palpability of the knots Extensive preclinical testing was conducted to ensure that the tensile strength of the Quill materials provided sustained soft tissue approximation with an absorption curve compatible with the time required for neo-collagen formation to maintain the integrity of the soft tissue approximation10
The Quill Monoderm (Figure 5B) is the most recently available absorbable bidirectional barbed suture It is designed for placement in the mid-dermis Compared with Quill PDO the Quill Monoderm has a more rapid absorp-tion curve and eliminates the exposureextrusion issue
that has been seen when larger diameter PDO sutures are placed too superficially in the dermis
Barb morphology influences holding and tensile strength The deeper the barb is cut the lower the tensile strength Therefore with the Quill device it is important to select a suture size that is 1 thickness above the size of any conventional suture For example in cases where a 2-0 absorbable conventional suture would have been used a 0 bidirectional barbed suture should be used to account for the difference in the strength of the suture material
In my experience both midface and brow elevation can be maintained with absorbable bidirectional barbed sutures but as expected patients with the most favorable anatomy (eg low body mass index minimal fullness to the soft tissues strong underlying bony projection to sup-port the elevated tissue good skin quality) have shown the best results and most commonly extensive soft tissue dissection has been required to ensure that elevated soft tissue remains elevated2324 Specific techniques in aes-thetic facial plastic surgery that I have developed to take advantage of the unique properties of the Quill device are outlined below Unfortunately no large data sets of patient experience have been reported to date with this device in aesthetic facial plastic surgery As a result no objective outcome data accompany these descriptions My prefer-ence for the use of the bidirectional barbed device over conventional sutures for these procedures is based solely on anecdotal experience that better outcomes are achieved with the Quill barbed device
Quill Techniques
Suspension of the browIn this technique incisions are made behind the temporal hairline The temporal dissection proceeds on top of the deep temporal fascia releasing the periorbital lateral to
Figure 5 Absorbable bidirectional barbed sutures (A) The Quill SRS polydioxanone (PDO) device (B) The Quill Monoderm device Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

18S Aesthetic Surgery Journal 33(3S)
EArly BArBEd SuturE tEchnologyAptos ThreadThe introduction of suture suspension techniques in aes-thetic plastic surgery began in the late 1990s with the presentations and publications of Dr Marlen Sulamanidze who introduced the Aptos threads3 His procedure called the ldquofeatherliftrdquo was performed by inserting bidirectional barbed sutures into the subcutaneous plane of the face These sutures were manufactured with a nonabsorbable polymer (polypropylene) and designed to be used in freely mobile tissue Barbs are cut at an angle in the suture and organized facing toward the midline in a bidirectional fashion (Figure 1) Certainly it was attractive to be able to offer patients a ldquononinvasiverdquo approach to lifting ptotic facial soft tissues As we do with all new technology we
began with ldquoexuberant enthusiasmrdquo (in the words of the former Federal Reserve Chairman Alan Greenspan) However as we witnessed the relapse of ptosis and the possible complications of a nonabsorbable suturemdashwhich included palpation migration extrusion and abnormal facial expression on animationmdashour initial ldquoexuberant enthusiasmrdquo was replaced with unhappiness Reports of these types of complications began to appear in the litera-ture throughout the early 2000s based on large retrospec-tive data sets of more than 100 patients with up to 25 years of follow-up14-7 Modifications have since been made to the Aptos thread needle design and its placement method8 and further experience has allowed the tech-nique and technology to assume a niche in our surgical repertoire However there has never been widespread acceptance in the US market for this type of nonanchored nonabsorbable barbed suture suspension device
This experience with the Aptos device clearly illustrates the 3 phases in the introduction of a new technique andor technology first excitement followed by disappoint-ment then by defined applications This was certainly the case with the ldquofree-floatingrdquo nonabsorbable Aptos barbed suture technology
continuEd Evolution of BArBEd SuturE tEchnology
Stress relaxation occurs when soft tissue particularly skin is held under tension in 2 points The tensile relaxation properties of the dermis will reorganize the collagen elas-tin and ground substances to lengthen the distance between the fixation points As with tissue expansion the bodyrsquos ability to recruit tissue to reduce tension loading will compromise the elevation when the repositioning is supported in only 2 points (Dr Stephen Mulholland oral communication) Multiple-point fixation techniques and technologies such as the Endotine device (Coapt Systems Inc Palo Alto California) or barbed sutures can greatly minimize the stress relaxation and ldquocheese wiringrdquo associ-ated with 2-point fixation9 Without multiple fixation
Table 1 Comparison of Barbed Suture Devices
Suture Name Description Suture Placement
Aptos Thread (Kolster Methods Inc Anaheim California) Bidirectional nonabsorbable barbed suture Free floating
Contour Thread (Surgical Specialties Reading Pennsylvania) Unidirectional nonabsorbable looped or nonlooped barbed suture Anchored proximally
Isse Endo Progressive Facelift Suture (Kolster Methods Inc Anaheim California) Unidirectional nonabsorbable barbed suture Anchored proximally
Silhouette Mid-Face Suture (Kolster Methods Inc Anaheim California) Nonabsorbable suture material with absorbable knots at 10-mm intervals Anchored proximally
Woffles Thread (Kolster Methods Inc Anaheim California) Bidirectional nonabsorbable barbed suture doubled in a sling format Anchored proximally
V-Loc Wound Closure Device (Covidien Mansfield Massachusetts) Unidirectional knotless absorbable barbed suture Anchored or not anchored
Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada)
Absorbable and nonabsorbable knotless bidirectional barbed suture with central nonbarbed segment
Anchored or not anchored
Figure 1 Aptos thread 2G suture with insertion needles From Sulamanidze and Sulamanidze3 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 19S
points pure suture suspension techniques often have lim-ited long-term efficacy1011 An implied benefit of bidirec-tional barbed suture technology which can elevate tissue by compressing the tissues between the barbs in 1 direc-tion without placing tension at the opposite end is that it distributes retention forces along the entire length of the barbed segments12 Any device with an anchoring mecha-nism fixed at one end does not possess this feature
Contour Thread
In a renewed effort to introduce barbed suture technology into the field of aesthetic plastic surgery the Contour Thread device was developed by Dr Gregory Ruff and mar-keted by Surgical Specialties (Reading Pennsylvania) It received US Food and Drug Administration (FDA) clear-ance for midface suspension in 2005 This clear nonab-sorbable polypropylene unidirectional thread was designed with barbs arranged in a helical design similar to DNA The basic advantage of this suture was that it could be fixed at the proximal end to a nonmobile structure such as the deep temporal fascia or mastoid fascia In addition it was thought that having barbs along almost the full length of the suture eliminated cheese wiring reduced stress relaxation and allowed for tension unloading The origi-nal and most widely used design included a long Keith needle at one end and a curved needle at the other end (Figure 2) Another design featured a looped barbed suture with long needles on both ends The looped suture did not require the tying of a knot at the proximal ends of the sutures since the needle from one end of the suture was passed through the fixation point in fascia and then advanced to pierce the target soft tissue The procedure was labeled the ldquoContour Threadliftrdquo and the device was marketed along with numerous teaching courses that taught participants both through didactic lectures and live surgical demonstrations how to utilize the device for brow lifting midface lifting and jawline lifting
Again the initial enthusiasm for the Contour Thread was replaced with disappointment in many cases when the suspension simply did not hold nonundermined soft tissue In a report of 33 patients followed for a mean of 21 months aesthetic improvements noted at 1 month were not maintained in those who had received a threadlift13 In contrast patients who underwent other rejuvenation pro-cedures (eg lipotransfer chemical peels surgical rhytidec-tomies) showed longer-lasting improvements In a second reportmdashthis time of 72 proceduresmdash31 of patients required revision cosmetic surgery after a mean of 87 months14 A third report 45 of 29 subjects who under-went threadlift procedures experienced recurrence of lax-ity within 6 months15 Other problems with the Contour Thread emerged due to the position of the device and the fact that the suture was nonabsorbable Although some including myself were able to achieve some reasonably good results with repositioned soft tissue of the brow midface and neck in well-selected cases the efficacy of
threadlift procedures tended to be unpredictable In addi-tion to the problem of failure to maintain soft tissue eleva-tion complications of the threadlift included palpability of sutures tenderness extrusion of knots fracture of the suture migration and abnormal traction lines in the skin with or without animation1016 While acceptable improve-ments in the position of ptotic soft tissue were achieved in select patient groups surgeons could not consistently pre-dict who would do well and who would not This led for the most part to the abandonment of the use of the Contour Thread to hold nondissected soft tissue Today the device is no longer manufactured Evolving concepts for utilizing fixed-point barbed sutures included minimal and extensive dissection to free the soft tissue attachments
Figure 2 The Contour Thread a 25-cm 2-0 polypropylene suture with barbs cut into the central 10 cm of suture The Contour Thread device was the first contour suture approved by the US Food and Drug Administration From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
20S Aesthetic Surgery Journal 33(3S)
and then use of the barbed sutures to support the soft tis-sues1718 Soft tissue dissection followed by the use of barbed sutures to suspend tissue has been more reliable as a method to correct ptotic soft tissues than simply passing these sutures subcutaneously without first performing the dissection
Other Suture Designs
Dr Nicanor Isse a plastic surgeon in Newport Beach California first developed a unidirectionally barbed non-absorbable polypropylene suture known as the Isse Endo Progressive Face Lift Suture (Kolster Methods Inc) before designing an alternate type of modified suture the Silhouette Mid-Face Suture (Kolster Methods Inc) which received its US FDA approval for midface suspension in November 2006 Instead of having barbs contained within the polypropylene suture the Silhouette suture has knots tied at 10-mm intervals along the distal 10 cm of the suture (Figure 3)19 The knots hold unidirectional absorbable cones of polyglactic acid in place These cones which are actually a copolymer of glycolic acid and lactic acid pro-vide the tension loading for soft tissue elevation The cone anchors the suture and allows in-growth of soft tissue Whereas a barb only grasps the soft tissue at 1 fixed point the cone grasps tissue across 360 degrees This enhances the tensile loading capability which is no longer just across the barbed length of the suture but 360 degrees around the cone and the cone length of the suture The Silhouette suture is used principally for lifting and reposi-tioning the soft tissue of the midface and not for wound closure The initial reports on the Silhouette based on 17 patients who underwent midface repositioning with this suture have been favorable20 Patient satisfaction was 90 at 9 months resuspension of the sutures was neces-sary in only 1 case No larger data sets for this device are yet available
Still another barbed suture developed for facial soft tissue suspension is the Woffles thread (Kolster Methods) (Figure 4)721 With the Woffles lift a bidirectional non-absorbable polypropylene thread is introduced using an 18-gauge spinal needle placed in the temporal region The thread is doubled to form a sling suspending sag-ging tissues of the face from the stable temporal scalp Data published in 2004 from 112 patients indicated that approximately 30 of the aesthetic benefit of the Woffles lift was lost at 3 months but was otherwise maintained at 1 year7 Knot palpabilityexposure occurred in 9 of cases
Although the bidirectional Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada) described below is by far the most commonly used barbed suture in aesthetic plastic surgery at this time a unidirectional absorbable barbed suture device (V-Loc Wound Closure Device Covidien
Figure 3 Silhouette Midface Suture From Kress33 Reprinted with permission from Springer-Verlag
Figure 4 Woffles thread version 30 X From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 21S
Mansfield Massachusetts) has also been developed for knotless soft tissue approximation with the goal of reduc-ing operating times and knot-related complications The V-Loc is armed with a surgical needle attached to one suture end and a loop end effector at the other end I have had no experience with this device and at the time of writing there have been few publications of its use in plastic surgery applications
Quill Device
Since the development of the early barbed suture devices described above barbed suture technology has progressed to the development of both absorbable and nonabsorbable bidirectionally barbed sutures with barbs arranged in opposing directions on either side of an unbarbed segment (ie the Quill device)22 This device is armed with a surgi-cal needle on each end Absorbable materials for the device include polydioxanone (PDO) and Monoderm (Angiotech Pharmaceuticals Inc) a polyglycolide-poly-e-caprolactone copolymer (Figure 5) Nonabsorbable mate-rials include nylon and polypropylene A novel helical design in the placement of the barbs supports the concept of better tissue adherence to the barbs (Figure 6) As with prior barbed suture configurations the goal of this new design was to avoid knot tying which has on occasion resulted in palpability of the knots Extensive preclinical testing was conducted to ensure that the tensile strength of the Quill materials provided sustained soft tissue approximation with an absorption curve compatible with the time required for neo-collagen formation to maintain the integrity of the soft tissue approximation10
The Quill Monoderm (Figure 5B) is the most recently available absorbable bidirectional barbed suture It is designed for placement in the mid-dermis Compared with Quill PDO the Quill Monoderm has a more rapid absorp-tion curve and eliminates the exposureextrusion issue
that has been seen when larger diameter PDO sutures are placed too superficially in the dermis
Barb morphology influences holding and tensile strength The deeper the barb is cut the lower the tensile strength Therefore with the Quill device it is important to select a suture size that is 1 thickness above the size of any conventional suture For example in cases where a 2-0 absorbable conventional suture would have been used a 0 bidirectional barbed suture should be used to account for the difference in the strength of the suture material
In my experience both midface and brow elevation can be maintained with absorbable bidirectional barbed sutures but as expected patients with the most favorable anatomy (eg low body mass index minimal fullness to the soft tissues strong underlying bony projection to sup-port the elevated tissue good skin quality) have shown the best results and most commonly extensive soft tissue dissection has been required to ensure that elevated soft tissue remains elevated2324 Specific techniques in aes-thetic facial plastic surgery that I have developed to take advantage of the unique properties of the Quill device are outlined below Unfortunately no large data sets of patient experience have been reported to date with this device in aesthetic facial plastic surgery As a result no objective outcome data accompany these descriptions My prefer-ence for the use of the bidirectional barbed device over conventional sutures for these procedures is based solely on anecdotal experience that better outcomes are achieved with the Quill barbed device
Quill Techniques
Suspension of the browIn this technique incisions are made behind the temporal hairline The temporal dissection proceeds on top of the deep temporal fascia releasing the periorbital lateral to
Figure 5 Absorbable bidirectional barbed sutures (A) The Quill SRS polydioxanone (PDO) device (B) The Quill Monoderm device Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 19S
points pure suture suspension techniques often have lim-ited long-term efficacy1011 An implied benefit of bidirec-tional barbed suture technology which can elevate tissue by compressing the tissues between the barbs in 1 direc-tion without placing tension at the opposite end is that it distributes retention forces along the entire length of the barbed segments12 Any device with an anchoring mecha-nism fixed at one end does not possess this feature
Contour Thread
In a renewed effort to introduce barbed suture technology into the field of aesthetic plastic surgery the Contour Thread device was developed by Dr Gregory Ruff and mar-keted by Surgical Specialties (Reading Pennsylvania) It received US Food and Drug Administration (FDA) clear-ance for midface suspension in 2005 This clear nonab-sorbable polypropylene unidirectional thread was designed with barbs arranged in a helical design similar to DNA The basic advantage of this suture was that it could be fixed at the proximal end to a nonmobile structure such as the deep temporal fascia or mastoid fascia In addition it was thought that having barbs along almost the full length of the suture eliminated cheese wiring reduced stress relaxation and allowed for tension unloading The origi-nal and most widely used design included a long Keith needle at one end and a curved needle at the other end (Figure 2) Another design featured a looped barbed suture with long needles on both ends The looped suture did not require the tying of a knot at the proximal ends of the sutures since the needle from one end of the suture was passed through the fixation point in fascia and then advanced to pierce the target soft tissue The procedure was labeled the ldquoContour Threadliftrdquo and the device was marketed along with numerous teaching courses that taught participants both through didactic lectures and live surgical demonstrations how to utilize the device for brow lifting midface lifting and jawline lifting
Again the initial enthusiasm for the Contour Thread was replaced with disappointment in many cases when the suspension simply did not hold nonundermined soft tissue In a report of 33 patients followed for a mean of 21 months aesthetic improvements noted at 1 month were not maintained in those who had received a threadlift13 In contrast patients who underwent other rejuvenation pro-cedures (eg lipotransfer chemical peels surgical rhytidec-tomies) showed longer-lasting improvements In a second reportmdashthis time of 72 proceduresmdash31 of patients required revision cosmetic surgery after a mean of 87 months14 A third report 45 of 29 subjects who under-went threadlift procedures experienced recurrence of lax-ity within 6 months15 Other problems with the Contour Thread emerged due to the position of the device and the fact that the suture was nonabsorbable Although some including myself were able to achieve some reasonably good results with repositioned soft tissue of the brow midface and neck in well-selected cases the efficacy of
threadlift procedures tended to be unpredictable In addi-tion to the problem of failure to maintain soft tissue eleva-tion complications of the threadlift included palpability of sutures tenderness extrusion of knots fracture of the suture migration and abnormal traction lines in the skin with or without animation1016 While acceptable improve-ments in the position of ptotic soft tissue were achieved in select patient groups surgeons could not consistently pre-dict who would do well and who would not This led for the most part to the abandonment of the use of the Contour Thread to hold nondissected soft tissue Today the device is no longer manufactured Evolving concepts for utilizing fixed-point barbed sutures included minimal and extensive dissection to free the soft tissue attachments
Figure 2 The Contour Thread a 25-cm 2-0 polypropylene suture with barbs cut into the central 10 cm of suture The Contour Thread device was the first contour suture approved by the US Food and Drug Administration From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
20S Aesthetic Surgery Journal 33(3S)
and then use of the barbed sutures to support the soft tis-sues1718 Soft tissue dissection followed by the use of barbed sutures to suspend tissue has been more reliable as a method to correct ptotic soft tissues than simply passing these sutures subcutaneously without first performing the dissection
Other Suture Designs
Dr Nicanor Isse a plastic surgeon in Newport Beach California first developed a unidirectionally barbed non-absorbable polypropylene suture known as the Isse Endo Progressive Face Lift Suture (Kolster Methods Inc) before designing an alternate type of modified suture the Silhouette Mid-Face Suture (Kolster Methods Inc) which received its US FDA approval for midface suspension in November 2006 Instead of having barbs contained within the polypropylene suture the Silhouette suture has knots tied at 10-mm intervals along the distal 10 cm of the suture (Figure 3)19 The knots hold unidirectional absorbable cones of polyglactic acid in place These cones which are actually a copolymer of glycolic acid and lactic acid pro-vide the tension loading for soft tissue elevation The cone anchors the suture and allows in-growth of soft tissue Whereas a barb only grasps the soft tissue at 1 fixed point the cone grasps tissue across 360 degrees This enhances the tensile loading capability which is no longer just across the barbed length of the suture but 360 degrees around the cone and the cone length of the suture The Silhouette suture is used principally for lifting and reposi-tioning the soft tissue of the midface and not for wound closure The initial reports on the Silhouette based on 17 patients who underwent midface repositioning with this suture have been favorable20 Patient satisfaction was 90 at 9 months resuspension of the sutures was neces-sary in only 1 case No larger data sets for this device are yet available
Still another barbed suture developed for facial soft tissue suspension is the Woffles thread (Kolster Methods) (Figure 4)721 With the Woffles lift a bidirectional non-absorbable polypropylene thread is introduced using an 18-gauge spinal needle placed in the temporal region The thread is doubled to form a sling suspending sag-ging tissues of the face from the stable temporal scalp Data published in 2004 from 112 patients indicated that approximately 30 of the aesthetic benefit of the Woffles lift was lost at 3 months but was otherwise maintained at 1 year7 Knot palpabilityexposure occurred in 9 of cases
Although the bidirectional Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada) described below is by far the most commonly used barbed suture in aesthetic plastic surgery at this time a unidirectional absorbable barbed suture device (V-Loc Wound Closure Device Covidien
Figure 3 Silhouette Midface Suture From Kress33 Reprinted with permission from Springer-Verlag
Figure 4 Woffles thread version 30 X From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 21S
Mansfield Massachusetts) has also been developed for knotless soft tissue approximation with the goal of reduc-ing operating times and knot-related complications The V-Loc is armed with a surgical needle attached to one suture end and a loop end effector at the other end I have had no experience with this device and at the time of writing there have been few publications of its use in plastic surgery applications
Quill Device
Since the development of the early barbed suture devices described above barbed suture technology has progressed to the development of both absorbable and nonabsorbable bidirectionally barbed sutures with barbs arranged in opposing directions on either side of an unbarbed segment (ie the Quill device)22 This device is armed with a surgi-cal needle on each end Absorbable materials for the device include polydioxanone (PDO) and Monoderm (Angiotech Pharmaceuticals Inc) a polyglycolide-poly-e-caprolactone copolymer (Figure 5) Nonabsorbable mate-rials include nylon and polypropylene A novel helical design in the placement of the barbs supports the concept of better tissue adherence to the barbs (Figure 6) As with prior barbed suture configurations the goal of this new design was to avoid knot tying which has on occasion resulted in palpability of the knots Extensive preclinical testing was conducted to ensure that the tensile strength of the Quill materials provided sustained soft tissue approximation with an absorption curve compatible with the time required for neo-collagen formation to maintain the integrity of the soft tissue approximation10
The Quill Monoderm (Figure 5B) is the most recently available absorbable bidirectional barbed suture It is designed for placement in the mid-dermis Compared with Quill PDO the Quill Monoderm has a more rapid absorp-tion curve and eliminates the exposureextrusion issue
that has been seen when larger diameter PDO sutures are placed too superficially in the dermis
Barb morphology influences holding and tensile strength The deeper the barb is cut the lower the tensile strength Therefore with the Quill device it is important to select a suture size that is 1 thickness above the size of any conventional suture For example in cases where a 2-0 absorbable conventional suture would have been used a 0 bidirectional barbed suture should be used to account for the difference in the strength of the suture material
In my experience both midface and brow elevation can be maintained with absorbable bidirectional barbed sutures but as expected patients with the most favorable anatomy (eg low body mass index minimal fullness to the soft tissues strong underlying bony projection to sup-port the elevated tissue good skin quality) have shown the best results and most commonly extensive soft tissue dissection has been required to ensure that elevated soft tissue remains elevated2324 Specific techniques in aes-thetic facial plastic surgery that I have developed to take advantage of the unique properties of the Quill device are outlined below Unfortunately no large data sets of patient experience have been reported to date with this device in aesthetic facial plastic surgery As a result no objective outcome data accompany these descriptions My prefer-ence for the use of the bidirectional barbed device over conventional sutures for these procedures is based solely on anecdotal experience that better outcomes are achieved with the Quill barbed device
Quill Techniques
Suspension of the browIn this technique incisions are made behind the temporal hairline The temporal dissection proceeds on top of the deep temporal fascia releasing the periorbital lateral to
Figure 5 Absorbable bidirectional barbed sutures (A) The Quill SRS polydioxanone (PDO) device (B) The Quill Monoderm device Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

20S Aesthetic Surgery Journal 33(3S)
and then use of the barbed sutures to support the soft tis-sues1718 Soft tissue dissection followed by the use of barbed sutures to suspend tissue has been more reliable as a method to correct ptotic soft tissues than simply passing these sutures subcutaneously without first performing the dissection
Other Suture Designs
Dr Nicanor Isse a plastic surgeon in Newport Beach California first developed a unidirectionally barbed non-absorbable polypropylene suture known as the Isse Endo Progressive Face Lift Suture (Kolster Methods Inc) before designing an alternate type of modified suture the Silhouette Mid-Face Suture (Kolster Methods Inc) which received its US FDA approval for midface suspension in November 2006 Instead of having barbs contained within the polypropylene suture the Silhouette suture has knots tied at 10-mm intervals along the distal 10 cm of the suture (Figure 3)19 The knots hold unidirectional absorbable cones of polyglactic acid in place These cones which are actually a copolymer of glycolic acid and lactic acid pro-vide the tension loading for soft tissue elevation The cone anchors the suture and allows in-growth of soft tissue Whereas a barb only grasps the soft tissue at 1 fixed point the cone grasps tissue across 360 degrees This enhances the tensile loading capability which is no longer just across the barbed length of the suture but 360 degrees around the cone and the cone length of the suture The Silhouette suture is used principally for lifting and reposi-tioning the soft tissue of the midface and not for wound closure The initial reports on the Silhouette based on 17 patients who underwent midface repositioning with this suture have been favorable20 Patient satisfaction was 90 at 9 months resuspension of the sutures was neces-sary in only 1 case No larger data sets for this device are yet available
Still another barbed suture developed for facial soft tissue suspension is the Woffles thread (Kolster Methods) (Figure 4)721 With the Woffles lift a bidirectional non-absorbable polypropylene thread is introduced using an 18-gauge spinal needle placed in the temporal region The thread is doubled to form a sling suspending sag-ging tissues of the face from the stable temporal scalp Data published in 2004 from 112 patients indicated that approximately 30 of the aesthetic benefit of the Woffles lift was lost at 3 months but was otherwise maintained at 1 year7 Knot palpabilityexposure occurred in 9 of cases
Although the bidirectional Quill Knotless Tissue-Closure Device (Angiotech Pharmaceuticals Inc Vancouver British Columbia Canada) described below is by far the most commonly used barbed suture in aesthetic plastic surgery at this time a unidirectional absorbable barbed suture device (V-Loc Wound Closure Device Covidien
Figure 3 Silhouette Midface Suture From Kress33 Reprinted with permission from Springer-Verlag
Figure 4 Woffles thread version 30 X From Kress33 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 21S
Mansfield Massachusetts) has also been developed for knotless soft tissue approximation with the goal of reduc-ing operating times and knot-related complications The V-Loc is armed with a surgical needle attached to one suture end and a loop end effector at the other end I have had no experience with this device and at the time of writing there have been few publications of its use in plastic surgery applications
Quill Device
Since the development of the early barbed suture devices described above barbed suture technology has progressed to the development of both absorbable and nonabsorbable bidirectionally barbed sutures with barbs arranged in opposing directions on either side of an unbarbed segment (ie the Quill device)22 This device is armed with a surgi-cal needle on each end Absorbable materials for the device include polydioxanone (PDO) and Monoderm (Angiotech Pharmaceuticals Inc) a polyglycolide-poly-e-caprolactone copolymer (Figure 5) Nonabsorbable mate-rials include nylon and polypropylene A novel helical design in the placement of the barbs supports the concept of better tissue adherence to the barbs (Figure 6) As with prior barbed suture configurations the goal of this new design was to avoid knot tying which has on occasion resulted in palpability of the knots Extensive preclinical testing was conducted to ensure that the tensile strength of the Quill materials provided sustained soft tissue approximation with an absorption curve compatible with the time required for neo-collagen formation to maintain the integrity of the soft tissue approximation10
The Quill Monoderm (Figure 5B) is the most recently available absorbable bidirectional barbed suture It is designed for placement in the mid-dermis Compared with Quill PDO the Quill Monoderm has a more rapid absorp-tion curve and eliminates the exposureextrusion issue
that has been seen when larger diameter PDO sutures are placed too superficially in the dermis
Barb morphology influences holding and tensile strength The deeper the barb is cut the lower the tensile strength Therefore with the Quill device it is important to select a suture size that is 1 thickness above the size of any conventional suture For example in cases where a 2-0 absorbable conventional suture would have been used a 0 bidirectional barbed suture should be used to account for the difference in the strength of the suture material
In my experience both midface and brow elevation can be maintained with absorbable bidirectional barbed sutures but as expected patients with the most favorable anatomy (eg low body mass index minimal fullness to the soft tissues strong underlying bony projection to sup-port the elevated tissue good skin quality) have shown the best results and most commonly extensive soft tissue dissection has been required to ensure that elevated soft tissue remains elevated2324 Specific techniques in aes-thetic facial plastic surgery that I have developed to take advantage of the unique properties of the Quill device are outlined below Unfortunately no large data sets of patient experience have been reported to date with this device in aesthetic facial plastic surgery As a result no objective outcome data accompany these descriptions My prefer-ence for the use of the bidirectional barbed device over conventional sutures for these procedures is based solely on anecdotal experience that better outcomes are achieved with the Quill barbed device
Quill Techniques
Suspension of the browIn this technique incisions are made behind the temporal hairline The temporal dissection proceeds on top of the deep temporal fascia releasing the periorbital lateral to
Figure 5 Absorbable bidirectional barbed sutures (A) The Quill SRS polydioxanone (PDO) device (B) The Quill Monoderm device Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 21S
Mansfield Massachusetts) has also been developed for knotless soft tissue approximation with the goal of reduc-ing operating times and knot-related complications The V-Loc is armed with a surgical needle attached to one suture end and a loop end effector at the other end I have had no experience with this device and at the time of writing there have been few publications of its use in plastic surgery applications
Quill Device
Since the development of the early barbed suture devices described above barbed suture technology has progressed to the development of both absorbable and nonabsorbable bidirectionally barbed sutures with barbs arranged in opposing directions on either side of an unbarbed segment (ie the Quill device)22 This device is armed with a surgi-cal needle on each end Absorbable materials for the device include polydioxanone (PDO) and Monoderm (Angiotech Pharmaceuticals Inc) a polyglycolide-poly-e-caprolactone copolymer (Figure 5) Nonabsorbable mate-rials include nylon and polypropylene A novel helical design in the placement of the barbs supports the concept of better tissue adherence to the barbs (Figure 6) As with prior barbed suture configurations the goal of this new design was to avoid knot tying which has on occasion resulted in palpability of the knots Extensive preclinical testing was conducted to ensure that the tensile strength of the Quill materials provided sustained soft tissue approximation with an absorption curve compatible with the time required for neo-collagen formation to maintain the integrity of the soft tissue approximation10
The Quill Monoderm (Figure 5B) is the most recently available absorbable bidirectional barbed suture It is designed for placement in the mid-dermis Compared with Quill PDO the Quill Monoderm has a more rapid absorp-tion curve and eliminates the exposureextrusion issue
that has been seen when larger diameter PDO sutures are placed too superficially in the dermis
Barb morphology influences holding and tensile strength The deeper the barb is cut the lower the tensile strength Therefore with the Quill device it is important to select a suture size that is 1 thickness above the size of any conventional suture For example in cases where a 2-0 absorbable conventional suture would have been used a 0 bidirectional barbed suture should be used to account for the difference in the strength of the suture material
In my experience both midface and brow elevation can be maintained with absorbable bidirectional barbed sutures but as expected patients with the most favorable anatomy (eg low body mass index minimal fullness to the soft tissues strong underlying bony projection to sup-port the elevated tissue good skin quality) have shown the best results and most commonly extensive soft tissue dissection has been required to ensure that elevated soft tissue remains elevated2324 Specific techniques in aes-thetic facial plastic surgery that I have developed to take advantage of the unique properties of the Quill device are outlined below Unfortunately no large data sets of patient experience have been reported to date with this device in aesthetic facial plastic surgery As a result no objective outcome data accompany these descriptions My prefer-ence for the use of the bidirectional barbed device over conventional sutures for these procedures is based solely on anecdotal experience that better outcomes are achieved with the Quill barbed device
Quill Techniques
Suspension of the browIn this technique incisions are made behind the temporal hairline The temporal dissection proceeds on top of the deep temporal fascia releasing the periorbital lateral to
Figure 5 Absorbable bidirectional barbed sutures (A) The Quill SRS polydioxanone (PDO) device (B) The Quill Monoderm device Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

22S Aesthetic Surgery Journal 33(3S)
the supraorbital neurovascular bundle The bidirectional barbed suture is threaded onto a long Keith needle that is passed over the deep temporal fascia piercing the flap about 1 cm above the orbital rim exiting below the lowest brow hairs The second half of the suture is placed through the deep temporal fascia continuing above the plane of dissection then exiting the lowest brow hairs about 1 cm medial to the first suture The brow is lifted on the barbs of both suture halves until satisfactory correc-tion has been achieved The temporal incision is closed with skin clips after securing the superficial temporal fas-cia to the deep fascia with an absorbable suture (3-0 PDS
Ethicon Somerville New Jersey) (Figure 7) If the brows are symmetrical the opposite brow may be positioned the same way If there is asymmetry or if the tissues are heavy the ends of the sutures are left long and covered with an antibacterial ointment a nonadherent pad and sterile gauze Two to 3 days later the brow(s) may be further adjusted if necessary In the case of brow asymmetry the higher brow is positioned at the right level and the sutures are cut at the skin level in the operating room (OR) The lower brow height is adjusted in the OR and the suture ends are left long to be adjusted as needed a few days after surgery to achieve brow symmetry This allows further elevation only on the more ptotic side a few days later and avoids ldquochasingrdquo the other side in the clinic
Midface suspensionIn a technique for midface elevation similar to that of Hobar and Flood25 I have used a temporal access incision (similar to that described above for a lateral browlift) dis-sected over the malar bone and joined this with a trans-buccal approach (Figure 8) A suture was placed intraorally through the soft tissue over the malar bone and then passed out of the temporal access incision anchoring it to the deep temporal fascia (Figure 9) With conventional sutures this was at times quite tedious It also required more precision in placement to produce a symmetrical result and in a few cases resulted in a midface infection that required intraoral drainage The availability of the bidirectional absorbable barbed suture has allowed me to perform a much easier dissection one that requires little visualization and produces lasting improvement in elevat-ing and repositioning ptotic midface soft tissues (Figure 10) Using barbed sutures for midface lifting allows one to support the elevated tissues by passing the bidirectional barbed suture through all tissue planes exiting lateral to the nasolabial crease avoiding intraoral suture placement
PlatysmaplastyThe neck has always been challenging to correct when addressing facial aging I have utilized Joel Feldmanrsquos cor-set platysmaplasty to unite the platysmal muscles in the midline combined with pre- inter- and subplatysmal fat removal as indicated by the patientrsquos anatomy26 The advent of the bidirectional barbed absorbable PDO suture allows more finesse in suture placement and impressive cervicomental contouring Two or 3 permanent nylon sutures should be used at key points as an added support to the underlying corset (Figures 11 and 12)
Lateral neck suspensionThe bidirectional barbed device can similarly be anchored in the mastoid fascia One end is passed through the platysma muscle along the jawline exiting the skin in the submental area The second half of the suture parallels the first half and may support a ptotic submaxiallary gland The central neck skin is advanced on the barbs to tighten the upper neck (Figure 13)
Figure 6 Gradients of tension and compression created with the bidirectional barbed suture (A) Linear compression at the point where the barbs change direction (B) Arcuate placement imparts a mound by adding a vertical vector to the horizontal vector (C) U-shaped deployment results in the forces on the barbs being opposed by the bend in the U rather than by the opposing barbs From Ruff10 Reprinted with permission from Sage Publications
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 23S
Lateral SMASectomyOne of the most frequently performed procedures for face lifting is the lateral SMASectomy27 Bidirectional barbed absorbable sutures allow secure plication of the mobile to the nonmobile SMAS and allow ldquoanywhererdquo suture placement that will enhance results Avoiding knots is valuable as is the availability of an absorbable polymer (Figure 14)
MACS liftAnother frequently performed facelift technique is the minimal access cranial suspension (MACS) lift28 This technique utilizes a purse-string suture beginning and ending with anchor points in the deep temporal fascia in front of the ascending helix Utilizing the bidirectional barbed PDO suture there is no need for a purse string to achieve the desired result Therefore there is no knot tying nor is there the bunching of the soft tissue that fre-quently requires trimming and the placement of a layer of sutures to control shape (Figure 15)
Basic wound closure techniques with the Quill deviceEmerging applications for barbed sutures in wound closure followed the availability of bidirectional barbed sutures in both absorbable and nonabsorbable materials Fundamental to an understanding of the application of bidirectional barbed sutures to wound closure are the basic wound clo-sure techniques utilizing these devices It is my opinion that the learning curve with this technology is short requiring the completion of only 1 to 2 cases to achieve competency in the closure techniques outlined below
Simple wound closure If the wound includes only the full thickness of the skin and subcutaneous fat a single bidi-rectional barbed suture can be started in the middle of the wound Each half travels to opposite ends of the wound The needle exits the skin 1 cm lateral to the end of the inci-sion on each side (Figure 16)
Multilayered skin closure A multilayered closure is neces-sary when the wound includes the full thickness of the
Figure 7 Browlift procedure with the bidirectional barbed suture showing (A) the area of dissection (B) placement of the threads and (C) anchoring of the threads From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

24S Aesthetic Surgery Journal 33(3S)
skin subcutaneous fat and superficial fascia (deep fat may be included) First the deep layer is closed utilizing the bidirectional barbed suture At each end of the wound the needle is passed in a J-loop to ensure good wound
approximation Then the full-thickness skin incision is closed as described above (Figure 17)
Figure 8 Transtemporal and intraoral incisions for the midface lift From Paul24 Reprinted with permission from Sage Publications
Figure 9 (A) Passage of the bidirectional barbed suture from the temporal area exiting lateral to the nasolabial crease (B) Volumetric stacking of soft tissue (the ldquoshish kebabrdquo effect) SMAS superficial musculoaponeurotic system SOOF suborbicularis oculi fat From Paul24 Reprinted with permission from Sage Publications
Figure 10 (A) A 37-year-old woman shown preoperatively (B) Five months after open subperiosteal browlift and midface lift with the bidirectional barbed suture From Paul34 Reprinted with permission from Springer-Verlag
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 25S
Closure of wounds with excessive tension In cases where there is excessive tension the wound can be closed in 2 directions First a bidirectional barbed suture with a short straight needle is passed at right angles to the wound and exits the skin The opposite end of the suture is passed in the opposite direction Having been divided into equal seg-ments the wound is then closed at right angles to the wound with several of the short sutures on the straight needle After the right angle tension is adjusted the stand-ard closure is performed as described above (Figure 18)
Aesthetic plastic surgery wound closure applications with the Quill deviceHaving mastered the routine closures one can move on to utilizing this technology in closing incisions in aesthetic plastic surgery including breast and body contouring applications which may bring with it benefits such as shorter operating time
To provide convincing evidence that fewer sutures were required and the operating time was shortened when bidi-rectional barbed sutures were deployed in aesthetic plastic surgery procedures I measured time for incision closure in a single cadaver29 Procedures included closure of brachio-plasty mastopexy and abdominoplasty incisions Separate surgeons performed each of the 3 procedures Closure of a single half of the cadaver (breast arm abdomen) was performed with a bidirectional barbed suture (Quill PDO device) Serving as the control arm closure of the other matched half of the cadaver was performed by the same surgeon with absorbable standard sutures (eg Vicryl Ethicon) In every case the operating time was shortened with the use of the bidirectional barbed closure technique (Figure 19) This is an important consideration since shorter operating times translate to cost savings for the patient and may allow the surgeon to add another case on the same day if so desired
The following aesthetic plastic surgery procedures have been found to be appropriate for utilization of the bidirectional barbed suture technology
Mastopexy Using the Quill PDO device the deep dermis can be closed around the areola One half of the suture begins at 12 orsquoclock and travels clockwise to the 6-orsquoclock position
Figure 11 Platysmaplasty performed with the bidirectional barbed suture showing midline placement with platysma backcut From Paul23 Reprinted with permission from Elsevier
Figure 12 (A) A 60-year-old woman is shown preoperatively (B) Two months after open face- and necklift with superficial musculoaponeurotic system (SMAS) flap and midline platysmaplasty performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

26S Aesthetic Surgery Journal 33(3S)
The other half of the suture travels the same distance coun-terclockwise The sutures can be continued down the vertical limb and each half can continue in opposite directions to close the inframammary incision if indicated for breast shap-ing Going the full distance requires a suture 24 cm to 30 cm long so that enough suture length is available to close the incisions with one suture The mid- and superficial dermis is closed in a similar manner with the Quill Monoderm device which is used instead of Monocryl (poliglecaprone 25 Ethi-con) (Figure 20) In patients with a thin dermis a 1-layer closure with the Monoderm is indicated to avoid the possibil-ity of extrusion of barbed segments with a longer lasting polymer (ie Quill PDO)
Reduction mammaplasty The pedicle can be supported to the pectoralis fascia with a larger diameter 0 or 1 PDO or nonabsorbable barbed suture This allows firm fixation of the pedicle and may decrease the chance for late ldquobottoming outrdquo of the breast The incisions are closed the same as for a mastopexy Interestingly the even distribution of tension along the incisions may result in better scar cosmesis and a lesser tendency for dehiscence of the tension point where the medial and lateral breast flaps are brought to the inframammary incision line (an area prone to dehiscence and delayed healing)
Figure 13 Lateral neck contouring with the bidirectional barbed sutures (A) Placement of the sutures (B) A 40-year-old woman is shown preoperatively (B) Three months after subperiosteal browlift and midface lift with barbed sutures liposuction of the jawline and barbed suture suspension and chin augmentation From Paul23 Reprinted with permission from Elsevier
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 27S
Abdominoplasty Extensive experience with the bidirec-tional barbed device in abdominoplasty has convinced me that there are clear advantages to using this technology The midline diastasis recti and periumbilical hernias can
be securely approximated and repaired quickly To perform the repair a larger diameter 1 nylon barbed suture is passed from the fascia adjacent to the umbilicus to the xiphoid The other half travels from the umbilicus to the
Figure 14 Lateral SMASectomy performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 15 Minimal access cranial suspension (MACS) technique performed with the bidirectional barbed suture From Paul23 Reprinted with permission from Elsevier
Figure 16 A simple wound closure technique utilizing the bidirectional barbed suture (A) Begin by taking one end of the suture and pulling it through until the transition zone has reached the tissue Estimation of the center of the device can be aided by taking a single bite of tissue then aligning the needles until both ends of the suture are of roughly equal lengths (B) Taking one arm of the suture complete at least 2 loose arcs through the tissue then takes a few tissue bites with the other arm of the device (C) Once at least 2 arcs per side have been deployed each of the strands can be grasped and the tissue approximated to the desired tension Continue the bites sinusoidally until the end of the wound is reached (D) Take the last bite 2 cm beyond the end of the wound exiting through the skin Repeat the technique on the opposite side Complete the procedure by pushing down on the tissue and cutting the device and needle flush with the skin Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

28S Aesthetic Surgery Journal 33(3S)
Figure 17 Multilayered wound closure technique utilizing the bidirectional barbed suture (A) Begin the wound closure with a Quill PDO suture of appropriate size Place the suture in the superficial fascia at the midpoint of the wound pulling the suture until it locks due to barbs facing the opposite direction (B) Continue suture placement in a sinusoidal fashion until the end of the wound is reached (C) Then reverse the direction of the needle placing it under the last suture loop and continue in a J-loop fashion to secure the closure (D) Then complete the wound closure as described in Figure 16 From Paul and Budd29 Reprinted with permission from Allied Media
Figure 18 Closure technique for wounds with excessive tension utilizing the bidirectional barbed suture (A) Mark the vector lines of the suture at 5-cm intervals Insert the needle from either side of the wound through the full thickness of the wound exiting the skin at least 3 cm from the border of the wound (B) Hold tension on the device and ratchet the wound edges close together (C) Repeat the procedure until the wound is an optimal size Close the wound in layers as shown in Figure 17 Copyright 2011 Angiotech Pharmaceuticals Inc Reprinted with permission
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 29S
suprapubic incision This is followed with a second row using 1 or 0 PDO (Figure 21) I have demonstrated the strength of this closure in the cadaver laboratory where a midline laparotomy incision was closed in layers with the bidirectional barbed suture and the incision could not be dehisced when pressure was applied from behind the clo-sure (data unpublished) If a high-tension lateral abdominoplasty is preferred the barbed sutures can be used to apply evenly distributed tension to the lateral aspect of the flap anchoring the flap to the deep fascia This may take the place of basting sutures which are important in reducing incision-line tension At the same time by eliminating the dead space the incidence of seroma formation is reduced A larger diameter (1 or 0
PDO) is useful for this purpose The effectiveness of this progressive tension quilting suture technique to close the dead space and thus reduce the risk of seroma formation was first established more than 13 years ago by Baroudi and Ferreira30 and later by Pollock and Pollock3132
The transverse abdominoplasty incision can be closed in 2 layers with the deep layer including Scarparsquos fascia closed with a 0 or 2-0 PDO device The deep dermis is closed with a 3-0 Monoderm device A few 3-0 nylon sutures are placed to set up the closure and add addi-tional support in areas of tension which are important in patients who are encouraged to ambulate soon after the abdominoplasty procedure is performed (Figure 21) If a seroma develops the wound can be readily opened by cutting the device in the nonbarbed middle segment Each device arm can then be pulled out from the distal end
Bodylifting In a similar manner as described for abdomi-noplasty the extensive incisions required in postbariatric surgery skin envelope reduction and shaping can be closed more securely and quickly with bidirectional barbed sutures
Brachioplasty Prone to scar widening this incision can easily be closed in layers with bidirectional sutures One can choose to add additional barbed sutures at a right angle to allow distribution of tension in 2 directions
concluSionS
Thought and process in the emerging technology of barbed sutures has evolved from procedures that were ineffective and prone to complicationsmdashincluding relapse palpability and extrusionmdashto reliable methods to reposi-tion dissected and mobilized soft tissues of the aging brow face and neck The bidirectional barbed Quill Knotless Tissue-Closure Device with a helical barb design
Figure 19 Mean time to closure with bidirectional barbed suture and traditional suture techniques In this series traditional and barbed suture abdominoplasty brachioplasty and mastopexy closures were performed using a single cadaver Each procedure required closure of 3 layers the superficial fasciadeep tissue deep dermis and superficial dermis Closures were performed by a junior plastic surgery resident a senior plastic surgery resident and a senior plastic surgery professor each serving as his own control From Paul22 Reprinted with permission from Elsevier
Figure 20 Mastopexy closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

30S Aesthetic Surgery Journal 33(3S)
and available in absorbable and nonabsorbable polymers has allowed this technology to be applied to longer inci-sions that carry varying soft tissue loads Controlling ten-sion along the incision line has always been the goal of any wound closure It is my experience that the Quill device decreases the incidence of wound dehiscence and subsequent unfavorable scarring The observation that wound closure times are shortened that fewer sutures are required and that many of the scars may be better in appearance than scars resulting from standard wound clo-sure techniques has led to widespread adoption of this technology Both patients and surgeons are the beneficiar-ies of the value added by use of bidirectional barbed sutures
disclosures
Dr Paul is currently employed on a part-time basis as a consul-tant for Angiotech Pharmaceuticals Inc (Vancouver British Colombia Canada) He receives a consultant fee and holds stock options
funding
Publication of the articles in this supplement was supported by a grant from Surgical Specialties Corporation but the
authors did not receive any direct compensation for writing the manuscripts
rEfErEncES
1 Villa MT White LE Alam M Yoo SS Walton RL Barbed sutures a review of the literature Plast Reconstr Surg 2008121102e-108e
2 Atiyeh BS Dibo SA Costagliola M Hayek SH Barbed sutures ldquolunch timerdquo lifting evidence-based efficacy J Cosmet Dermat 20109132-141
3 Sulamanidze MA Shiffman MA Paikidze TG et al Face-lifting with APTOS threads Int J Cosmet Surg Aesthetic Dermatol 20014275-280
4 Sulamanidze MA Fournier PF Paikidze TG Sulamanidze GM Removal of facial soft tissue ptosis with special threads Dermatol Surg 200228367-371
5 Sulamanidze MA Paikidze TG Sulamanidze GM Neigel JM Facial lifting with ldquoAPTOSrdquo threads featherlift Oto-laryngol Clin North Am 2005381109-1117
6 Lycka B Bazan C Poletti E Treen B The emerging tech-nique of the antiptosis subdermal suspension thread Dermatol Surg 20043041-44
7 Wu WTL Barbed sutures in facial rejuvenation APTOS threads and the WOFFLES LIFT Aesthetic Surg J 200424582-587
Figure 21 Abdominoplasty closure performed utilizing the bidirectional barbed suture From Paul and Budd29 Reprinted with permission from Allied Media
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from
Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from

Paul 31S
8 Sulamanidze M Sulamanidze G APTOS suture lift-ing methods 10 years of experience Clin Plastic Surg 200936281-306
9 Mulholland RS Paul MD Lifting and wound closure with barbed sutures Clin Plastic Surg 201138521-535
10 Ruff G Techniques and uses for absorbable barbed sutures Aesthetic Surg J 200626620-628
11 Murtha AP Kaplan AL Paglia MJ et al Evaluation of a novel technique for wound closure using a barbed suture Plast Recontr Surg 20061171769-1780
12 Leung JC Barbed suture technology recent advances Paper presented at Medical Textiles 2004 Conference Proceedings October 26-27 2004 Pittsburg PA
13 Abraham RF DeFatta RJ Williams EF III Thread-lift for facial rejuvenation assessment of long-term results Arch Facial Plast Surg 200911178-183
14 Garvey PB Ricciardelli EJ Gampper T Outcomes in threadlift for facial rejuvenation Ann Plast Surg 200962482-485
15 Rachel JD Lack EB Larson B Incidence of complica-tions and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting Dermatol Surg 201036(3)348-354
16 DeLorenzi CL Barbed sutures rationale and technique Aesthetic Surg J 200626223
17 Mulholland RS The composite barbed suture lift of the brow and midface Paper presented at Canadian Society of Aesthetic Plastic Surgery Meeting September 16 2006 Toronto Canada
18 Mulholland RS Advances and updates in barbed suture composite facelifts Paper presented at IMCAS January 9-12 2008 Paris France
19 Isse N Silhouette sutures for treatment of facial aging facial rejuvenation remodeling and facial tissue support Clin Plastic Surg 200835481-486
20 Gamboa GM Vasconez LO Suture suspension technique for midface and neck rejuvenation Ann Plast Surg 200962478-481
21 Wu W Innovative uses of BOTOX and the WOFFLES LIFT In Panfilov D ed Aesthetic Surgery of the Facial Mosaic Berlin Germany Springer 2006636-649
22 Paul MD Bidirectional barbed sutures for wound closure evolution and applications J Am Coll Certif Wound Spec 2009151-57
23 Paul MD Barbed sutures for aesthetic facial plastic surgery indications and techniques Clin Plastic Surg 200835451-461
24 Paul MD Using barbed sutures in opensubperiosteal midface lifting Aesthetic Surg J 200626725-732
25 Hobar PC Flood J Subperiosteal rejuvenation of the midface and periorbital area a simplified approach Plast Reconstr Surg 1999104842-851
26 Feldman J Necklift St Louis MO Quality Medical Pub-lishing 2006
27 Baker DC Lateral SMASectomy Plast Reconstr Surg 1997100509-513
28 Tonnard P Verpaele A Monstrey S et al Minimal access cranial suspension lift a modified S-lift Plast Reconstr Surg 20021092074-2086
29 Paul MD Budd M Evaluating the Quill self-retaining sys-tem closure time cost analysis and current clinical appli-cations PlasticSurgeryPracticecom 200930-33
30 Baroudi R Ferreira CA Seroma how to avoid it and how to treat it Aesthetic Surg J 199818439-441
31 Pollock H Pollock T Progressive tension sutures a tech-nique to reduce local complications in abdominoplasty Plast Reconstr Surg 20001052583-2586
32 Pollock T Pollock H Progressive tension sutures in abdominoplasty Clin Plast Surg 200431583-589
33 Kress DW The history of barbed suture suspension applications and visions for the future In Shiffman MA Mirrafati SJ Lam SM eds Simplified facial rejuvenation Berlin Germany Springer-Verlag 2008247-256
34 Paul MD Barbed sutures in aesthetic facial plastic surgery evolution of thought and process In Eisenmann-Klein M Neuhann-Lorenz C eds Innovations in Plastic and Aesthetic Surgery Berlin Germany Springer-Verlag 2008235-243
by guest on July 20 2016httpasjoxfordjournalsorg
Dow
nloaded from