Advanced Review Drug-eluting stent coatings
12
Advanced Review Drug-eluting stent coatings Judit E. Puskas, 1∗ Lyn G. Mu ˜ noz-Robledo, 1 Robert A. Hoerr, 2 John Foley 2 , Steven P. Schmidt 3 , Michelle Evancho-Chapman 3 , Jinping Dong 4 , Chris Frethem 4 and Greg Haugstad 4 This paper reviews the development of coronary stents from a polymer scientist’s view point, and presents the first results of an interdisciplinary team assembled for the development of new stent systems. Poly(styrene-b-isobutylene-b-styrene) block copolymer (SIBS), a nanostructured thermoplastic elastomer, is used in clinical practice as the drug-eluting polymeric coating on the Taxus coronary stent (trademark of Boston Scientific Co.). Our group has been developing new architectures comprising of arborescent (dendritic) polyisobutylene cores (D SIBS), which were shown to be as biocompatible as SIBS. ElectroNanospray (Nanocopoeia Inc. ) was used to coat test coupons and coronary stents with selected D S IBS polymers loaded with dexamethasone, a model drug. The surface topology varied from smooth to nanosized particulate coating. This paper will demonstrate how drug release profiles were influenced by both the molecular weight of the polyisobutylene core and spraying conditions of the polymer-drug mixture. 2009 John Wiley & Sons, Inc. WIREs Nanomed Nanobiotechnol INTRODUCTION T his interdisciplinary paper intends to discuss drug- eluting coronary stents (DES) and novel stent coatings mostly from the perspective of a polymer scientist who has been involved in the development of a polymer currently in clinical practice. Developing improved polymeric coatings will require close col- laboration between medical professionals and experts in natural science and engineering. Communication is critical but difficult when even the vocabulary is vastly different. This paper first will give an overview of the history of stent development, followed by a glimpse into the first results coming from our interdisciplinary group. It is not intended to be an exhaustive review, and it may be lacking from some perspectives. It is hoped, however, that it will contribute to a Additional Supporting Information may be found in the online version of this article. ∗ Correspondence to: [email protected] 1 The University of Akron, Akron, OH 44325-3909, USA 2 Nanocopoeia, Inc., St. Paul, MN 55104, USA 3 Division of Surgical Research, Summa Health System, Akron, OH 44304, USA 4 Characterization Facility, University of Minnesota, 12 Shepherd Labs, 100 Union St. SE, Minneapolis, MN 55455, USA DOI: 10.1002/wnan.038 better understanding of this topic, and hence some terminology will be ‘translated’ for the benefit of all. Overview of coronary stents Coronary stents revolutionized interventional cardiol- ogy to treat the narrowing of coronary arteries caused by the build-up of atherosclerotic plaque (heart dis- ease), which is the leading cause of death for both women and men in the United States. 1–7 If this con- dition goes untreated, it can result in heart attacks or angina (pain in the chest, arms, or lower jaw that occurs when insufficient blood flows to the heart muscle). Before Andreas Gr ¨ untzig introduced balloon angioplasty to treat arterial narrowings in 1977, 8 bypass grafts utilizing the patient’s own arter- ies were used. During angioplasty (some prefer the term ‘percutanueous transluminal coronary angio- plasty’ or PTCA) a balloon-tipped catheter is inflated inside the artery (Figure 1(a) and (b)). Stretching the intima (innermost layer of an artery) causes injury, leaving a ragged interior surface after deflation of the balloon, which triggers a healing response. A signif- icant problem is the elastic recoil or collapse of the artery after stretch injury. This collapse can occur during the procedure after the balloon is deflated and also after the angioplasty when the patients are in the recovery room. After such a collapse, the only option for the patient is emergency bypass graft surgery to 2009 John Wiley & Sons, Inc.
Transcript of Advanced Review Drug-eluting stent coatings

Advanced Review
Drug-eluting stent coatingsJudit E. Puskas,1∗ Lyn G. Munoz-Robledo,1 Robert A. Hoerr,2 JohnFoley2, Steven P. Schmidt3, Michelle Evancho-Chapman3, JinpingDong 4, Chris Frethem4 and Greg Haugstad4
This paper reviews the development of coronary stents from a polymer scientist’sview point, and presents the first results of an interdisciplinary team assembledfor the development of new stent systems. Poly(styrene-b-isobutylene-b-styrene)block copolymer (SIBS), a nanostructured thermoplastic elastomer, is used inclinical practice as the drug-eluting polymeric coating on the Taxus coronarystent (trademark of Boston Scientific Co.). Our group has been developingnew architectures comprising of arborescent (dendritic) polyisobutylene cores(D SIBS), which were shown to be as biocompatible as SIBS. ElectroNanospray(Nanocopoeia Inc.) was used to coat test coupons and coronary stents withselected DSIBS polymers loaded with dexamethasone, a model drug. The surfacetopology varied from smooth to nanosized particulate coating. This paper willdemonstrate how drug release profiles were influenced by both the molecularweight of the polyisobutylene core and spraying conditions of the polymer-drugmixture. 2009 John Wiley & Sons, Inc. WIREs Nanomed Nanobiotechnol
INTRODUCTION
This interdisciplinary paper intends to discuss drug-eluting coronary stents (DES) and novel stent
coatings mostly from the perspective of a polymerscientist who has been involved in the developmentof a polymer currently in clinical practice. Developingimproved polymeric coatings will require close col-laboration between medical professionals and expertsin natural science and engineering. Communication iscritical but difficult when even the vocabulary is vastlydifferent. This paper first will give an overview of thehistory of stent development, followed by a glimpseinto the first results coming from our interdisciplinarygroup. It is not intended to be an exhaustive review,and it may be lacking from some perspectives.It is hoped, however, that it will contribute to a
Additional Supporting Information may be found in the onlineversion of this article.∗Correspondence to: [email protected] University of Akron, Akron, OH 44325-3909, USA2Nanocopoeia, Inc., St. Paul, MN 55104, USA3Division of Surgical Research, Summa Health System, Akron, OH44304, USA4Characterization Facility, University of Minnesota, 12 ShepherdLabs, 100 Union St. SE, Minneapolis, MN 55455, USA
DOI: 10.1002/wnan.038
better understanding of this topic, and hence someterminology will be ‘translated’ for the benefit of all.
Overview of coronary stentsCoronary stents revolutionized interventional cardiol-ogy to treat the narrowing of coronary arteries causedby the build-up of atherosclerotic plaque (heart dis-ease), which is the leading cause of death for bothwomen and men in the United States.1–7 If this con-dition goes untreated, it can result in heart attacksor angina (pain in the chest, arms, or lower jawthat occurs when insufficient blood flows to theheart muscle). Before Andreas Gruntzig introducedballoon angioplasty to treat arterial narrowings in1977,8 bypass grafts utilizing the patient’s own arter-ies were used. During angioplasty (some prefer theterm ‘percutanueous transluminal coronary angio-plasty’ or PTCA) a balloon-tipped catheter is inflatedinside the artery (Figure 1(a) and (b)). Stretching theintima (innermost layer of an artery) causes injury,leaving a ragged interior surface after deflation of theballoon, which triggers a healing response. A signif-icant problem is the elastic recoil or collapse of theartery after stretch injury. This collapse can occurduring the procedure after the balloon is deflated andalso after the angioplasty when the patients are in therecovery room. After such a collapse, the only optionfor the patient is emergency bypass graft surgery to
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
Stent deployed
CollapsedBallonCatheter Dilated
ballon catheter
Dilatedballoncatheterand stent
Plaque
(a) (b) (c) (d)
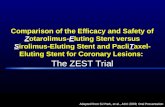
FIGURE 1 | Balloon angioplasty and stenting (Reprintedwith permission from www.applesnail.net Copyright 2007Boston Scientific Corporation).
repair the problem. Moreover, ∼30% of all coronaryarteries begin to ‘restenose’ (close back) as a result ofcellular proliferation in response to the stretch injury.In other words, overstretch shearing of the diseasedwall with PTCA leads to vascular spasm and, in someinstances, severe vessel wall weakening or dissection,both of which could require emergent salvage revas-cularization. By the mid-1980s, various cardiologistsand radiologists were working on solutions to theseproblems, designing new devices that would providemore safety and durability to the procedures. Onesuch device was the stent—an expandable metal tubeor ‘scaffold’. The metallic stents are crimped onto aballoon-tipped catheter and positioned in the coro-nary artery at the site of the narrowing (Figure 1(b)).The balloon is inflated, and the stent expands andpresses against the arterial wall (Figure 1(c)). Theballoon is deflated and removed. The stent remainspermanently in place, helping to keep the artery open(Figure 1(d)). Within a few weeks, new tissue willgrow over the stent. In 1985, Palmaz et al. implantedthe first balloon-mounted stent in a peripheral artery.9
Others in Europe were developing their own designs.In 1986, Puel and Sigwart10 inserted the first stentinto a human coronary artery. With the modificationsby Schatz et al. of the original Palmaz stent,11 the firstcoronary stent became commercially available in theUnited States (Palmaz–Schatz stent). The first devicewas implanted in 1987 at Brooke Army Medical Cen-ter. In 1994 the Palmaz–Schatz stent was approvedfor use in the United States.12 Since their approval,over 1.5 million coronary stents have been implantedinto patients each year. Over the years, several gen-erations of bare metal stents (BMSs) were developed,and it has been shown that they can significantlydecrease the chance of vessel restenosis at the site oftreatment. However, ∼20–30% of patients still devel-oped significant scar formation at the site of the stentplacement, which in turn caused restenosis.7 Thus the
introduction of these bare metal endoluminal scaf-folds, i.e., stents, provided a convenient and effectiveapproach to prevent acute arterial closure followingPTCA, but the technique was plagued by a 30%restenosis rate within 6 months, resulting from anexuberant vascular tissue neointimal growth aroundthe stent and within the lumen. Many investigatorshave tried to prevent restenosis by administering drugssystematically, but this has had little success despitepromising preliminary work in animal models. A newsolution to the problem of restenosis has been thedevelopment of DES.2–5,13 DES are made by coatinga standard coronary stent with a thin polymer filmcontaining a drug, which is released in controlledamounts directly into the region of the injury, therebypreventing the formation of scar tissue at the site ofcoronary intervention. BMS reduce the incidence ofclinically significant restenosis by expanding the ves-sel lumen area; restenosis still occurs in virtually allinstances. With DES, the remodeling is often positive(vessel expansion) because the vessel wall retracts fromthe stent because of the drugs. Comparative studieshave shown that DES are better than BMS for treat-ing coronary diseases.13–16 For example, the Taxus(coronary stent trademark of Boston Scientific Co.) Vclinical trial reported 13.7% verus 31.9% restenosiswith DES and BMS, respectively.14 Since the Food andDrug Administration (FDA) approval of the first DES,the market has grown explosively. The current U.S.market is dominated by two DES: the Taxus by BostonScientific Co. (BSC) and the Cypher (Coronary stenttrademark of Johnson&Johnson Inc.) by Johnson &Johnson Inc. (J&J) The worldwide market was pre-dicted to reach 6.1 billion by 2010. Table 1 comparesvarious DES technologies under development.
2009 John Wiley & Sons, Inc.

WIREs Nanomedicine and Nanobiotechnology Drug-eluting stent coatings
TABLE 1 DES Technologies
Manufacturer Trade name Stent Polymer Drug
Abbott ZoMaxx Tantalum/SS Durable Zotarolimus
Boston Scientific Taxus SS Durable Taxus
Cordis J&J Cypher Cobalt chromium/SS Durable Sirolimus
Guidant Champion SS Bioabsorbable Everolimus
Terumo Nobori SS Bioabsorbable Biolimus-A9
SS, Stainless steel.
Polymers used in drug eluting stentsThe biocompatibility of the polymers used for coatingstents in contact with the blood is vital. Biocom-patibility is hard to define, especially for a polymerscientist, but the term describes how cells respondbiologically to the presence of a material in theirenvironment.17 The polymer must not stimulate aninflammatory response. In addition, for DES applica-tions it must be capable of being stretched withoutflaking or delaminating. Secondly, the polymer needsto be able to deliver the drug at a sustained, con-trolled, and predictable rate. Only a few polymersmeet these requirements. These polymers may bebiodegradable or non-biodegradable (durable). Somebiodegradable polymers investigated as coatings instents include polyglycolic or polylactic acid or theircopolymers, and poly(ethylene glycol-block-ethyleneterephthalate). Examples of durable polymers testedin DES are methacryloyl phosphorylcholine–lau-rylmethacrylate, poly(ε-caprolactone), poly(ethyleneterephthalate), silicone, and polyurethane.18 Theexact polymeric compositions are usually propri-etary. Unfortunately, the polymers listed above haveshown less than optimal biocompatibility in a porcinemodel.18,19 Polyurethanes are classified as ‘durable’but in fact they are not biostable over an extendedperiod of time and the degradation products havebeen shown to be toxic.20 However, thermoplasticpolyurethanes with shape memory properties wereinvestigated as DES.21
Pinchuk recently advanced a hypothesis ofbiostability and biocompatibility on the basisof the analysis of the degradation mechanism ofpolyurethanes combined with an understanding oforganic chemistry principles.18 According to thishypothesis, the long-term stability of a polymericmaterial in living tissue can be jeopardized when thepolymer contains unprotected ester, amide, ether, car-bamate, urea, or any other groups that are proneto oxidation, hydrolysis, or enzymatic cleavage. Fur-ther, secondary carbon-containing polymers such aspolyethylene, and secondary and tertiary carbon-containing polymers such as polypropylene, are also
to be avoided, as double bond formation leads toembrittlement and stress-cracking. Clinical evidenceseems to support this hypothesis.
In addition to effective suppression of inti-mal growth, the ideal DES polymer shouldbe non-thrombotic, non-inflamatory, non-toxic tocells, and should encourage arterial healing byre-endotheliatization. Long-term safety and efficacyis important; therefore incidences of late thrombosisled to controversy over DES versus BMS, which willbe discussed in more detail in a later section.22
The two DES approved by the FDA employpoly(ethylene-co-vinyl acetate) (PEVA) and poly(n-butyl methacrylate) (PBMA) (J&J), and poly(styrene-b-isobutylene-b-styrene) (SIBS) (BSC).
DES approved by the FDAThe Cypher is manufactured by Cordis (J&J). Itis made of 316 L stainless steel (SS) (low-magnetic,low-carbon) and coated with a mixture of polymers(PEVA:PBMA 67:33) containing the sirolimus drug.A drug-free top coat of PBMA is also applied to thestent surface to control drug release.
Sirolimus is a natural macrocyclic lactone, whichis a fermentation product of Streptomyces hygro-scopicus originally identified in a soil sample fromPara Nui (Easter Island) to combat restenosis. Thisantibiotic has potent immunosuppressant propertiesand is used as an oral agent to prevent rejectionin patients who have undergone renal transplant.Furthermore, this drug has the ability to inhibitcytokine- and growth-factor-mediated proliferationof lymphocytes and smooth muscle cells.23 Severalstudies have been conducted with this drug and theresults were reportedly excellent. It was demonstratedthat for up to 24 months neointimal hyperplasia, asdetected by intravascular ultrasound, was virtuallyabsent, and there was no late thrombosis close tothe stent area. The Ravel Trial24 demonstrated thereduction of restenosis and associated clinical events.In addition to the Ravel study, the results of the Siriusstudy25 showed that after 9 months the patients whoreceived DES had significantly lower rates for repeat
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
procedures than those who received BMS (4.2% vs.16.8%).14 Thus, the FDA decided to approve thesestents on April 24, 2003.
The Taxus stent is made of 316 L SS andis coated with SIBS or Translute produced underlicense from the University of Akron, where SIBSwas invented,26 mixed with paclitaxel (PTx). PTx(Taxus brevifolia) was originally isolated from thebark of the Pacific yew tree and has been usedto treat several types of cancer (e.g., breast andovarian cancer). SIBS belongs to the family ofnovel thermoplastic elastomeric (TPE) biomaterialsbased on polyisobutylene (PIB) soft segments withphase-separated glassy (amorphous) domains suchas polystyrene (PS) or PS derivatives.26–40 In TPEs,nano-sized discrete glassy phases embedded in acontinuous elastomer phase provide ‘thermolabilecrosslinks’, giving rise to rubbery properties. TPEsdo not need to be chemically crosslinked like siliconerubber, and therefore offer many advantages overchemically crosslinked rubbers while being processibleas thermoplastics. SIBS is transparent and resemblessilicone rubber, whereas it is much stronger and hasbetter fatigue properties.
Multiple clinical trials have been performedto investigate the efficacy and the safety of thisstent,16,41–43 and because of the excellent results fromthese trials the FDA approved the use of the Taxusstent on March 6, 2004. Extensive testing in vitroand in vivo18,44 as well as clinical evidence showsthat this polymer has excellent vascular compatibility.In the smooth stent coating, the PTx was shown toexist as discrete particles, mostly in the PS domainsdue to weak π–π interactions between the aromaticrings of PS and PTx.45 The release kinetics of the drugfrom the polymer matrix was shown to correlatewith drug-to-polymer ratio. However, in vivo, atthe clinically relevant dosage only about 10% ofthe drug is eluted from the matrix in about 3 days,and the rest remains practically entrapped as a resultof the extreme impermeability of the polymer.44,45
Eventually, the entrapped drug will be released veryslowly by diffusion, which may take years, but‘permanent’ entrapment would be against the lawsof physics.
Stent controversyDES technology was the fastest introduction andscale-up of a combination medical device therapyever introduced. In late 2006, there were only twodomestic products approved by the FDA for usein the United States. Many more were poised forintroduction with international trials in progress.
Then, the market for the product crashed because ofunanticipated complications with the devices. Recentstudies indicate that the rapamycin- and PTx-elutingstents may be accompanied by rare, but serious, late-term thrombotic events.
In April 2003 FDA’s Manufacture and UserDevice Experience (MAUDE) (center received unfa-vorable event reports from patients implanted withDES. The problems associated with using the Taxusand Cypher stents were hypersensitivity (includingrashes), dyspnea (labored breathing), hives, and ana-phylaxis. Additionally, in other studies it was reportedthat patients were suffering thrombocytopenia (notenough platelets), itching, arthralgia (pain in thejoints), joint swelling, myalgia (muscle pain), or fever.These symptoms started within 1 day of the stentimplantation (20%), or manifested at later times(2–7 days (46%), 8–14 days (19%) and > 14 days(15%)).15,46–48 In spite of these problems, 88% ofpatients had favorable outcomes from the placementof DES—compared to BMS which have a higher per-centage of restenosis (∼40%)—and claimed DES tobe a better option. However, concerns were raisedthat while DES might reduce restenosis significantly inthe first few months, post-procedure (9–12 months)rates for DES and BMS were found to be essentiallythe same, and it was suggested that DES posed andan increased risk of thrombosis (ST-segment elevationand myocardial infarction) or death.46–49 However,it was pointed out that thrombosis was typicallyoccurring when the patient discontinued anticoagu-lant/antiplatelet therapy (the Swedish study47 did notinclude this factor).
Early thrombotic events are a well-knowncomplication of stent therapies. Combination anti-platelet regimens have reduced the incidence ofthese events from as high as 24% to below 1%for BMSs.50,51 DES were thought to be especiallysusceptible to late thrombosis events because ofdelayed re-endothelialization caused by the drugs.There are conflicting reports on whether or not thisis the case. Randomized trials of DES did not show adifference in thrombosis events at 1 year.52,53 Follow-up on patients from the initial clinical trials (4–5 years)has not shown any increased risk of major cardiacevents for DES versus BMS. However, these studieslack the statistical power to identify rare events.
Meta-analyses were performed in the hopeof gaining statistical significance by pooling dataacross multiple studies. It should also be notedthat meta-analysis studies are controversial, as therewere no consensus on the validity of makingpooled comparisons across existing methodologies.54
However, these studies are routinely reported in the
2009 John Wiley & Sons, Inc.

WIREs Nanomedicine and Nanobiotechnology Drug-eluting stent coatings
medical literature indicating general acceptance ofthe approach. The 1-year findings of no differencebetween DES and BMS were confirmed by meta-analyses.55,56 While the initial studies showed nodifference in thrombosis out to 1 year, other studiesat longer time points were conflicting. For example,in 2006 Pfisterer et al. reported that in patients whostopped anti-coagulation therapies, late thromboticevents were two to three times more frequent amongthose who had received DES than among those whohad received BMS and that these events carriedfour times greater risk of cardiac death/myocardialinfarction versus non-thrombosis-related events.57
Another important study suggested an increased rateof death or Q-wave myocardial infarction with DES.58
The Camenzind analysis was based on publishedstudies. However, another set of studies based on rawdata from the two major stent companies concludedthat long-term mortality did not differ for patientswith DES or BMS.59,60
What is one to make of all of this controversy?Consensus is emerging that the decision to implantBMS versus DES needs to be made after carefulconsideration of whether the benefits of a reductionin restenosis outweigh the potential risks of long-termanti-platelet treatment to prevent late thrombosis.61
BMS are an appropriate choice for some patientsbut not others. What is clear, however, is that thereis a need for new stent alternatives. The ideal stentcoating would be one that inhibits smooth muscle cellproliferation in response to the stenting injury whilepromoting rapid re-endothelialization. New polymers,drugs, and biological agents are being screened inpreclinical studies in the hope that the next-generationstents can alleviate potential pitfalls of the currentstents.
What is most surprising to the polymer scientistis that the long-term clinical effects of the polymerhave not been investigated separately. At presentthere is no evidence that the presence of the polymerleads to thrombosis, which happens with both theJ&J and BSC DES62 in spite of the very differentpolymers. Poly(isobutylene) has alternating secondaryand quaternary carbons and no labile pendantgroups, and hence the excellent biocompatibility andbiostability of SIBS-type biomaterials. In comparison,methacrylate polymers have unprotected ester sidegroups. The corresponding author of the present paperbelieves that the impermeability of the PIB may also bea contributing factor since enzymes cannot penetratethe film. On the other hand, this may lead to drugentrapment, as discussed before.
It would be ideal to have long-term clinical dataon the behavior of polymers used in DES coating,
or a comparative study involving BMS and stentscoated with the polymer in question. Barring thispossibility, the role of polymers in the controversyremains unclear.
Whatever the outcome of the controversy,62–64
it appears that the problems related to the first gener-ation of DES will inspire scientists to develop newtechnologies. This will necessitate close interdisci-plinary efforts among polymer and surface scientists,medical professionals, and clinicians.
A personal note from the corresponding author:most likely all polymers eventually suffer degradationin the body, and therefore the term ‘biodegradable’polymer appears to be an oxymoron. The differenceis only in the rate of degradation—one polymer maydegrade in vivo in a day, while another in 10 years.The real question is what the degradation productsare and how the body can deal with them. Therefore‘biodegradable stents’ may not be magic bullets either.
This paper will discuss the hypothesis thatthe synergistic combination of ElectroNanospraycoating technology65 and a new generation of SIBS-type polymers28,37,40 could open new avenues intocontrolled drug release in general and improved DEStechnologies in particular. We will present data of invitro drug release from the new generation of SIBScopolymers electronanosprayed with the model drugdexamethasone (DXM).
RESULTS AND DISCUSSION
New polymers for stent coatingWith the development of various controlled/livingpolymerization techniques, we are in the positionto synthesize a wide variety of architectures, e.g.,stars, brush-like chains, centipedes, dendritic (hyper-branched and arborescent) structures, self-assemblingblock copolymers, and supramolecular structures.Figure 2 compares the architecture of linear tri-blocks and dendritic (arborescent) blocks (DIBs forshort).37,39,40 Structurally, all these constructs com-prise a rubbery (soft) inner segment (core) bound totwo or more glassy (hard) outer segments (corona).The spatial arrangement of the rubbery/glassy moieties(i.e., linear, star, dendritic), the molecular parametersof the segments (i.e., molecular weight, Tg, relativeamounts of rubbery/glassy components, degree of seg-mental incompatibility), and the micro-morphologyof the constructs control the ultimate TPE propertiesand processibility. Macroscopically, these materialsare transparent rubbers. For our studies, we selectedto use three different DIBS: TPE1, TPE4, and TPE5,which differed in molecular weight, PS content, and
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
SIBS
D_SIBS all architectures
FIGURE 2 | Polyisobutylene (PIB)-based Thermoplastic elastomers(TPEs); architecture and macroscopic appearance, where = PIB and=glassy segments.
TABLE 2 Industrial Stent Coating Technologies
Method Comments
Atomization Single layer; large particle size
Dipping Inside coverage may be difficult
Ultrasound Single layer; large particle size
Inkjet printinga Difficult to get complete coverage
Gas-Phase Depositiona Not suitable for biodegradablepolymers
aSpecific applications.
the average number of PS blocks (see Table 3). Theaverage number of PS blocks at the end of each branchof the PIB was 3 and 4, but the high molecular weightfractions had up to 15–20 end blocks. These materialscan be synthesized very reproducibly and were foundto be as biocompatible as SIBS (to be published).
ElectroNanosprayCommonly used industrial coating methods suchas ion beam deposition, chemical vapor deposition,plasma vacuum technology, etc. are not compatiblewith the coating of DESs. Table 2 lists industrialtechnologies currently used for stent coating.
Electrohydrodynamic atomization, commonlycalled ‘electrospray’, has been used in traditionalapplications such as surface coating, agricultural treat-ments, emulsion or supermicron aerosol production,fuel spraying, micro-encapsulation, ink-jet printers,and colloid micro-thrusters. However, in this appli-cation we will be referring to a particular mode ofelectrospray operating in the ‘cone jet’ mode. In thismode it can be used to produce airborne nanoparti-cles from a solution or colloidal suspension of desired
drug loaded nanoparticles
target to be coated
solventevaporation
+
–
FIGURE 3 | Schematic of the ElectroNanospray process.
solute materials, typically in a size range of 2–100 nm,hence the term ‘ElectroNanospray’.65 In its simplestconfiguration, a syringe pump is used to deliver asolution or suspension into a capillary tube. The liq-uid exiting through the capillary tube is exposed to ahigh electric field established between the tip of thecapillary, to which a high voltage is applied, and atarget that is grounded or oppositely charged. Thenonuniform electric field causes the liquid meniscus toassume a conical shape (see Figure 3) established bythe balance between the surface tension force and theelectrical force on the cone. The liquid is dispensedthrough the cone tip in the form of a liquid jet ofnanometer diameter. The instability of the liquid jetcauses it to fragment into nanoparticles, each carryinga very high charge level—on the order of 80–90% ofthe Rayleigh limit. Since the particles are positivelycharged, they repel each other in the gas phase allow-ing solidification as discrete nanometer-sized objects.The key variables that govern particle size when theelectrospray is operated in the cone jet mode are theflow rate and the conductivity of the solution. Otherfactors, such as the diameter of the feed capillary, vis-cosity of the fluid, and volatility of the carrier solvent,also affect particle size. A unique configuration of thissystem is a spray nozzle comprised of coaxial cap-illaries. This configuration produces highly uniformparticles and provides significant process flexibility.The spray process can accommodate a broad range
2009 John Wiley & Sons, Inc.

WIREs Nanomedicine and Nanobiotechnology Drug-eluting stent coatings
TPE 4
TPE 1
TPE 5
FIGURE 4 | Scanning electron microscope images of continuous(5000 × magnification) and particulate (20,000 × magnification) filmssprayed onto SS plates.
of chemical and biological agents as well as multipleand potentially incompatible solvents. The ability tomerge streams at the spray tip enables particle engi-neering: for example, to give coated drug particles withcore–shell architecture. Spraying conditions have beendeveloped with more than 60 different solvents andseveral different model pharmaceutical compoundsand biomedically relevant polymer systems. Particlescan be delivered into liquid media or deposited ontosolid surfaces to produce nanocomposite films. Whenthe spray nozzle and cone jet are positioned near agrounded or oppositely charged target, the particlescan be collected in a dry, or nearly dry, or viscous liq-uid. This results in a variety of reproducible surfacesand drug-release profiles.
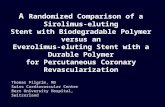
Figure 4 shows the scanning electron microscope(SEM) images of a smooth (continuous) and partic-ulate films with DXM sprayed onto SS plates. Thesmooth film of TPE4 shows ‘islands’ of DXM par-ticles on the surface, similar to the PTx particlesreportedly seen in the Taxus stent coating.45 The con-tinuous films sprayed with TPE1 and TPE5 seem tohave fully encapsulated/coated particles and no DXMexposed on the surface. The particulate films also seemto have encapsulated DXM, and the size of the fea-tures increases in the order of TPE4 < TPE1 < TPE5.
0102030405060708090
100
0 7 14 21 28
Days
DX
M %
C
umul
ativ
e re
leas
eD
XM
%
Cum
ulat
ive
rele
ase
DX
M %
C
umul
ativ
e re
leas
e
0102030405060708090
100
0 7 14 21 28
Days
010203040506070
8090
100
0 7 14 21 28
Days
(a)
(b)
(c)
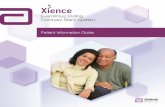
FIGURE 5 | DXM release from TPE4, TPE1 and TPE5.• smooth film;o particulate film.
These plates were used to obtain the release profilesshown in Figure 5.
Drug releaseThe smooth film of TPE4 showed a burst releaseof 20.3% in 6 h of the DXM loaded into the film,followed by a very slow release reaching 26.7% by day28 (Figure 5(a)). The particulate film of TPE4 showed3.3% burst release in 6 h, followed by continuousrelease reaching 23.2% by day 28. In the case ofTPE1, both films showed ∼3% burst release in 6 h,followed by a slower release reaching 20% by day 28(Figure 5(b)).
In case of TPE5, the continuous film showed lessburst release (2.6%) than the particulate film (6.3%).
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
Both films displayed gradual release, but the rate wasmuch slower for the continuous film. The cumulativerelease was ∼14% for the smooth film and 25% forthe particulate film in 28 days, see Figure 5(c). Table 4summarizes the drug release data.
Neither the burst nor the cumulative releasefrom either film correlated with the PS content ofthe blocks (Table 4). In spite of the nearly 10 wt%higher PS content of TPE4 than TPE1, the formerhad a higher cumulative release than the latter, incontrast to that reported for the Taxus stent where thedrug was shown to preferentially segregate in the PSphases where it remained trapped.45 However, boththe burst and cumulative release from the continuousfilms were inversely correlated with the Mn of thePIB inner core (Table 4). It can be theorized that moreDXM is being fully encapsulated by the materials withhigher molecular weight PIB. It has been demonstrated
by X-ray photoelectron spectroscopy analysis thatthe surface of PIB-based styrenic block copolymersis covered with a layer of pure PIB, on accountof its lower surface energy compared to PS.36 PIBhas very low permeability, so diffusion of the DXMfrom the matrix through the PIB layer is expected tobe slow. With increasing PIB molecular weight, thethickness of the outer PIB layer might increase, orhigher extensibility during electrospraying may leadto better encapsulation.
The high initial burst release in Taxus wasattributed to the drug particles exposed on thesurface.45 We have investigated this aspect using insitu confocal Raman spectroscopy. Figure 6 shows theRaman spectra of DXM and TPE4.
The carbonyl resonance of DMX at ∼1660 cm−1
and the alkyl group resonances (in both the PIB and PS,and-CH3 in the PIB) of the polymer at ∼2920 cm−1
TABLE 3 Properties of the D SIBS Used
ID Block Mn (kg/mol) Mw/Mn PS (wt%) PIB Mn (kg/mol) Avg. # PS blocks
TPE4 70 4.5 32.8 47 4.1
TPE1 110 2.4 23.1 85 3.2
TPE5 220 1.8 29.4 154 3.2
D SIBS, SIBS with a dendritic (branched) polyisobutylene core and polystyrene end blocks; Mw/Mn, Molecularweight distribution; Mn, Number average molecular weight, Da or g/mol.
TABLE 4 DXM Release from D SIBS
ID Block Mn (kg/mol) PIB Mn (kg/mol) PS wt% % Release
Smooth Particulate
Burst Total Burst Total
TPE4 70 47 32.8 20.3 26.7 3.3 23.2
TPE1 110 85 23.1 3.2 20.2 3.1 19.7
TPE5 220 154 29.4 2.6 14.0 6.3 26.7
D SIBS, SIBS with a dendritic (branched) polyisobutylene core and polystyrene end blocks; Mn, Numberaverage molecular weight, Da or g/mol.
3500300025002000150010005000
400
800
1200
1600
2000
2400
rel. 1/cm
CC
D c
ts
3500300025002000150010005000
340
360
380
rel. 1/cm
CC
D c
ts
FIGURE 6 | Raman spectra of DXM powder and a TPE4 film.
2009 John Wiley & Sons, Inc.

WIREs Nanomedicine and Nanobiotechnology Drug-eluting stent coatings
FIGURE 7 | Raman images (z and x–yscans) of TPE4/DXM smooth films.
Before incubation After 10 hrs incubation in water
DXMPolymerDXMPolymer
FIGURE 8 | Optical images of TPE4/DMX continuousfilms. Before incubation After 10 hrs incubation in water
Openmatrix
SmoothFilm
StainlessSteelPlate
FIGURE 9 | Hybrid coating.
were used to monitor changes due to incubation inpure water. Figures 7 and 8 summarize the findings.
In Figure 7, the left image is the cross-sectionscan of the film (scan size 30 × 6 µm2). The top darkregion is air, and the bottom dark region is the SSsubstrate. The middle bright region is the coatingfilm (∼4µm). Lateral scans were performed at threedifferent levels (three black lines corresponding tolateral planes close to the surface, in the middle of thefilm and close to the substrate). The two columns ofthe images on the right show the polymer and drugcontrast (brighter meaning higher concentration) fromthe three layers (scan size 30 × 30 µm2). The Raman
Continuous Particulate
FIGURE 10 | Stents coated with TPE4/DXM.
images in Figure 7 reveal that DXM particles (2–6 µm)are distributed evenly within the polymer film. After10 h incubation in pure water, holes appeared inthe polymer, from where the drug particles wereremoved. The optical images (Figure 8) also showthe presence of holes on the surface of the polymerfilm after incubation. In contrast, the surface of theparticulate TPE4/DXM coating shown in Figure 4appeared unchanged and did not become porous.These results support the conclusion that burst releasecomes from the drug particles exposed on the surface.Figure 9 shows a hybrid film of TPE4/DXM, with25% particulate film on top of the smooth coating.
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
Burst release was reduced to 10% from 20% mea-sured with the smooth coating, while the cumulativerelease decreased to 22.2% (only a 16% relative drop,see Table 4).
Figure 10 shows examples of coated stents.Coatings were remarkably uniform on both inter-nal and external surfaces with no visible webbing.DXM release profiles from coated stents were verysimilar to those from SS plates (Figure 5). Followingincubation in buffered saline for 28 h, the continuouscoating became porous, whereas the appearance ofthe particulate coating did not change.
The results presented here demonstrate that drugrelease profiles can be influenced by both the molecularweight of the dendritic PIB block of the polymer sam-ples and spraying conditions of the polymer–drugmixture. Future work will include precision synthe-sis of new biocompatible polymers and fine controlof drug release profiles via both bulk and surfacematerial properties. Polyisobutylene-based polymersas a platform will remain strong because of their inert-ness in the body. Search for more effective drugsor drugs with different modus operandi will alsocontinue.
ACKNOWLEDGEMENTS
This material is based upon work supported by the National Science Foundation under DMR-0509687 andSBIR Phase II: 0620563 and the National Institutes of Health SBIR Phase I: 1R43HL079690-01A1. The authorswould like to acknowledge the contribution of Reza Lalani to this work.
REFERENCES
1. Moses JW, Weisz G, Mishkel G, Caputo R,O’shaughnessey C, et al. Catheterization and cardiovas-cular interventions. Catheter Cardiovasc Interv 2007,70(4):505–512.
2. Fontos G. Drug eluting coronary stents. Orv Hetil2006, 147(43):2059–2066.
3. Sutton AGC, Campbell PG, Graham R, Price DJA,Gray JC, et al. One year results of the Middles-borough early revascularization to limit infarction(MERLIN) trial. Heart (British Cardiac Society) 2005,91(10):1330–1337.
4. Arjomand H, Turi Z, McCormick D, Goldberg S.Percutaneous coronary intervention: historical perspec-tives, current status, and future direction. Am Heart J2003, 146:787–796.
5. Jenkins NP, Predergast BD, Thomas M, Drug elutingcoronary stents. BMJ 2002, 325:1315–1316.
6. Bitl JA, Scwartz L, Serruys PW, Fischmann DL, Sav-age SP, et al. Coronary-Stent placement comparedwith balloon angioplasty. N Engl J Med 1995, 332:536–538.
7. Serruys PW, Jaegere PD, Kiemenij F, Macaya C,Rutsch W, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patientswith coronary artery disease. N Engl J Med 1994,331:489–495.
8. Gruntzig A. Transluminal dilatation of coronary-arterystenosis. Lancet 1978, 1(8058):263.
9. Palmaz JC, Richter GM, Noldge G, KauffmannGW, Wenz WDR. Intraluminal Palmaz stent implan-tation. First clinical case report on a balloon-expanded vascular prosthesis. Radiologe 1987, 27(12):560–563.
10. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappen-berger L. Intravascular stents to prevent occlusion andrestenosis after transluminal angioplasty. N Engl J Med1987, 316:701–706.
11. Erbel R, Schatz R, Dietz U, Nixdorff U, Haude M,et al. Balloon dilatation and coronary vascular stentimplantation. Z Kardiol 1989, 78(2):71–77.
12. Miller LA, Briscoe A, Bailey SR, Wright WT Jr, EbersoleDG. Care of the elective intracoronary stent patient.Crit Care Nurs Q 1996, 18(4):777–791.
13. Gerschlick AH, Baron J. Dealing with in-stent resteno-sis. Heart 1998, 79:319.
14. Morice MA, Serruys PW, Sousa JE, Fajadet J, HayashiEB, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revas-cularization. N Engl J Med 2002, 346:1773–1780.
15. Bhatia V, Bhatia R, Dhinkda SJ. Drug-eluting intra-coronary stents: Have we got the magic bullet.J Postgrad Med 2003, 49:291–296.
16. Stone GW, Ellis SG, O’Shaughnessy CD, et al.Paclitaxel-eluting stents vs vascular brachytherapy forin-stent restenosis within bare-metal stents the TAXUSV ISR randomized trial. JAMA 2006, 295:1253–1263.
2009 John Wiley & Sons, Inc.

WIREs Nanomedicine and Nanobiotechnology Drug-eluting stent coatings
17. Ratner BD. New ideas in biomaterials science, A pathto engineered biomaterials. J Biomed Mater Res 1993,27(7):837–850.
18. Pinchuk L, Wilson GJ, Barry JJ, Schoepho-erster RT, Parel JM, et al. Medical applica-tions of poly(styrene-block-isobutylene-block-styrene)(’’SIBS’’). Biomaterials 2008, 29:448–460.
19. Ven der Giessen W, Lincoff AM, Schwartz RS, vanBeusekom HMM, Serruyset PW, et al. Marked inflam-matory sequalae to implantation of biodegradable andnonbiodegradable polymers in porcine coronary arter-ies. Circulation 1996, 94:1690–1697.
20. Pinchuk L. A review of the biostability and carcino-genicity of polyurethanes in medicine and the newgeneration of ‘biostable’ polyurethanes. J Biomater SciPolym Ed 1994, 6(3):225–267.
21. Wache HM, Tartakowska DJ, Hentrich A. Wagner:Development of a polymer stent with shape memoryeffect as a drug delivery system. J Mater Sci Mater Med2003, 14:109–112.
22. Muni NI, Gross TP. Problems with drug-eluting coro-nary stents- The FDA perspective. N Engl J Med 2004,351:1593–1595.
23. Weber F, Schneider H, Schwarz C, Holzhausen C, Pet-zsch M, et al. Sirolimus- eluting stents for percutaneouscoronary intervention in acute myocardial infarction.Z Kardiol 2004, 93:938–943.
24. Morice MC, Serruys PW, Barragan P, Bode C, Van EsGA, et al. Long-term clinical outcomes with sirolimus-eluting coronary stents: five-year results of the RAVELtrial. J Am Coll Cardiol 2007, 50(14):1299–1304.
25. Morice MA, Serruys PW, Sousa JE, Fajadet J, HayashiEB, Perin M, et al. A randomized comparison ofa sirolimus eluting stent with a standard stent forcoronary revascularization. N Engl J Med 2002,346:1773–1780.
26. Kennedy JP, Kaszas G, Puskas JE, Hager WG.Thermoplastic elastomers of isobutylene and processof preparation. U.S. Patent 4,946,899, August 7,1990.
27. Lawrence SS, Shinozaki DM, Puskas JE, Ger-chcovich M, Myler U. Micro-mechanical testingof polyisobutylene-polystyrene block-type thermo-plastic elastomers. Rubber Chem. Technol. 2001,74:601–613.
28. Puskas JP, Paulo C, Antony P. Arborescent thermo-plastic elastomers and products therefrom. U.S. Patent6,747,098, June 8, 2004.
29. Cadieux P, Watterson JD, Harbottle R, Howard J,Puskas JE, et al. A new biomaterial for applicationto the urinary tract, and potential for lactobacillusproteins to reduce the risk of device-associated infec-tions. J Colloids Surf B Biointerfaces 2002, 28(2–3):95–105.
30. Puskas JE, Chen Y, Antony P, Kwon Y, Kovar M, et al.Atomic force microscopic and encrustation studies ofnovel prospective polyisobutylene-based thermoplasticelastomeric biomaterials. Polym Adv Technol 2003,14(11–12):763–770.
31. Antony P, Kwon Y, Puskas JE, Kovar M, NortonPR. Atomic force microscopic studies of polystyrene-polyisobutylene block copolymers. Eur Polym J 2003,40:149–157.
32. Puskas JE, Antony P, El Fray M, Altstadt V. Effect ofhard and soft segment composition on the mechanicalproperties of polyisobutylene-polystyrene thermoplas-tic elastomeric block copolymers. Eur Polym J 2003,39:2041–2049.
33. Puskas JE, Chen Y. Biomedical application of com-mercial polymers and novel polyisobutylene-basedthermoplastic elastomers for soft tissue replacement.Biomacromolecules 2004, 5(4):1141–1154 (German)GAK-GV. 2004 7:455–461; 8:526–534.
34. Puskas JE, Chen Y, Dahman Y, Padavan D.Polyisobutylene-based biomaterials. Feature article.J Polym Sci Chem 2004, 42(13):3091–3109.
35. Kennedy JP, Puskas JE, Holden G, Kricheldorf HR,Quirk RP. Thermoplastic Elastomers. 3rd ed. Munich:Hanser Publishers; 2004.
36. Puskas JE, Kwon Y, Prince A, Bhowmick AK. Synthe-sis and characterization of novel dendritic(arborescent,hyperbranched) polyisobutylene-polystyrene. J PolymSci [A1] 2005, 43:1811–1826.
37. Puskas JE, Dos Santos L, Kaszas G. Innovation in mate-rial science: the chameleon block copolymer. J PolymSci Chem 2006, 44:6494–6497.
38. El Fray M, Prowans P, Puskas JE, Altstadt V. Bio-compatibility and fatigue properties of polystyrene-polyisobutylene-polystyrene, an emerging thermoplas-tic elastomeric biomaterial. Biomacromolecules 2006,7(3):844–850.
39. Puskas JE, Kwon Y. Biomacromolecular engineer-ing: desing, synthesis and characterization one-postsynthesis of block copolymers of arborescent poly-isobutylene and polystyrene. Polym Adv Technol 2006,17:615–620.
40. Foreman EA, Puskas JE, Kaszas G. Synthesis andcharacterization of arborescent (hyperbranched) poly-isobutylenes from the 4-(1,2-oxirane-isopropyl)styreneinimer. J Polym Sci Chem 2007, 45:5847–5856.
41. Turco MA, Ormiston JA, Popma JJ, Mandinov L,O’Shaughnessy CD, et al. Polymer-based, paclitaxel-eluting TAXUS Liberte stent in de novo lesions: thepivotal TAXUS ATLAS trial. J Am Coll Cardiol 2007,49(16):1676–1683.
42. Keiichi T, Serruys PW, Bruining N, Dudek D,Drzewiecki J, et al. Two-year serial coronary angio-graphic and intravascular ultrasound analysis ofin-stent angiographic late lumen loss and ultrasonic
2009 John Wiley & Sons, Inc.

Advanced Review www.wiley.com/wires/nanomed
neointimal volume from the TAXUS II trial. Am JCardiol 2007, 99(5):607–615.
43. Moses JW, Mehran R, Nikolsky E, Lasala JM, CoreyW, et al. Outcomes with the paclitaxel-eluting stentin patients with acute coronary syndromes: analysisfrom the TAXUS-IV trial. J Am Coll Cardiol 2005,45(8):1165–1171.
44. Ranade SV, Richard RE, Helmus MN. Styrenic blockcopolymers for biomaterial and drug delivery applica-tions. Acta Biomater 2005, 1:137–144.
45. Ranade SV, Miller KM, Richard RE, Chan AK, AllenMJ, Helmus MN. et al. Physical characterization ofcontrolled release of paclitaxel from the TAXUSTMExpress2TM drug eluting stent. J Biomed Mater Res2004, 71A(4):625–634.
46. Long D. DES2.0—and beyond. AHC Media LLCCardiovascular Device Update. AHC Media 2007,13(2):1–7.
47. Lagerqvist B, James SK, Stenestrand U, Lindback J,Nilsson T, et al. Long-term outcomes with drug-elutingstents versus bare-metal stents in Sweden. N Engl JMed 2007, 356:1009–1019.
48. Galoe AM, Thuesen L, Kelbaek H, Thayssen P,Rasmussen K, et al. Comparison of paclitaxel- andsirolimus-eluting stents in everyday clinical practice:the SORT OUT II randomized trial. JAMA 2008,299(4):409–416.
49. Blagosklonny MV, Darzynkiewicz Z, Halicka HD,Pozarowski P, Demidenko ZN. Paclitaxel induces pri-mary and postmitotic g1 arrest in human arterialsmooth muscle cells. Cell Cycle 2004, 3(8):1050–1056.
50. Haude M, Erbel R, Straub U, Dietz U, Schatz R, et al.Results of intracoronary stents for management of coro-nary dissection after balloon angioplasty. Am J Cardiol1991, 67(8):691–696.
51. Schatz RA, Baim DS, Leon M, Ellis SG, GoldbergS, et al. Clinical experience with the Palmaz-Schatzcoronary stent. Initial results of a multicenter study.Circulation 1991, 83(1):148–161.
52. Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ,et al. Stent thrombosis in the modern era: a pooledanalysis of multicenter coronary stent clinical trials.Circulation 2001, 103(15):1967–1971.
53. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, HolmesDR, et al. Sirolimus-eluting stents versus standardstents in patients with stenosis in a native coronaryartery. N Engl J Med 2003, 349(14):1315–1323.
54. Stone GW, Ellis SG, Cox DA, Hermiller J,O’Shaughnessy C, et al. A polymer-based paclitaxel-eluting stent in patients with coronary artery disease.N Engl J Med 2004, 350(3):221–231.
55. Kereiakes DJ. The Emperor’s new clothes: anothercipher versus taxus post-hoc meta-analysis. J Am CollCardiol 2007, 50(14):5.
56. Bavry AA, Kumbhani DJ, Helton TJ, Bhatt DL. Whatis the risk of stent thrombosis associated with the useof paclitaxel-eluting stents for percutaneous coronaryintervention? A meta-analysis. J Am Coll Cardiol 2005,45(6):941–946.
57. Pfisterer ME, Kaiser CA, Bader F, Brunner-La RoccaHP, Bonetti PO. BASKET-LATE: Late clinical eventsrelated to late stent thrombosis after stopping clopido-grel: Drug-eluting vs bare-metal stenting. In AmericanCollege of Cardiology 55th Annual Scientific Meeting,Atlanta, GA, 2006, Abstract 422-11.
58. Camenzind E, Steg PG, Wijns W. A cause for concern.Circulation 2007, 115:1440–1455.
59. Leon BM. Independent physician-led patient-levelanalysis: TAXUS randomized trials. In Programand abstracts from the Transcatheter Cardiovascu-lar Therapeutics 18th Annual Scientific Symposium,Washington, DC, October 22–27, 2006.
60. Stone GW. Independent physician-led patient-levelanalysis: CYPHER randomized trials. In Programand abstracts from the Transcatheter Cardiovascu-lar Therapeutics 18th Annual Scientific Symposium,Washington, DC, October 22–27, 2006.
61. Bavry AA, Bhatt DL. Appropriate use of drug-eluting stents: balancing the reduction restenosiswith the concern of late thrombosis. Lancet 2008,371(9630):2134–2143.
62. Marroquin OC, Mulukutla SR, Kip KE. Bare-metal ver-sus drug-eluting coronary stents. N Engl J Med 2008,358(23):2517–2518.
63. Pierfrancesco A, Vermersch P. Bare-metal versus drug-eluting coronary stents New England. J Med 2008,358(23):2516–2517.
64. Austin D, Pell JP, Oldroyd KG. Bare-metal versusdrug-eluting coronary stents. N Engl J Med 2008,358(23):2516.
65. Pui DYH, Chen DR. Electrospraying Apparatus andMethod for Coating Particles. US Patent 6,746,869,June 8, 2004.
2009 John Wiley & Sons, Inc.