Acute and Chronic Liver Disease Acute – < 6 months duration – No permanent damage – Often...
102
Acute and Chronic Liver Disease Acute – < 6 months duration – No permanent damage – Often resolves spontaneously Chronic – > 6 months – May progress to cirrhosis after many years – Must look for treatable causes
-
Upload
chrystal-parker -
Category
Documents
-
view
217 -
download
0
Transcript of Acute and Chronic Liver Disease Acute – < 6 months duration – No permanent damage – Often...

Acute and Chronic Liver Disease
Acute– < 6 months duration– No permanent damage– Often resolves spontaneously
Chronic– > 6 months– May progress to cirrhosis after many years– Must look for treatable causes




Diagnosis of Acute hepatitis
Nausea, anorexia, Mild RUQ discomfort Rarely jaundice, dark urine Occas low grade fever ALT in 100’s or 1000’s (N<40) Cannot usually differentiate cause by clinical
presentation


Causes of “acute hepatitis”
Hepatitis A,B,C,D,E Other viruses eg CMV (cytomegalovirus),
EBV (mono), HSV (herpes simplex virus) Medications Wilson's Disease Autoimmune Hepatitis Common Bile Duct Stone

Hepatitis A Virus (HAV) Fecal-oral spread
Never cause chronic infection
More severe illness in adults
Only 20% of Canadian army recruits immune to HAV compared with 70% of 60 year-olds
Outbreaks world-wide from imported Infected shell-fish, berries
Travel to endemic area eg Mexico

Occupations at risk of Hepatitis A
Military personnel
Food handlers
Health care workers
Child care workers
Sanitation workers

Acute Type A Hepatitis

Complications of Hepatitis A
Cholestatic Jaundice
Relapsing Hepatitis
Fulminant Hepatitis

Hepatitis A vaccine
Available alone (Havrix)or combined with Hepatitis B (Twinrix)
Almost 100% effective Recommended in individuals travelling to
high risk countries, patients with cirrhosis, MSM, sanitation workers

Hepatitis B HBV is a DNA virus, discovered in
1966
350 million people worldwide infected
A leading cause of cirrhosis and hepatocellular (HCC) carcinoma
1 million deaths yearly

Geographic Distribution of Chronic HBV Infection
HBsAg Prevalence
≥ 8% (high)2% to 7% (intermediate)
< 2% (low)
Weinbaum CM, et al. MMWR Recomm Rep. 2008;57(RR-8):1-20.

Outcome of neonatal InfectionAcute Infection (< 10%)
Neonatal Infection ( from infectious mother)
Chronic Carrier(90%)
Normal Histolo
gy
Mild hepatiti
s
Active hepatiti
sCirrhosis
Hepatocellular
Carcinoma

Consequences of Acute HBV infection- in an adult
CLINICAL INFECTION(icteric or anicteric)
FULMINANTHEPATITIS (<
1%)
RECOVERY AND
IMMUNITY (95%)
CHRONIC CARRIER (5%)
DEATH

Outcome of Acute HBV Infection

Transmission of HBV InfectionTransfusion
(Blood, blood products)
Fluids(blood, semen)
Organs and tissue
transplantation
Mother to baby
Contaminated needles and
syringes
Child to child
HEPATITIS B

Impact of Immigration on US HBV Prevalence
HBsAg Prevalence[2]
≥ 8% (high)2% to 7% (intermediate)
< 2% (low)
Immigration Numbers by Continent: 2000-2009[1]
~ 3.6 million Asians
~ 875,000South Americans
~ 804,000 Africans
~ 1.3 million
Europeans
1. US Department of Homeland Security. Yearbook of Immigration Statistics: 2009. 2. Weinbaum CM, et al. MMWR Recomm Rep. 2008;57(RR-8):1-20.

Hepatitis B in Ottawa 90 % are Immigrants from high-
risk countries eg. SE Asia, Viet Nam, Africa
IV drug users
Hemodialysis patients ( rare now)
MSM (rare now)
Multiply-transfused patients (rare now)

Consequences of HBV infectionCLINICAL
INFECTION
CHRONIC CARRIER
CHRONIC Mild HEPATITIS
Reactivation
Liver Cancer
DEATH
CIRRHOSIS
SUBCLINICALINFECTION
CHRONIC ACTIVE
HEPATITIS
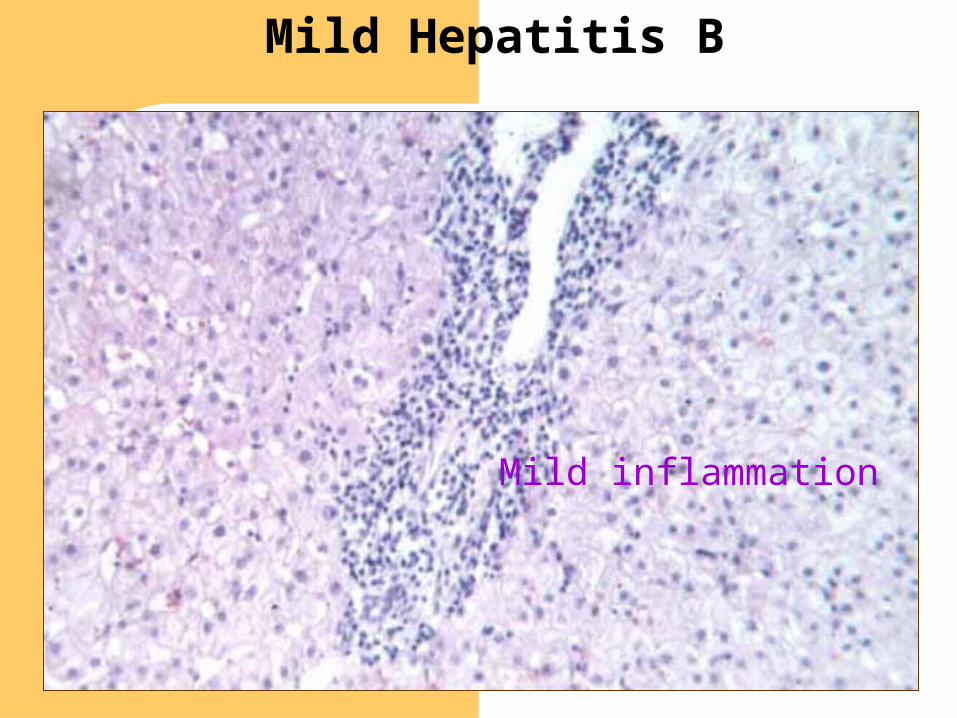
Mild inflammation
Mild Hepatitis B
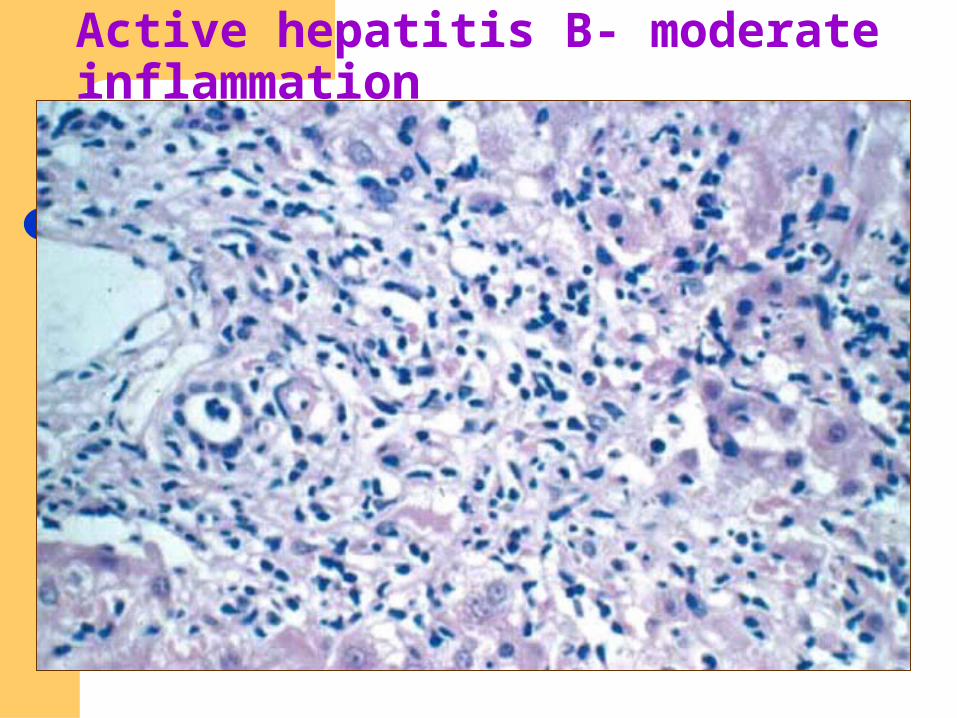
Active hepatitis B- moderate inflammation

The structure of the Hepatitis B Virus (HBV


HBV-DNA Integration in HepatocytesEpisomal HBV-
DNA
Chromosomal HBV-DNA(Integrated into host cell chromosome)
Cytoplasm

Acute Hep B infection

Treatment of Acute Hepatitis B- No specific treatment
- Avoid alcohol and hepatotoxic drugs
- Hospitalization if protracted vomiting or PT > 3 seconds prolonged
- Immunization (active and passive) of contacts

Immunization against HBVPassive
Hepatitis B Immune Globulin(Anti-HBS Titer > 1:1 000 000) Needle-stick Acute sexual contact Perinatal transmission
ActiveHepatitis B vaccine

Chronic Hepatitis B

clinicaloptions.com/hep
HBV Core Curriculum 2008: Treatment and Management
Phase Immune Tolerant
Immune Clearance
Inactive Carrier State
Reactivation
LiverMinimal
inflammation and fibrosis
Chronic activeinflammation
Mild hepatitis and minimal
fibrosis
Active inflammation
Yim HJ, et al. Hepatology. 2006;43:S173-S181.Optimal treatment times
Anti-HBeAg
HBV DNA
ALT activity
Current Understanding of HBV Infection
4 Phases of Chronic HBV Infection
HBeAg

Indications for Treatment of
Chronic Hepatitis B Infection
• HBsAg positive, HBV DNA positive
• Persistent elevation of ALT
• Significant liver fibrosis (Liver Biopsy/ fibroscan)
• Other factors eg infectivity in healthcare worker

Antivirals in Chronic Hepatitis B
• Generally well-tolerated oral agents
• Effectively ( 90%) suppress HBV DNA – but need ?life-long Rx
• Resistance a potential problem with Lamivudine- so not used in high level viral DNA
• Tenofovir ( Reverse transcriptase inhibitor) or Entecavir (DNA polymerase inhibitor) are indicated in patients with high viral DNA levels

Hepatocellular Carcinoma (HCC) = Hepatoma

HBsAg As a Risk Factor for primary hepatocellular carcinoma (P.H.C.) - Taiwan
22,708subjects
19,254HBsAg Negative
Controls
3,454HBsAg Positive
Carriers
9 P.H.C. 152 P.H.C.
Risk = 5/100,000/Year Risk = 495/100,000/YearRelative Risk - 94

Morphologic Forms of HBsAg
HBcAg
HBsAg


Who should receive hepatitis B vaccine?
• Infants of Infected Mothers (plus HBIg
• MSM
• IV Drug users
• Heterosexual and household Contacts of Hepatitis B carrier
• Travelers to Endemic Areas
• Hemodialysis Patients
• Health Care Workers
• Universal Vaccination?

Hepatitis C


Hepatitis CSpectrum of
DiseaseAcute HCV Infection
Recovery
15%-30%
Chronic HCV Infection
70%-85%
Chronic Hepatitis C
Mild Moderate Severe
End-stage Liver Disease
Cirrhosis
Hepatocellular carcinoma
Liver Transplantation Death

Acute Hepatitis C
Estimated Incidence,United States, 1982-1996

Prevalence of anti-HCV in
various Study populations
Population NAnti-HCV
Reactivity
IV Drug users 41475.6%
Hemophiliacs 18459.8%
Renal Dialysis Pt 697 20.0%
MSM 3884.4%
Random Population 2432.1%
Blood Donors 9,9980.6%

HCV Infection
Risk FactorsKnown Risk
• Injection-drug use(i.e., shared paraphenalia)
• Receipt of clotting factor before 1987
• Immigration from areaswithout universal precaution
Unproved/Low Risk
• Perinatal transmission
• Transfusion after 1992
• Body piercing/scarification
• Long-term hemodialysis
• Occupational exposure (eg. Healthcare worker)
• Intranasal cocaine use
• Sex with multiple partners

Risk Factors


Pull out, pull out, you’ve hit an artery!!!


How to diagnose Hepatitis C: (HCV)
1. HCV Antibody positive
2. Confirm with HCV RNA-pcr based assay
3. 6 Genotypes world-wide: influences RX regimen
4. Liver biopsy or fibroscan to determine degree of fibrosis

1a, 1b 2a,
2b, 3a
1a, 1b 2a, 2b,
2c, 3a
4
5a
1b
1b, 6
1b, 3a
1b, 3a
3b
4
Fang et al. Clin Liver Dis. 1997.
HCV Infection: Worldwide Genotype Distribution
1a, 1b, 2b, 3a
2a
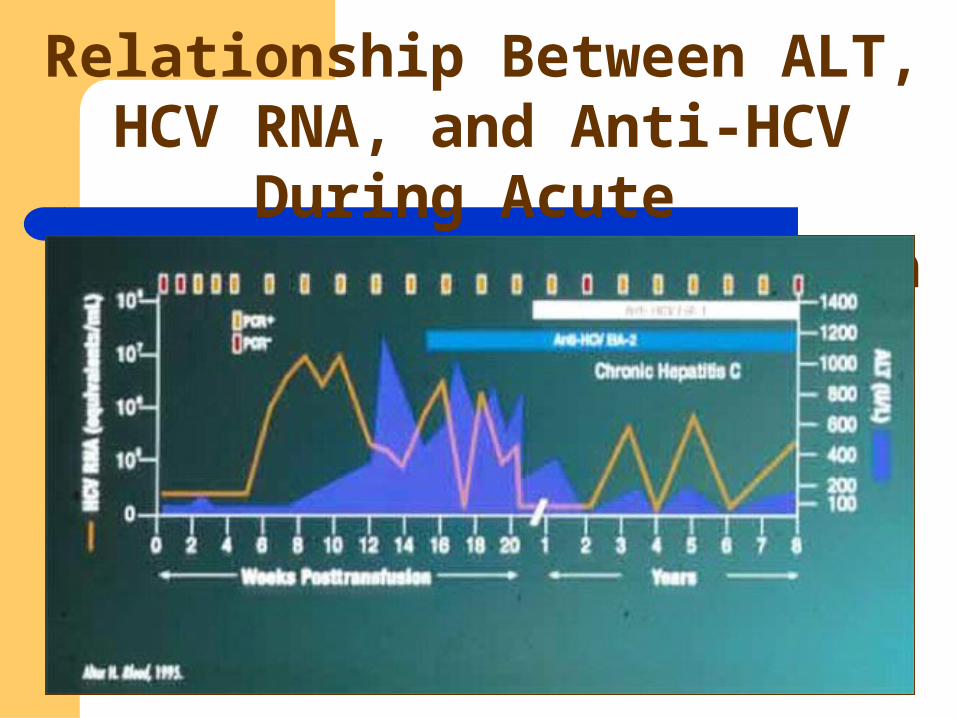
Relationship Between ALT, HCV RNA, and Anti-HCV
During Acute and Chronic HCV Infection


Hepatitis C and cryoglobulinemia/ leukocytoclastic vasculitis

Hepatitis C and Porphyria Cutanea Tarda

Treatment of HCV: indications• Transaminases (ALT) > 1.5 X normal
• ? Symptoms
• Significant fibrosis on biopsy/fibroscan
• Age
• Presence of associated conditions
• No current alcohol or drug abuse

Rapidly evolving Rx of Hepatitis C
Pegylated Interferon plus Ribavirin: overall 55% success rate ie. “cured” but major side-effects
New antivirals ( Protease and Reverse Transcriptase Inhibitors) : about to be licensed: 97% cure rate with 12- 24 weeks of Rx (Sofosbuvir/ Ledipasvir)
Cost ? > $70,000 for 12 weeks

Hepatitis C
Epidemic in baby boomers secondary to use of IV drugs in 60’s/70’s
Virtually no newly acquired Hepatitis C except current drug users
Aggravated by alcohol and fatty liver Cause of 50% of liver transplants in Canada Spectrum of disease from minimal fibrosis to
cirrhosis at 20 years New treatments > 70% successful
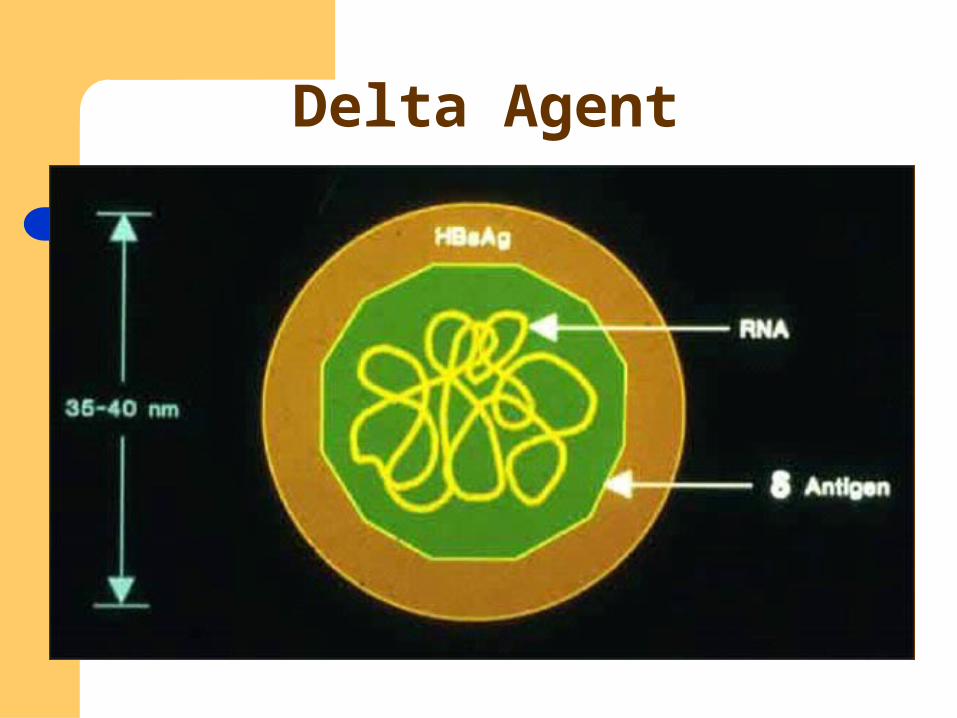
Delta Agent

Delta Hepatitis
Rare in Canada Delta is incomplete virus which requires
HBsAg to enter hepatocytes Causes more aggressive liver damage No effective treatment

Hepatitis E
• Epidemic form of Non-A Non-B hepatitis
• Similarities to Hepatitis A
• Waterborne, Outbreaks
• High morality in pregnant women
• Rarely found in North America- ?sausage

Etiology Agents of Chronic Viral Hepatitis

Alcoholic Liver Disease (ALD)
“To a Liver, they are all the same!” Each unit = 14 gm Etoh.

Alcoholic Liver Disease:
Causes 40% of cirrhosis deaths in UK: 27% of men and 13% of women drink > recommended (30 gm/day for men, 20 gm/day for women)
Increasing prevalence in last 2 decades < 20% of very heavy drinkers (>120gm/day)
develop Cirrhosis after 20 years: genetic factors??

Alcoholic Liver Disease: Pathology
Spectrum of Liver Damage from Fatty liver to Alcoholic Hepatitis to Cirrhosis
Fatty liver:>50%of liver cells contain large droplet fat Alcoholic Hepatitis: fat and inflammatory infiltrate
with lymphocytes and PMN’s/ ballooned cells and variable degrees of fibrosis: ?TNF/cytokine mediated
Cirrhosis: micronodular or mixed micro/macronodular cirrhosis

Acute Alcoholic Hepatitis
Often presents with sudden jaundice, RUQ pain, nausea, fever: after years of drinking
Spider nevi, palmar erythema, frequent edema and ascites. Patient looks sick, malnourished.
Elevated Total Bilirubin, Macrocytosis, elevated WBC (PMN’s), low platelet ct, low albumin.
AST>ALT but usually only mild to moderately elevated (<5XN)
Treatment of Alcoholic Hepatitis:
Admit to hospital. Stop alcohol/ nutritional support/ thiamine/ vitamins
Look for infection Alcoholic Hepatitis Score: Maddrey
Discriminant Function: (Bili and INR);>32 have 6 month mortality of 50%
Prednisilone 40 mg/day for 1 month: still controversial. ? Pentoxifyline
?Liver Transplant

Risk factors for NAFLD (Non-alcoholic fatty liver disease) 69-100% obese 34-75% Diabetic 20-80% hyperlipidemic Central obesity more important than total
weight Insulin resistance invariable

NAFLD:Non Alcoholic Fatty Liver Disease:Spectrum
Benign steatosis- large droplet fat found in most patients with significant central obesity
NASH- found in 8.5% of morbidly obese at Surgery and in 18.5% of obese at autopsy; resembles ALD pathologically: Mechanisms unkown: genetic factors/ cytokines/ TNF?

NASH: Non-Alcoholic Steatohepatitis
% of patients with fatty liver who develop NASH/ cirrhosis unknown
Reason? Genetic,” second hit”? Recent association with various SNP’s
Natural history: 3-15% of patients with NASH have cirrhosis on Bx. ? Commonest cause of cirrhosis in Canada
Third most common cause of liver transplant and increasing in frequency
Rx: gradual weight loss

Other causes of Cirrhosis:
Genetic eg. Wilson's Disease, Hemochromatosis
Autoimmune eg. Autoimmune Hepatitis, Primary Biliary Cirrhosis, Primary Sclerosing cholangitis
Alcoholic Liver Disease NASH (Non-Alcoholic Steatohepatitis) Misc: eg Budd-Chiari Syndrome




Wilson’s Disease•Autosomal recessive
•Abnormality in handling of copper
•Copper deposits in liver and basal ganglia
•Presentation age 5-30 years with either neurologic or hepatic disease
•Liver disease can vary from acute hepatitis to cirrhosis

Wilson’s Disease•Must be ruled out in all patients < age 30 with liver disease
•May present as 1) ABN LFT’s 2) Fulminant Hepatic Failure 3) Chronic Active Hepatitis 4) Cirrhosis
•CNS Features
Wilson’s Disease•Decreased ceruloplasmin (a copper binding protein)
• Increased Urinary Copper
•Kayser-Fleisher Rings
•Neurologic manifestations esp tremor and psychiatric abnormalities



Presentation of Wilson’s Disease

Wilson’s DiseaseTreatment
•D-Penicillamine- binds copper so not absorbed from diet and copper deposits gradually decline

Hereditary hemochromatosis
0.4-1.0% of N European One of the most common inherited
disorders Autosomal recessive Leads to excess iron absorption in gut
and deposition in liver,heart,joints,pancreas and other endocrine organs

HFe

HFe


Hemochromatosis genes:
85% of HFe patients are Homozygous for C282Y mutation
5% are C282Y/H63D heterozygote C282Y predominantly northern Europe
(1/300) H63D common in all ethnic groups-
14% allelic frequency, low penetrance

Management of Hemochromatosis:
Gene testing Phlebotomy/ Become Blood Donor Family screening ?MRI Screening for hepatoma in Cirrhotics

Other causes of iron overload: Metabolic syndrome
Obesitas Hypertension Insulin resistance
Chronic Liver Disease Hepatitis Alcohol use NASH Porphyria Cutanea Tarda
Iron overload in sub-Saharan Africa

α-1 Antitrypsin Deficiency•Hereditary deficiency of α-1 antitrypsin
•Often presents as neonatal Jaundice EG: - 5/28 infants with neonatal hepatitis ultimately diagnosed as α-1 at deficiency. - 9/13 patients with α-1
antitrypsin deficiency presented as jaundice < age 1 year.
•Liver disease associated with Pizz Phenotype


Autoimmune Chronic Active Hepatitis
• Disease of young women and menopausal women
• C/O fatigue
• AST, ALT
• High IgG levels
• ANA +VE in 80%
• Anti-smooth muscle antibody most specific test (80%)
• Liver biopsy shows chronic hepatitis with plasma cells and more damage than anticipated
• Treatment = Corticosteroids

Primary Biliary Cirrhosis (PBC)
•Disease of Middle-aged women
•Presents with fatigue, hepatomegaly, +- pruritus (itch)
• Increased Alkaline phosphate
•Cell-mediated damage to intrahepatic ductules
•+ve antimitochondrial antibodiesin 95%



Primary Biliary Cirrhosis
Was major cause of liver transplant URSO (Ursodeoxycholic Acid)
treatment since 1986 .. Few progress Itch can be debilitating: Rx
cholystyramine which binds bile salts in GI tract

Primary Sclerosing Cholangitis: PSC
70% have Ulcerative colitis Either can present first PSC can develop after colectomy Autoimmune damage of medium size
intra and extra- hepatic bile ducts Presents as abnormal cholestatic liver
enzymes and occasionally recurrent cholangitis



Primary Sclerosing Cholangitis
• Frequently progresses to Liver transplant- but age varies
• No Known treatment• ERCP dilatation of tight strictures• Risk of cholangiocarcinoma ( and
hepatoma)

Budd-Chiari Syndrome:
Blockage of Hepatic veins Usually secondary to Hypercoagulable state Often presents with ascites Diagnosed with US/doppler of hepatic veins Rx: anticoagulation +/- Tipps +/- Liver
transplant Rare

Medication Induced Liver Disease
Several medications/herbal products can cause severe liver disease
Nitrofurantoin and Minocycline –Autoimmune hepatitis
Methotrexate and Amiodarone- NASH/cirrhosis
Hydroxycut/Tylenol –fulminant liver failure