Acute and Chronic Cholecystitis
18
Harvest Time
-
Upload
made-widiastika -
Category
Documents
-
view
131 -
download
1
description
gastro
Transcript of Acute and Chronic Cholecystitis

Harvest Time

Acute and Chronic Cholecystitis and Cholelithiasis

CLINICAL MANIFESTATION

KOLESISTITIS AKUTAdalah reaksi inflamasi akut dinding kandung empedu dgn ditandai adanya:
= Nyeri perut kanan atas
= Panas badan
Faktor yg berperan :
= stasis cairan
= infeksi kuman
= iskemia dinding

PEMBAGIANBerdasar penyebab dibagi 2:
= Kolesistitis akut kalkulus : (90%) terjadi
karena ada batu yg menyumbat ductus
cysticus
= Kolesistitis akut akalkulus : didapat pd
pasien yg dirawat cukup lama dan dgn
nutrisi parenteral, keganasan GB, atau
merupakan komplikasi demam tifoid atan
DM

Acute calculous cholecystitis
• Persistent cystic duct obstruction leads to GB distension, wall inflammation & edema
• Can lead to: empyema, gangrene, rupture
• Pain persists >24hrs with fever
• Palpable/tender or even visible RUQ mass
• Sg: Cholecystectomy within 48hrs

Chronic calculous cholecystitis
• Recurrent inflammatory process due to recurrent cystic duct obstruction, 90% of the time due to gallstones
• Overtime, leads to scarring/wall thickening
• Treatment: laparoscopic cholecystectomy

Acute acalculous cholecystitis
• In 5-10% of cases of acute cholecystitis
• Seen in critically ill pts or prolonged TPN
• More likely to progress to gangrene, empyema, perforation due to ischemia
• Caused by gallbladder stasis from lack of enteral stimulation by cholecystokinin
• Tx: Emergent cholecystectomy

GEJALA KLINISKeluhan dan tanda yg khas adalah :
= Kolik perut kanan atas
= Nyeri tekan perut kanan atas
= kenaikan temperatur
= Rasa sakit menjalar ke pundak atau
scapula kanan
= Murphy sign positif

MURPHY SIGN• Pasien terlentang dan pemeriksa ada di sisi
kanan penderita
• Dilakukan penekanan dengan tangan kanan di
perut kanan atas, tahan pada posisi ini, dan
pasien diminta menarik nafas dalam : nafas
terhenti krn pasien kesakitan, Murphy sign
positif

Diagnosis• History• Physical exam• Labs & Diagnostic Tests
– Elevated WBC
– Elevated bilirubin in serum & urine
– Prolonged PT resulting from interference with vitamin K absorption
• Alkaline phosphatase, serum amylase levels to differentiate between gallbladder & pancreas
• Serial enzyme tests & ECG heart disease• Calculi observed on USG

PAIN PHOTO ABDOMEN

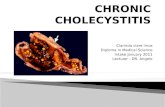
ULTRASONOGRAPHY


Case 3
• → denotes the GB wall thickening
• ► denotes the fluid around the GB
• GB also appears distended
→
►

Complications of acute cholecystitis
Empyema of gallbladder
Pus-filled GB due to bacterial proliferation in obstructed GB. toxic, high fever
Emphysematous cholecystitis
More commonly in men and diabetics. Severe RUQ pain, generalized sepsis. Imaging shows air in GB wall or lumen
Perforated gallbladder
Occurs in 10% of acute chol’y, usually becomes a contained abscess in RUQ
Less commonly, perforates into adjacent viscus = cholecystoenteric fistula & the stone can cause gallstone ileus

PENGOBATAN
= Puasa/ bed rest
= Nutrisi parenteral
= Pain killer gol. Meperidine
= Antibiotik sistemik
= Kolesistektomi

TERIMA KASIH