Abnormal Amygdalar Activation and Connectivity in ... · Connectivity in Adolescents With...
13
NEW RESEARCH Abnormal Amygdalar Activation and Connectivity in Adolescents With Attention- Deficit/Hyperactivity Disorder Jonathan Posner, M.D., Bonnie J. Nagel, Ph.D., Tiago V. Maia, Ph.D., Anna Mechling, B.A., Milim Oh, M.A., Zhishun Wang, Ph.D., Bradley S. Peterson, M.D. Objective: Emotional reactivity is one of the most disabling symptoms associated with attention-deficit/hyperactivity disorder (ADHD). We aimed to identify neural substrates associated with emotional reactivity and to assess the effects of stimulants on those substra- tes. Method: We used functional magnetic resonance imaging (fMRI) to assess neural activity in adolescents with (n 15) and without (n 15) ADHD while they performed a task involving the subliminal presentation of fearful faces. Using dynamic causal modeling, we also examined the effective connectivity of two regions associated with emotional reactivity, i.e., the amygdala and the lateral prefrontal cortex (LPFC). The participants with ADHD underwent scanning both on and off stimulant medication in a counterbalanced fashion. Results: During the task, we found that activity in the right amygdala was greater in adolescents with ADHD than in control subjects. In addition, in adolescents with ADHD, greater connectivity was detected between the amygdala and LPFC. Stimulants had a normalizing effect on both the activity in the right amygdala and the connectivity between the amygdala and LPFC. Conclusions: Our findings demonstrate that in adolescents with ADHD, a neural substrate of fear processing is atypical, as is the connectivity between the amygdala and LPFC. These findings suggest possible neural substrates for the emotional reactivity that is often present in youths with ADHD, and provide putative neural targets for the development of novel therapeutic interventions for this condition. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(8):828 – 837. Key Words: ADHD, amygdala, effective connectivity, fear, stimulant medication A lthough attention-deficit/hyperactivity disorder (ADHD) is characterized by in- attention, hyperactivity, and impulsiv- ity, 1 one of the most disabling symptoms of the disorder is the heightened emotional reactivity that is present in so many youths with ADHD. 2,3 Youths with ADHD frequently display poorly reg- ulated outbursts of emotion, 1 and they have rates of mood disorders that are far beyond those that would be expected by chance alone. 4 Despite the clinical significance of emotional reactivity in ADHD, the neurobiological substrates for this as- pect of the disorder remain poorly investigated. In the current study, we investigated emo- tional processing in youths with ADHD using a task that engages the amygdala through the subliminal presentation of fearful faces. 5 This task is useful for several reasons. First, the im- portance of the amygdala in emotional process- ing has been clearly established. 6 Second, ana- tomical and functional MRI (fMRI) studies suggest that amygdalar morphology and func- tioning may be anomalous in youths with ADHD. 7,8 Third, by using subliminal presenta- tions of emotional stimuli, we aimed to diminish the effects of differences in supraliminal attention as a potential confound in comparing control subjects versus youths with ADHD. 9 We focused our study on amygdalar responses to affective stimuli, and also on the neural connec- tions between the amygdala and the lateral pre- frontal cortex (LPFC; Brodmann area 47). We inves- tigated the connectivity of the amygdala and LPFC using dynamic causal modeling (DCM) 10 and chose this circuit because the amygdala and LPFC have well described and abundant reciprocal con- Supplemental material cited in this article is available online. JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY VOLUME 50 NUMBER 8 AUGUST 2011 828 www.jaacap.org
Transcript of Abnormal Amygdalar Activation and Connectivity in ... · Connectivity in Adolescents With...

NEW RESEARCH
Abnormal Amygdalar Activation andConnectivity in Adolescents With Attention-
Deficit/Hyperactivity DisorderJonathan Posner, M.D., Bonnie J. Nagel, Ph.D., Tiago V. Maia, Ph.D.,
Anna Mechling, B.A., Milim Oh, M.A., Zhishun Wang, Ph.D., Bradley S. Peterson, M.D.
Objective: Emotional reactivity is one of the most disabling symptoms associated withattention-deficit/hyperactivity disorder (ADHD). We aimed to identify neural substratesassociated with emotional reactivity and to assess the effects of stimulants on those substra-tes. Method: We used functional magnetic resonance imaging (fMRI) to assess neural activity inadolescents with (n � 15) and without (n � 15) ADHD while they performed a task involving thesubliminal presentation of fearful faces. Using dynamic causal modeling, we also examined theeffective connectivity of two regions associated with emotional reactivity, i.e., the amygdala andthe lateral prefrontal cortex (LPFC). The participants with ADHD underwent scanning both on andoff stimulant medication in a counterbalanced fashion. Results: During the task, we found thatactivity in the right amygdala was greater in adolescents with ADHD than in control subjects. Inaddition, in adolescents with ADHD, greater connectivity was detected between the amygdala andLPFC. Stimulants had a normalizing effect on both the activity in the right amygdala and theconnectivity between the amygdala and LPFC. Conclusions: Our findings demonstrate that inadolescents with ADHD, a neural substrate of fear processing is atypical, as is the connectivitybetween the amygdala and LPFC. These findings suggest possible neural substrates for theemotional reactivity that is often present in youths with ADHD, and provide putative neuraltargets for the development of novel therapeutic interventions for this condition. J. Am. Acad.Child Adolesc. Psychiatry, 2011;50(8):828–837. Key Words: ADHD, amygdala, effectiveconnectivity, fear, stimulant medication
s
tstA
A lthough attention-deficit/hyperactivitydisorder (ADHD) is characterized by in-attention, hyperactivity, and impulsiv-
ity,1 one of the most disabling symptoms of thedisorder is the heightened emotional reactivitythat is present in so many youths with ADHD.2,3
Youths with ADHD frequently display poorly reg-ulated outbursts of emotion,1 and they have rates ofmood disorders that are far beyond those thatwould be expected by chance alone.4 Despite theclinical significance of emotional reactivity inADHD, the neurobiological substrates for this as-pect of the disorder remain poorly investigated.
In the current study, we investigated emo-tional processing in youths with ADHD using atask that engages the amygdala through the
Supplemental material cited in this article is available online.
JOURN
828 www.jaacap.org
ubliminal presentation of fearful faces.5 Thistask is useful for several reasons. First, the im-portance of the amygdala in emotional process-ing has been clearly established.6 Second, ana-omical and functional MRI (fMRI) studiesuggest that amygdalar morphology and func-ioning may be anomalous in youths withDHD.7,8 Third, by using subliminal presenta-
tions of emotional stimuli, we aimed to diminishthe effects of differences in supraliminal attentionas a potential confound in comparing controlsubjects versus youths with ADHD.9
We focused our study on amygdalar responsesto affective stimuli, and also on the neural connec-tions between the amygdala and the lateral pre-frontal cortex (LPFC; Brodmann area 47). We inves-tigated the connectivity of the amygdala and LPFCusing dynamic causal modeling (DCM)10 andchose this circuit because the amygdala and LPFC
have well described and abundant reciprocal con-AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

AMYGDALAR FUNCTIONING IN ADHD
nections.11,12 The LPFC receives affective inputsfrom the amygdala and integrates this informationwith other sensory inputs, while at the same timecoordinating motor output.13 Through connectionswith the amygdala, the LPFC is thought to inte-grate affective cues, such as potential threats, allow-ing these cues to guide goal-directed behaviors.Conversely, disturbances of the amygdalar–LPFCcircuit produce impulsive behaviors characterizedboth by a disregard for salient, affective cues andby inattention with enhanced effects of distractingstimuli.14
We also examined the effects of stimulant med-ications on amygdalar functioning and amygdalar–LPFC connectivity. We did this by scanning youthswith ADHD both on and off of their normallyprescribed stimulant medication. Our a priori hy-potheses, based on the heightened emotional reac-tivity that is often present in youths with ADHD,was that these individuals, during their unmedi-cated scans, would demonstrate the following: 1)amygdalar hyperactivity relative to that in controlsubjects, and 2) anomalous amygdalar–LPFC con-nections.7,8 We further hypothesized that stimulantmedications would attenuate amygdalar hyperac-tivity and anomalous amygdalar–LPFC connec-tions. Stimulants often have a calming effect onyouths with ADHD, and this calming effect oftenincludes a reduction in emotional lability. Theneural mechanisms by which stimulants reduceemotional lability are largely unknown; few studieshave examined this issue. In animal models, how-ever, single-unit recordings during fear condition-
TABLE 1 Clinical and Demographic Characteristics of th
ADHD(mean � SD)
H
Age (y) 13.5 � 1.2 13.4 �
Gender 3 Male 13 Ma2 Female 2 Fem
Ethnicity 15 White 14 Wh1 Mu
Hollingshead Index of SocialPosition
32.4 � 13.9 31 � 1
FSIQ 111.4 � 16 114.1 �
Pubertal status 2.5 � 0.8 2.7 �
STAI 45.2 � 7.3 39.5 �
CDI 46.4 � 7.0 39.5 �
Note: Socioeconomic status was assessed with the Hollingshead Index of S(PDS). ADHD � attention-deficit/hyperactivity disorder; CDI � ChildSpielberger State Anxiety Inventory.
aIndicates a statistically significant difference.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
ing indicate that dopamine attenuates activity inboth the amygdala and prefrontal cortex.15,16 Wethus reasoned that by augmenting dopamine trans-mission, stimulants may attenuate the amygdalar–LPFC circuitry in youths with ADHD.
METHODThe Institutional Review Board of the Oregon Health& Science University (OHSU) approved the studyprocedures. All child participants provided written,informed assent, and a parent or legal guardian pro-vided informed, written consent.
ParticipantsThe participants were 15 youths with ADHD and 15healthy control subjects. Controls were group-matchedto the ADHD participants by age, gender, and ethnic-ity (Table 1) and screened for psychiatric disordersusing the Diagnostic Interview Schedule for Children(DISC) Predictive Scales17 and excluded for any prob-able active Axis I disorder. A child psychiatrist inter-viewed all participants with ADHD and at least oneparent; for all of the ADHD participants, child andparent versions of the DISC18 were completed. ADHDparticipants were excluded if they had any active AxisI disorder other than ADHD, oppositional defiantdisorder, or conduct disorder. ADHD participantswere also excluded if they were taking any nonstimu-lant psychotropic medication. Control subjects weremedication free. Additional exclusion criteria for bothADHD participants and controls included (1) age �11years or �16 years; (2) neurological illness; (3) signif-icant head trauma (loss of consciousness �2 minu-
dy Sample
Controlsn � SD) Test Statistic p Value
t � 0.3 .8�2 � 0 1.0
Mann–Whitney U � 105 .3ethnicities
t � 0.3 .8
t � 0.5 .6Mann–Whitney U � 98 .5
t � 2.1 .04a
t � 3.4 .003a
Position. Pubertal status was assessed with the Puberty Development ScaleDepression Inventory; FSIQ � Full Scale Intelligence Quotient; STAI �
e Stu
ealthy(mea
1.2lealeiteltiple1.8
100.77.40.9
ocialren’s
829www.jaacap.org

POSNER et al.
tes); (4) serious medical problems; (5) pregnancy; (6)IQ �80; (7) left-handedness; (8) non–native Englishspeaking; and (8) MRI contraindications.
Parents completed the Conners’ Parent RatingScales19 and Child Behavior Checklist.20 The parents ofADHD participants completed these assessmentsbased on their child’s unmedicated presentation.ADHD participants completed the Wechsler Abbrevi-ated Scale of Intelligence (WASI)21; control subjectscompleted the short form of the WASI, which consistsof the Matrix Reasoning and Vocabulary subtests. Allparticipants were administered the Edinburgh Hand-edness Inventory,22 Hollingshead Index of Social Po-sition,23 Children’s Depression Inventory (CDI),24
Spielberger State Anxiety Inventory (STAI),25 and Pu-berty Development Scale (PDS).26 The ADHD partici-pants were to complete two MRI scans; because ratingson the CDI and STAI could in theory vary between thefirst and second scan, the ADHD participants com-pleted these measures twice, i.e.. once at the time oftheir first MRI scan and again at their second MRIscan. Scores did not differ significantly at these twotime points (CDI: p � .36; STAI: p � .38); therefore weused only the scores obtained with the first MRI scan.ADHD participants and controls did not differ signif-icantly in regard to age, IQ, socioeconomic status, orpubertal stage (Table 1). ADHD participants hadhigher levels of depressive and anxiety symptoms (asmeasured by the CDI and STAI, respectively), andthese differences were controlled for in the fMRIanalyses. Within the ADHD sample, 13 participantswere classified as ADHD, Combined Type, and twowere classified as ADHD, Predominantly InattentiveType. The fMRI analyses covaried for ADHD subtype.
MRI Scanning SessionsADHD participants completed two scanning sessions:one while on their normally prescribed stimulant, andanother after abstaining from the stimulant for at least48 hours (i.e., exceeding at least four half-lives foravailable stimulant formulations). The order of thescanning sessions was counterbalanced across ADHDparticipants to control for medication status. Controlparticipants completed a single scanning session.
fMRI TaskThe task used a block design consisting of two blocktypes: 1) neutral faces presented supraliminally, and 2)fearful faces presented subliminally followed by neu-tral faces presented supraliminally. For simplicity, wewill refer to the first block type as “neutral face blocks”and to the second block type as “subliminal fearfulface blocks.” Each block type had 60 trials. On eachtrial of the neutral face blocks, participants wereshown a face with a neutral facial expression for thefull duration of the trial (500 milliseconds). On each
trial of the subliminal fearful face blocks, participantsJOURN
830 www.jaacap.org
were shown a fearful face for 30 milliseconds; then, forthe remainder of the trial (i.e., 470 milliseconds), theywere shown the same face but with a neutral expres-sion rather than a fearful one. Prior research indicatesthat such a brief presentation of a fearful face does notpermit supraliminal perception.5 The experiment con-sisted of two runs of the task. Each run consisted offour blocks, alternating between neutral face blocksand subliminal fearful face blocks with 15 seconds offixation at the beginning and end of each run. The totalscan time per run was 2 minutes 30 seconds.
The fMRI paradigms were presented with E-Prime (v. 1.0; Psychology Software Tools, Pitts-burgh, PA) running on a desktop computer. Weback-projected the task stimuli onto a screen thatparticipants viewed via a mirror attached to the MRIhead coil. Before beginning the task, participantswere instructed to try to remember the faces thatwould be presented. This was done to ensure thatthe participants were attending to the task. At theconclusion of the scanning session, participantswere shown a random selection of the faces pre-sented during the task and asked to circle those theyremembered seeing. The faces used during the taskwere obtained from the NimStim sample; in thesupplemental material, we provide further informa-tion about the specific faces selected from the Nim-Stim sample,27 as well as the instructions for thefMRI task and the post-scanning questionnaire (Sup-plement 1 and Table S1, available online). The faceswere presented as grayscale images at the center ofthe subject’s visual field with a visual angle ofapproximately 15° vertical and 12° horizontal.
Image AcquisitionImages were acquired using a 3.0-Tesla Siemens Mag-netom Tim Trio scanner with a 12-channel head coil atthe OHSU Advanced Imaging Research Center. Thescanning protocol started with a high-resolution,whole-brain structural image series collected in thesagittal plane using a T1-weighted MPRAGE sequence(TI � 900 milliseconds, flip angle � 10°, TE � 3.58milliseconds, TR � 2300 milliseconds, bandwidth �180 Hz/Px, 256 � 240 matrix, slice thickness � 1 mm).Blood oxygen level–dependent (BOLD) images werecollected in an oblique plane (parallel to the AC–PCline) using T2*-weighted echo-planar imaging (TR �2,000 milliseconds, TE � 30 milliseconds, flip angle �90°, FOV � 240 mm, in-plane resolution � 3.8 � 3.8mm, 33 slices covering the whole brain, slice thickness �3.8 mm, no skip).
Data AnalysisBehavioral Analyses. The total number of recalledfaces was calculated for each participant. To compare
medicated and unmedicated ADHD participants, weAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

tpcqspIacaoy
SstocThc
mDmmqde
AMYGDALAR FUNCTIONING IN ADHD
used a paired t test; to compare ADHD participantswith control subjects, we used independent sample ttests.Image Processing. Images were analyzed using SPM8(Wellcome Department of Imaging Neuroscience). Im-ages were motion and slice time corrected, coregis-tered with a high-resolution anatomical scan, normal-ized into the Montreal Neurological Institute (MNI)space, resampled at 2 mm3, and smoothed with aGaussian kernel of 6 mm3 FWHM.28 A 128-secondtemporal high-pass filter removed low-frequencynoise. For each participant, linear models were con-structed using regressors indexing the duration of eachblock type (neutral faces and subliminal fearful faces)convolved with the canonical hemodynamic responsefunction.
To account for head motion during scanning, wecalculated the root mean square (RMS) values of theadjustments needed to realign each participant’s headposition into its original position at the beginning ofeach scanning run. The RMS values were calculated onthe basis on three translational directions and rota-tions. Only runs with �2 mm RMS of motion wereused in the imaging analyses. The head motion for thethree groups is presented in the supplemental materialaccompanying this article (Supplement 1, availableonline). A non–statistically significant trend suggestedgreater motion in unmedicated ADHD participantsthan in controls. To control for this trend, we incorpo-rated into each participant’s linear model 6 nuisanceregressors reflecting motion parameters in three trans-lational directions and rotations.fMRI Activation Analyses. We used hierarchical lin-ear models and for each participant generated a whole-brain voxelwise contrast image that compared sublim-inal fearful face blocks with neutral face blocks. Thecontrast images were then entered in factorial modelsthat incorporated random effects and covaried for 1)depressive and anxiety symptoms, 2) ADHD subtype,and 3) presence of comorbid oppositional defiant dis-order (ODD)/conduct disorder (CD). In the supple-mental material, we include an additional analysis inwhich depressive and anxiety symptoms were notincluded as covariates; there was a nominal differencein the level of statistical significance for the study’smain findings (Supplement 1, available online). Wetreated Group as a between-subject factor when com-paring ADHD patients with controls, and as a within-subject factor when comparing medicated and un-medicated ADHD participants. Group � taskinteractions were planned to isolate brain regions thatdiffered between the groups in their response to sub-liminal fearful faces compared to neutral faces. Weused separate factorial models to compare 1) unmedi-cated ADHD participants versus controls; 2) medi-cated ADHD participants versus controls; and 3) med-icated versus unmedicated ADHD participants. These
analyses could not be reduced into a single model withJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
hree levels for Group (controls, unmedicated ADHDarticipants, and medicated ADHD participants) be-ause comparing ADHD patients versus controls re-uired a between-subject analysis, whereas a within-ubject analysis was necessary to compare ADHDatients in a medicated versus an unmedicated state.
n the supplemental material, we include a habituationnalysis (Supplement 1, available online). This wasonducted to exclude the possibility that differences inctivation could be the result of differences in the ratesf habituation to the fearful faces between ADHDouth and controls.
We localized regions of activation by attaining inPM the MNI coordinates of the voxel with the peakignal intensity within each area of activation. Weransformed the MNI coordinates into Talairach co-rdinates using mni2tal (http://imaging.mrc-cbu.am.ac.uk/imaging/MniTalairach) and then usedalairach deamon (http://www.talairach.org/daemon.tml) to obtain an anatomical label. The labels wereonfirmed via visual inspection.
Dynamic Causal Modeling: Background. We imple-ented dynamic causal modeling (DCM) using SPM8.CM permits the construction and statistical testing ofodels of interacting brain regions.10 The constructedodels are elaborated based on a balloon model that
uantifies how synaptic activity translates into hemo-ynamic responses; coupling parameters are thenstimated based on the observed fMRI signal.10,29,30
Using bilinear differential equations, DCM explicitlymodels the activity in a given brain area and howthis activity causes changes in the neural dynamicsof other brain regions. Given the observed data, thelikelihood that the model accurately represents thetrue neural dynamics is then estimated within aBayesian framework.31
Three coupling parameters are estimated. The firstparameter (DCM.A) estimates intrinsic connectionsbetween two brain regions. DCM.A estimates theeffect that one brain region has upon another, irrespec-tive of the fMRI task (i.e., an intrinsic or “baseline”connection between brain regions). The second param-eter (DCM.B) estimates perturbations in the intrinsicconnections (that is, DCM.A) between two brain re-gions that are the result of the fMRI task. DCM.Bquantifies the effect that the fMRI task has upon theinterregional connections rather than the effects thatthe task has upon specific brain regions. The thirdparameter (DCM.C) indexes the effects of the fMRItask on specific brain regions. DCM.C replicates theprimary fMRI analyses and is therefore not reported.29
Time series data for the amygdala and LPFC wereextracted using the Wake Forest PickAtlas (http://www.fmri.wfubmc.edu/download.htm). Blood Oxy-gen Level-Dependent (BOLD) signal changes wereaveraged across the voxels in each of the four regions
of interest (i.e., right and left amygdala, right and left831www.jaacap.org

caccgcA
DCWpipTtipscwa
DCIW
POSNER et al.
LPFC). Visual inspection of the functional imagesensured that the LPFC was free of signal dropout.Dynamic Causal Models: Between-Group Analyses.For each participant, we calculated 1) the intrin-sic connectivity (DCM.A) for top– down (LPFC¡amygdala) and bottom–up (amygdala¡LPFC) con-nections; and 2) the effects of the fMRI task on theseconnections (DCM.B). We compared the intrinsic con-nectivity between the sample groups using 2 � 2 � 2factorial models with diagnostic group as the firstfactor, connection type as the second factor (levels: 1,top–down; 2, bottom–up), and hemisphere as thethird factor (levels: 1, left side; 2, right side). As withthe fMRI activation analyses, separate factorial modelswere used to compare the following: 1) unmedicatedADHD participants versus controls; 2) medicatedADHD participants versus controls; and 3) medica-ted versus unmedicated ADHD participants.
We used a similar approach to examine groupdifferences in DCM.B (i.e., the effects of the task uponthe intrinsic connections). A positive DCM.B, herewould suggest that the presentation of fearful facesenhanced the connection. Conversely, a negativeDCM.B would suggest that the presentation of fearfulfaces reduced or inhibited the connection.Statistical Thresholds. For the fMRI activation analy-ses, we determined our statistical threshold using10,000 Monte Carlo simulations based on a connectiv-ity radius of 3.0 mm. These simulations determinedthat the conjoint requirement of a volume of 630 mLwith a voxelwise p value of �0.01 would yield aneffective p value of �0.000001. After accounting formultiple comparisons, the corrected � is 0.001, a con-servative statistical cutoff that minimizes the risk ofType I errors. We conducted the Monte Carlo simula-tions with AlphaSim32 adapted to run on a Matlabplatform (http://restfmri.net/forum). For the DCManalyses, we used the Bonferroni correction for multi-ple comparisons.Stimulant Effects Analysis. We used a nonparametricanalysis as a post hoc method of examining the hy-pothesis that stimulants have a normalizing effect onamygdalar activation and amygdalar–LPFC connectiv-ity. We conducted the test by assigning a positive (�)or negative (�) value to each of the analyses ofamygdalar activation and amygdala–LPFC connectiv-ity. We assigned an analysis a (�) value if the testindicated that with stimulants, the results for theADHD particpants became more similar to those forcontrols. Conversely, we assigned an analysis a (–)value if the test indicated that with stimulants, theresults for the ADHD participants became less similarto those for controls. A statistically significant result inthe positive direction would suggest a nonrandompattern, consistent with our hypothesis that stimulantshave a normalizing effect on amygdalar activation and
connectivity. pJOURN
832 www.jaacap.org
RESULTSBehavioral ResultsThe number of recalled faces did not differ sig-nificantly across groups. No more than a nominalnumber of fearful faces were recalled (Tables S2and S3, available online).
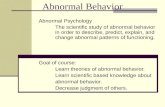
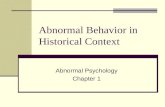
Imaging ResultsAll of the imaging results are based on wholebrain voxelwise analyses. In Table 2, we presentthe task-related activations for each group (i.e.,unmedicated ADHD participants, medicatedADHD participants, and control subjects), as wellas the main effects of the task (i.e., the effects ofthe task across the three groups) based on thecontrast: subliminal fearful face blocks versusneutral face blocks. To test our primary hypoth-esis that amygdala responses in youths withADHD would differ from controls, we examinedgroup � task interactions. We detected an inter-action in the right amygdala that was driven bygreater activation in the right amygdala in theunmedicated ADHD participants compared withcontrols (Figures 1 and 2; t � 3.64; p � .001). Nogroup � task interaction was detected whenomparing the medicated ADHD participantsnd controls (Figure 2), because stimulant medi-ation reduced amygdala activation to a levelomparable to the levels detected in controls. Noroup � task interaction was detected whenomparing the medicated and unmedicatedDHD participants.
ynamic Causal Modeling: Between-Groupomparisons of Intrinsic Connectionshen comparing unmedicated ADHD partici-
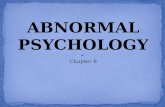
ants with controls, we found greater connectiv-ty in the unmedicated ADHD participants com-ared with controls (F1,27 � 6.5, p � .01; Figure 3).hese findings demonstrate stronger bidirec-
ional and bilateral amygdala–LPFC connectionsn the unmedicated ADHD participants com-ared with controls (Figure 3). We found noignificant differences when comparing unmedi-ated and medicated ADHD participants orhen comparing medicated ADHD participants
nd controls.
ynamic Causal Modeling: Between-Groupomparisons of the Effects of the Task on the
ntrinsic Connectionshen comparing unmedicated ADHD partici-
ants with controls, we found a statistical trend
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

t/hype
AMYGDALAR FUNCTIONING IN ADHD
suggesting a larger negative DCM.B in thecontrols compared with the unmedicatedADHD sample (F1,27 �3.1, p � .09; Figure 4). A
TABLE 2 Activations Detected During the Functional MagBetween Subliminal Fearful Face Blocks and Neutral Face
M
x
Task main effectsActivations
Inferior frontal gyrus �48Middle temporal gyrus 52Middle temporal gyrus �62
DeactivationsFusiform gyrus �30Insular cortex 42Superior frontal gyrus 28Precuneus �10
Within-group analysesUnmedicated ADHD youth
ActivationsAmygdala 22Middle occipital gyrus 32
DeactivationsMedicated ADHD youth
ActivationsSuperior occipital gyrus �22
DeactivationsAnterior cingulate cortex 10Superior occipital gyrus 22
Healthy controlsActivations
Superior temporal gyrus 68Middle frontal gyrus �32
DeactivationsPrecentral gyrus 30Cuneus 18Insular cortex 38Parietal cortex �26Cingulate cortex �10
Group � task interactionsADHD unmedicated youth � controls
Amygdala 20Middle occipital gyrus 30
Controls � ADHD unmedicated youthADHD medicated youth � controlsControls � ADHD medicated youthADHD unmedicated � ADHD medicated youthMedicated ADHD � ADHD unmedicated youth
Note: Activations detected during the functional magnetic resonance imagneutral face blocks. The coordinates and t values are reported at the peanalyses. The task main effects indicate activations detected across thetask-related activation. One voxel � 2 mm3. ADHD � attention-deficicoordinates; NA � no cluster meets statistical significance; R � right.
post hoc t test demonstrated a significant dif-
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
ference in DCM.B for the right-sided connec-tions (t � 2.5; p � .01; Figure 4) with a positiveDCM.B in the unmedicated ADHD participants
c Resonance Imaging (fMRI) Task Based on the Contrastks
oordinate
R/L Cluster Size t Valuey z
48 0 L 70 2.7538 6 R 666 3.4752 10 L 128 2.45
38 �16 L 99 �2.5622 10 R 172 �2.4954 32 R 119 �2.6254 40 L 114 �2.28
12 �10 R 89 4.0664 2 R 70 3.22
NA
90 30 L 282 3.55
38 14 R 265 �3.1698 6 R 73 �3.20
26 0 R 83 4.6318 38 L 542 5.90
34 60 R 942 �6.5798 10 R 74 �3.2416 6 R 198 �4.1236 66 L 158 �4.4112 46 L 84 �3.50
10 �10 R 71 3.6462 2 R 78 3.56
NANANANANA
RI) task based on the contrast between subliminal fearful face blocks andels in each cluster. All imaging results are based on whole-brain voxelwisegroups. Group � Task interactions indicate between group differences inractivity disorder; L � left; MNI � Montreal Neurological Institute brain
netiBloc
NI C
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
ing (fMak voxthree
(mean � 0.008) and a negative DCM.B for the
833www.jaacap.org

POSNER et al.
controls (mean � �0.005). This suggests thatfor the controls, the presentation of fearfulfaces appears to have inhibited the amygdala–LPFC connections bidirectionally on the rightside, whereas in the unmedicated ADHD pa-tients the presentation of fearful faces mayhave increased bidirectional connectivity be-tween the amygdala and LPFC. We found nodifferences when comparing unmedicated andmedicated ADHD participants or when wecompared medicated ADHD participants and
FIGURE 1 Group � task interactions. Note: Thefigure shows coronal slices through the MontrealNeurological Institute (MNI) y-coordinate �10.Activations are shown in red/orange. Deactivationsare shown in blue/purple. Results are based on thecontrast: subliminal fearful face blocks versus neutralface blocks. (A) The unmedicated attention-deficit/hyperactivity disorder (ADHD) participants comparedwith the healthy controls demonstrated greateractivation in the amygdala as indicated by the greencircle. (B) The unmedicated as compared with themedicated ADHD participants demonstrated greateractivation in the right amygdala, but the differencewas not statistically significant, as indicated by thegreen arrow. (C) No differences were detected inamygdalar activation between the medicated ADHDparticipants and healthy controls, as indicated by thegreen arrow.
controls (Figure 4).
JOURN
834 www.jaacap.org
Stimulant Effects AnalysisWe conducted a nonparametric analysis by as-signing (�) or (�) values to nine analyses ofamygdalar activation and connectivity (Table 3).For example, we found that during the medi-cated sessions, amygdalar activation for theADHD youth shifted in the direction of thecontrols (Figure 2; i.e., the level of amygdalaractivation for ADHD subjects in the medicatedversus unmedicated scans become more, ratherthan less, similar to that in controls). We there-fore assigned this analysis a (�) value. Of thenine tests conducted, seven yielded findings inwhich the stimulant medication was associatedwith a normalizing effect. This was a nonrandomeffect (Kolmogorov–Smirnov Test, p � .04) andsupports the hypothesis that stimulants had anormalizing effect of amygdalar activation andamygdalar–LPFC connectivity.
DISCUSSIONOur study examined the processing of sublimi-nally presented fearful faces in youths withADHD and the effects of stimulant medicationson this processing. We found that in unmedi-cated youths with ADHD, right amygdalar hy-peractivation was associated with the presenta-tion of the fearful faces. This finding overlapswith that of another recent fMRI study in which
FIGURE 2 Parameter estimates for the activity in theright amygdala (Montreal Neurological Institute braincoordinates: x � 20, y � �10, z � �10). Note:Greater activation was detected in the right amygdala inthe unmedicated attention-deficit/hyperactivity disorder(ADHD) participants as compared with the controls (t �3.64; p � .001). Conversely, amygdalar activation inthe medicated ADHD sample did not differ significantlyfrom that in controls.
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

wrt
amawnc
dhf(ts(cwcs
AMYGDALAR FUNCTIONING IN ADHD
ADHD subjects were asked to provide subjectiveratings of fear in response to neutral faces.8
Although that task design differed from ours inimportant ways, both studies suggest that fearprocessing is associated with amygdalar hyper-activation in youths with ADHD. Our studyextends these findings by also demonstratingthat stimulant medications normalize amygdalarhyperactivation in youths with ADHD. This isconsistent with an often-noted clinical responseof improved emotional control resulting from theuse of stimulant medication.33 A recent positronemission tomography (PET) study described at-tenuated release of dopamine in the amygdala ofpatients with ADHD,34 a finding that helps ex-plain why dopaminergic agents such as stimu-lants may help to normalize amygdalar function-ing in ADHD patients.
Along with abnormal amygdalar activation,we also found abnormal connectivity betweenthe LPFC and amygdala in unmedicated ADHDparticipants. Although some studies suggest thatthe prefrontal cortex (PFC) and in particular, theorbitofrontal cortex, may be involved in the reg-
FIGURE 3 Connectivity parameters for the attention-deficit/hyperactivity disorder (ADHD) participants andhealthy controls. Note: Baseline connectivity (dynamiccausal model matrix A [DCM.A; intrinsic connectivity])was estimated between the amygdala and lateralprefrontal cortex (LPFC) separately for the left and righthemispheres. Bottom–up (amygdala¡LPFC) and top–down (LPFC¡amygdala) connection strengths wereestimated. Greater connectivity was detected in theunmedicated ADHD participants compared with controls(F1,27 � 6.5, p � .01). No difference in connectivitywas found when comparing unmedicated andmedicated ADHD participants or when comparingmedicated ADHD participants and controls.
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
Le� Right Le� Right
Control
ADHD Medicated
ADHD Unmedicated
Top-down Bo�om-up
Coup
ling
Para
met
er
Intrinsic Connec�vity
ulation of emotion,35,36 others suggest a division
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
ithin the PFC with the medial portion indexingeward and pleasure, and the more lateral por-ion indexing loss and negative affect.11,37 This
functional division of the medial and lateralportions of the PFC was supported by a recentmeta-analysis of 87 functional neuroimagingstudies involving the PFC.37 The enhancedmygdala–LPFC connectivity in ADHD patientsay therefore suggest an over-representation, or
mplification, of the negative affect associatedith fearful faces. Indeed, intense outbursts of
egative emotion, such as frustration, are quiteommon in youths with ADHD.38 Similarly, we
found that the presentation of fearful faces pro-duced a greater inhibitory effect on the amygdala–LPFC connection in the controls compared withthe unmedicated ADHD participants. This differ-ence seemed to be greater in the right amygdala–LPFC connections than on the left, consistentwith our main finding of right amygdalar hyper-activation in the unmedicated ADHD sample.Taken together, our findings support the inter-pretation that anomalous processing of negativestimuli within the amygdala and amygdala–LPFC circuit may underlie the intense, negativeemotional reactions often seen in youths with
FIGURE 4 Connectivity parameters for the attention-eficit/hyperactivity disorder (ADHD) participants andealthy controls. Note: The modulatory effect of theunctional magnetic resonance imaging (fMRI) taskDCM.B) on baseline connectivity was estimated betweenhe amygdala and lateral prefrontal cortex (LPFC)eparately for the left and right hemisphere. Bottom–upamygdala¡LPFC) and top–down (LPFC¡amygdala)onnection strengths were estimated. A statistical trendas found suggesting a larger negative DCM.B in theontrols as compared with the unmedicated ADHDample (F1,27 � 3.1, p � .09). DCM.B � dynamic
causal model matrix B (modulatory connectivity).
Task Dependent Changes in Connec�vity
0.015
0.02y
0.01
met
er
0
0.005Control
ADHD Medicated
ng P
aram
0 01
-0.005ADHD Unmedicated
Coup
li
-0.015
-0.01
Le� Right Le� Right
Top-down Bo�om-up835www.jaacap.org

POSNER et al.
ADHD. Subsequent investigations with largersample sizes and more detailed assessments ofbehavioral responses to negative stimuli shouldbe able to test this interpretation.
Several limitations of this study merit consid-eration. First, because ADHD participants werescanned twice and the controls only once, thepossibility that practice effects account for someof our findings cannot be excluded. This is un-likely, given that the ADHD participants demon-strated amygdalar hyperactivation, and practiceeffects should produce less amygdalar activation,not more. Second, the ADHD participants beganthe study on stimulant medications, and it istherefore possible that our results were the prod-uct not of ADHD but, rather, of medicationexposure itself. This is also unlikely, given ourfindings that the stimulant medications seem tonormalize neural activity. Third, the ADHD par-ticipants were not all taking the same stimulantmedication. Although stimulant medicationsoverlap considerably in their clinical effects andmechanisms of action, they may nonethelesshave different effects on the processing of fearfulfaces; a larger, follow-up study would be neces-sary to examine this possibility. Fourth, our sam-
TABLE 3 Nonparametric Analysis
Analysis Value Assigned
Right amygalar activation �
DCM.AL. amygdala¡L. LPFC �
L. LPFC¡L. amygdala �
R. amygdala¡R. LPFC �
R. LPFC¡R. amygdala �
DCM.BL. amygdala¡L. LPFC �
L. LPFC¡L. amygdala �
R. amygdala¡R. LPFC �
R. LPFC¡R. amygdala �
Note: A nonparametric analysis was conducted on the basis of the nineanalyses listed in the table. The Kolmogorov–Smirnov test examinedthe effects of stimulant medication on amygdalar activation andamygdalar–lateral prefrontal cortex (LPFC) connectivity. For each ofthe tests listed, a (�) value was assigned if the test indicated that in themedicated versus unmedicated scans, the results for the attention-deficit/hyperactivity disorder (ADHD) subjects become more, ratherthan less, similar to controls. A (–) value was assigned if the testindicated that with stimulants, the results for the ADHD patients shiftedaway from controls. DCM.A � dynamic causal model, matrix A(intrinsic connectivity); DCM.B � dynamic causal model, matrix B(modulatory connectivity); L � left; R � right.
ple size was small, and thus a follow-up study
JOURN
836 www.jaacap.org
with a larger sample is needed to establish thestability of our findings. Fifth, the thresholdbetween subliminal and supraliminal perceptionmay differ between youths with ADHD andcontrols. Thus, it is possible that for the youthswith ADHD, the presentation of the fearful faceswere, at times, supraliminal whereas for thecontrols, the presentation of the fearful facesremained subliminal. This is unlikely, given thatpost-scanning questionnaires indicate that theyouths with ADHD were no more likely than thecontrols to recall having seen the fearful faces;but this potential confound cannot be fully ex-cluded. Sixth, dynamic causal modeling is de-pendent on the construction of a priori modelsof interacting brain regions. For each model,causality (i.e., neural activity in region Acauses change in the neural activity of regionB) is mathematically specified and statisticallytested; however, as with all cross-sectionalresearch, causal versus correlational links can-not be definitively established.
In conclusion, we have shown increasedamygdalar activation in unmedicated youthswith ADHD in response to subliminal fearfulface processing, as well as the coupling of thisincreased activation with enhanced connectivitybetween the amygdala and LPFC. Finally, ourstudy demonstrates that by altering amygdalaractivation and amygdalar–LPFC connectivity,stimulant medications can have a normalizingeffect on emotional processing. &
Accepted May 20, 2011.
Drs. Posner, Maia, Wang, and Peterson, and Ms. Mechling and Ms.Oh are with the Columbia College of Physicians and Surgeons and theNew York State Psychiatric Institute in New York, NY. Dr. Nagel iswith Oregon Health and Science University in Portland, OR.
This work was supported by the American Academy of Child andAdolescent Psychiatry, Pilot Research Award (J.P.), Klingenstein ThirdGeneration Foundation (J.P., T.V.M.), National Institute of MentalHealth grants K23 MH091249 (J.P.) and K02 MH074677 (B.S.P.),National Institute of Neurological Disorders and Stroke grant K08NS52147 (B.J.N.), and National Institute on Alcohol Abuse andAlcoholism grant P60 AA010760 (B.J.N.).
Disclosure: Drs. Posner, Nagel, Maia, Wang, and Peterson, and Ms.Mechling, and Ms. Oh report no biomedical financial interests orpotential conflicts of interest.
Correspondence to: Dr. Jonathan Posner, College of Physicians andSurgeons and New York State Psychiatric Institute, Unit 74, 1051Riverside Drive, New York, NY 10032. E-mail: [email protected]
0890-8567/$36.00/©2011 American Academy of Child andAdolescent Psychiatry
DOI: 10.1016/j.jaac.2011.05.010
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

AMYGDALAR FUNCTIONING IN ADHD
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
REFERENCES1. Barkley R. Attention-Deficit Hyperactivity Disorder: a Handbook
for Diagnosis and Treatment. 3rd ed. New York: Guilford Press;2005.
2. Barkley R, Fischer M. The unique contribution of emotionalimpulsiveness to impairment in major life activities in hyperac-tive children as adults. J Am Acad Child Adolesc Psychiatry.2010;49:503-513.
3. Chronis-Tuscano A, Molina BSG, Pelham WE, et al. Very earlypredictors of adolescent depression and suicide attempts inchildren with attention-deficit/hyperactivity disorder. Arch GenPsychiatry. 2010;67:1044-1051.
4. Biederman J, Newcorn J, Sprich S. Comorbidity of attentiondeficit hyperactivity disorder with conduct, depressive, anxiety,and other disorders. Am J Psychiatry. 1991;148:564-577.
5. Whalen PJ, Rauch SL, Etcoff NL, McInerney SC, Lee MB, JenikeMA. Masked presentations of emotional facial expressions mod-ulate amygdala activity without explicit knowledge. J Neurosci.1998;18:411-418.
6. LeDoux J. The Emotional Brain. New York: Simon & Schuster;1996.
7. Plessen KJ, Bansal R, Zhu H, et al. Hippocampus and amygdalamorphology in attention-deficit/hyperactivity disorder. ArchGen Psychiatry. 2006;63:795-807.
8. Brotman M, Rich B, Guyer A, et al. Amygdala activation duringemotion processing of neutral faces in children with severe mooddysregulation versus ADHD or bipolar disorder. Am J Psychia-try. 2010;167:61-69.
9. Pessoa L, Ungerleider LG. Neuroimaging studies of attention andthe processing of emotion-laden stimuli. Prog Brain Res. 2004;144:171-182.
10. Friston K, Harrison L, Penny W. Dynamic causal modelling.NeuroImage. 2003;19:1273-1302.
11. Kringelbach M. The human orbitofrontal cortex: linking rewardto hedonic experience. Nature Rev Neurosci. 2005;6:691-702.
12. Ongur D, Price J. The organization of networks within the orbitaland medial prefrontal cortex of rats, monkeys and humans. CerebCortex. 2000;10:206-219.
13. Barbas H, Zikopoulos B, Timbie C. Sensory pathways and emo-tional context for action in primate prefrontal cortex. Biol Psychi-atry. 2011;69:1133-1139.
14. Gehring WJ, Knight RT. Lateral prefrontal damage affects pro-cessing selection but not attention switching. Cogn Brain Res.2002;13:267-279.
15. Rosenkranz JA, Grace AA. Dopamine attenuates prefrontal cor-tical suppression of sensory inputs to the basolateral amygdala ofrats. J Neurosci. 2001;21:4090-4103.
16. Rosenkranz JA, Grace AA. Cellular mechanisms of infralimbicand prelimbic prefrontal cortical inhibition and dopaminergicmodulation of basolateral amygdala neurons in vivo. J Neurosci.2002;22:324.
17. Lucas C, Zhang H, Fisher P, et al. The DISC Predictive Scales(DPS): efficiently screening for diagnoses. J Am Acad ChildAdolesc Psychiatry. 2001;40:443-449.
18. Shaffer D, Schwab-Stone M, Fisher P, et al. The DiagnosticInterview Schedule for Children—Revised version (DISC-R): I.
Preparation, field testing, interrater reliability, and acceptability. JAm Acad Child Adolesc Psychiatry. 1993;32:643-650.3
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
9. Conners C, Sitarenios G, Parker J, Epstein J. The revised Conners’Parent Rating Scale (CPRS-R): factor structure, reliability, andcriterion validity. J Abnorm Child Psychol. 1998;26:257-268.
0. Achenbach TM, Rescorla LA. Manual for ASEBA School-AgeForms & Profiles. Burlington, VT: University of Vermont, Re-search Center for Children, Youth, & Families; 2001.
1. Wechsler D. Wechsler Abbreviated Scale of Intelligence: SanAntonio, TX: Psychological Corporation; 1999.
2. Oldfield R. The assessment and analysis of handedness: theEdinburgh inventory. Neuropsychologia. 1971;9:97-113.
3. Hollingshead A. Four Factor Index of Social Status [thesis]. NewHaven, CT: Yale University; 1975.
4. Kovacs M. The Children’s Depression Inventory (CDI). Psychop-harmacol Bull. 1985;21:995-998.
5. Spielberger C, Gorsuch R. STAI Manual for the State-Trait Anx-iety Inventory. Palo Alto, CA: Consulting Psychologists Press;1970.
6. Petersen A, Crockett L, Richards M, Boxer A. A self-reportmeasure of pubertal status: reliability, validity, and initial norms.J Youth Adolesc. 1988;17:117-133.
7. Tottenham N, Borscheid A, Ellertsen K, Marcus D, Nelson C.Categorization of Facial Expressions in Children and Adults:Establishing a Larger Stimulus Set. Cognitive Neuroscience Soci-ety Annual Meeting, San Francisco, CA, April 2002.
8. Friston KJ, Ashburner CD, Frith JB, Poline JB, Heather RS,Frackowiak RS. Spatial registration and normalization of images.Hum Brain Mapping. 1995;3:165-189.
9. Mechelli A, Price C, Noppeney U, Friston K. A dynamic causalmodeling study on category effects: bottom-up or top-downmediation? J Cogn Neurosci. 2003;15:925-934.
0. Stephan K, Weiskopf N, Drysdale P, Robinson P, Friston K.Comparing hemodynamic models with DCM. NeuroImage. 2007;38:387-401.
1. Friston K. Causal modelling and brain connectivity in functionalmagnetic resonance imaging. PLoS Biol. 2009;7:e1000033.
2. Cox R. AFNI: software for analysis and visualization of functionalmagnetic resonance neuroimages. Comput Biomed Res. 1996;29:162-173.
3. Findling R, Ginsberg L, Jain R, Gao J. Effectiveness, safety, andtolerability of lisdexamfetamine dimesylate in children withattention-deficit/hyperactivity disorder: an open-label, dose-optimization study. J Child Adolesc Psychopharmacol. 2009;19:649-662.
4. Volkow N, Wang G, Newcorn J, et al. Depressed dopamineactivity in caudate and preliminary evidence of limbic involve-ment in adults with attention-deficit/hyperactivity disorder.Arch General Psychiatry. 2007;64:932.
5. Almeida J, Versace A, Mechelli A, et al. Abnormal amygdala-prefrontal effective connectivity to happy faces differentiatesbipolar from major depression. Biol Psychiatry. 2009;66:451-459.
6. Quirk G, Beer J. Prefrontal involvement in the regulation ofemotion: convergence of rat and human studies. Curr OpinNeurobiol. 2006;16:723-727.
7. Kringelbach M, Rolls E. The functional neuroanatomy of thehuman orbitofrontal cortex: evidence from neuroimaging andneuropsychology. Prog Neurobiol. 2004;72:341-372.
8. Barkley R. ADHD and the Nature of Self-Control. New York:Guilford Press; 1997.
837www.jaacap.org

.rdpwaAt
POSNER et al.
SUPPLEMENT 1Subject Instructions for the Functional MagneticResonance Imaging (fMRI) Task and Post-Scanning QuestionnaireSubjects were given the following instructions forthe fMRI task:
You will be shown several faces. Please lookat the faces and try to remember them. Afterthe MRI scan, you will be asked about thefaces that you remember seeing.
After the MRI scan, we asked subjects toidentify the faces that they recalled seeing. Theywere shown a sample of the faces presented (sixneutral faces and six fearful faces). They wereasked to circle the faces that they recalled seeing.We instructed the subjects to circle the face if theyremembered seeing both 1) the person and 2) thatperson’s facial expression.
Faces Used for the fMRI TaskWe selected 15 faces from the NimStim sample touse in the fMRI task. The characteristics of thefaces are provided in Table S1, available online.
Head Motion During ScanningWe calculated the root mean square (RMS) val-ues of the adjustments needed to realign eachsubject’s head position into the position that itwas in at the beginning of each scanning run.Only runs with less than 2 mm RMS of motionwere used in these analyses. Greater motion wasdetected in unmedicated ADHD subjects as com-pared with control subjects; however, after cor-recting for multiple comparisons, this was notstatistically significant. To control for this trendof greater motion in the unmedicated ADHDparticipants, we incorporated into each subject’slinear model six nuisance regressors reflectingmotion parameters in three translational direc-tions and rotations. The motion across the threegroups was as follows: mean RMS values forcontrols: 0.37 mm; medicated ADHD subjects:0.48 mm; and unmedicated ADHD subjects: 0.61mm; comparison of controls and medicatedADHD subjects: p �.24; comparison of controlsand unmedicated ADHD subjects: p � .05; com-parison of medicated versus unmedicated ADHDsubjects: p � .13.
Each of the three groups (unmedicated ADHDparticipants, medicated ADHD participants, and
control subjects) consisted of 15 subjects, withJOURN
837.e1 www.jaacap.org
each subject completing two runs of the fMRItask for total of 30 runs per group. The numbersof runs excluded because of excessive motion, foreach group were as follows:1. unmedicated ADHD participants: three runs
excluded (two runs from one subject and onerun from a second subject).
2. medicated ADHD participants: one run ex-cluded.
3. and control subjects: four runs excluded (tworuns from one subject and two runs fromanother subject).Based on the following nonparametric tests,
we found no evidence to suggest that the threegroups differed in terms of the number of scansexcluded because of excessive motion: ADHDunmedicated versus ADHD medicated:1. related-samples Wilcoxon signed ranks test,
p � .3.2. ADHD unmedicated participants versus con-
trols: independent-samples Kruskal–Wallistest, p � .9.
3. and ADHD medicated participants versuscontrols: independent-samples Kruskal–Wal-lis test, p � .5.
fMRI Activation Analyses—Without Covarying forDepressive and Anxiety SymptomsWe initially conducted group-level analyses byentering contrast images from the subject-levelanalyses into factorial models that included co-variates for depressive and anxiety symptoms.The results indicated that right amygdalar acti-vation was greater in unmedicated ADHD sub-jects as compared with controls (t � 3.64; p �001). We repeated these analyses without cova-ying for depressive and anxiety symptoms toetermine whether these covariates removed im-ortant variance from the analysis. The resultsere only nominally different. Right amygdalar
ctivation remained greater in the unmedicatedDHD subjects as compared with controls, al-
hough the � level changed slightly (t � 3.00; p �.004). We suspect that including depressive andanxiety symptoms as covariates had little impacton the results because the ADHD subjects andcontrols differed minimally on anxiety and de-pression measures.
Habituation AnalysisEach subject completed two runs of the fMRI
task. We reasoned that if habituation were occur-AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011

number of faces presented during the post-scanning questionnaire.
AMYGDALAR FUNCTIONING IN ADHD
ring, amygdalar activation for the contrast ofsubliminal fearful face blocks versus neutral faceblocks would be greater in run 1 versus run 2.Therefore, we generated for each subject, a con-trast image that compared: run 1 versus run 2based on the contrast of subliminal fearful faceblocks versus neutral face blocks. These contrastimages were then entered into group level anal-yses. In this analysis, greater amygdalar activa-tion in run 1 versus run 2 would suggest habit-uation. Conversely, if amygdalar activation didnot differ significantly between run 1 and run 2,habituation would be unlikely. We found noevidence for habituation in the unmedicatedADHD subjects (p � .3), medicated ADHD sub-
TABLE S1 Characteristics of the Faces Used in theFunctional Magnetic Resonance Imaging Task
Gender Race/Ethnicity Positiona
Female (n � 8) White (n � 9) Mouth open (n � 8)Male (n � 7) Asian (n � 2)
African American(n � 4)
Mouth closed (n � 7)
Note: aThe neural and fearful faces were matched according to themouth position.
jects (p � .06), or control subjects (p � .4).
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011
TABLE S2 Faces Recalled During the Post-ScanningQuestionnaire
Subject Group
Faces Recalled (%)a
NeutralFaces
Subliminal FearfulFaces
Unmedicated ADHD subjects 71 7Medicated ADHD subjects 80 7Healthy controls 83 9
Note: ADHD � attention-deficit/hyperactivity disorder.aFor each group, the number of faces recalled as percentage of the total
837.e2www.jaacap.org

POSNER et al.
TABLE S3 Group Comparisons of the Number of Faces Recalled During the Post-Scanning QuestionnaireAdministration
Comparison
Neutral Faces RecalledSubliminal Fearful Faces
Recalled
Test Statistic p Value Test Statistic p Value
Controls vs. unmedicated ADHD subjects t � 1.7 .1 t � 0.4 .7Controls vs. medicated ADHD subjects t � 0.4 .7 t � 0.4 .7Unmedicated vs. medicated ADHD subjects Paired t � 1.7 .1 Paired t � 0 1.0
Note: No group differences were detected in the number of faces recalled during the post-scanning questionnaire. ADHD � attention-deficit/hyperactivity
disorder.JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 8 AUGUST 2011837.e3 www.jaacap.org