
A multiprofessional approach to patient safety
25
Clinical pharmacy services in the EU A multiprofessional approach to patient safety Andras Sule Director of Finance, EAHP October 25, 2019
Transcript of A multiprofessional approach to patient safety

Clinical pharmacy services
in the EU
A multiprofessional approach
to patient safety
Andras Sule
Director of Finance, EAHP
October 25, 2019






Studies on the future(?) of pharmacy
• Pharmacists’ „incomplete professionality” (Denzin & Mettlin 1968)– Pharmacists have no real competence of medicines!
• The „over-educated” or „under-employed” professional image(Eaton & Webb. 1979)
• Expanding the reach of pharmacy is key for the profession’s survival. (Edmunds, Calnan. 2001).
• Health systems have recognized the concept of pharmaceutical care. (Smith, Picton, Dayan. 2014.)
– Besides ensuring a fluid supply chain, it is the (shared) responsibility of the pharmacist to ensure the success ofpharmacotherapy.
– Pharmaceutical care enables patients to achieve the best possibletherapeutic outcome with minimized medication-related risks.
Historical Perspective Up to the 1960’s, pharmacy services were performed
from a central pharmacy
often located in the basement of the hospital
services were often limited
Focus
procurement
repackaging & labeling bulk supplies
delivery to patient care areas

Floor Stock Was Still OK Boxed medications was stored on nursing stations
Nurse took medication from floor stock
Nurses prepared all intravenous (IV) medications
Potential for medication errors was very high
Mid 1960s-pharmacies assumed more accountability

Dispensing...
MENTAL
HEALTH
SERVICE
PHARMACY
TECHNICIAN
HOSPITAL
MANAGEMENT
NURSEMEDICAL
DOCTOR
ANTIMICROBIAL
STEWARDSHIP
TEAM
PHARMACIST
CLINICAL
NUTRITION
TEAM
PATIENT

Our main task…
The Vision: Am. J. Hosp. Pharm 1990.

The Reason: medication-related errors
• Medication-related errors are inadvertent mistakes in patient care, occuring atprescribing, dispensing and/or administration of medicinal therapies, potentiallyleading to patient harm.
• Medication errors are the most common causes of preventable adverse events inthe healthcare system.
• Types of medication errors:
– Prescribing error (occurrence rate: 0,3% – 9,1%*)
– Dispensing error (occurrence rate: 2,4% - 49,3%*)
• Up to 10% of harms occured result in irreversible patient harm, of which 5% provesto be lethal*.
• A complete identification of the medicine, up to its point of administration is key tosafe medication practice!
Source: European Medicines Agency Science
Medicines Health Human Medicines Research and
Development Support: Medication Errors – Follow-up
Actions from Workshop. Implementation Plan 2014-
2015. EMA/20791/2014: 1-5, 2014;

Therapeutic decision support at patient rounds
Medication reconciliation, medicinal history
Clinical laboratory follow-up and evaluation
Side-effect management
Direct patient counsel by the bedside, CAM evaluation
Main duties of clinical pharmacy services
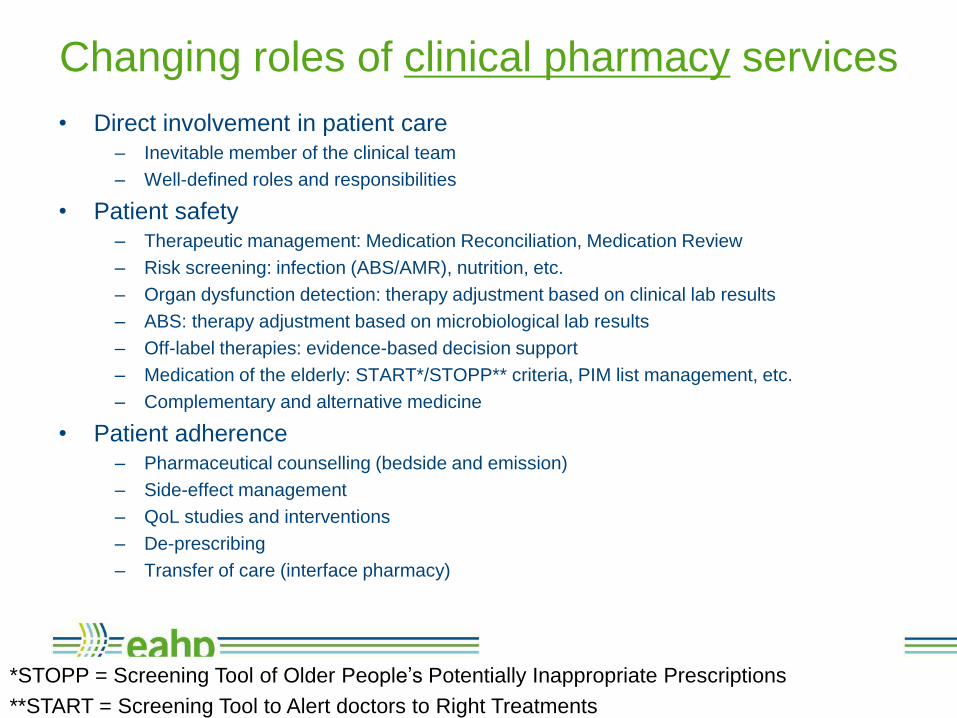
• Direct involvement in patient care– Inevitable member of the clinical team
– Well-defined roles and responsibilities
• Patient safety– Therapeutic management: Medication Reconciliation, Medication Review
– Risk screening: infection (ABS/AMR), nutrition, etc.
– Organ dysfunction detection: therapy adjustment based on clinical lab results
– ABS: therapy adjustment based on microbiological lab results
– Off-label therapies: evidence-based decision support
– Medication of the elderly: START*/STOPP** criteria, PIM list management, etc.
– Complementary and alternative medicine
• Patient adherence– Pharmaceutical counselling (bedside and emission)
– Side-effect management
– QoL studies and interventions
– De-prescribing
– Transfer of care (interface pharmacy)
Changing roles of clinical pharmacy services
*STOPP = Screening Tool of Older People’s Potentially Inappropriate Prescriptions
**START = Screening Tool to Alert doctors to Right Treatments

• Supply chain management– Procurement & Stock management
– Dispensary
• Product information, NCA liaison
• Compounding– Aseptic procedures (IV, TPN, dialysis solutions, radiopharmacy, etc.)
– Cytotoxics
– Individualized therapies (incl. small-scale GxP mfg. & magistral formulae)
• Formulary development & management– Hospital set of policies for pharmaceutics
– Including therapeutic information (protocols, interactions, etc), not only a list of approved
drugs.
• HTA based on pharmaco-economic analyses– Cost control
– Financing and reimbursement feedback
• Clinical Trial involvement
Changing roles of hospital pharmacy services

• Prudent medication management (quantitative, direct costs)
– Direct expenditure calculations
– Drug utilization analyses
– Comparative metrics
– Correlation with patient care indicators
• LOS/ALOS (Average Length of Stay)
• CPP (Cost Per Procedure)
– …
• Prudent medicine use (quantitative, indirect costs)
– Best possible outcome, lowest possible risk of treatment-related hazards
– Avoidable harms („NEVER” events: medication-related errors, adverse events)
– Side effects and complications
– Responsible use of antibiotics
– Increased therapeutic adherence of patients
– Quality of life and other standardized subjective indicators
– …
Metrics

How can EAHP help?
• Vision: enable pharmacist to truly act as experts of pharmacotherapy
• Implementation background
– Based on: European Statements of Hospital Pharmacy
• Pillars of implementation
– Education (clinical pharmacy specialization, CTF)
– „Champion” hospitals/university (SAT)
– Exchange programs (SILCC)
– Youth engagement
– Communications plan
– Collaboration with other HCPs
• Metrics(!)

Metrics development
• A toolkit for HPs that shows
– What to measure
– How to interpret the results
– Link with the Self Assessment Tool
• Evidence gathering (feed into Common Training Framework)
• Feedback gathering (from EAHP members)
• Reimbursement strategies for HP services?

Communication plan and guidance
• Provide specific action items for both EAHP and its members on how to
communicate on behalf of the HP profession with stakeholders.
• The activities of the guide should be followed-up and reinforced at
national levels via member associations.
• Statement Implementation Ambassadors’ role
• Strengthen collaboration with other HCPs
• Further expansion of the HP’s role in (direct) patient care
• Available to all EAHP members through national organizations!

Thank you for your attention!
Questions?
Andras Sule
(Director of Finance, EAHP)


















