A Canadian Perspective on Addiction Treatment
7
This article was downloaded by: [University of Saskatchewan Library] On: 19 November 2014, At: 05:04 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Substance Abuse Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wsub20 A Canadian Perspective on Addiction Treatment Nady el-Guebaly MD a a Addiction Division, University of Calgary, Calgary, Alberta, Canada Accepted author version posted online: 23 May 2014.Published online: 08 Aug 2014. To cite this article: Nady el-Guebaly MD (2014) A Canadian Perspective on Addiction Treatment, Substance Abuse, 35:3, 298-303, DOI: 10.1080/08897077.2014.923362 To link to this article: http://dx.doi.org/10.1080/08897077.2014.923362 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
Transcript of A Canadian Perspective on Addiction Treatment

This article was downloaded by: [University of Saskatchewan Library]On: 19 November 2014, At: 05:04Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Substance AbusePublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/wsub20
A Canadian Perspective on Addiction TreatmentNady el-Guebaly MDa
a Addiction Division, University of Calgary, Calgary, Alberta, CanadaAccepted author version posted online: 23 May 2014.Published online: 08 Aug 2014.
To cite this article: Nady el-Guebaly MD (2014) A Canadian Perspective on Addiction Treatment, Substance Abuse, 35:3,298-303, DOI: 10.1080/08897077.2014.923362
To link to this article: http://dx.doi.org/10.1080/08897077.2014.923362
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

A Canadian Perspective on Addiction Treatment
Nady el-Guebaly, MD
ABSTRACT. This paper presents a synopsis of addiction treatment in Canada, along with
some available comparative figures with other North American countries. Within the
framework of Canada’s Medicare, a largely single-payer system, addiction and psychiatric
disorders are insured on par with other medical disorders. Canada’s strategy recognizes the
four pillars of prevention, treatment, harm reduction, and enforcement. The Canadian
Alcohol and Drug Use Monitoring Survey is the yearly main source of data on alcohol and
illicit drug use. The main features of the Canadian addiction treatment network are identified
as a “top 10” list, outlining early identification and intervention, assessment, and referral;
detoxification; ambulatory care/day treatment programs; residential care; hospitals;
concurrent disorders networks and regionalization; drug specific strategies; mutual help;
behavioral addictions; and training, qualification, and research.
Keywords: Addiction treatment, Canada, drug strategy
INTRODUCTION
Canada is the second largest country in the world, and its geo-
graphic footprint is larger than Europe. The general principles
concerning the delivery of health care in the country’s 10 provin-
ces and 3 territories are remarkably congruent overall.
Canada’s Medicare
Since 1967, the country has enjoyed a national Medicare insur-
ance. The principles underpinning Medicare are a single-payer
system and public administration provided by the federal and pro-
vincial governments through taxation. Other principles involve
universal coverage for all citizens and insurance portability across
the country. The last principle is a promise of accessibility to all
medically necessary services.1,2 The report “More for the Mind”
is credited for ensuring a parity of coverage by Medicare to addic-
tion and psychiatric disorders equivalent to other medical disor-
ders.3 Although these principles still largely apply, Canada is
possibly the western country where a promise of universal cover-
age for all medically necessary services has been kept the longest,
for 45 years.
These principles face a mix of challenges, including rising
costs, successful medical advances in the management of an ever-
expanding range of disorders, a plethora of new medications, an
aging population, and rising consumer expectations. The health
indicators in Table 1 show that, although the proportion of health
expenditures as a percentage of the gross domestic product (GDP)
remains one third lower than in the United States (US), the public
expenditures cover only 70% of the costs.1 The rest, such as outpa-
tient medication, is from private insurance or out-of-pocket. The
lower expenditures in Canada are due mainly to the lower admin-
istrative costs resulting from the single-payer system. Increasing
waitlists for a range of nonacute services are now prompting a
reconsideration of the tenets of Medicare, including its long-term
sustainability. Repeated population surveys support Medicare as a
critical ingredient of the national fabric.
Canada’s Drug Strategy
The federal government’s key initiative to address the harmful
effects of substance use and abuse on individuals, families, and
communities in coordination with the provinces is described in its
drug strategy, with the four pillars of prevention, treatment, harm
reduction, and enforcement.2 The Canadian Centre on Substance
Abuse (CCSA) is the body mandated to spearhead the activities
emanating from such a strategy and, with the federal government,
plays largely a standard-setting role.
Prevention
The most visible federal activities include mass media aware-
ness campaigns, such as anti-smoking advertisements and regular
health warnings. The federal government, through its National
Native Alcohol and Drug Abuse Program (NNDAP), aims specifi-
cally at preventing alcohol and other drug abuse among First
Nations people and Inuit.4 Recently, programs to manage posttrau-
matic stress disorder and its sequelae, such as substance use disor-
ders, have been prioritized by the Armed Forces.5
Provincially, a range of approaches are implemented, such as
school programs; community-based programs for high-risk
Addiction Division, University of Calgary, Calgary, Alberta, Canada
Correspondence should be addressed to Nady el-Guebaly, MD, Foot-
hills Hospital, Addiction Centre, 1403 29th Street NW, Calgary, Alberta,
T2N 2T9, Canada. E-mail: [email protected]
SUBSTANCE ABUSE, 35: 298–303, 2014
Copyright� Taylor & Francis Group, LLC
ISSN: 0889-7077 print / 1547-0164 online
DOI: 10.1080/08897077.2014.923362
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14

populations; recreational activities for youth groups; family-based
approaches; and policies against drug use and possession in the
school as well as the workplace, particularly for safety-sensitive
positions.
Treatment and rehabilitation
The Canadian Centre on Substance Abuse database on addic-
tion organizations (including gambling) lists more than 2500 such
organizations.6 Provinces, territories, and local communities fund
more than 1000 drug and alcohol treatment and rehabilitation pro-
grams, varying in their approach, philosophy, principles, and
goals. Canada supports opioid agonist therapy. A registry of physi-
cians able to prescribe methadone was instituted federally and
only recently delegated to provincial licensing boards. The restric-
tions on prescribing vary between provinces but all potential pre-
scribers are required to undergo an initiation course. The
prescription of buprenorphine is limited to those physicians on the
methadone registry.7
Harm reduction
The third pillar of the drug strategy, harm reduction, aims at
reducing the health and social harms related to substance use and
abuse and grew in the 1980s from the goal of reducing the risks of
blood-borne diseases (i.e., human immunodeficiency virus/
acquired immunodeficiency virus [HIV/AIDS], hepatitis) among
intravenous drug users (IDUs). Harm reduction accepts the fact
that some users cannot or will not stop using psychoactive sub-
stances, particularly at the early steps of their treatment engage-
ment. The panoply of harm reduction measures include
community-based outreach programs targeted at marginalized
populations and providing them with low-threshold services, such
as needle exchange programs and, more recently, clean pipes for
crack users; methadone maintenance programs; and a clinic for
supervised use for heroin.8 Although these expanding measures
regularly test the population’s tolerance and values, overall, they
are remarkably well accepted.
Enforcement and control
From the need to reduce both the supply and demand for drugs,
the Controlled Drugs and Substances Act (CDSA) “provides the
framework for the control, import, production, export, distribution,
and possession of psychoactive substances.”2 The Royal Canadian
Mounted Police (RCMP) is responsible for enforcing the CDSA in
collaboration with provincial and municipal police forces. Argu-
ments for a less costly strategy of drug decriminalization are regu-
larly made and face challenges ranging from potential public
safety issues to Canada’s obligations under international treaties.
Harm reduction measures, such as the availability of methadone,
are being progressively adopted in correctional institutions.
FEATURES OF CANADIAN ADDICTIONTREATMENT
Although Canadian addiction treatment is national and provincial,
10 selected aspects are considered critical to promote reduction of
the harms of illicit and unhealthy alcohol and drug use.
Early Identification and Intervention, Assessment,and Referral
Like in the US, concerted effort is ongoing to reach out to family
physicians and other primary care providers beyond a few pilot
projects and establish sustainable parameters for early identifica-
tion of substance use and intervention.9 Canada’s population has
traditionally benefited from ready access to a family physician.
Recent challenges in the recruitment of these physicians has pro-
moted a paradigm shift from solo to group primary care practices,
with the added incentive of funded multidisciplinary support for
TABLE 1
Snapshot of Indicators in Health Across North America
Indicator Year Canada USA Mexico
Health expenditure
Total as% of GDP 2010 11.4 17.6 6.2
Public as% total 2010 71.1 48.2 47.3
Resource
Physicians/1000 population 2010 2.4 2.4 2.0
Hospital beds/1000 population 2009 3.2 3.1 1.7
Life expectancy at birth—Female 2010 83.1 (2008) 81.1 77.8
Life expectancy at birth—Male 2010 78.5 (2008) 76.2 73.1
Infant mortality/1000 live births 2010 5.1 (2008) 6.1 14.1
Suicide rates/100,000 population 2009 11.1 12.0 (2008) 5.0
% Adults reporting good health—Male 2007 89 89 67
% Adults reporting good health—Female 2007 88 87 64
AIDS incidence rates (new cases/million population) 2006 9.5 127.0 45.3 (2003)
% Females with obesity 2008 23.3 35.5 34.5 (2006)
% Males with obesity 2008 25.2 32.2 24.2 (2006)
Daily smokers as% population 2010 16.3 15.1 13.3 (2006)
Alcohol consumption (L/capita): Age 15C 2009 8.2 8.7 5.9 (2008)
Note. Adapted from OECD Health, 2013.
N. EL-GUEBALY 299
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14

the groups. These Practice Community Networks (PCNs), as they
have been called in Alberta, have their counterparts in an expand-
ing number of provinces. Start-up initiatives have targeted the
reduction of use of tobacco and are credited for a significant reduc-
tion in national prevalence to the current 17.5%. The early identifi-
cation efforts to address other substances, such as alcohol and
marijuana, are more limited, despite the fact that they are also
common among the population above age 15, i.e., past 12 months’
use of alcohol is 76.5%, whereas cannabis is 10.6%.10,11
Detoxification
A national network of so-called “nonmedical” detoxification cen-
ters is available in most urban centers. In these centers, physicians
are part-time consultants. The Canadian Alcohol and Drug Use
Monitoring Survey (CADUMS) 2009 reports that 5.1% of Cana-
dians were heavy frequent drinkers in the past year (consumption
of 5C drinks 1 or more times per week).11 An internationally
known scale to assess the severity of alcohol withdrawal has been
the Clinical Institute Withdrawal Assessment—Alcohol (CIWA),
created by the Addiction Research Foundation in Canada and
monitored by nursing staff.12 Sensitive detoxifications, including
in pregnancies as well as polysubstance abuse, would be referred
to a neighboring hospital.
Ambulatory Care/Day Treatment Programs
A focus on ambulatory, rather than residential or hospital, care has
been an early feature of the Canadian Medicare System. Screening
and brief intervention are mostly delivered through primary care,
with specialized addiction treatment clinics of various sizes and
range of services, as back-up, available in most urban centers.
Patients discharged from these specialized treatment settings are
referred back to their primary physician for follow-up and medical
monitoring of their recovery.
Residential Care
Various levels of residential care for both genders are available in
urban centers as well as rural areas, and they mostly receive local
referrals. A formalized grid of level of care is not available in Can-
ada. Contrary to the US, the emergence of major interstate referral
centers, such as Hazelden or Betty Ford Center, has been limited
in Canada. A network of “interventionists” providing intervention
services and referring to these centers is practically nonexistent. A
select number of residential programs, such as Homewood Hospi-
tal and Bellwood Treatment Centre in Ontario and Edgewood
Centre in British Columbia, receive referrals from Worker’s Com-
pensation, Armed Forces, and the Police forces, who have supple-
mentary benefits to Medicare. Residential programs are not
funded by Medicare, except for related physicians’ services and
charge a variable admission fee. Residential programs are partly
funded by sources other than Medicare. A limited number of rela-
tively wealthy Canadians travel to residential programs in the US
for their care.
Hospitals
General hospitals have very few departments of addiction medi-
cine or addiction psychiatry and rarely identify designated beds
for the care of addicted patients. Access to beds most frequently is
through a range of admitting physicians, with consultations pro-
vided by specialists in addiction medicine or psychiatry. Desig-
nated beds, mostly for concurrent disorders are, however,
available in provincial Mental Health Centres.
Concurrent Disorders Networks and Regionalization
Over the last few years, a major national effort has been to inte-
grate administratively both addiction and mental health services.
Based on a best-practices document from Health Canada, the inte-
gration of the two cultures has been challenging, while prioritizing
a continuum of care through case management.13 In Alberta, for
example, the parameters of a concurrent disorders system
approach involve a welcoming and engaging consumer strategy, a
working knowledge of addiction and mental health disorders, a
standard approach to screening, a comprehensive assessment, inte-
grated treatment planning, comprehensive interventions, case
management and service coordination, and continuous care recog-
nizing the chronic nature of the disorders involved.14
Another major development, at the same time, has been a pol-
icy to regionalize the delivery of health care. With a single-payer
system, the planning of services on a regional basis enhances the
coordination and continuum of care. Models of comprehensive
delivery of services have been drafted in most provinces. An
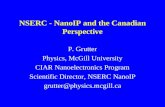
example would be the Progressive and Integrated Recovery
(PaIR) model, originating in southern Alberta (see Figure 1).15
This model recognizes that at any one time, most residents suffer-
ing from substance use disorders would not be ready to change. Of
those ready to do so, a stepped care model is proposed, matching
the level of intervention to patient needs and preference. The plan-
ning of a recovery process is also included.
Drug-Specific Strategies
Aside from a tobacco strategy, focused on primary care, other
drug-specific strategies include the following.
The options of opioid management
According to the United Nations Office on Drugs and Crime
(UNODC), Canada’s prevalence for opiates in the population age
range of 15–64 is 0.68% for opioids, 0.36% for opiates, and 0.5%
for prescriptions (see Table 2). Opioids are the primary drug of
abuse for 22% of persons treated with drug problems (see
Table 3).
Canada has been an early adopter of methadone as far back as
the early 1960s (Dr. Robert Halliwell in Vancouver). More than
1000 physicians are now registered with their provincial licensing
colleges to prescribe methadone, mostly in specialized clinics.7
The prescription of buprenorphine has been mostly limited to
physicians on the methadone registry, with the result that the
incorporation of its prescription into primary care practices has
been limited.
Over the last 6 years, the North American Opiate Medication
Initiative (NAOMI) project in Vancouver, a controlled clinical
trial of heroin maintenance funded by the Canadian Institute of
Health Research (CIHR), has made headlines in the media.16 A
successful outcome has been reported in top medical publica-
tions.17 Insite, the clinic where the supervision occurred, was
threatened with closure by the federal government as contravening
300 SUBSTANCE ABUSE
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14

the CDSA but won a landmark ruling by Canada’s Supreme Court
that upheld its right to exist through an exemption.
Codeine is currently a source of public concern. In 2009,
CADUMS reported that 25% of respondents used a psychoactive
pharmaceutical in the past year, but only 2.3% of these users used
such drug to get high. Among the youth, 15 to 24 years of age,
9.5% of current users reported such use to get high (1.7% of
population). Opioid pain relievers were the most common cate-
gory of pharmaceuticals used (19.2%), and of these, 2.3% used
them to get high. Among the youth, this percentage was much
higher, 8.5%. The Canadian Society of Addiction Medicine has
developed a position paper outlining opioid prescription guide-
lines.18 Among users of stimulants, 9.4% used them to get high in
the past 12 months, and among users of sedatives or tranquilizers,
1.7% used them to get high.
Cannabis and medical marihuana
CADUMS reports in 2009 that the prevalence of past-year can-
nabis use among Canadians 15 years and older was 10.6%, statis-
tically significantly lower than the rate of 14.1% reported in 2001.
Despite the decline, the prevalence of use by youth was 26.3%. In
general, male’s use was twice as high as females.11
Two oral medications, a chemically synthesized tetrahydrocan-
nabinol (THC; Marinol) and nabilone (Cesamet), a synthetic can-
nabinoid, are readily available. In 2001, public pressure prompted
the federal government to introduce a medical access regulation
under the CDSA. Since then, persistent consumer advocacy, con-
sistent with other countries, has occurred to increase the availabil-
ity of smoked marihuana for an ever-expanding range of disorders
despite limited scientific evidence of the benefits of its
FIGURE 1. The Progressive and Integrated Recovery model.
TABLE 2
Annual Prevalence as a Percentage of the Population Aged 15–64
Across North America
Drug Canada USA Mexico
Opiates
Opioids 0.68 5.90 0.08
Opiates 0.36 0.57 0.04
Prescription opioids 0.5 5.60 0.06
Cocaine 1.4 2.40 0.4
Cannabis 12.6 13.7 1.0
Amphetamines 0.7 1.5 0.2
Ecstasy 1.1 1.4 <0.1
Source: UNODC World Drug Report 2011 Statistical Annex (http://
www.unodc.org/documents/data-and-analysis/WDR2011/World_Drug_
Report_2011_ebook.pdf).
N. EL-GUEBALY 301
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14

administration through smoking and larger evidence of side effects
akin to tobacco use.19 There is growing popular consensus in Can-
ada on the need to decriminalize the possession of marihuana as
well as differentiate the therapeutic promises of cannabinoids
from the mode of administration through smoke inhalation.20 The
Canadian Medical Protective Association has successfully warned
physicians of potential compromise in their practice insurance
resulting from the prescription of smoked marihuana. The federal
government will now allow physicians to write prescriptions that
would be filled by licensed suppliers.21
Options for nicotine and alcohol
The use of nicotine replacement therapies and other medica-
tions to control tobacco use has been widespread. Recent attempts
to promote the use of anti-craving medication, including naltrex-
one or acamprosate, have been met with skepticism due to their
low effect size. Unfortunately, this has led to some reluctance by
insurers to adopt newer promising pharmaceutical products in the
field.
Mutual Help
Mutual help originated in Canada in 1902, with the Ontario Soci-
ety for the Reformation of Inebriates. Currently, Alcoholics Anon-
ymous and other 12-Step mutual help groups are available in
every urban or rural center. Other groups, including SMART
Recovery (Self Management and Recovery Training), Women for
Sobriety, and Gamblers Anonymous are also available but on a
more limited basis. The concept of recovery and its requirements
promoted by mutual help groups is now receiving widespread
attention from planners and decision makers as a potential new
paradigm for the delivery of addiction and mental health
services.22
Behavioral Addictions
In Canada, provincial governments are both the regulators and
major recipients of gambling revenue. Compared with the US,
governments have funded an extensive research network aimed at
studying the risks of problem gambling as well as creating a num-
ber of specialized treatment programs. Other behavioral addic-
tions, such as Internet and sex addictions, are addressed much
more sporadically and, to our knowledge, struggle to establish a
treatment network as yet.23
Training, Qualification, and Research
The training of medical students in substance use disorders in the
18 medical schools remains marginal.10 National training require-
ments have been established for psychiatric residents and are
developing in family practice.24
The qualification of physicians is the jurisdiction of the College
of Family Physicians and the Royal College of Physicians and
Surgeons. Traditionally, both colleges, worried about fragmenta-
tion of the practice of medicine, have promoted the training of
generalists in the traditional specialties. Recently, the College of
Family Physicians has recognized special interest or focused prac-
tices and the Royal College may offer a diploma recognition
requiring an extra year of training.25 Recognizing the complemen-
tary roles of family physicians and specialists, a model of collabo-
rative care is being proposed to modify the training requirements
of addiction medicine leading to potential certification by either
the International or the American Medical Society of Addiction
Medicine.26 In addition, a major effort to flesh out the required
competencies for a multidisciplinary workforce is ongoing.27 Fel-
lowships in addiction medicine/psychiatry in training centers such
as Calgary, Toronto, and Vancouver are emerging, funded through
the reallocation from existing residency training spots or through
philanthropic donations.
Under the aegis of the Institute for Neurosciences, Mental
Health, and Addiction (INMHA), one of the institutes of CIHR,
the field of addiction is added to the neurological and mental
health portfolios, creating some discrepancy in visibility. Access
by Canadian researchers to the support of the National Institute of
Drug Abuse (NIDA) and the National Institute of Alcohol Abuse
and Alcoholism (NIAAA) in the US is welcomed. Leading
research efforts include studies on tobacco, psychiatric comorbid-
ities, opiates and the NAOMI project, cannabis, and gambling
research.
SUMMARY
This snapshot of Canadian addiction treatment highlights assets
such as the presence of parity in insurance coverage for both
addiction and mental health as well as 10 selected features of our
TABLE 3
Primary Drugs of Abuse Among Persons Treated for Drug Problems Across North America
Drug Canada (Ontario) % USA % Mexico %
Opioids 22.0 34.1 18.2
Cocaine group 33.4 19.5 26.9
Cannabis 32.5 29.3 21.2
Amphetamine-type stimulants 3.1 10.9 17.9
Ecstasy 2.4 — —
Solvents and inhabitants 0.6 0.1 11.4
Sedatives and tranquilizers 3.9 1.5 2.3
Drug-related deaths (rate per million aged 15–64) 93.3 182.4 63.9
Hepatitis C among IDUs 69 Unknown 96
Source: UNODC World Drug Report 2011 Statistical Annex (http://www.unodc.org/documents/data-and-analysis/WDR2011/World_Drug_Report
_2011_ebook.pdf).
302 SUBSTANCE ABUSE
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14

delivery of care. In a climate of economic constraints and the con-
cern of policy makers about the rising costs of health care, one
must address the additional challenge of stigma while advocating
for our patients. Compared with other visible health consumer
groups, the anonymity of our major mutual help groups may pres-
ent an additional advocacy hurdle. A vocal group of opiate users
recently were instrumental in gaining the support of Canada’s
Supreme Court. The struggle continues for meeting the needs of
our patients, providing the highest possible standard of empirically
based care, and ensuring a competent workplace to staff our
resources.
REFERENCES
[1] Organization for Economic Co-operation and Development (OECD).
OECD health data Web site. Available at: http://www.oecd.org/els/
health-systems/oecdhealthdata2013-frequentlyrequesteddata.htm.
2013. Accessed March 4, 2014.
[2] Collin C. Substance Abuse Issues and Public Policy in Canada: I.
Canada’s Federal Drug Strategy PRB06-15E. Ottawa: Parliamentary
Information and Research Service, Library of Parliament; 2006.
[3] Tyhurst JS, Chalke FCR, Lawson FS, et al. More for the Mind: A
Study of Psychiatric Services in Canada. Toronto: Canadian Mental
Health Association; 1963.
[4] Health Canada’s National Native Alcohol and Drug Abuse Program
(NNADAP). Web site. Available at: http://www.hc-sc.gc.ca/fniah-
spnia/pubs/substan/_ads/1998_rpt-nnadap-pnlaada/index-eng.php.
Accessed May 1, 2013.
[5] Veterans Affairs Canada. Mental health. Available at: http://www.
veterans.gc.ca/eng/mental-health. Accessed March 4, 2014.
[6] Canadian Centre on Substance Abuse. About the database of addic-
tions organizations in Canada. Available at: http://www.ccsa.ca/Eng/
KnowledgeCentre/OurDatabases/AddictionsOrganizations/Page/
AbouttheDatabaseofAddictionsOrganizationsinCanada.aspx.
Accessed May 1, 2013.
[7] Luce J, Strike C. A cross-Canada scan of methadone maintenance
treatment policy developments. Canadian Executive Council on
Addiction, Toronto, January 2011. Available at: http://www.ccsa.ca/
ceca/pdf/CECA%20MMT%20Policy%20Scan%20April%202011.
pdf. Accessed May 1, 2013.
[8] Wood E, Tyndall MW, Zhang R, et al. Attendance at supervised
injecting facilities and use of detoxification services. N Engl J Med.
2006;354:2512–2514.
[9] Substance Abuse and Mental Health Services Administration
(SAMHSA) - Center for Integrated Health Solutions, Department of
Health and Human Services. SBIRT: screening, brief intervention,
and referral to treatment. Available at: http://www.integration.
samhsa.gov/clinical-practice/sbirt. Accessed March 4, 2014.
[10] Midner D, Kahan M, Wilson L, and Borsoi D. Medical faculty mem-
bers’ perspectives on substance use disorders: a survey and focus-
group study. Ann R Coll Physicians Surg Can. 2002;35(8 Suppl
1):1–6.
[11] Health Canada. Canadian Alcohol and Drug Use Monitoring Survey
(CADUMS–2009) Web site. Available at: http://www.hc-sc.gc.ca/
hc-ps/drugs-drogues/stat/_2011/summary-sommaire-eng.php. Pub-
lished 2011. Accessed May 1, 2013.
[12] Sullivan JT, Sykor T, Schneiderman J, et al. Assessment for alcohol
withdrawal: the revised Clinical Institute Withdrawal Assessment for
Alcohol Scale. Br J Addict. 1989;84:1353–1357.
[13] Centre for Addiction and Mental Health. Best Practices. Concurrent
Mental Health and Substance Use Disorders. Toronto: Health Can-
ada; 2010.
[14] Alberta Health Services. Every door is the right door. Alberta Health
Services Web site. Available at: http://www.albertahealthservices.ca/
careers/page405.asp. Accessed May 10, 2013.
[15] el-Guebaly N, Daniels K, Winsor T. Capturing the role of the health
region in the management of addictions: the PAIR Model. In Issues
of Substance 2007: National Conference; Edmonton, Alberta;
November 25–28, 2007. Ottawa: Canadian Centre on Substance
Abuse; 2007.
[16] NAOMI project Web site. Available at: http://www.naomistudy.ca/
pdfs/noami_faq.pdf. Accessed May 1, 2013.
[17] Oviedo-Joekes E, Brissette S, Marsh David C, et al. Diacetylmor-
phine versus methadone for the treatment of opioid addiction. N
Engl J Med. 2009;361:777–786.
[18] Kahan M, Lim R, el-Guebaly N. CSAM position statement on opioid
prescribing for chronic non-cancer pain. CSAM Web site. Available
at: http://www.csam.org/non_member/policy/UseOfOpiods.aspx.
Published 2011. Accessed May 1, 2013.
[19] Canadian Society of Addiction Medicine. Medicinal use of cannabis:
perspectives and policy statement. CSAM Web site. Available at:
http://www.csam.org/non_member/policy/MedicinalUseOfCannabis.
aspx. Published 2012. Accessed May 1, 2013.
[20] el-Guebaly N. Forum: for a balanced and integrated legislated con-
trol of cannabis. Curr Opin Psychiatry. 2008;21:116–121.
[21] Health Canada. Marihuana for medical purposes regulations. Avail-
able at: http://gazette.gc.ca/rp-pr/p2/2013/2013-06-19/html/sor-dor
s119-eng.php. Accessed 25 July 2013.
[22] el-Guebaly N. The meanings of recovery from addiction: evolution
and promises. J Addict Med. 2012;6:1–9.
[23] Mudry TE, Hodgins DC, el-Guebaly N, et al. Conceptualizing exces-
sive behavior syndromes: a systematic review. Curr Psychiatr Rev.
2011;7:138–151.
[24] Crockford DN, el-Guebaly N. Addiction psychiatry. In: Leverette JS,
Hnatko GS, Prasad E, eds. Approaches to Postgraduate Education in
Psychiatry in Canada: What Educators and Residents Need to
Know. Ottawa: Canadian Psychiatric Association; 2009:167–182.
[25] el-Guebaly N, Crockford D, Cirone S, Kahan M. Addiction med-
icine in Canada: challenges and prospects. Subst Abus. 2011;
32:93–100.
[26] Kates N, Mazowita G, Lemire F, et al. The evolution of collaborative
mental health care in Canada: a shared vision for the future. Can J
Psychiatry. 2011;56:Insert 1–10.
[27] Canadian Centre on Substance Abuse. Behavioral Competencies for
Canada’s Substance Abuse Workforce. Ottawa: Canadian Centre on
Substance Abuse; 2010.
N. EL-GUEBALY 303
Dow
nloa
ded
by [
Uni
vers
ity o
f Sa
skat
chew
an L
ibra
ry]
at 0
5:04
19
Nov
embe
r 20
14