A-1 Q-Pan H5N1 Influenza A (H5N1) Virus Monovalent Vaccine, Adjuvanted Donna Boyce Head North...
100
A-1 Q-Pan H5N1 Influenza A (H5N1) Virus Monovalent Vaccine, Adjuvanted Donna Boyce Head North America, Global Regulatory Affairs GlaxoSmithKline Vaccines
-
Upload
madisyn-goldson -
Category
Documents
-
view
216 -
download
1
Transcript of A-1 Q-Pan H5N1 Influenza A (H5N1) Virus Monovalent Vaccine, Adjuvanted Donna Boyce Head North...

A-1
Q-Pan H5N1Influenza A (H5N1) Virus
Monovalent Vaccine, Adjuvanted
Donna BoyceHead North America, Global Regulatory Affairs
GlaxoSmithKline Vaccines
A-2
Introduction Donna BoyceHead, North AmericaGlobal Regulatory Affairs
Immunogenicity & Effectiveness
Bruce Innis, MDVice PresidentVaccine Discovery and Development
Safety Felix Arellano, MDVice PresidentVaccines Clinical Safety and Pharmacovigilance
Conclusion Donna Boyce
GSK Presentation

A-3
BARDA / GSK Partnership:Develop & License Q-Pan H5N1
• HHS Pandemic Influenza Plan encourages manufacturers to develop pandemic vaccines
• GSK / BARDA partnership to develop and submit for licensure H5N1 vaccine with antigen-sparing potential
• Vaccine will be distributed by US Government
• US Government will determine use of vaccine

A-4
Q-Pan H5N1 Desired Characteristics
• Acceptable reactogenicity and safety profile
• Rapid induction of protective immune responses in immunologically naïve persons
• Antigen-sparing
• Rapid production using existing facilities and processes

A-5
Q-Pan H5N1 Proposed Indication and Usage
• Intended for active immunization for the prevention of disease in persons 18 years of age and older who are at increased risk of exposure to the H5N1 influenza virus subtype contained in the vaccine
• 2-dose series (0.5 mL each) by intramuscular injection
• ~21 days interval between doses

A-6
FluLaval(Accelerated Approval)Quebec
(Q)
Q-Pan H5N1
Q-Pan H1N1
Fluarix(Traditional Approval)Dresden
(D)
D-Pan H5N1
D-Pan H1N1
Seasonal Pandemic
Q-QIV
D-QIV
GSK’s Influenza Vaccines

A-7
Q-Pan H5N1 Registered in 30 Countries
Q-Pan H5N1 Under Review
Q-Pan H5N1

A-8
GSK’s H1N1 Pandemic Experience: Registered in > 50 Countries Worldwide
Quebec & Dresden H1N1 Registrations
> 90 Million Doses Administered

A-9
Q-Pan H5N1: Two Component Vaccine
H5N1 Antigen
• Egg-based inactivated, split A/H5N1 influenza type A virus (A/Indonesia/5/2005)
• Manufactured in Quebec (Q) according to FluLaval® process
AS03 Adjuvant System
• D, L-α-tocopherol, squalene & polysorbate 80
• Manufactured in Belgium
Final Vaccine Composition (0.5 mL dose)10 doses per vial
3.75 µg HA per doseD,L-α-tocopherol (11.86 mg), squalene (10.69 mg) & polysorbate 80 (4.86 mg)
5 µg thimerosal per dose
Mixed 1:1 Prior to Injection

A-10
Pathway for Accelerated Approval of Q-Pan H5N1
US Licensed Seasonal Influenza Vaccine
Accelerated Approval
Efficacy not yet confirmed
Source
FluLaval
Pre-approval
2006
2012 BLA
2013
During a Pandemic
Timing
Q-Pan H5N1 licensure approach: Accelerated Approval
• Safety• Immunogenicity
Q-Pan H5N1-001Q-Pan H5N1-002
Effectiveness of Q-Pan H5N1 inferred when the efficacy of the seasonal confirmed
FluLavalQ-QIV-006
Post-approval
Work with US Gov’t to collect safety/effectiveness data
with Q-Pan H5N1CBER Guidance

A-11
Large and Comprehensive Development Program
N = number of subjects receiving active or control vaccine (Total Vaccinated Cohort)( ) = subjects receiving final formulation of vaccine (Q-Pan 3.75 µg HA + AS03A) or any formulation with AS03 for ISS
Supportive H1N1
EffectivenessStudies
Pivotal StudiesN=5,341 (3,574)
Supportive Dosing Interval and
Booster StudiesN=1,153 (431)
Dose FindingStudy
N=400 (0)
Q-Pan-009Short Interval
18-64 years
Q-Pan-005Long Interval
≥ 18 years
Q-Pan-010Boost 00118-64 years
D-PanH5N1-00718-64 years
Q-Pan-001Dose
Confirmation18-64 years
Q-Pan-002Safety,
Consistency≥ 18 years
New Brunswick6 mo-9 years
Manitoba≥ 6 months
CanadaMulti-Province
≥ 6 months
SupportiveSafety
SummariesN=22,521 (16,160)
H5N1ISS-1 [2009]
≥ 18 years
H5N1+H1N1ISS-2 [2011]
≥ 18 years
BLA Database
Q-QIV-006Absolute Vaccine Efficacy
3-8 years
Q-Pan H1N1-035Relative Vaccine Efficacy
6 mo-8 years
Post-Licensure Commitment Key Supportive Data

A-12
Introduction Donna BoyceHead, North AmericaGlobal Regulatory Affairs
Immunogenicity & Effectiveness
Bruce Innis, MDVice PresidentVaccine Discovery and Development
Safety Felix Arellano, MDVice PresidentVaccines Clinical Safety and Pharmacovigilance
Conclusion Donna Boyce
GSK Presentation

A-13
Immunogenicity and Effectiveness Outline
• Rationale for addition of AS03 to Q-Pan H5N1
• Q-Pan H5N1 immunogenicity data
• Clinical endpoint data from vaccines manufactured using Quebec process

A-14
CBER Immunogenicity Criteria
CBER’s Immune ResponseThresholds
Sero-conversion rate (SCR)
Proportion with a 4-fold increase in HI titers (note: if < 1:10 at baseline, must increase to at least 1:40)
LL 95% CI ≥ 18-64 years: 40% ≥ 65 years: 30%
Sero-protection rate (SPR)
Proportion with HI titers ≥ 1:40
LL 95% CI ≥ 18-64 years: 70% ≥ 65 years: 60%
In some human challenge studies of seasonal influenza viruses, HI titers of ≥ 1:40 have been associated with protection from illness
in up to 50% of subjects

A-15
A Pandemic Vaccine Optimally Should Be Effective at Antigen-Sparing Doses
• Licensed H5N1 vaccine (no adjuvant) at 90 µg HA x2 weakly immunogenic
• Whole virus adsorbed to aluminum limited antigen-sparing
• AS03 – Amenable to stockpiling and surge production– Antigen-sparing relative to licensed vaccine– Enhanced immunologic priming after 1 dose– Strong homologous (and cross-reactive) responses to 2 doses
Hehme et al., International Conference on Influenza Vaccines the World, 18-20 October 2006, Vienna, AustriaGarçon et al., Expert Rev. Vaccines 2012; 11(3), 349–366

A-16
AS03 Elicits an Enhanced, Transient, Local Innate Immune Response
• Co-injection of AS03 + antigen is necessary for effect
• Induces a transient innate immune response at the injection site and draining lymph nodes
• Accounts for– Injection site reactions– Potent humoral and cellular adaptive immune
response
Morel et al., Vaccine 2011; 29:2461-2473
Characterized in vivo in mice, ex vivo in human cells

A-17
Large and Comprehensive Development Program
N = number of subjects receiving active or control vaccine (Total Vaccinated Cohort)( ) = subjects receiving final formulation of vaccine (Q-Pan 3.75 µg HA + AS03A) or any formulation with AS03 for ISS
Supportive H1N1
EffectivenessStudies
Pivotal StudiesN=5,341 (3,574)
Supportive Dosing Interval and
Booster StudiesN=1,153 (431)
Dose FindingStudy
N=400 (0)
Q-Pan-009Short Interval
18-64 years
Q-Pan-005Long Interval
≥ 18 years
Q-Pan-010Boost 00118-64 years
D-PanH5N1-00718-64 years
Q-Pan-001Dose
Confirmation18-64 years
Q-Pan-002Safety,
Consistency≥ 18 years
New Brunswick6 mo-9 years
Manitoba≥ 6 months
CanadaMulti-Province
≥ 6 months
SupportiveSafety
SummariesN=22,521 (16,160)
H5N1ISS-1 [2009]
≥ 18 years
H5N1+H1N1ISS-2 [2011]
≥ 18 years
BLA Database
Q-QIV-006Absolute Vaccine Efficacy
3-8 years
Q-Pan H1N1-035Relative Vaccine Efficacy
6 mo-8 years
Post-Licensure Commitment Key Supportive Data
D-PanH5N1-00718-64 years
Q-Pan-001Dose
Confirmation18-64 years
Q-Pan-002Safety,
Consistency≥ 18 years
New Brunswick6 mo-9 years
Manitoba≥ 6 months
CanadaMulti-Province
≥ 6 months

A-18
Q-Pan H5N1 Immunogenicity Data
A-19
SC
R (
%)
0
25
50
75
100
Post dose 1 Post dose 2
3.75µg7.5µg 15µg 30µg
3.75µg + AS03A
7.5µg + AS03A
15µg + AS03A
30µg + AS03A
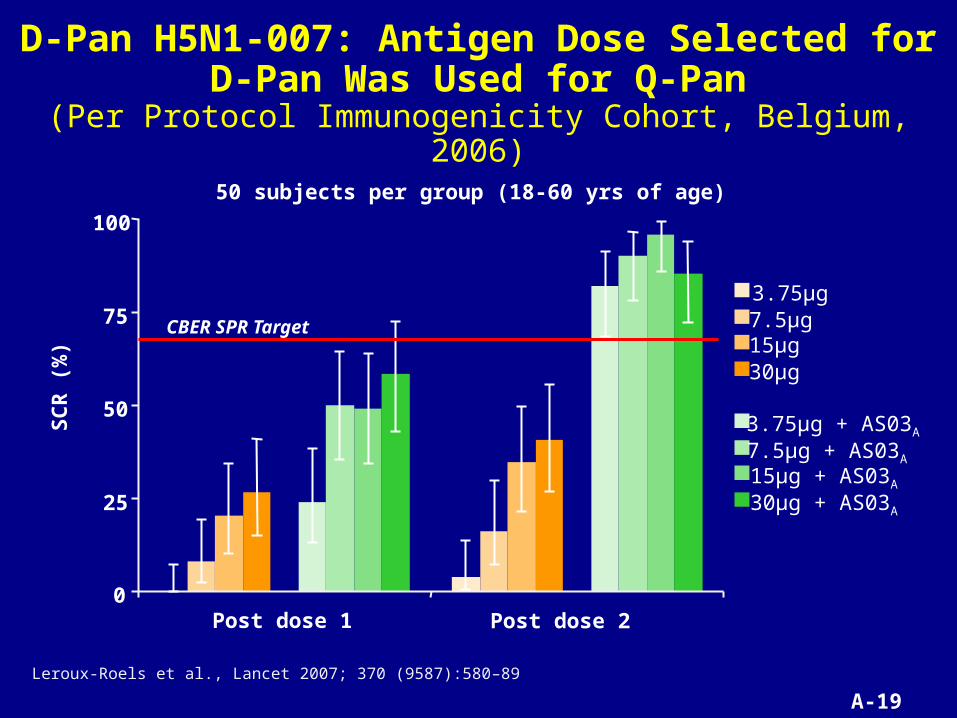
Leroux-Roels et al., Lancet 2007; 370 (9587):580–89
D-Pan H5N1-007: Antigen Dose Selected for D-Pan Was Used for Q-Pan
(Per Protocol Immunogenicity Cohort, Belgium, 2006)
50 subjects per group (18-60 yrs of age)
CBER SPR Target

A-20
Q-Pan H5N1-001: To Confirm AS03 Benefit, Equivalence to D-Pan, and AS03 Dose
(Total Vaccinated Cohort = 780 adults, USA/Canada, 2007-8)
Q-Pan 3.75 µg N=78
Q-Pan 3.75 µg + AS03A N=152
Q-Pan 3.75 µg + AS03B N=150
D-Pan 3.75 µg + AS03A N=151
D-Pan 3.75 µg + AS03B N=149
Q-Pan 1.9 µg + AS03A N=50
Q-Pan 1.9 µg + AS03B N=50
Adjuvant benefit
Immunogenicityequivalence
If Q-Pan/AS03 groups have SPR ≥ 76%, enrollhalf dose groups

A-21
Q-Pan H5N1-001 Confirmed AS03 Benefit (SCR increase > 15%)
(Per Protocol Immunogenicity Cohort)
0
10
20
30
40
50
60
70
80
90
100
SP
R (%
)
A/Indonesia HI ResponsesGroup Size 140-146 in adjuvant groups, 75 controls
CBER SPR Target
ΔSPR/SCR ~ 80%
Langley et al., JID 2010; 201:1644-53.
Day 0 Day 21 Day 42
Q-Pan Only Q-Pan + AS03A D-Pan + AS03A Q-Pan + AS03B D-Pan + AS03B

A-22
1
10
100
1000
GM
T (9
5%
CI)
A/Indonesia HI Responses,Group size 140-146 in adjuvant groups, 75 controls
Q-Pan H5N1-001 Confirmed AS03 Benefit (GMT increase > 2-fold)
(Per Protocol Immunogenicity Cohort)
Langley et al., JID 2010; 201:1644-53.
Day 0 Day 21 Day 42
GMT increase 43-fold
Q-Pan Only Q-Pan + AS03A D-Pan + AS03A Q-Pan + AS03B D-Pan + AS03B

A-23
Q-Pan H5N1-001 Confirms Q-Pan Equivalence to D-Pan (GMT ratio within 0.67 – 1.5)
(Per Protocol Immunogenicity Cohort)
1
10
100
1000
GM
T (9
5%
CI)
A/Indonesia HI Responses,Group size 140-146 in adjuvant groups, 75 controls
GMT ratio 0.94 (95% CI 0.75, 1.17)
Langley et al., JID 2010; 201:1644-53.
Q-Pan Only Q-Pan + AS03A D-Pan + AS03A Q-Pan + AS03B D-Pan + AS03B
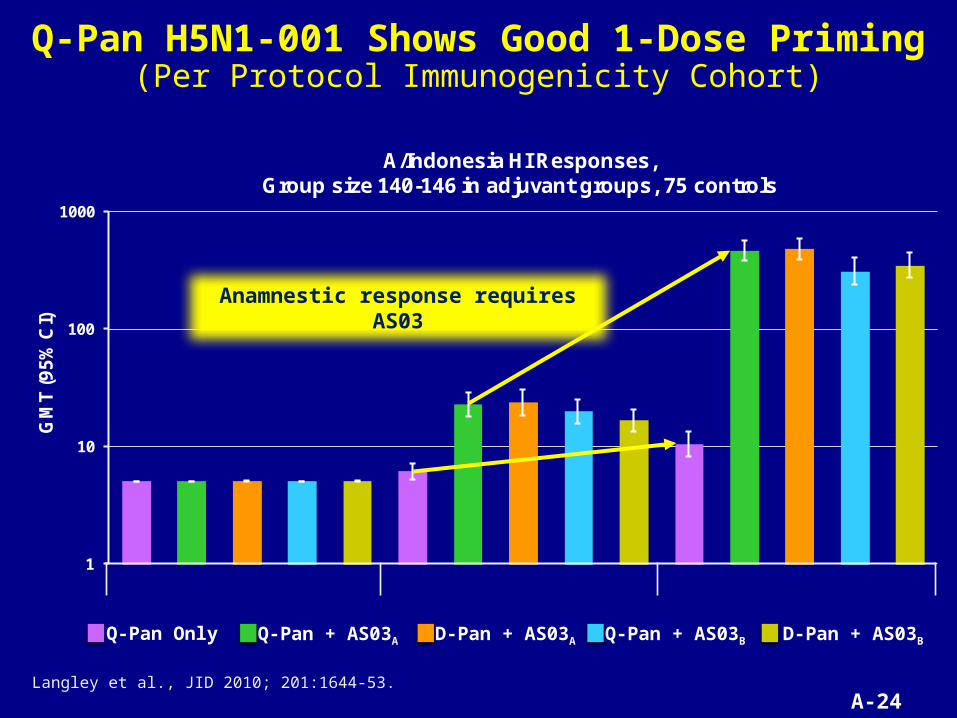
A-24
Q-Pan H5N1-001 Shows Good 1-Dose Priming(Per Protocol Immunogenicity Cohort)
1
10
100
1000
GM
T (9
5%
CI)
A/Indonesia HI Responses,Group size 140-146 in adjuvant groups, 75 controls
Anamnestic response requires AS03
Langley et al., JID 2010; 201:1644-53.
Q-Pan Only Q-Pan + AS03A D-Pan + AS03A Q-Pan + AS03B D-Pan + AS03B
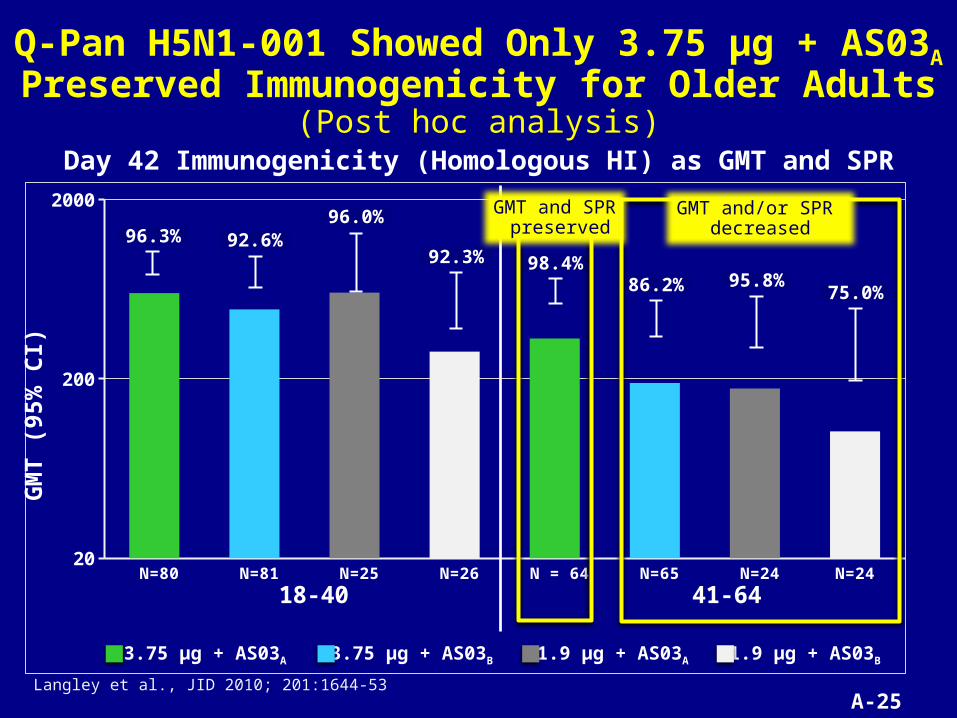
A-25
N=80 N=81 N=25 N=26 N = 64 N=65 N=24 N=2420
200
2000
18-40 41-64
Q-Pan H5N1-001 Showed Only 3.75 µg + AS03A Preserved Immunogenicity for Older Adults
(Post hoc analysis)
Langley et al., JID 2010; 201:1644-53
3.75 μg + AS03A 3.75 μg + AS03B 1.9 μg + AS03A 1.9 μg + AS03B
96.3%
98.4%86.2%
96.0%
95.8%92.3%
75.0%
92.6%
GM
T (
95%
CI)
Day 42 Immunogenicity (Homologous HI) as GMT and SPR
GMT and/or SPR decreased
GMT and SPR preserved

A-26
Q-Pan H5N1-002: To Confirm Lot Consistency and Immunogenicity (Safety) for Adults of All Ages
(Total Vaccinated Cohort = 4561, USA/Canada, 2008)
Ag lot A + AS03 lot 1 N=570, 18-49 yrs
Ag lot B + AS03 lot 2 N=568, 18-49 yrs
Ag lot C + AS03 lot 3 N=569, 18-49 yrs
Placebo (PBS) N=568, 18-49 yrs
Ag lot ABC + AS03 lot 1 N= 597, 50-64 yrs
Placebo (PBS) N=200, 50-64 yrs
Ag lot ABC + AS03 lot 1 N=1118, > 64 yrs
Placebo (PBS) N=371, > 64 yrs
Immunogenicity:SCR & SPRages 18-64
Lot to lot consistency:
GMT ratioages 18-49
Healthy
Stable health
Immunogenicity:SCR & SPRages > 64

A-27
Q-Pan H5N1-002 Demonstrated Good Immunogenicity Regardless of Age
(Per Protocol Immunogenicity Cohort)
Immunogenicity (Homologous HI) as Day 0 and 42 GMTs and SCRs
Day 0 Day 42 Day 0 Day 42
All lots Placebo
≥ 75
N=11972% SCR
N=39674% SCR
Day 0 Day 42 Day 0 Day 42
All lots Placebo
≥ 65
N=157191% SCR
Day 0 Day 42 Day 0 Day 42
All lots Placebo
18-64
1
10
100
1000
Day 42 Day 42 Day 42
Lot A Lot B Lot C
18-49
GM
T (
95%
CI)
Langley et al. JID 2011; 203:1729-38.

A-28
Pivotal Trial Data Fulfill Immunogenicity Requirements for Accelerated Approval
• Q-Pan H5N1 given 21 days apart met CBER criteria in adults 18-64 and ≥ 65 years of age
• Manufacturing consistency demonstrated
• 3.75 µg HA + AS03A formulation had better immunogenicity profile than currently licensed vaccine (not studied concurrently)

A-29
Clinical Endpoint Data from Vaccines Manufactured Using
Quebec Process

A-30
Q-QIV-006: To Confirm the Clinical Benefit of Influenza Vaccine Antigens Manufactured in Quebec
(8 Countries in Caribbean and Asia, 2010-11)
*Only for primed subjects† Only for unprimed
Havrix (N = 2,600)
Blood sample†Vaccination†
Blood sample*Vaccination
Blood sample
Day 0
Q-QIV (N = 2,600) (unadjuvanted)
Age stratified 3–4 and 5–8 years
ILI case count ~OCT
Surveillance during 2010-11 influenza season
Havrix dose 2* or 3† for
control group
N~5,200
Visit Day 180
Blood sample
Day 28 Day 56
Children 3 to 8 years of age
Randomization 1:1

A-31
Q-QIV-006 Evaluated Vaccine Efficacy Against Two Influenza Disease Endpoints
• Any influenza– Temperature ≥ 37.8° C, and– One or more symptoms on the same day (cough, sore
throat, runny nose or nasal congestion)
• Moderate to severe influenza = “any influenza” plus – Fever > 39°C, or – Physician-verified acute otitis media, or– Physician-verified lower respiratory infection, or– Physician-diagnosed serious extra-pulmonary
complication of influenza
Definitions for Influenza Confirmed by RT-PCR Test for Viral RNA

A-32
Q-QIV-006 Confirmed Efficacy of Influenza Vaccine Antigens Manufactured in Quebec
ATP Cohort for Efficacy Q-QIVN=2,379
HavrixN=2,398 Vaccine efficacy (95% CI)
Endpoint n % n % % LL UL
Any influenza A or B 58 2.44 128 5.34 55.4 39.15* 67.29
Moderate to severe influenza A or B 14 0.59 52 2.17 73.1 47.11** 86.30
* Success criterion, LL >30%** 97.5% CI, success criterion, LL >0%
Post-hoc analysis, TVCQ-QIV
N=2,379Havrix
N=2,398 Vaccine efficacy (95% CI)
Endpoint n % n % % LL UL
Any influenza H1N1 17 0.66 41 1.59 59.0 27.80 76.69
Any influenza H3N2 20 0.77 50 1.93 60.7 34.00 76.61

A-33
Q-Pan H1N1-035 Confirmed the Value of Adding AS03 to Influenza Vaccine Antigens Manufactured in Quebec
(8 Countries in Latin America & Asia, TVC=6,145)
Q-Pan H1N1 =1.9 µg HA /AS03B x2
Q-Pan H1N1 = 1.9 µg HA/AS03B x1
H1N1 control = 7.5 or 15 µg HA x2
100 200 300 400 500 600
Time (Days)
00.985
0.990
0.995
1.000
Dis
ease
Fre
e P
rop
ort
ion
Group Relative VE (95% CI) Comment
Q-Pan H1N1 x2 vs control 76.8 (18.5, 93.4) Primary objective
Q-Pan H1N1 x1 vs control 46.4 (-34.4, 78.6) Secondary objective
Children 6 months to 9 years of age followed for 385 days
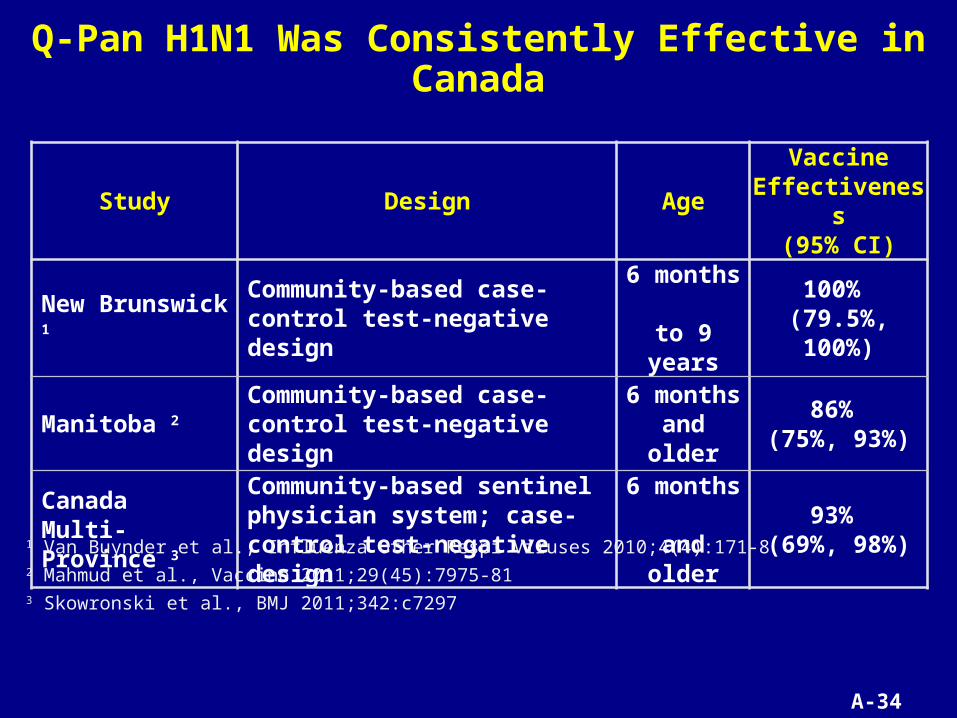
A-34
Q-Pan H1N1 Was Consistently Effective in Canada
Study Design AgeVaccine
Effectiveness(95% CI)
New Brunswick 1 Community-based case-control test-negative design
6 months to 9 years
100% (79.5%, 100%)
Manitoba 2 Community-based case-control test-negative design
6 months and older
86% (75%, 93%)
Canada Multi-Province 3
Community-based sentinel physician system; case-control test-negative design
6 months and older
93% (69%, 98%)
1 Van Buynder et al., Influenza Other Respi Viruses 2010;4(4):171-82 Mahmud et al., Vaccine 2011;29(45):7975-813 Skowronski et al., BMJ 2011;342:c7297

A-35
Clinical Trial Data with Influenza Vaccines Manufactured in Quebec Support that Q-Pan H5N1
Will Reduce Risk of Disease
Unadjuvanted Q-QIV
Adjuvanted Q-Pan H1N1
55% efficacy - “any” influenza59% efficacy - “any” H1N1 influenza73% efficacy - “moderate-severe influenza”
77% relative efficacy - “any” H1N1 influenza
86-100% effectiveness - “any” H1N1 influenza
VEQ-Pan = VEcontrol + (rel eff x [100% - VEcontrol]) 90% = 59% + (77% x [100% - 59%])
90% absolute efficacy – “any” H1N1 influenza
GSK proposes Q-QIV-006 as the required study to confirm clinical benefit of Q-Pan H5N1
(it provides a minimum estimate)

A-36
GSK Will Collaborate in Government-Sponsored Studies of Q-Pan H5N1 Effectiveness in a Pandemic
• Observational study feasible and reliable if– Population-based, test-negative controls – Cases systematically evaluated– Vaccination status captured by product
• In the US and Canada (where Q-Pan H5N1 might be deployed), governments are best able to conduct observational studies– Control vaccine distribution– Guide case assessments (testing for H5N1 disease)– Capture vaccination status

A-37
Introduction Donna BoyceHead, North AmericaGlobal Regulatory Affairs
Immunogenicity & Effectiveness
Bruce Innis, MDVice PresidentVaccine Discovery and Development
Safety Felix Arellano, MDVice PresidentVaccines Clinical Safety and Pharmacovigilance
Conclusion Donna Boyce
GSK Presentation

A-38
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1 (Integrated Summary Safety [ISS]-1, ISS-2 and postmarketing)
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-39
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-40
Non-clinical Safety Data Supported Testing in Humans
• Standard non-clinical toxicology studies (n=12)– Local tolerance, single-dose toxicity, repeat-dose
toxicity, genotoxicity, and reproductive and developmental toxicity studies
• Standard safety pharmacology studies (n=2)– Cardio-respiratory function in rats and dogs
• Findings– Injection site inflammation as expected with adjuvanted
vaccine

A-41
• Non-clinical safety data
• Clinical trial safety data: Pivotal trial Q-Pan H5N1-002
• Analysis of signals from H5N1 and H1N1
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-42
Clinical Trial Data: Pivotal Study Q-Pan H5N1-002
• N = 4,561 subjects– 3,422 Q-Pan H5N1 recipients– 1,139 placebo recipients
• Follow-up to 12 months– 2,606 Q-Pan H5N1 recipients– 870 placebo recipients
• Solicited local and general symptoms for 7 days after each dose
• Unsolicited AEs through day 84
• Medically-attended AEs and SAEs through day 364

A-43
Q-Pan H5N1-002: Increased Incidence of Local Reactogenicity Compared to Placebo
0
10
20
30
40
50
60
70
80
90
100
All Grade 3 All > 100 All > 100
Pain Redness (mm) Swelling (mm)
Incidence of solicited local adverse events
Q-Pan H5N1Placebo

A-44
Q-Pan H5N1-002: Increased Incidence of General Reactogenicity, But Not Grade 3 Events,
Compared to Placebo
0
10
20
30
40
50
60
70
80
90
100
All
Gra
de
3 All
Gra
de
3 All
≥39
.0 All
Gra
de
3 All
Gra
de
3 All
Gra
de
3 All
Gra
de
3
Arthralgia Fatigue Fever (°C) Headache Myalgia Shivering Sweating
Incidence of solicited general adverse events
Q-Pan H5N1Placebo

A-45
Q-Pan H5N1-002: Conclusions
• Greater frequency and intensity of reactogenicity for Q-Pan H5N1 compared to saline placebo
• Similar frequencies between Q-Pan H5N1 and placebo for– Lymphadenopathy– Unsolicited adverse events– MAEs– SAEs, including fatal AEs– AEs leading to withdrawal

A-46
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1 (ISS-1, ISS-2 and postmarketing)
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-47
Main Safety Signals1 Related to the GSK Adjuvanted Pandemic Influenza Program
Signal Source Assessment
Potential Immune-Mediated Diseases
Numerical imbalance in ISS-1
Current data do not support causal association
Narcolepsy D-Pan H1N1 postmarketing
Inconclusive; additional studies ongoing
Autoimmune Hepatitis Q-Pan and D-Pan H5N1 clinical development
Current data do not support causal association
Anaphylaxis Q-Pan H1N1 postmarketing
Similar to other flu vaccines
Guillain-BarréSyndrome Pre-specified Excess risk 0-2 / million
persons vaccinated
Solid Organ Transplant Rejection
Q-Pan H1N1 postmarketing
Current data do not support causal association; additional studies ongoing
1 CIOMS IV/VI definition: report(s) of an event with an unknown causal relationship to treatment that is recognized as worthy of further exploration and continuous surveillance

A-48
pIMDs: H5N1 Signal Evaluation Included Data from H1N1 Pandemic Response
• Source of signal: group of AEs that, together, occurred more frequently among H5N1 recipients than control recipients
• Evaluation of signal– Creation of case series (qualitative analysis; medical review)– Examination of H1N1 clinical trial data– External analysis of H1N1 vaccines’ spontaneous reports
(EudraVigilance)– External analysis of H1N1 vaccines (Swedish study)

A-49
Aggregate Data from H5N1 and H1N1 Adjuvanted Pandemic Clinical Development Programs
Aggregate data analyses = Integrated Summaries of Safety (ISSs)
• ISS-1– 9,873 D-Pan and Q-Pan H5N1 recipients (8 trials)– Numerical imbalance for pIMDs in aggregate
• pIMDs identified by 120 MedDRA Preferred Terms• List of terms developed with input from external experts and CBER
• ISS-2– 11,376 D-Pan and Q-Pan H5N1 recipients– 28 adult clinical trials of Q-Pan and D-Pan H5N1 and H1N1
vaccines• Included all trials in ISS-1
– Numerical imbalance for pIMDs persisted

A-50
pIMDs Reported by H5N1 Recipients in Controlled, Uncontrolled and Booster Studies
• Autoimmune hepatitis (n = 1)
• Autoimmune thyroiditis or Basedow’s disease (n = 2)
• Celiac disease (n = 1)
• Crohn’s disease (n = 1)
• Erythema nodosum (n = 1)
• IIIrd nerve paralysis (n = 1)
• IVth nerve paresis (n = 1)
• Multiple sclerosis (n = 1)
• Neuritis (n = 1)
• Optic neuritis (n = 1)
• Polymyalgia rheumatica (PMR) or temporal arteritis (n = 4)
• Psoriasis (n = 3)
• Radiculitis or radiculopathy (n = 1)
• Rheumatoid arthritis (n = 1)
• Scleroderma (n = 1)
• Systemic lupus erythematosus (n = 1)
• Uveitis (n = 1)
• Ulcerative colitis (n = 1)
• VIIth nerve paralysis, facial paresis, or facial palsy (n = 5)
A-51
pIMDs: H5N1 Case Review Suggested Pre-existing or Alternative Plausible Causes
3 events accounted for much of the imbalance:
• Bell’s palsy/facial palsy / facial paresis / VII nerve paralysis (n=5)– One diagnosis subsequently changed to stroke– One event began 8 hours after vaccination and had negative
rechallenge (recovered after receiving second dose)
• Psoriasis (n=3)– One subject had psoriasis at study enrollment and the investigator
did not think it had worsened after receiving vaccination– One subject developed guttate psoriasis attributed to a
streptococcal infection by the investigator
• Polymyalgia rheumatica / temporal arteritis (n=4)– One subject had symptoms prior to vaccination; PMR
symptomatology did not change; temporal arteritis diagnosed after vaccination
– Another diagnosis was changed to fibromyalgia

A-52
No Difference in the Reporting of Autoimmune Diseases Between Adjuvanted and
Non-adjuvanted H1N1 Vaccines
• EudraVigilance data and literature review
• All spontaneous cases reported to EU during 2009-2010 pandemic for all H1N1 vaccines (adjuvanted and non-adjuvanted)
• Reporting rates of autoimmune diseases, per million
– Adjuvanted 6.87 (95% CI: 6.06–7.68)– Non-adjuvanted 9.98 (95% CI: 6.81–13.16)
Isai et al., Vaccine 2012; 30: 7123-7129

A-53
No Increased Risk of Selected Autoimmune Diseases Among Persons Vaccinated
with D-Pan H1N1 Retrospective cohort study in Stockholm county, Sweden; 1.02 million vaccinated; 921 K unvaccinated followed over 8-10 months
Bardage et al., BMJ 2011; 343:d5956
Event Adjusted Hazard Ratio 95% CI
Rheumatoid Arthritis 0.94 (0.81, 1.09)
Insulin-dependent Diabetes 0.99 (0.67, 1.47)
Inflammatory Bowel Disease 1.13 (0.97, 1.32)
Multiple Sclerosis 0.93 (0.68, 1.26)
Guillain-Barré Syndrome 1.07 (0.66, 1.74)
Bell’s Palsy 1.25 (1.06, 1.48)

A-54
pIMDs – Conclusion
• Currently available data from clinical trials, spontaneous reports and an epidemiological study do not support a relationship between Q-Pan H5N1 and the induction of pIMDs
• GSK will continue to monitor reports of pIMDs when vaccine is used

A-55
Narcolepsy: Context of Signal Evaluation
• During pandemic– Mass vaccination with GSK H1N1 vaccines in 47
countries – High coverage and/or exclusive use in several countries
(Finland, Sweden, Canada)
• Feb 2010– First case report received by GSK; reported in sPSUR;
monitoring initiated
• Apr 2010 - end May 2010– Second case (April), additional 2 cases
• Jul-Aug 2010– Sweden reports cluster of cases– GSK first analysis and EMA mandates investigation– Widespread media attention begins in EU

A-56
Narcolepsy: Background
• Very rare disease– Background incidence around 10 per million person-years– Incidence lower in children 1-5 per million person-years1
• Difficult to diagnose / validate – Characterized by excessive daytime sleepiness and sleep
paralysis2, frequently associated with cataplexy3
– Diagnosis requires access to sleep clinic– Decreased hypocretin-1 in CSF4
• HLA DQB1*0602 allele – necessary – Present in 15-25% of population, more prevalent in N. Europe– Possible autoimmune mechanism
1 VAESCO report 20122 Han et al. Respirology 2012; doi:10.1111/j.1440-1843.2012.02178.x 3 Dauvilliers et al : Lancet 2007; 369: 499–5114 Mignot, et al.. Arch Neurol 2002; 59: 1553–1562
A-57
Narcolepsy: Summary of Exposure
• Clinical trials– almost 23,000 subjects in H5N1 and H1N1, no reports
• Q-Pan H1N1: 58.5 million vaccinated– 111,836 pregnant women; 2.8 million children
• D-Pan H1N1: 31 million vaccinated– 194,780 pregnant women; 6.7 million children

A-58
Narcolepsy: Q-Pan H1N1 - No Evidence of a Signal from Epidemiological Study
Quebec study (preliminary results)
• Total 20 cases (6 exposed cases and 14 non-exposed cases)
• Incidence rate 0.13 per 100,000 person-years (vaccinated and unvaccinated)
• Age- and gender-adjusted risk ratio 1.06 (95% CI: 0.33, 2.97)
J. Montplaisir, Université de Montréal, personal communication

A-59
Summary of Results from European Epidemiological Studies
Study Country RR (95%CI) Attributable Risk (per 100,000)
VAESCO (EU)
Finland 10.2 (1.8-Inf)
Not calculated
Sweden 3.5 (0.4-Inf)
Signalling countries pooled (SWE, FIN) 14.2 (2.5-Inf)
Non-signalling countries 1.6 (0.5-6.1)
THL (Finland) Finland 12.7 (6.1-30.8) 6.25
MPA (Sweden) Sweden 6.6 (3.1-14.5) 3.6
Irish Dept. of Health Ireland 13.0 (4.8–34.7) 5.3
ANSM/AFFSAPS (France) France
< 19 years5.1 (2.1 – 12.3)
≥ 19 years3.9 (1.4 – 11)
Not calculated

A-60
D-Pan H1N1: VAESCO Study - Primary Analysis Yields Inconclusive Results
• Commissioned by European CDC, robust, large-scale, standardised case-control study, attempting to consider biases
• Signaling countries (where signal arose; predefined): association in children
• Non-signaling countries: no association in children
*95% CI: 1.8-
Non-signaling countries Signaling countries
Rel
ati
ve
Ris
k
Pooled PooledNorway France Denmark NL UK Sweden Finland
100
10
1
0.1
2.9
1.3
4.1
1.6
3.5
10.2*14.2*

A-61
D-Pan H1N1: Main Limitations of Studies
• Close temporal proximity between H1N1 peak and vaccination – potentially confounds results
• Important potential referral and ascertainment / recall biases not fully accounted for in most studies to date
– Biases better accounted for by VAESCO study
• Lack of adjustment for potential confounders, such as co-morbidities
• Swedish study included spontaneous reports as cases, biasing results towards association with vaccine
A-62
GSK’s Ongoing Narcolepsy Research Activities
• Non-clinical and epidemiological investigations ongoing– Epidemiologic study (Quebec)– Non-clinical experiments– Animal studies
• Research plan developed after experts consultation
• Agreed by Regulatory Authority (EMA Scientific Advice)
• Conducted in collaboration with recognized experts
A-63
Narcolepsy: Summary
• No signal to date with Q-Pan H5N1
• No signal to date with Q-Pan H1N1
• Signal with D-Pan H1N1
• D-Pan H1N1 in EU: observational data – inconclusive– Currently available data insufficient to determine whether
there is a causal relationship between D-Pan H1N1 and narcolepsy and further research is necessary
• Extensive research program under way

A-64
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-65
Q-Pan H5N1: Pharmacovigilance Plan (PVP)
• Includes general (e.g., all pandemic flu vaccines) and specific (e.g., Q-Pan H5N1) activities
• Specific activities depend upon circumstances of use for vaccine (e.g., civilian or military population)

A-66
Q-Pan H5N1: Pharmacovigilance Plan for US
Activities to be agreed-upon with CBER:
• Close monitoring of “adverse events of special interest” (AESIs) for all pandemic vaccines1, plus autoimmune hepatitis, increased concentrations of hepatic enzymes, narcolepsy
• Weekly, computerized signal detection2
• Monthly simplified Periodic Safety Update Reports to regulators2
• Will rely on US agencies for near real-time analysis of AEs in data systems not available to sponsors
– Rapid-cycle analysis of VSD– Mini-sentinel or Sentinel
1 Anaphylaxis, Bell’s palsy, convulsions, demyelinating disorders, encephalitis, Guillain-Barré syndrome neuritis, vasculitis, vaccination failure
2 During H5N1 pandemic

A-67
Q-Pan H5N1: Pharmacovigilance Plan for US
The following activities will be contingent on their feasibility at the time of vaccine use:
• Establish US Pregnancy Registry, as is done for seasonal flu vaccines
• Determine background incidence rates in US for AESIs and other AEFIs, as necessary, for observed:expected analyses
• Conduct prospective cohort study
• Continue to work with sleep experts and professional societies to establish sentinel network for early detection and validation of narcolepsy cases

A-68
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-69
Potential Impact of an H5N1 Pandemic
• Current status of H5N1 human disease (2003 – 2012)– 608 cases with 359 deaths reported to WHO– Overall case fatality ratio 59%*
• Projected social consequences of H5N1 pandemic– US: 25-50% of population infected; 1-5% mortality,
2 million excess deaths – Worldwide: 25-50% morbidity; 16 million – 160 million
excess deaths
*http://www.who.int/influenza/human_animal_interface/H5N1_cumulative_table_archives/en/index.html
A-70
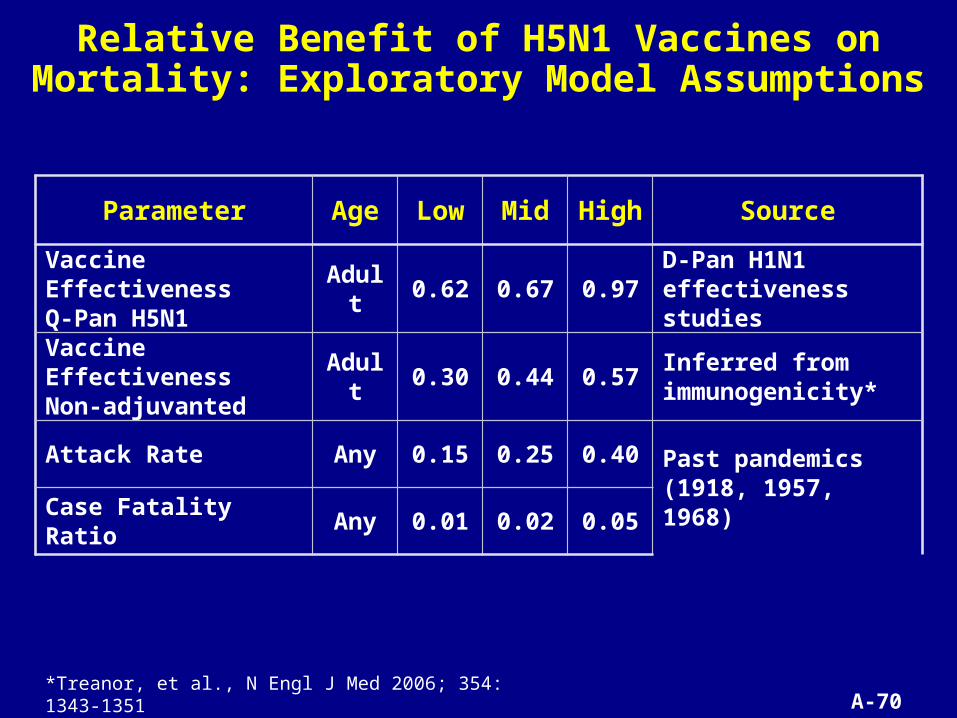
Relative Benefit of H5N1 Vaccines on Mortality: Exploratory Model Assumptions
Parameter Age Low Mid High Source
Vaccine Effectiveness Q-Pan H5N1 Adult 0.62 0.67 0.97 D-Pan H1N1
effectiveness studies
Vaccine Effectiveness Non-adjuvanted Adult 0.30 0.44 0.57 Inferred from
immunogenicity*
Attack Rate Any 0.15 0.25 0.40Past pandemics(1918, 1957, 1968)
Case Fatality Ratio Any 0.01 0.02 0.05
*Treanor, et al., N Engl J Med 2006; 354: 1343-1351

A-71
Relative Benefit Scenarios in a Pandemic Setting (Conservative Analysis)
ScenariosVE
Q-Pan H5N1
VE Non- Adjuvanted AR
Case Fatality Ratio
Prevented Deaths
Adjuvanted *
Prevented Deaths Non- Adjuvanted*
Best 0.97 0.57 0.15 0.01 146 86
Most Realistic 0.67 0.3 0.25 0.05 838 375
Worst 0.62 0.3 0.40 0.05 1240 600
*per 100,000 persons vaccinated. VE = vaccine effectiveness, AR = attack rate,

A-72
Relative Benefit: Adjuvanted Vaccine Prevents Approximately Twice as Many Deaths as Non-Adjuvanted Vaccine in All Scenarios
0 200 400 600 800 1000 1200 1400
Prevented Deaths Non Adjuvanted
Prevented Deaths Adjuvanted
Worst case
Most likelycase
Prevented deaths per 100,000 persons vaccinated
Best case

A-73
• Non-clinical safety data
• Clinical trial safety data
• Analysis of signals from H5N1 and H1N1
• Pharmacovigilance Plan
• Relative benefit scenarios in a pandemic setting
• Assessment of safety and benefit-risk
Safety Presentation Outline

A-74
Overall Safety and Benefit-Risk Conclusions
• Q-Pan H5N1 safety profile supports licensure for the proposed indication
• Reactogenicity (general and local) is greater than for placebo
• Benefit-risk balance of Q-Pan H5N1 is positive
• Pharmacovigilance Plan is built upon experience with H1N1 pandemic and will allow GSK to monitor the safety of Q-Pan H5N1
A-75
Introduction Donna BoyceHead, North AmericaGlobal Regulatory Affairs
Immunogenicity & Effectiveness
Bruce Innis, MDVice PresidentVaccine Discovery and Development
Safety Felix Arellano, MDVice PresidentVaccines Clinical Safety and Pharmacovigilance
Conclusion Donna Boyce
GSK Presentation

A-76
Pathway for Accelerated Approval of Q-Pan H5N1
US Licensed Seasonal Influenza Vaccine
Accelerated Approval
Efficacy not yet confirmed
Source
FluLaval
Pre-approval
2006
2012 BLA
2013
During a Pandemic
Timing
Q-Pan H5N1 licensure approach: Accelerated Approval
• Safety• Immunogenicity
Q-Pan H5N1-001Q-Pan H5N1-002
Effectiveness of Q-Pan H5N1 inferred when the efficacy of the seasonal confirmed
FluLavalQ-QIV-006
Post-approval
Work with US Gov’t to collect safety/effectiveness data
with Q-Pan H5N1CBER Guidance
A-77
Benefit-Risk is Positive
• Q-Pan H5N1 immunogenicity and safety profile support licensure for the proposed indication
• AS03 – High immunogenicity – Antigen-sparing
• Global H1N1 pandemic experience will enable effective safety monitoring of Q-Pan H5N1 through planned pharmacovigilance

A-78
Licensure Improves Pandemic Preparedness
• Offers US Government more immunogenic alternative to currently licensed H5N1 vaccine
• Establishes regulatory platform to enable rapid licensure of pandemic strain specific vaccine
• Antigen-sparing property will increase number of doses available for distribution
Significant public health benefit in event of H5N1 pandemic

A-79
Additional as Slides Shown
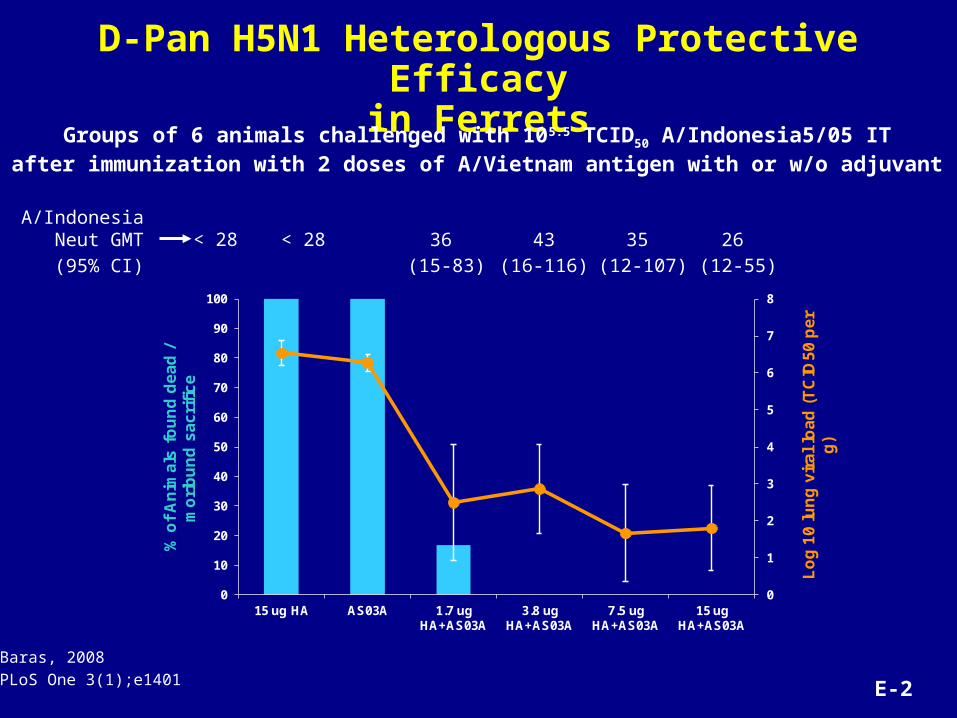
D-Pan H5N1 Heterologous Protective Efficacyin Ferrets
0
1
2
3
4
5
6
7
8
0
10
20
30
40
50
60
70
80
90
100
15 ug HA AS03A 1.7 ug HA+AS03A
3.8 ug HA+AS03A
7.5 ug HA+AS03A
15 ug HA+AS03A
Lo
g 1
0 l
un
g v
ira
l lo
ad
(T
CID
50
pe
r g
)
% o
f A
nim
als
fo
un
d d
ea
d /
m
ori
bu
nd
sa
cri
fic
e
< 28 < 28 36
(15-83)
43
(16-116)
35
(12-107)
26
(12-55)
A/Indonesia Neut GMT
(95% CI)
Groups of 6 animals challenged with 105.5 TCID50 A/Indonesia5/05 ITafter immunization with 2 doses of A/Vietnam antigen with or w/o adjuvant
Baras, 2008
PLoS One 3(1);e1401 E-2
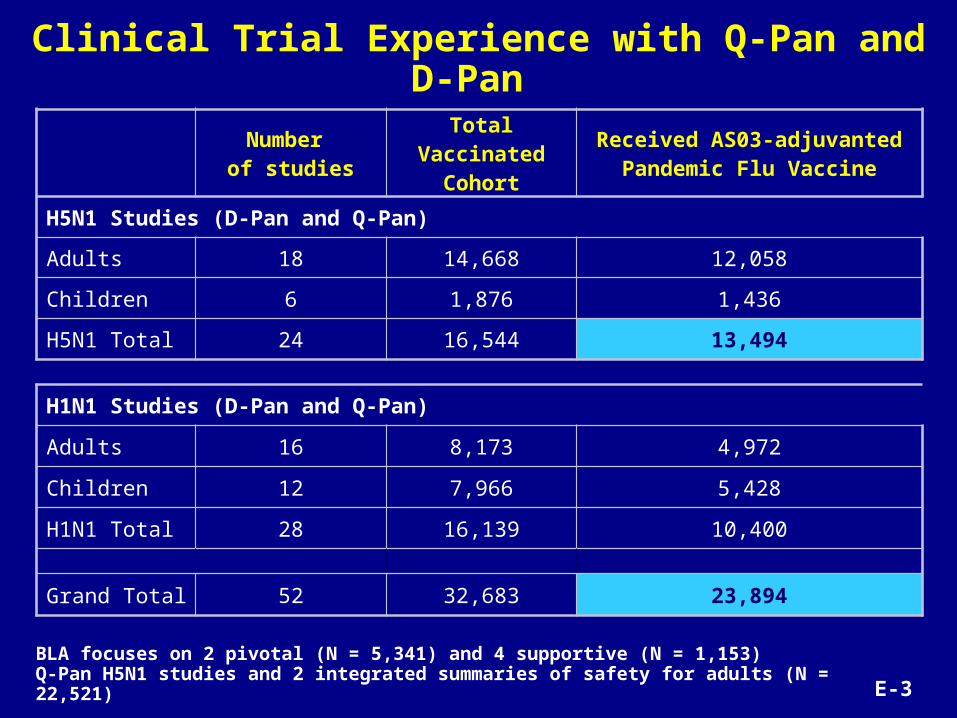
Clinical Trial Experience with Q-Pan and D-Pan
BLA focuses on 2 pivotal (N = 5,341) and 4 supportive (N = 1,153) Q-Pan H5N1 studies and 2 integrated summaries of safety for adults (N = 22,521)
Number of studies
Total Vaccinated Cohort
Received AS03-adjuvanted Pandemic Flu Vaccine
H5N1 Studies (D-Pan and Q-Pan)
Adults 18 14,668 12,058
Children 6 1,876 1,436
H5N1 Total 24 16,544 13,494
H1N1 Studies (D-Pan and Q-Pan)
Adults 16 8,173 4,972
Children 12 7,966 5,428
H1N1 Total 28 16,139 10,400
Grand Total 52 32,683 23,894
E-3

Q-Pan H5N1-001 Heterologous H5N1 MN Data (A/Indonesia/05/2005 vaccine at Day 0 and Day 42)
A/Indonesia (clade 2.1) GMT >1:28 VRR
GroupTime point
N VALUE95% CI
%95% CI
%95% CI
LL UL LL UL LL UL
Q 3.8 µg + AS03A
PRE 47 22.3 17.4 266.1 27.7 15.6 42.6 - - -
D42 47 1566.8 1227.3 2000.2 100 92.5 100 97.9 88.7 99.9
A/Vietnam (clade 1)
Q 3.8 µg + AS03A
PRE 47 57 41.3 78.6 70.2 55.1 82.7 - - -
D42 47 264.8 216.7 323.6 100 92.5 100 53.2 38.1 67.9
A/Anhui/1/05 (clade 2.3)
Q 3.8 µg + AS03A
PRE 143 14 14 14 0 0 2.5 - - -
D42 142 91.3 78.4 106.4 95.1 90.1 98 78.9 71.2 85.3
A/Turkey/1/05 (clade 2.2)
Q 3.8 µg + AS03A
PRE 143 25.6 21.9 29.9 35.7 27.8 44.1 - - -
D42 143 594.4 523.6 674.7 100 97.5 100 88.8 82.5 93.5
VRR = vaccine response rate = 4-fold or great increase in MN titerPlain antigen A/Indo 3.75µg HA A/Indo GMT: PRE: 25.7; Day 42: 183.8; VRR: 73.5%A/Vietnam GMT: PRE: 55.7; Day 42: 143.9; VRR: 30.6 (no data A/Anui or A/turkey) E-7
1
10
100
1000
GM
T
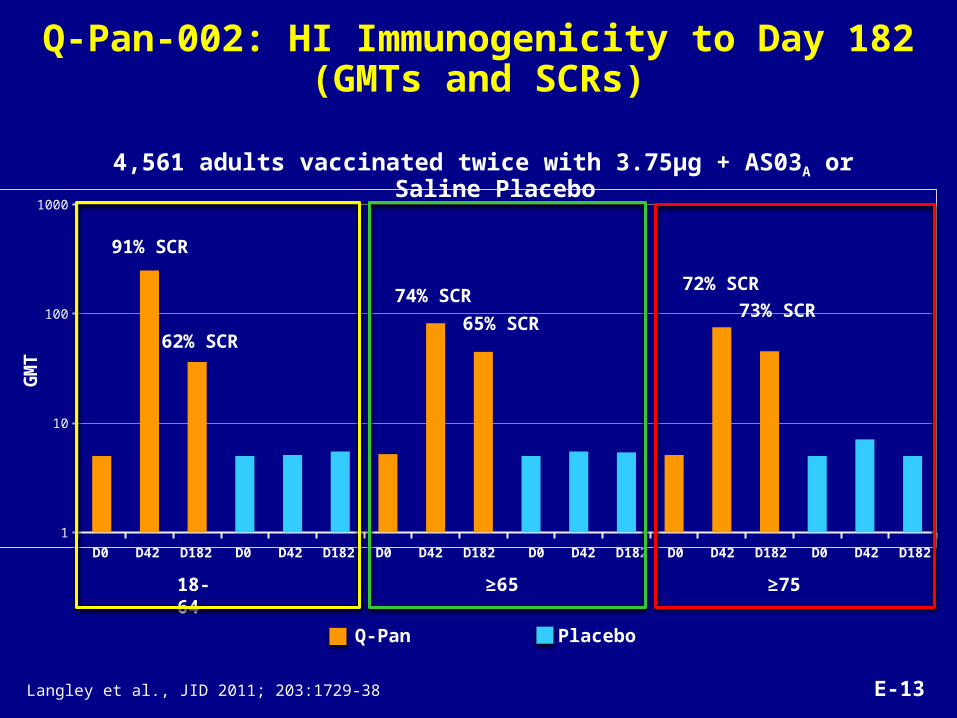
91% SCR
62% SCR
74% SCR
65% SCR73% SCR
72% SCR
PlaceboQ-Pan
18-64 ≥65 ≥75
D0 D42 D182 D0 D42 D182 D0 D42 D182 D0 D42 D182 D0 D42 D182 D0 D42 D182
Q-Pan-002: HI Immunogenicity to Day 182(GMTs and SCRs)
4,561 adults vaccinated twice with 3.75µg + AS03A or Saline Placebo
Langley et al., JID 2011; 203:1729-38 E-13
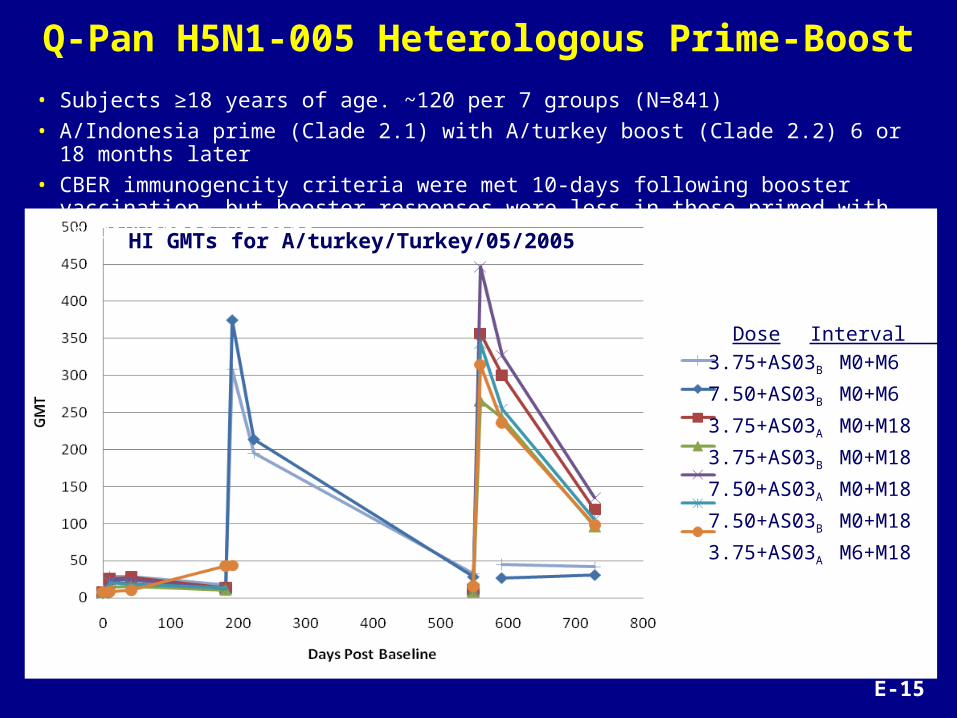
Q-Pan H5N1-005 Heterologous Prime-Boost
• Subjects ≥18 years of age. ~120 per 7 groups (N=841)
• A/Indonesia prime (Clade 2.1) with A/turkey boost (Clade 2.2) 6 or 18 months later
• CBER immunogencity criteria were met 10-days following booster vaccination, but booster responses were less in those primed with unadjuvanted vaccine
HI GMTs for A/turkey/Turkey/05/2005
Dose Interval
3.75+AS03B M0+M6
7.50+AS03B M0+M6
3.75+AS03A M0+M18
3.75+AS03B M0+M18
7.50+AS03A M0+M18
7.50+AS03B M0+M18
3.75+AS03A M6+M18
E-15

D-Pan H5N1-007 Frequency of CD4 T-Cells Specific for H5N1 A/Vietnam Split Antigen
0
500
1000
1500
2000
2500
3000
3500
40003.
8 µg
7.5
µg
3.8
µg +
Ad
j
7.5
µg +
Ad
j
3.8
µg
7.5
µg
3.8
µg +
Ad
j
7.5
µg +
Ad
j
3.8
µg
7.5
µg
3.8
µg +
Ad
j
7.5
µg +
Ad
j
3.8
µg
7.5
µg
3.8
µg +
Ad
j
7.5
µg +
Ad
j
3.8
µg
7.5
µg
3.8
µg +
Ad
j
7.5
µg +
Ad
j
ALL DOUBLES CD4OL IFNg IL2 TNFa
Med
ian
at D
ay42
-Day
0 (Q
1 an
d Q
3)
***
***
***
*** ******
***
***
***: p<0.001: significancy for adjuvant effect
Moris P, et al., J. Clin. Immunol. 2011;31(3):443-54 E-18
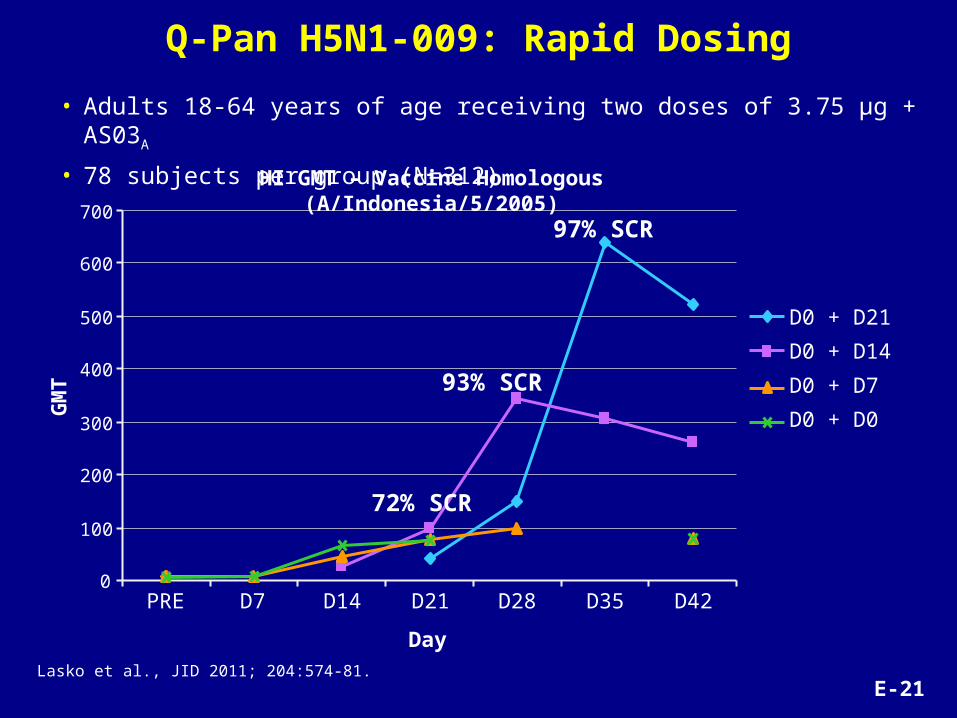
Q-Pan H5N1-009: Rapid Dosing
• Adults 18-64 years of age receiving two doses of 3.75 µg + AS03A
• 78 subjects per group (N=312)
D0 + D21
D0 + D14
D0 + D7
D0 + D0
0
100
200
300
400
500
600
700
PRE D7 D14 D21 D28 D35 D42
Day
GM
T
97% SCR
93% SCR
72% SCR
Lasko et al., JID 2011; 204:574-81.
HI GMT – Vaccine Homologous (A/Indonesia/5/2005)
E-21

Q-Pan H5N1-010 Boost of Q-Pan-001 Subjects(value of adjuvanted vaccine priming and boosting)
• Q-Pan H5N1-001 Veterans received heterologous (A/turkey) boost 15 months later• Q-Pan and D-Pan A/turkey HI responses equivalent (pooled in figure below)• GMT and SCR 10-days following booster vaccination shown below
10
100
1000
Q-Pan H5N1-001 dosing
Boost with A/turkey 3.75µg HA + AS03A Boost with A/turkey 3.75µg HA
92% SCR
96% SCR97% SCR
68% SCR70% SCR
Q Indo 3.75 x2 Q&D Indo 3.75+ AS03A x2
Q&D Indo 3.75+ AS03B x2
Q&D Indo 3.75+ AS03A x2
Q&D Indo 3.75+ AS03B x2
HI
GM
T
Risi et al., Vaccine 2011; 29:6408-18. E-23

Q-QIV-006 Vaccine Efficacy by Sub-Type/Lineage
(Total vaccinated cohort – post hoc exploratory analysis)
Event Group
AR VE
95% CI 95% CI
N n % LL UL T/N % LL UL
Moderate to severe - Type A
Q-QIV 2584 8 0.31 0.13 0.61 5.1 82.04 61.87 91.55
HAVRIX 2584 44 1.70 1.24 2.28 5.0
Moderate to severe - H1N1
Q-QIV 2584 4 0.15 0.04 0.40 5.1 79.10 38.58 92.89
HAVRIX 2584 19 0.74 0.44 1.15 5.0
Moderate to severe - H3N2
Q-QIV 2584 4 0.15 0.04 0.40 5.1 84.27 54.81 94.53
HAVRIX 2584 25 0.97 0.63 1.42 5.1
T/N = mean follow-up period in each group (person-months)
Vaccine efficacy assessed using Cox Regression model adjusted for covariates (age category, region, priming status)
E-29

Q-QIV-006 Immunogenicity Geometric Mean Titer 28 Days After Vaccination
(ATP immunogenicity subset)
PR
E
PO
ST
PR
E
PO
ST
PR
E
PO
ST
PR
E
PO
ST
Flu A/CAL/7/09 (H1N1) Flu A/Victoria/210/09 (H3N2)
FluB/Bri/60/08 (Victoria) Flu B/Florida/4/06 (Ya-magata)
10
100
1000
15.3
318.8
24.3
264.7
13.7
239.9
16.2
361.5
16.1 16.1
28.6 30.3
15.617.8 18.8 19.2
Ge
om
etr
ic m
ea
n t
itre
s
Q-QIV Havrix™ ControlE-30

Immunogenicity Comparisons Q-Pan H1N1 to H5N1
• Different dosing regimens – Q-Pan H1N1: single dose– Q-Pan H5N1: 2 doses, given 21 days apart
• Similar HI antibody responses are observed in adults
18-64 64+ 18-64 64+H1N1 H1N1 H5N1 H5N1
0.0
0.5
1.0
1.5
2.0
2.5
3.0
2.57
2.12
2.40
1.91
Post-Vaccination Log10 GMT w/ 95% CI
18-64 64+ 18-64 64+H1N1 H1N1 H5N1 H5N1
0%
20%
40%
60%
80%
100%90.1%
78.2%
90.8%
74.0%
Seroconversion Rate w/ 95% CI
65+ 65+ 65+ 65+
E-35

Q-Pan H5N1-021: HI Responses
PRE (n=182)
PI(D21) (n=179)
PII(D42) (n=175)
PRE (n=184)
PI(D21) (n=184)
PII(D42) (n=185)
PRE (n=204)
PI(D21) (n=204)
PII(D42) (n=203)
6M-<36M 3Y-<9Y 9Y-<18Y
1
10
100
1000
5.3
38.7
777.1
5.6
44.6
543.8
5.7
35.3
416.2
GM
Ts
wit
h 9
5%
CI
SCR: 57.5% 100% 58.5% 99.5% 51.5%99.0%
E-43

Q-Pan H5N1-021: Incidence of Injection Site Pain by Dose Number and Age
All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3 All
Gra
de 3
6M-<36M 3Y-<9Y 9Y-<18Y 6M-<36M 3Y-<9Y 9Y-<18Y 6M-<36M 3Y-<9Y 9Y-<18Y 6M-<36M 3Y-<9Y 9Y-<18YQ Pan Saline Q Pan Saline
Dose 1 Dose 2
0
10
20
30
40
50
60
70
80
90
100Incidence of pain per dose/per age stratum
E-44
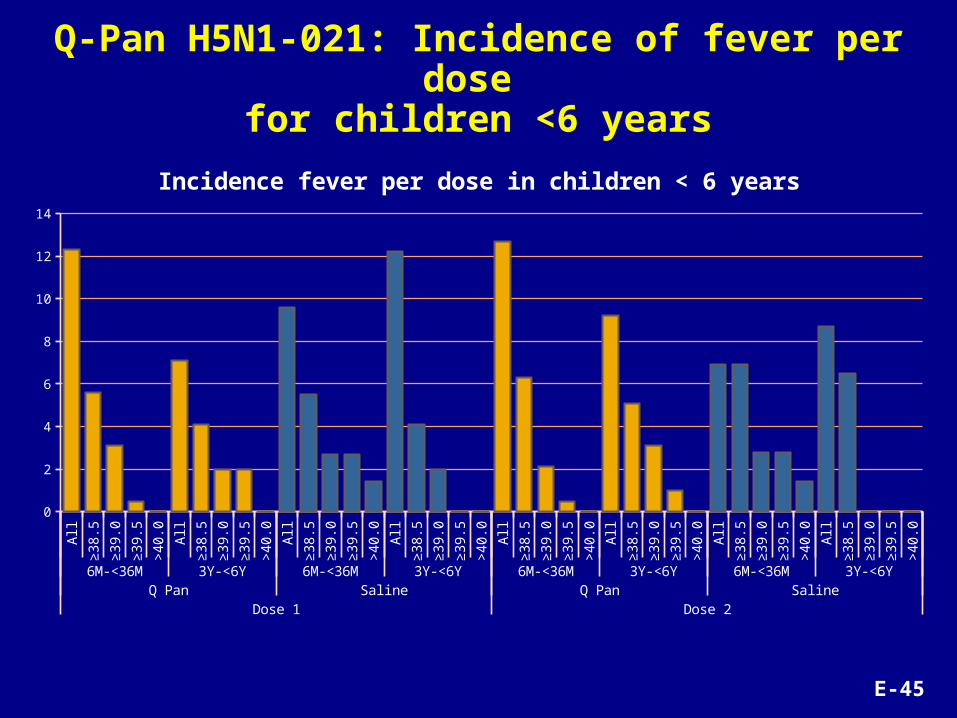
Q-Pan H5N1-021: Incidence of fever per dose for children <6 years
All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0 All
≥3
8.5
≥3
9.0
≥3
9.5
>4
0.0
6M-<36M 3Y-<6Y 6M-<36M 3Y-<6Y 6M-<36M 3Y-<6Y 6M-<36M 3Y-<6YQ Pan Saline Q Pan Saline
Dose 1 Dose 2
0
2
4
6
8
10
12
14
Incidence fever per dose in children < 6 years
E-45

Quebec* and Dresden* Manufacturing Processes
Downstream Process & Formulation
Quebec Dresden
virus inactivated UV followed by formaldehyde
virus concentrated and purified by zonal centrifugation using a linear sucrose density gradient solution containing detergent to split the virus
purified by centrifugation and disrupted by deoxycholate
further purified by diafiltration
inactivated by consecutive effect of deoxycholeate and formaldehyde
Tween-80, triton X-100 and magnesium chloride used as excipients for the formulation
* As per US PI 2012/2013
No Difference In Upstream Process
MW-1MW-94

Injection site pain (18 to 64 years) (Q-Pan-002)Q
-PAN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Q-P
AN
Plac
ebo
Day 0 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 0 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Dose 1 Dose 2
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
69.2
13.8
74.6
6.9
55.0
4.4
29.3
2.3
12.7
1.16.3
1.13.7
0.4
67.2
9.2
66.8
6.0
44.6
2.5
20.1
1.6
8.4
0.83.7
0.5 2.3 0.4
1.7
0.3
2.4
0.0
1.4
0.0
0.6
0.1
0.3
0.1
0.1
0.00.0
0.0
2.1
0.1
1.9
0.1
0.8
0.3
0.4
0.1
0.1
0.00.0
0.00.0
0.0
Percentage of subjects who reported Pain
Grade3
Any
Pe
rce
nta
ge
of
Su
bje
cts
S-5

Autoimmune Hepatitis: Evidence Does Not Support a Causal Relationship
Q-Pan H5N1 and D-Pan H5N1 clinical trials
• 2 reports– Q-Pan-H5N1 002 – 29 y/o male, AIH experts considered
diagnosis doubtful, possibly non-specific reactive hepatitis; likely prevalent disease
– D‑Pan H5N1 009– 3.5 y/o, female; probable AIH, prevalent (pre-existing) disease
• Both CHMP and a panel of external experts concluded, after review of GSK’s of H5N1 and H1N1 clinical development programs: the evidence does not support a causal association between AS03-adjuvanted vaccines and AIH
S-15

Autoimmune Hepatitis: D-Pan H1N1 Spontaneous Reports
Postmarketing use of D-Pan H1N1
• 5 spontaneous reports
• at least 31 million doses administered
• well below the expected (background) incidence of 1 – 2 cases/100,000 person-years, taking underreporting into account
Age (years), gender
AIH Diagnostic
Score
Comments
14, F 3 Concurrent cholecystitis and E. coli bacteremia
10, F 6 Severe acne, family h/o lupus
17, F 0 JRA with renal involvement
65, F 3 h/o bile duct surgery
14, F 7 Abdominal pain, nausea and cold sweat 7 mos prior to vaccination
Definite AIH: score 7; Probable AIH: score 6
S-16

Non-Adjuvanted H1N1 Vaccine Postmarketing Studies: Guillain-Barré Syndrome (GBS)
SCCS= Self controlled case series
Author(country)
Study design (Age range)
N Cases
N Exposed Adjuvant
OR: overall + age stratified
95% CI
Tokars, 2012 (USA)
SCCS (1 – 84) 59 59 Non-
adjuvanted
Overall: 2.1 (1.2 – 3.5)0.5 – 24: 3.0 (1.0 – 9.1)25 – 49: 2.0 (0.7 – 5.5)50 – 64: 2.1 (0.8 – 5.6) ≥ 65: 1.0 (0.5 – 4.3)
Greene, 2012 (USA)
Self controlled risk interval (1- 71)
29 13 Non-adjuvanted Overall: 4.4 (1.3 – 14.2)
Wise, 2012 (USA)
Cohort 411 29Non-
adjuvantedOverall: 1.57 (1.02 – 2.21)< 25: 1.67 (0.58 – 3.22)≥ 25: 1.54 (0.90 – 2.25)
Yih, 2011 (USA)
Self controlled risk interval
(<18 - 65+)5 3
Non-adjuvanted Overall: 2.5 (0.42 – 15.0)
S-34
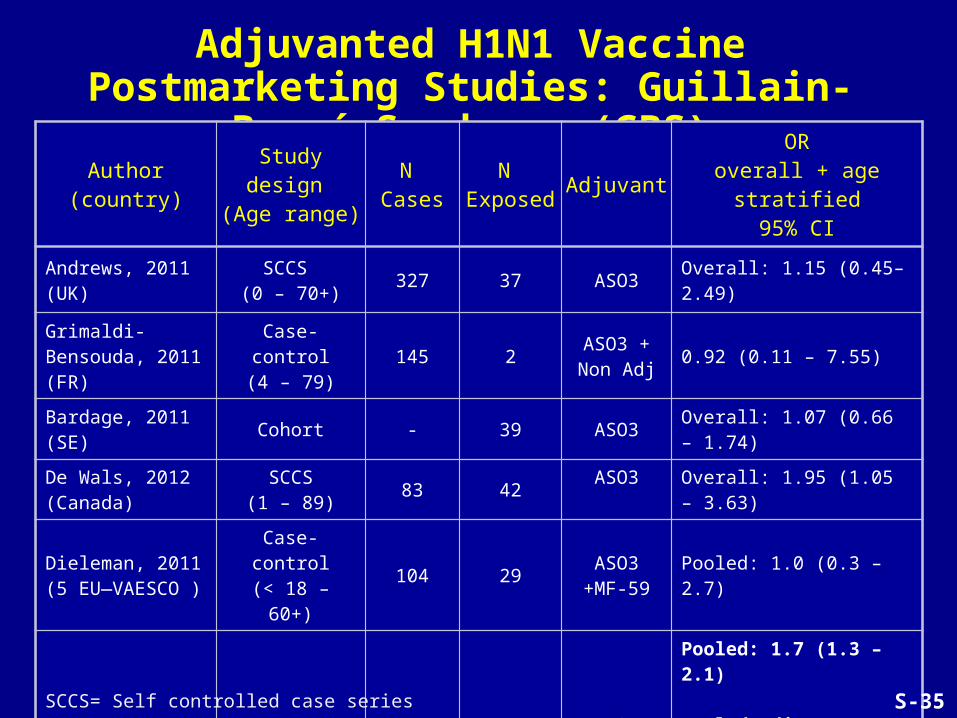
Adjuvanted H1N1 Vaccine Postmarketing Studies: Guillain-Barré Syndrome (GBS)
Author(country)
Study design (Age range)
N Cases
N Exposed Adjuvant
ORoverall + age stratified
95% CI
Andrews, 2011 (UK)
SCCS (0 – 70+)
327 37 ASO3 Overall: 1.15 (0.45–2.49)
Grimaldi-Bensouda, 2011 (FR)
Case-control(4 – 79)
145 2ASO3 + Non Adj
0.92 (0.11 – 7.55)
Bardage, 2011 (SE)
Cohort - 39 ASO3 Overall: 1.07 (0.66 – 1.74)
De Wals, 2012 (Canada)
SCCS(1 – 89)
83 42ASO3
Overall: 1.95 (1.05 – 3.63)
Dieleman, 2011(5 EU—VAESCO )
Case-control(< 18 – 60+)
104 29ASO3
+MF-59Pooled: 1.0 (0.3 – 2.7)
WeibelGlobal
Meta-analysis1,163 253
ASO3 +MF-59
+ Non Adj
Pooled: 1.7 (1.3 – 2.1)
Pooled Adj (UK, EU, CA, Fr, SE): 1.3(0.9 – 1.8)
Pooled non-Adj (USA): 1.9 (1.4 — 2 .6)
SCCS= Self controlled case series S-35

SOTR: Results of selected, published studiesStudy size Outcome Reference
216 SOTR 138 controls
No increase in incidence of graft rejection Siegrist 2012
151 kidney TR Anti-HLA antibodies in 17.3% and 11.9% (2 cohorts) vs. 6% in historical controls (seasonal TIV); transient, no change in graft function
Katerinis 2011
111 kidney TR No change in anti-HLA I/II antibody prevalence Broeders 2011
47 heart TR No clinical graft rejection Meyer 2011
15 heart TR60 controls
No clinical graft rejection, increase in cellular rejection on biopsies (small numbers, limited adjustment for confounding)
Schaffer 2011
168 lung TR No rejection events reported Schuurmans 2011
107 kidney TR 5.6% de novo DSA, comparable to seasonal flu vaccine; 2 humoral rejections with graft loss (no unvaccinated controls)
Brakemeier 2011
5 heart TR No clinical evidence of rejection after 6 months follow-up Altamirano 2011
127 liver Similar % of AEs in vaccinated transplant recipients and healthy controls. No clinical rejection
Goldschmidt 2011
79 kidney No rejection events reported Crespo 2011
S-39