Magnetic resonance imaging and nuclear magnetic resonance ...
Upload
muhammad-bin-zulfiqarCategory
view
107download
0
85 Magnetic Resonance Pancreatography

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

• Fig GI 85-1 Anatomic variant. Persistent duct of Santorini (arrow) enters the minor ampulla and lies cephalad to the duct of Wirsung.179

• Fig GI 85-2 Pancreas divisum. (A) The distal bile duct (arrowhead) joins the ventral pancreatic duct (arrows) to enter the major ampulla. (B) The dorsal pancreatic duct (arrows) enters the minor ampulla (arrowhead) cephalad to the major ampulla. Subsequent images helped confirm the absence of communication between the central and dorsal pancreatic ducts.180

• Fig GI 85-3 Annular pancreas. The lesion was detected incidentally in a 61-year-old man, in whom cannulation of the bile duct was not possible during ERCP. (A) Curvilinear duct (arrows) in the annular pancreas. (B) Coronal T1-weighted abdominal image demonstrates the annular pancreas (arrows) lying lateral to the fluid-filled duodenum (arrowhead).179

Fig GI 85-4 Anomalous union of the pancreatic and bile ducts. The anomalous union (arrowhead) is associated with a choledochal cyst (arrows).179

• Fig GI 85-5 Pancreatic trauma. (A) Acute disruption of the pancreatic duct (arrowheads), which terminates in an 8-mm fluid collection (arrow) in the pancreatic tail. Note the large adjacent pseudocyst (*). (B) In another patient 17 years after blunt abdominal trauma, there is an abrupt point of transition between the normal pancreatic duct (arrow) and the dilated duct (arrowheads) in the body and tail of the gland.179
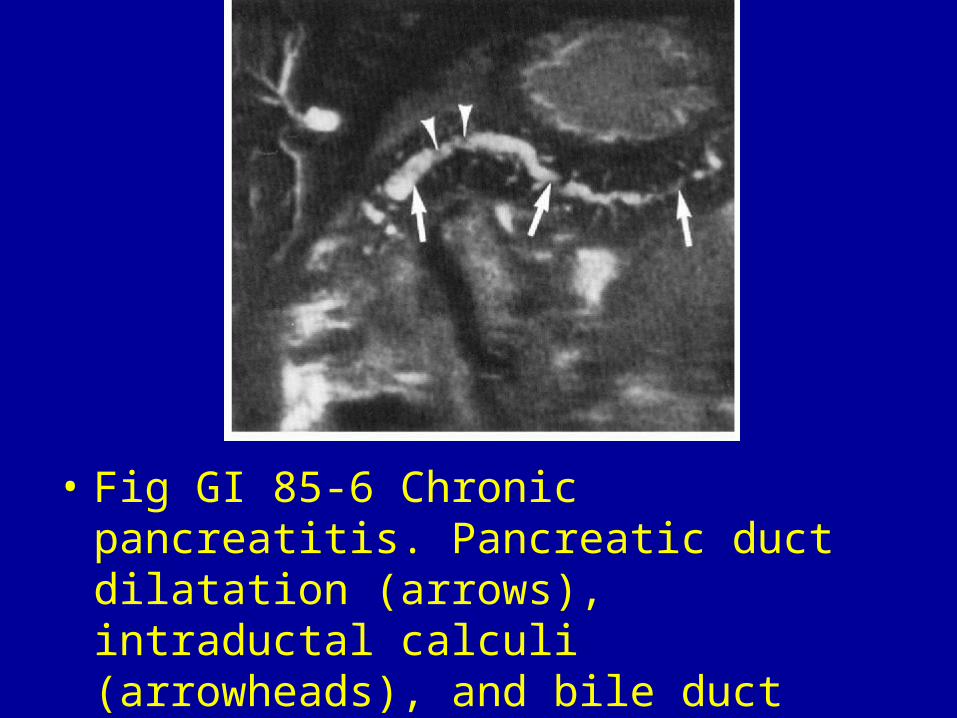
• Fig GI 85-6 Chronic pancreatitis. Pancreatic duct dilatation (arrows), intraductal calculi (arrowheads), and bile duct stricture.179

• Fig GI 85-7 Chronic pancreatitis. Smooth, tapering stricture of the intrapancreatic bile duct (arrowhead), which is characteristic of this condition. The pancreatic duct (arrows) is dilated and tortuous. The gallbladder (*) is distended.179

• Fig GI 85-8 Pseudocyst. Dilatation of the pancreatic duct and its side branches (arrows), which terminate in a large pseudocyst (*) that is inseparable from the pancreatic tail (arrowhead). MR pancreatography was performed to delineate the ductal anatomy prior to pancreaticojejunostomy.179

• Fig GI 85-9 Carcinoma of the pancreas. The dilated extrahepatic bile duct (straight arrow) terminates in a pancreatic head mass (*). A biliary stent, which appears as a linear filling defect in the dilated bile duct, is seen to contain fluid (arrowhead) as it traverses the mass in the pancreatic head. Note the narrowing of the pancreatic duct (curved arrow) secondary to the mass.179