
24-Hour infusion of cis-platinum in head and neck cancers
6
24-HOUR INFUSION OF CIS-PLATINUM IN HEAD AND NECK CANCERS CHARLOTTE JACOBS, MD,* JOSEPH R. BERTINO, MD,? DON R. GOFFINET, MD,$ WILLARD E. FEE, MD,§ AND RICHARD L. GOODE, MD" Eighteen patients with advanced squamous cell cancer of the head and neck were treated with cis-diamminedichloroplatinum in a 24-hour infusion. The most frequent dose used was 80 mg/m2 repeated every three weeks. Six were treated preoperatively for Stage I11 or IV disease, and twelve were treated for recurrent disease. The overall response rate was 72% with one complete remission, >50% regression in six patients, and 25-50% regres- sion in six patients. Toxicity was minimal: creatinine >2 in 6% of courses, leukopenia in 9%, anemia in 29%, vomiting in 76%, and documented minimal hearing loss in one patient. Plasma and urine platinum levels during infusion are presented. The dosage of 80 mg/m2 administered over 24 hours gives a response rate in head and neck cancers equivalent to that reported with higher doses given by rapid infusion, and toxicity is minimal. Cancer 42:2135-2140. 1978. IS-DIAMMINEDICHLOROPLATINUM (CP, C NSC 119875) has been noted in clinical trials to have activity in several human malig- nancies, including squamous cell cancer of the head and neck.6,10,13 However, nephrotoxicity has prevented more extensive use of this com- p~und.~,"~ In an attempt to modify renal toxicity, a variety of doses and schedules have been used. Animal studies have shown that prehydration and concomitant mannitol diuresis allowed larger doses of CP to be given without serious nephrotoxicity.2 Sub- sequently, Hayes' showed that patients could From the Departments of Medicine, Radiology, and Surgery, Stanford University, Stanford, California. Supported by grants CA 08122-10 and 05822 from the National Cancer Institute, National Institute of Health. * Acting Assistant Professor, Division of Oncology, Department of Medicine, Stanford University School of Medicine. t American Cancer Society Professor of Medicine and Pharmacology, Chief of Oncology, and Josiah Macy Jr. Faculty Scholar, Yale University School of Medicine, New Haven, Connecticut. $ Assistant Professor of Radiation Therapy, Depart- ment of Radiology, Stanford University School of Medicine. 0 Assistant Professor of Otolaryngology, Department of Surgery, Stanford University School of Medicine. I' Associate Professor of Otolaryngology, Department of Surgery, Stanford University of School of Medicine. Address for reprints: Charlotte Jacobs, MD, Division of Oncology, Room S-025, Stanford University Medi- cal Center, Stanford, CA 94305. Accepted for publication January 18, 1978. tolerate high doses of CP with minimal renal toxicity if adequate prehydration and vigorous mannitol diuresis were used. Drewinko et aL4 studied the killing effect of CP given as pulse vs. infusion in cultured human lymphoma cells. Their findings suggested that better antitumor effect with less toxicity may be ob- tained by infusion of low doses of CP. Since renal toxicity may be related to high plasma levels of CP achieved after rapid injec- tion, the purpose of this investigation was to attempt to improve the therapeutic index of this drug in patients with squamous cell carcinoma of the head and neck by use of a 24-hour infusion with adequate hydration but without mannitol diuresis. MATERIALS AND METHODS Between November 1976 and April 1977, 18 patients with advanced squamous cell cancer of the head and neck were treated with 34 courses of Cis-Platinum. The group consisted of 14 men and 4 women with a mean age of 60 and a range of 36-78 years. All patients had a Karnovsky status of >60. The primary sites of disease were (Table 1): oral cavity - 8, larynx - 5, nasopharynx- 2, oropharynx-2, and hypopharynx-1. Six pa- tients were treated with one or two courses preoperatively for stage 111 or IV disease; twelve patients were treated for recurrent disease following radiation and surgery- nine of these twelve patients had local recur- 0008-543X/78/1100/2 135 $0.80 0 American Cancer Society 2135
-
Upload
charlotte-jacobs -
Category
Documents
-
view
216 -
download
0
Transcript of 24-Hour infusion of cis-platinum in head and neck cancers

24-HOUR INFUSION OF CIS-PLATINUM IN HEAD AND NECK CANCERS
CHARLOTTE JACOBS, MD,* JOSEPH R. BERTINO, MD,? DON R. GOFFINET, MD,$ WILLARD E. FEE, MD,§ A N D RICHARD L. GOODE, MD"
Eighteen patients with advanced squamous cell cancer of the head and neck were treated with cis-diamminedichloroplatinum in a 24-hour infusion. The most frequent dose used was 80 mg/m2 repeated every three weeks. Six were treated preoperatively for Stage I11 or IV disease, and twelve were treated for recurrent disease. The overall response rate was 72% with one complete remission, >50% regression in six patients, and 25-50% regres- sion in six patients. Toxicity was minimal: creatinine >2 in 6% of courses, leukopenia in 9%, anemia in 29%, vomiting in 76%, and documented minimal hearing loss in one patient. Plasma and urine platinum levels during infusion are presented. The dosage of 80 mg/m2 administered over 24 hours gives a response rate in head and neck cancers equivalent to that reported with higher doses given by rapid infusion, and toxicity is minimal.
Cancer 42:2135-2140. 1978.
IS-DIAMMINEDICHLOROPLATINUM (CP, C NSC 119875) has been noted in clinical trials to have activity in several human malig- nancies, including squamous cell cancer of the head and neck.6,10,13 However, nephrotoxicity has prevented more extensive use of this com- p ~ u n d . ~ , " ~ In an attempt to modify renal toxicity, a variety of doses and schedules have been used. Animal studies have shown that prehydration and concomitant mannitol diuresis allowed larger doses of CP to be given without serious nephrotoxicity.2 Sub- sequently, Hayes' showed that patients could
From the Departments of Medicine, Radiology, and Surgery, Stanford University, Stanford, California.
Supported by grants CA 08122-10 and 05822 from the National Cancer Institute, National Institute of Health.
* Acting Assistant Professor, Division of Oncology, Department of Medicine, Stanford University School of Medicine.
t American Cancer Society Professor of Medicine and Pharmacology, Chief of Oncology, and Josiah Macy Jr. Faculty Scholar, Yale University School of Medicine, New Haven, Connecticut.
$ Assistant Professor of Radiation Therapy, Depart- ment of Radiology, Stanford University School of Medicine. 0 Assistant Professor of Otolaryngology, Department
of Surgery, Stanford University School of Medicine. I' Associate Professor of Otolaryngology, Department
of Surgery, Stanford University of School of Medicine. Address for reprints: Charlotte Jacobs, MD, Division
of Oncology, Room S-025, Stanford University Medi- cal Center, Stanford, CA 94305.
Accepted for publication January 18, 1978.
tolerate high doses of CP with minimal renal toxicity if adequate prehydration and vigorous mannitol diuresis were used. Drewinko et aL4 studied the killing effect of CP given as pulse vs. infusion in cultured human lymphoma cells. Their findings suggested that better antitumor effect with less toxicity may be ob- tained by infusion of low doses of CP.
Since renal toxicity may be related to high plasma levels of CP achieved after rapid injec- tion, the purpose of this investigation was to attempt to improve the therapeutic index of this drug in patients with squamous cell carcinoma of the head and neck by use of a 24-hour infusion with adequate hydration but without mannitol diuresis.
MATERIALS AND METHODS
Between November 1976 and April 1977, 18 patients with advanced squamous cell cancer of the head and neck were treated with 34 courses of Cis-Platinum. The group consisted of 14 men and 4 women with a mean age of 60 and a range of 36-78 years. All patients had a Karnovsky status of >60. The primary sites of disease were (Table 1): oral cavity - 8, larynx - 5, nasopharynx- 2, oropharynx-2, and hypopharynx-1. Six pa- tients were treated with one or two courses preoperatively for stage 111 or IV disease; twelve patients were treated for recurrent disease following radiation and surgery- nine of these twelve patients had local recur-
0008-543X/78/1100/2 135 $0.80 0 American Cancer Society
2135

2136 CANCER Nouember 1978 Vol. 42
TABLE 1 . Clinical Data on 18 Patients with Head and Neck Cancers Treated with Platinum
Patient 1" Site Stage at Rx Prior Rx Dose Response
R.R.
F.M.
B.B.
J.P.
W.T.
F.G. S.L.
B.R.
H.Y.
R.F.
M.F. E.O.
W.M.
A.W.
A.T.
T.M.
J.S.
R.T.
floor of mouth
oral tongue
aryepiglottic fold
supraglottic larynx
floor of mouth
hard palate nasopharnyx
aryepiglottic fold
nasopharynx
base of tongue
buccal space oral tongue
base of tongue
arytenoid
arytenoid
oral tongue
pyriform sinus
oral tongue (& hypopharnyx)
local recurrence skin mets
local recurrence
lung mets
lung mets
local recurrence
T4NnMn* liver mets
local recurrence
local recurrence
TiNZMn
T,Ni&fn local recurrence
local recurrence skin mets
TJ'JoMo
base of tongue recurrence
T&"Mo
T&"Mo
local recurrence
surgery radiation
surgery radiation
surgery radiation chemotherapy
surgery radiation chemotherapy
radiation
none radiation chemotherapy
surgery radiation
radiation
none
none surgery radiation
surgery radiation
none
surgery radiation chemotherapy
none
none
surgery radiation
110, 100, 80 80, 80
80, 80
120, 120 50, 80
50
95, 130
120 80
80
80
80, 80
85, 85 80
80, 80, 95 80
80, 80
70
125
120
80, 110
CR
>50%
>50%
>50%
>50%
>50% >50%
25-50%
25-50%
25-50%
25-50% 25-50%
25-50%
subjective
subjective
N R
N R
NR
* Patients previously untreated were staged according to the TNM staging system.
rences, the other three patients had distant metastases (lung-2, liver- 1). Prior treatment consisted of surgery, radiation, and chemo- therapy in three patients; surgery and radia- tion in six patients; radiation and chemo- therapy in one patient; radiation in two pa- tients; and no prior treatment in six patients.
Pretreatment evaluation consisted of his- tory and physical exam, blood counts, liver function tests, BUN, creatinine, creatinine clearance, urinalysis, chest x-ray and audio- gram. Blood counts and creatinine were re- peated at least twice during each cycle. Audio- grams were repeated every two cycles. Gastro- intestinal toxicity was evaluated with each cycle.
Response was evaluated weekly by a team of observers consisting of an otolaryngologist, a radiotherapist, and a medical oncologist. Measurements in two dimensions were re- corded and photographs were used to fol- low patients with disease that was difficult to measure. A patient was called a com- plete responder only if biopsies of prior posi- tive sites showed no evidence of malignancy. Partial responders were categorized either as >50% decrease in all measureable disease or 25-50410 decrease in all measurable disease. Length of response was the time from onset of response to progression.
Blood and urine samples were obtained at various times during the treatment period in

No. 5 CIS-PLATINUM I N HEAD/NECK CA . Jacobs et al. 2137
selected patients. Platinum concentration in plasma and urine were determined by atomic absorption This method measures elemental platinum concen- tration, but does not distinguish between CP and its possible metabolites.
spec t r o p h o to m e try . ' 3 ' l
DKUG AIIMINISTKAI ION
CP was obtained from the National Cancer Institute. 'Ten mg vials were reconstituted with sterile water just before use. The total dose was delivered over 24 hours. One-sixth of the total dose was administered in 1 liter of fluid every 4 hours. This was followed by 24 hours of fluid at 150 cc/hour. The doses varied from 50 mg/m*- 130 mg/m2 with most patients receiving 80 mg/m2 (Table 1). Plati- num was given every 3-4 weeks and individ- ual patients received from one to five courses.
Therapeutic Results
The results in 18 cases are shown in Table 1. The overall response rate was 72% with 1 com- plete remission, >50% regression in 6 pa- tients, and 25-50s regression in 6 patients. Four patients with 25-50s regression under- went surgery or radiation after one or two courses as part of a pilot program and re- ceived no additional chemotherapy. All pa- tients who responded showed evidence of re- sponse after one course of the drug. Two pa- tients had subjective responses, relief of pain and hoarseness, and three patients had no improvement. All three patients with no re- sponse had bulky disease that was difficult to evaluate; two of these had no prior treat-
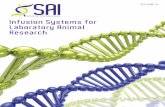
ment and underwent surgery within two weeks. These three patients received doses of 110- 120 mg/m2. Pathologic grading, prior radiation therapy and prior chemotherapy had no influence upon response rate. The three patients with distant metastases re- sponded well to CP (Fig. 1). The dose of 80 mg/m2 was sufficient for good responses, and although this was not a dose response study, higher doses than 80 mg/m2 did not appear to cause an improvement in response rate or magnitude or response. One patient is in complete remission at 6+ months, and partial responses have lasted from 2-4+ months.
Toxicity
Toxicity was minimal and tolerable (Table 2). There was no renal toxicity associated with 27 of the 34 courses. Five courses were associated with transient and reversible crea- tinine elevations of >2 mg/dl. Two courses were associated with creatinine elevations >2 mg/dl. Both occurred after repeated doses of 120 mg/m2 and were partially reversible. N o patient had renal failure. The creatinine elevations were noted as early as one week posttreatment and lasted from two weeks to two months.
Hematologic toxicity was mild. Leukopenia of <3000/mm3 occurred in 4/34 courses at 3-4 weeks, usually following higher doses. Thronibocytopenia of <100,000 occurred transiently in 3/34 courses at 2-3 weeks. More striking was the anemia with 2-3 g decrease in hemoglobin in 10/34 courses. The anemia
FIG. 1. Patient B.R. with carcinoma of the aryepiglottir fold metastatic to lung. A) Before treatment; B) After treatment.

2138 CANCER November 1978 Vol. 42
TABLE 2. Toxicity with 24 Hour Infusion of Cis-Platinum
% of Average Total platinum
Toxicity courses (34) (mg/m2) No. of courses dose
Nausea and vomiting Mild Moderate Severe
Creatinine 1.2-2 mg/dl Creatinine >2 mg/dl
Leukopenia
Renal
Hematologic
3000-4000/mm3 <3000/mm3
Thrombocytopenia 100,000- 150,000/mm3 50,000- 100,00o/mm3
Hemoglobin decrease 2-3 gidl
Heptotoxicity (?SCOT) Seizure Hair loss Ototoxicity
Tinnitus Objective loss Subjective loss
17 50 8 23.5 1 3 120
5 14.7 90 2 5.9 120
4 11.8 84 4 11.8 103
3 8.8 124 3 8.8 90
10 29.4 88 2 5.9 80 1* 2.9 2 11.1t
1 5.6t 1 5.6t 1 5.6t
* Patient had hyponatremia. t % of number of patients.
occurred most frequently at 3-4 weeks and was normochromic-normocytic. There were no episodes of sepsis or hemorrhage.
Nausea and vomiting occurred with 26 courses. It was mild and of short duration in 17, moderate and of short duration in 8, and prolonged in 1. Nausea and vomiting were not present in 8 courses.
TIME AFTER START OF INFUSION (hours)
FIG. 2. Plasma Platinum Levels in 2 Patients 'Treated with 80 mg/rn2. ~ , patient E.O.; - - -, patient F.M.
Twenty-three serial audiograms were per- formed in 10 patients. Only one revealed a slight increase in neuro-sensory loss, and that patient noted transient tinnitus and subjec- tive hearing loss.
Two patients noted hair thinning and there were no episodes of dermatitis or cutaneous allergic reactions. Two patients experienced transient hyponatremia with large fluid load; one had a related seizure. There were no fistulae or delayed wound healing in patients who received CP prior to surgery. N o drug- related deaths occurred.
Pharmacology
During the 24-hour infusion of CP, plasma platinum levels were drawn at various time intervals, and 24-hour urine collections were obtained. The peak plasma levels occurred at 24 hours and ranged from 1.03 to 1.90 pglml with a mean of 1.39 pglml in nine patients tested. Figure 2 illustrates the typical time course of plasma levels of platinum in two patients during and following a 24- hour infusion of 80 mg/m2. Plasma levels were not obtained at higher doses. The per- centage of total dose excreted in the 24 hours during infusion averaged 14% (Table 3); in one case of renal insufficiency only 6.1% was excreted during this time period.
DISCUSSION
Chemotherapy for advanced squamous cell carcinoma of the head and neck has had limited effectiveness.' Single agent chemo- therapy responses with hydroxyurea, bleo- mycin or cyclophosphamide have been re- ported in 30-40% of patients. Thus far, methotrexate appears to be the most effec- tive agent with the range of response vary- ing from 30-50%. Responses are usually incomplete with short remission durations. The use of combination chemotherapy has not significantly improved responses.
CP is an effective new agent for squamous cell cancers of the head and neck. Gottlieb et al." reported a 41% response. Using high intermittent doses with diuresis, Wittes et al. have reported objective responses in 69% of patients.13 In our series of 18 patients, we noted 39% remissions of >50% and 33% re- missions of 25-50% with a total response rate of 72%. However, of greatest importance will be the remission duration. Although most

No. 5 CISPLATINUM IN HEAD~NECK CA . Jacobs et al. 2139
studies do not yet have long-term follow-up, Wittes13 reported complete response of 2 + and 6+ months and partial responses last- ing 1-8+ months. In our series one patient is in complete remission at 6+ months, and partial responses have lasted from 2-4+ months.
Ability to deliver optimal doses of this drug and to continue courses of drug is prohibited in many cases by renal toxicity. The renal pathology caused by CP has been described by Gonzales-Vitale5 as focal acute tubular necrosis affecting the distal convoluted tubules and collecting ducts. A variety of schedules have been used in hu- mans in an attempt to decrease renal toxic- ity.6 Pie1 and Perlia12 suggested that renal toxicity could be diminished by giving the drug IV drip at 1 mg/minute. Cvitkovic2 showed in animal studies that prehydration and concomitant mannitol diuresis allowed larger doses to be given with minimal nephrotoxicity. Hayes7 used this method of administration and showed that patients could tolerate high doses of CP with minimal nephrotoxicity. Although mannitol is felt to protect against this toxicity, the mechanism is not known.
In our study, we chose to deliver the total dose of CP over a 24-hour period while maintaining a large urine output--200-250 cc/hour, followed by vigorous hydration for the following 24 hours. We felt that toxicity may be reduced by delivering less drug to the kidney per unit of time while maintain- ing large urine volumes. Minimal and re- versible creatinine elevations of 1.2-2 oc- curred in 4 of 34 courses. Three patients who had transient creatinine elevations were treated again with CP with no toxicity. Creatinine elevations of > 2 occurred in 2 of 34 courses, and both of these were following repeated high doses (120 mg/m2). At 80 mg/m2 CP in a 24-hour infusion only mini- mal renal toxicity has been observed with no reduction in response rates. At this dose level it may be safe to give multiple courses on a 3-week schedule; however, more patients treated over a longer period of time will be necessary before this conclusion is firm.
Hematologic toxicity was minimal and rarely dose-limiting. Significant leukopenia was noted in 12% of cases and significant thrombocytopenia in 8%. As reported by other^,^,^,^ the nadir is at approximately 3 weeks. Progressive anemia has been noted
TABLE 3. 24-Hour Infusion of Cis-Platinum
% Dose platinum excretion excreted
Dose 24-Hour
Patient (mg) (mg) in 24 hours
A.W. 160 21.3 13.3% W.M. 140 17.9 12.8% E.O. 180 21.7 12.1% F.M. 130 21.7 16.7% B.B.* 100 6.1 6.1% A S . 180 26.3 14.6%
* Patient had creatinine clearance of 45 ccirninute.
following Cis-Plat in~m,~”~ and 29% of our courses had an associated normochromic- normocytic anemia.
The use of the 24-hour infusion resulted in some reduction of nausea and vomiting. Fifty percent of courses had mild GI toxicity, and 24% had no associated GI toxicity. In this series ototoxicity was minimal.
The toxicity of the 24-hour infusion regi- men compares favorably with other series. Hayes7 treated patients with 3-5 mg/kg platinum as a rapid infusion followed by mannitol diuresis and noted the following toxicity: serious myelosuppression-22%; creatinine >2- 19%; subclinical hearing loss- 90%; deafness-6%. However, most of our patients received only 80 mg/m2, and since good responses were obtained, the dose was not increased. There was no increase in renal toxicity in the few patients treated with higher doses, but the patient numbers are too small for comparison.
During a 24-hour infusion, peak plasma levels of platinum ranged from 1-2 kg/ml. Following 3 mg/kg platinum given by rapid infusion, peak plasma levels achieved were 10 ~ g / m l . ~ During the 24-hour infusion, urinary excretion was approximately 14% as compared with 18-30% following rapid in- fision.3 However, urinary excretion following the infusion should be performed. I t is of interest that in the patient with impaired creatinine clearance, only 6% of the dose was excreted in the first 24 hours. If peak plasma levels are related to renal toxicity, additional dose schedules of CP should be explored, ie., longer infusions or lower doses administered at more frequent intervals.
These studies indicate that CP can be given safely and effectively to patients with squa- mous cell cancer of the head and neck. The dosage of 80 mg/m2 administered over 24

2 140 CANCER November 1978 Vol. 42
hours gives a response rate equivalent to that reported with higher doses given by rapid injection. In addition, the 24-hour infusion has minimal toxicity, which may allow multi- ple courses to be given. It should be possible to combine CP given in this manner with
other agents such as methotrexate and bleo- mycin, and possibly improve response rates and duration of response of these patients. Another possible use may be as an adjunct to conventional treatment in patients with ad- vanced disease.
REFERENCES
1. Bertino, J. R., Boston, B., and Capizzi, R. L.: The role of chemotherapy in the management of cancer of the head and neck: A review. Cancer 36:752-758, 1975.
2. Cvitkovic, E., Spaulding, J., Bethune, V., Martin, J.,, and Whitmore, W. F.: Improvement of cis-dichloro- diammine platinurn: Therapeutic index in an animal model. Cancer 39:1357-1361, 1977.
3. DeConti, R. C., Toftness, B. R., Larrge, R. C., and Creasey, W. A,: Clinical and pharmacologic studies with cis-diamminedichloroplatinum (11). Cancer Res. 33: 1310- 1315, 1973.
4. Drewinko, B., Brown, B. W., and Gottlieb, J. A,: l ' he effect of cis-diamminedichloroplatinum (11) on cul- tured human lymphoma cells and its therapeutic implications. Cancer Res. 33:3091-3095, 1973.
5. Gonzalez-Vitale, J. C., Hayes, D. M., Cvitkovic, E., and Sternberg, S. S.: The renal pathology in clinical trials of cis-platinum (11) diamminedichloride. Cancer 39:1362-1371, 1977.
6 . Gottlieb, J . A,, and Drewinko, B.: Review of the current clinical status of platinum coordination com- plexes in cancer chemotherapy. Cancer Chemother. Rep. 59:621-628, 1975.
7. Hayes, D. M., Cvitkovic, E., Golbey, R. B., Scheiner, E., Helson, L., and Karkoff, I. H.: High dose cis- platinum diammine dichloride. Cancer 39: 1372- 1381, 1977.
8. Hill, J. M., Loeb, E, MacLellan, A., Hill, N. O., Khan, A, , and King, J . I.: Clinical studies of platinum coordination compounds in the treatment of various malignant diseases. Cancer Chemother. Rep. 59:647- 659, 1975.
9. LeRoy, A. F., Friauf, W. S., Litterst, C. L., Gram, T. E., Guarino, D. M., and Dedrick, R. L.: Platinum analysis in biological tissues and fluid. I n Proc. Interna- tional Conference on Heavy Metals in the Environ- ment. Toronto, Ontario, Canada, 1975; pp D-70-D-72.
10. Lippman, A.J., Helson, C., Helson, L., and Krakoff, I. H.: Clinical trials of cis-diamminedichloroplatinum 11. Cancer Chemother. Rep. 57:191-200, 1973.
11. Litterst, C. L., Gram, 1'. E., Dedrick, R. I.., LeRoy, A. F., and Guarino, A. M.: Distribution arid disposition of' platinum following intravenous adminis- tration of cis-diamminedichloroplatinum (11) to dogs. Cancer Re,\. 36:2340-2344, 1976.
12. Piel, I. J., and Perlia, C. P.: Phase I1 study of cis-dichlorodiammine platinum (11) in combination with cyclophosphamide in the treatment of human malig- nancies. Cancer Chemother. Rep. 59:995-999 1975.
13. Wittes, R. E., Cvitkovic, E., Shah, J., Gerold, F. P., and Strong, E. W'.: Cis-dichlorodiammineplatinum (11) in the treatment of epidermoid carcinoma of the head and neck. Cancer Twat. Rep. 61:359-366, 1977.











![Untitled-5 [astemcelljourney.com]...Stem Cells and Regenerative Medicine Cancer Gene Thera or Cancer Cancer Clinical Trials New Drugs in Cancer Gene cancers Platinum Strategies Gene](https://static.fdocuments.net/doc/165x107/60def03e1e865e129a0b4ecd/untitled-5-stem-cells-and-regenerative-medicine-cancer-gene-thera-or-cancer.jpg)




