
22. Kernicterus - Shapiro - Children's Mercy Kansas · PDF file10/29/12 2 P.I.C.K. Parents of...
13
10/29/12 1 Steven Steven M. Shapiro M. Shapiro M.D M.D.. November 16 November 16, 2012 , 2012 Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics •• Kansas City, MO Kansas City, MO Division of Neurology • Department of Pediatrics Division of Neurology • Department of Pediatrics [email protected] [email protected] Steven Steven M. Shapiro M. Shapiro M.D M.D.. November 16 November 16, 2012 , 2012 Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics •• Kansas City, MO Kansas City, MO Division of Neurology • Department of Pediatrics Division of Neurology • Department of Pediatrics [email protected] [email protected] Outline Outline Objectives: •To understand the classical and subtle manifestations of neonatal bilirubin neurotoxicity new definitions of kernicterus and bilirubin induced neurological disorders (BIND), •To understand that bilirubin neurotoxicity can cause auditory neuropathy spectrum disorders (ANSD), which can be an unrecognized cause of speech and language delays. 1. Why care about bilirubin? 2. How does bilirubin damage the brain? Review of bilirubin metabolism Objectives: •To understand the classical and subtle manifestations of neonatal bilirubin neurotoxicity new definitions of kernicterus and bilirubin induced neurological disorders (BIND), •To understand that bilirubin neurotoxicity can cause auditory neuropathy spectrum disorders (ANSD), which can be an unrecognized cause of speech and language delays. 1. Why care about bilirubin? 2. How does bilirubin damage the brain? Review of bilirubin metabolism Children’s Mercy HOSPITALS & CLINICS Kansas City – Review of bilirubin metabolism – Correlation of damage with total unconjugated and free bilirubin 3. What are the types of damage and clinical symptoms that result? – Classical definitions of kernicterus; – New definitions: motor and auditory subtypes (ANSD), BIND 4. Relationship of kernicterus subtypes to neurodevelopment at time of peak bilirubin level (prematures -> auditory/ANSD) 5. Mistakes that can lead to kernicterus 6. How to know if bilirubin causes a neurological problem? 7. Conclusion – Review of bilirubin metabolism – Correlation of damage with total unconjugated and free bilirubin 3. What are the types of damage and clinical symptoms that result? – Classical definitions of kernicterus; – New definitions: motor and auditory subtypes (ANSD), BIND 4. Relationship of kernicterus subtypes to neurodevelopment at time of peak bilirubin level (prematures -> auditory/ANSD) 5. Mistakes that can lead to kernicterus 6. How to know if bilirubin causes a neurological problem? 7. Conclusion Why care about newborn jaundice? Why care about newborn jaundice? l Visible jaundice occurs in 60% Visible jaundice occurs in 60% of of term and term and ~80% ~80% preterm infants preterm infants l Bilirubin is bound to albumin in blood. When Bilirubin is bound to albumin in blood. When bilirubin levels bilirubin levels exceed exceed binding binding capacity of blood capacity of blood albumin, bilirubin moves into brain and causes albumin, bilirubin moves into brain and causes l Visible jaundice occurs in 60% Visible jaundice occurs in 60% of of term and term and ~80% ~80% preterm infants preterm infants l Bilirubin is bound to albumin in blood. When Bilirubin is bound to albumin in blood. When bilirubin levels bilirubin levels exceed exceed binding binding capacity of blood capacity of blood albumin, bilirubin moves into brain and causes albumin, bilirubin moves into brain and causes Children’s Mercy HOSPITALS & CLINICS Kansas City brain damage called brain damage called kernicterus kernicterus. “Kern “Kern-” ” deep nuclei or deep nuclei or kernel kernel of the brain of the brain “-icterus” icterus” from Greek = from Greek = yellow yellow Kernicterus Kernicterus = yellow staining of deep nuclei or = yellow staining of deep nuclei or kernel kernel of of brain brain l Prior to screening, treating and preventing Prior to screening, treating and preventing excessively high bilirubin levels, excessively high bilirubin levels, kernicterus kernicterus accounted accounted for for ~10 ~10% of % of cerebral palsy (CP) cerebral palsy (CP) brain damage called brain damage called kernicterus kernicterus. “Kern “Kern-” ” deep nuclei or deep nuclei or kernel kernel of the brain of the brain “-icterus” icterus” from Greek = from Greek = yellow yellow Kernicterus Kernicterus = yellow staining of deep nuclei or = yellow staining of deep nuclei or kernel kernel of of brain brain l Prior to screening, treating and preventing Prior to screening, treating and preventing excessively high bilirubin levels, excessively high bilirubin levels, kernicterus kernicterus accounted accounted for for ~10 ~10% of % of cerebral palsy (CP) cerebral palsy (CP) Why care ? Why care ? l Excessive jaundice in newborns may cause preventable brain damage , kernicterus, in neonate. l Kernicterus, can be extremely disabling and difficult to treat, causing severe dystonia (abnormal muscle tone) and deafness or auditory neuropathy spectrum disorders (ANSD) yet normal cognitive function! l Excessive jaundice in newborns may cause preventable brain damage , kernicterus, in neonate. l Kernicterus, can be extremely disabling and difficult to treat, causing severe dystonia (abnormal muscle tone) and deafness or auditory neuropathy spectrum disorders (ANSD) yet normal cognitive function! Children’s Mercy HOSPITALS & CLINICS Kansas City yet normal cognitive function! l Children can be virtually “locked in.” l Neonatal jaundice is very common problem with concern about a very rare but tragic sequelae – kernicterus! l 1:100,000 live births (Denmark, Great Britain, ?USA) l ~25x higher without screening and treatment yet normal cognitive function! l Children can be virtually “locked in.” l Neonatal jaundice is very common problem with concern about a very rare but tragic sequelae – kernicterus! l 1:100,000 live births (Denmark, Great Britain, ?USA) l ~25x higher without screening and treatment Why care? Why care? l Re-emergence of kernicterus in the USA in the 1990’s in part due to: l Due to early hospital discharge; lack of concern l Brain damage (kernicterus) is preventable l Re-emergence of kernicterus in the USA in the 1990’s in part due to: l Due to early hospital discharge; lack of concern l Brain damage (kernicterus) is preventable Children’s Mercy HOSPITALS & CLINICS Kansas City l Effects of bilirubin may be more prevalent and different in prematurely born infants l Excessive hyperbilirubinemia causes central auditory processing e.g., auditory neuropathy spectrum disorders (ANSD) and may cause or contribute to learning disorders. l Effects of bilirubin may be more prevalent and different in prematurely born infants l Excessive hyperbilirubinemia causes central auditory processing e.g., auditory neuropathy spectrum disorders (ANSD) and may cause or contribute to learning disorders. Front page of USA Today, October 2000 Children’s Mercy HOSPITALS & CLINICS Kansas City
Transcript of 22. Kernicterus - Shapiro - Children's Mercy Kansas · PDF file10/29/12 2 P.I.C.K. Parents of...

10/29/12
1
Steven Steven M. Shapiro M. Shapiro M.DM.D..November 16November 16, 2012, 2012
Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics •• Kansas City, MOKansas City, MODivision of Neurology • Department of PediatricsDivision of Neurology • Department of Pediatrics
[email protected]@cmh.edu
Steven Steven M. Shapiro M. Shapiro M.DM.D..November 16November 16, 2012, 2012
Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics Clinical Advances in Pediatrics • Children’s Mercy Hospital & Clinics •• Kansas City, MOKansas City, MODivision of Neurology • Department of PediatricsDivision of Neurology • Department of Pediatrics
[email protected]@cmh.edu
OutlineOutlineObjectives: •To understand the classical and subtle manifestations of neonatal bilirubin neurotoxicity
new definitions of kernicterus and bilirubin induced neurological disorders (BIND), •To understand that bilirubin neurotoxicity can cause auditory neuropathy spectrum
disorders (ANSD), which can be an unrecognized cause of speech and language delays.
1. Why care about bilirubin?2. How does bilirubin damage the brain?
Review of bilirubin metabolism
Objectives: •To understand the classical and subtle manifestations of neonatal bilirubin neurotoxicity
new definitions of kernicterus and bilirubin induced neurological disorders (BIND), •To understand that bilirubin neurotoxicity can cause auditory neuropathy spectrum
disorders (ANSD), which can be an unrecognized cause of speech and language delays.
1. Why care about bilirubin?2. How does bilirubin damage the brain?
Review of bilirubin metabolism
Children’s MercyHOSPITALS & CLINICS
Kansas City
– Review of bilirubin metabolism– Correlation of damage with total unconjugated and free bilirubin
3. What are the types of damage and clinical symptoms that result?– Classical definitions of kernicterus;– New definitions: motor and auditory subtypes (ANSD), BIND
4. Relationship of kernicterus subtypes to neurodevelopment at time of peak bilirubin level (prematures -> auditory/ANSD)
5. Mistakes that can lead to kernicterus6. How to know if bilirubin causes a neurological problem?7. Conclusion
– Review of bilirubin metabolism– Correlation of damage with total unconjugated and free bilirubin
3. What are the types of damage and clinical symptoms that result?– Classical definitions of kernicterus;– New definitions: motor and auditory subtypes (ANSD), BIND
4. Relationship of kernicterus subtypes to neurodevelopment at time of peak bilirubin level (prematures -> auditory/ANSD)
5. Mistakes that can lead to kernicterus6. How to know if bilirubin causes a neurological problem?7. Conclusion
Why care about newborn jaundice? Why care about newborn jaundice?
ll Visible jaundice occurs in 60% Visible jaundice occurs in 60% of of term and term and ~80% ~80% preterm infantspreterm infants
ll Bilirubin is bound to albumin in blood. When Bilirubin is bound to albumin in blood. When bilirubin levels bilirubin levels exceedexceed binding binding capacity of blood capacity of blood albumin, bilirubin moves into brain and causes albumin, bilirubin moves into brain and causes
ll Visible jaundice occurs in 60% Visible jaundice occurs in 60% of of term and term and ~80% ~80% preterm infantspreterm infants
ll Bilirubin is bound to albumin in blood. When Bilirubin is bound to albumin in blood. When bilirubin levels bilirubin levels exceedexceed binding binding capacity of blood capacity of blood albumin, bilirubin moves into brain and causes albumin, bilirubin moves into brain and causes
Children’s MercyHOSPITALS & CLINICS
Kansas City
,,brain damage called brain damage called kernicteruskernicterus..
“Kern“Kern--” ” deep nuclei or deep nuclei or kernelkernel of the brainof the brain““--icterus” icterus” from Greek = from Greek = yellowyellowKernicterusKernicterus = yellow staining of deep nuclei or = yellow staining of deep nuclei or kernelkernel of of
brainbrain
ll Prior to screening, treating and preventing Prior to screening, treating and preventing excessively high bilirubin levels, excessively high bilirubin levels, kernicterus kernicterus accounted accounted for for ~10~10% of % of cerebral palsy (CP)cerebral palsy (CP)
,,brain damage called brain damage called kernicteruskernicterus..
“Kern“Kern--” ” deep nuclei or deep nuclei or kernelkernel of the brainof the brain““--icterus” icterus” from Greek = from Greek = yellowyellowKernicterusKernicterus = yellow staining of deep nuclei or = yellow staining of deep nuclei or kernelkernel of of
brainbrain
ll Prior to screening, treating and preventing Prior to screening, treating and preventing excessively high bilirubin levels, excessively high bilirubin levels, kernicterus kernicterus accounted accounted for for ~10~10% of % of cerebral palsy (CP)cerebral palsy (CP)
Why care ? Why care ? l Excessive jaundice in newborns may cause
preventable brain damage, kernicterus, in neonate.l Kernicterus, can be extremely disabling and difficult to
treat, causing severe dystonia (abnormal muscle tone) and deafness or auditory neuropathy spectrum disorders (ANSD) yet normal cognitive function!
l Excessive jaundice in newborns may cause preventable brain damage, kernicterus, in neonate.l Kernicterus, can be extremely disabling and difficult to
treat, causing severe dystonia (abnormal muscle tone) and deafness or auditory neuropathy spectrum disorders (ANSD) yet normal cognitive function!
Children’s MercyHOSPITALS & CLINICS
Kansas City
yet normal cognitive function!l Children can be virtually “locked in.”
l Neonatal jaundice is very common problem with concern about a very rare but tragic sequelae –kernicterus!
l 1:100,000 live births (Denmark, Great Britain, ?USA)l ~25x higher without screening and treatment
yet normal cognitive function!l Children can be virtually “locked in.”
l Neonatal jaundice is very common problem with concern about a very rare but tragic sequelae –kernicterus!
l 1:100,000 live births (Denmark, Great Britain, ?USA)l ~25x higher without screening and treatment
Why care? Why care? l Re-emergence of kernicterus in the USA in
the 1990’s in part due to:l Due to early hospital discharge; lack of concern
l Brain damage (kernicterus) is preventable
l Re-emergence of kernicterus in the USA in the 1990’s in part due to:
l Due to early hospital discharge; lack of concern
l Brain damage (kernicterus) is preventable
Children’s MercyHOSPITALS & CLINICS
Kansas City
g pl Effects of bilirubin may be more prevalent
and different in prematurely born infantsl Excessive hyperbilirubinemia causes central
auditory processing e.g., auditory neuropathy spectrum disorders (ANSD) and may cause or contribute to learning disorders.
g pl Effects of bilirubin may be more prevalent
and different in prematurely born infantsl Excessive hyperbilirubinemia causes central
auditory processing e.g., auditory neuropathy spectrum disorders (ANSD) and may cause or contribute to learning disorders.
Front page of USA Today, October 2000
Children’s MercyHOSPITALS & CLINICS
Kansas City

10/29/12
2
P.I.C.K.Parents of Infants and Children with Kernicterus
P.I.C.K.Parents of Infants and Children with Kernicterus
Kernicterus, permanent brain damage due to
excessive newborn jaundice, is preventable with bilirubin
measurements and treatment.
www pickonline orgwww.pickonline.org
Jess, Age 11,Birmingham, Al.
.Krista, Age 9, Lexington, Ma.
Justin, Age 2, St. Paul, Mn.
Nathaniel, Age 3, Eagan, Mn.
David, Age 6, Eden Prairie, Mn.
Cal, Age 4, Boise, Id
www.kernicterus.org
Why care? JCAHO 2001Why care? JCAHO 2001
Issue 18, April 2001
Published for Joint Commission accredited organizations and interested health care professionals, Sentinel Event Alert identifies the most frequently occurring sentinel events, describes their
common underlying causes, and suggests steps to prevent occurrences in the future.
Children’s MercyHOSPITALS & CLINICS
Kansas City
y g , gg p p f
Kernicterus threatens healthy newborns
Kernicterus is a condition of newborns that leads to severely disabling brain damage or death. It results from hyperbilirubinemia that can be caused by a number of factors. Kernicterus is preventable with techniques currently available. Nevertheless, in recent years cases of kernicterus have continued to be reported. One registry includes 90 cases in the United States from 1984 to the present in which three of the newborns died and all others sustained brain damage.1 "This is probably happening more than clinicians know about," says Sue Sheridan, spokesperson for the advocacy, educational and support group PICK, Parents of Infants and Children with Kernicterus. "With these recent cases, risk assessments were inadequate and unreliable, and bilirubin levels were not measured--or measured in time." PICK has been instrumental in drawing attention to the reemergence of kernicterus and its prevention.
Children’s MercyHOSPITALS & CLINICS
Kansas City
Current concernsCurrent concerns•Kernicterus still occurs (1:100,000 LBs)
•Kernicterus may be the “tip of the iceberg.”
•Subtle kernicterus (aka BIND or bilirubin induced neurological disorders) may account for many more cases of:
•Kernicterus still occurs (1:100,000 LBs)
•Kernicterus may be the “tip of the iceberg.”
•Subtle kernicterus (aka BIND or bilirubin induced neurological disorders) may account for many more cases of:
Children’s MercyHOSPITALS & CLINICS
Kansas City
y– Learning disabilities,
– Central auditory processing disorders (ANSD),
– Dyslexia, oculomotor dyspraxia,
– Movement disorders, and
– Autism
– Adult disorders? May even predispose to Parkinson’s disease or schizophrenia
y– Learning disabilities,
– Central auditory processing disorders (ANSD),
– Dyslexia, oculomotor dyspraxia,
– Movement disorders, and
– Autism
– Adult disorders? May even predispose to Parkinson’s disease or schizophrenia
Newborn Jaundice and Autism – Oct 2010Newborn Jaundice and Autism – Oct 2010
Children’s MercyHOSPITALS & CLINICS
Kansas City
Children’s MercyHOSPITALS & CLINICS
Kansas City

10/29/12
3
BloodBlood LiverLiver GutGutBrainBrain
UGST UGST
Conj.Bili
Bf
Biliverdin
heme heme oxygenaseoxygenase
CO
HemoglobinA.Conj.Bili
E. F.
B.biliverdinbiliverdin
reductasereductase
Bilirubin MetabolismBilirubin Metabolism
D. UCB
UCB
StooStooll
StooStooll
f
Bf
C. UCB
Albumin
Bf Bf UCB
AlbuminX
Shapiro, Pediatric Neurology 29:410, 2003Shapiro, Pediatric Neurology 29:410, 2003
--glucuronidaseglucuronidase--glucuronidaseglucuronidase
Why Bilirbuin? The neuroprotective effect of mild hyperbilirubinemia
Why Bilirbuin? The neuroprotective effect of mild hyperbilirubinemia
Children’s MercyHOSPITALS & CLINICS
Kansas City
l Q: Why do we make bilirubin?
l A: It is an antioxidant. A mechan-ism exists - the bilirubin-biliverdincycle to amplify the antioxidant effect of bilirubin 10,000 times.
l It “cleans up” reactive oxygen species produced by mild birth asphyxia.
l Q: Why do we make bilirubin?
l A: It is an antioxidant. A mechan-ism exists - the bilirubin-biliverdincycle to amplify the antioxidant effect of bilirubin 10,000 times.
l It “cleans up” reactive oxygen species produced by mild birth asphyxia.
Amplification of the neuroprotective effect of bilirubinby redox cycling. Biliverdin is reduced to bilirubin bybiliverdin reductase (BVR) and is regenerated whenthe detoxification of reactive oxygen species (ROS)oxidizes bilirubin back to biliverdin. In this manner,low concentrations of bilirubin can be recycled toneutralize large amounts of ROS. (Greenberg DA,PNAS 99:15837, 2002)
PNASPNAS 99:16093, 2002; PNAS 99:15837, 200299:16093, 2002; PNAS 99:15837, 2002
Important Determinants of Neuronal Injury by Bilirubin*Important Determinants of
Neuronal Injury by Bilirubin*
l Concentration of unconjugated bilirubin (UCB) and free bilirubin (Bf)
l Concentration of serum albumin
Concentration of hydrogen ion (pH) the
l Concentration of unconjugated bilirubin (UCB) and free bilirubin (Bf)
l Concentration of serum albumin
Concentration of hydrogen ion (pH) the
Children’s MercyHOSPITALS & CLINICS
Kansas City
l Concentration of hydrogen ion (pH) – the more acidotic (lower pH), the more Bf
l Neuronal susceptibility (prematurity)
l Blood-brain barrier (BBB)???l Note: BBB keeps out bilirubin bound to albumin,
but there is NO a BBB to free bilirubin (Bf)
l Concentration of hydrogen ion (pH) – the more acidotic (lower pH), the more Bf
l Neuronal susceptibility (prematurity)
l Blood-brain barrier (BBB)???l Note: BBB keeps out bilirubin bound to albumin,
but there is NO a BBB to free bilirubin (Bf)
*Volpe,JJ, Neurology of the Newborn, 2001*Volpe,JJ, Neurology of the Newborn, 2001
More on bilirubin: BindingMore on bilirubin: BindingBound vs. unbound or “free” bilirubin
l >99.99% of bilirubin is bound to albumin in the blood
l Bilirubin bound to albumin does not move into brain - it does not cause brain damage.
Bound vs. unbound or “free” bilirubin
l >99.99% of bilirubin is bound to albumin in the blood
l Bilirubin bound to albumin does not move into brain - it does not cause brain damage.
Children’s MercyHOSPITALS & CLINICS
Kansas City
l The unbound or “free” bilirubin can move from blood into brain tissue and cause brain damage.
l The amount of “free” bilirubin determines brain damage.
l We DO NOT measure free billirubin clinically!!!
l We only measure total bilirubin.
l The unbound or “free” bilirubin can move from blood into brain tissue and cause brain damage.
l The amount of “free” bilirubin determines brain damage.
l We DO NOT measure free billirubin clinically!!!
l We only measure total bilirubin.
Unbound “free” Bilirubin (Bf) vs. Total Serum Bilirubin (TSB)
Unbound “free” Bilirubin (Bf) vs. Total Serum Bilirubin (TSB)
Free unbound bilirubin (UB aka Bf) predicts outcome better than total serum bilirubin (TSB)
� Odell etal, 1970. J Pediatr, 76:12.� Johnson and Boggs,1974. In Phototherapy in the
Newborn: An Overview, eds, Odell GB, Schaffer R, Sionpoulous AP
Free unbound bilirubin (UB aka Bf) predicts outcome better than total serum bilirubin (TSB)
� Odell etal, 1970. J Pediatr, 76:12.� Johnson and Boggs,1974. In Phototherapy in the
Newborn: An Overview, eds, Odell GB, Schaffer R, Sionpoulous AP
Children’s MercyHOSPITALS & CLINICS
Kansas City
Sionpoulous, AP.
UB predicts ABRs better than TSB� Nakamura etal, Pediatrics 75:703, 1985� Funato etal, Pediatrics 93:50, 1994.� Amin etal, Pediatrics 107:664, 2001.� Ahlfors and Shapiro, Biol Neonate, 80:158, 2001.
Sionpoulous, AP.
UB predicts ABRs better than TSB� Nakamura etal, Pediatrics 75:703, 1985� Funato etal, Pediatrics 93:50, 1994.� Amin etal, Pediatrics 107:664, 2001.� Ahlfors and Shapiro, Biol Neonate, 80:158, 2001.
More on bilirubin: why care about total bilirubin?
More on bilirubin: why care about total bilirubin?
� If free bilirubin causes brain damage, why care about “total bilirubin”, bilirubin bound to albumin in blood?
� Total bilirubin correlates with free bilirubin:� Higher total -> more saturated albumin -> more free
� If free bilirubin causes brain damage, why care about “total bilirubin”, bilirubin bound to albumin in blood?
� Total bilirubin correlates with free bilirubin:� Higher total -> more saturated albumin -> more free
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Higher total > more saturated albumin > more free
� Total bilirubin is all we can measure (actually, total bilirubin = unconjugated+conjugated bilirubin)
� Though total bilirubin is not perfect, the higher the total bilirubin, the more likely to have brain damage.
� The clinical evidence . . . . .
� Higher total > more saturated albumin > more free
� Total bilirubin is all we can measure (actually, total bilirubin = unconjugated+conjugated bilirubin)
� Though total bilirubin is not perfect, the higher the total bilirubin, the more likely to have brain damage.
� The clinical evidence . . . . .

10/29/12
4
Relation Between Maximum Serum Bilirubin Concentration and Kernicterus in Newborns
with Hemolytic Disease*
Relation Between Maximum Serum Bilirubin Concentration and Kernicterus in Newborns
with Hemolytic Disease*No definition or description of kernicterus!
Children’s MercyHOSPITALS & CLINICS
Kansas City
* From Maisels and data of Mollison PL and Cutbush M, Recent Advances in Pediatrics, 110-132, 1954
* From Maisels and data of Mollison PL and Cutbush M, Recent Advances in Pediatrics, 110-132, 1954
Bhutani Hour-Specific NomogramBhutani Hour-Specific Nomogram
This nomogram does not indicate risk of brain damage, but the risk of a high bilirubin (>17 mg/dl) in the future.
•Bhutani, Johnson, Sivieri, Pediatrics 103:6, 1999•Bhutani, Johnson, Sivieri, Pediatrics 103:6, 1999
High Risk Zone
Low Risk Zone
“1-day-old” Normal at 47 h“1-day-old” Normal at 47 his >95th% at 25his >95th% at 25h
2/6/2007front page
2/6/2007front page
Baby Has Jaundice: Is That a Problem?; Mom of Disabled Boy Pushes for Tests;
Debating Risk of Rare SyndromeRachel Zimmerman. Wall Street Journal. (Eastern edition). New York, N.Y.: Feb 6,
Children’s MercyHOSPITALS & CLINICS
Kansas City
2007. pg. A.1
Bhutani Hour-Specific NomogramBhutani Hour-Specific Nomogram
8%
33% Risk for Kernicterus with Rh Hemolytic Disease
0%
- Bhutani, Johnson, Sivieri, Pediatrics 103:6, 1999- Bhutani, Johnson, Sivieri, Pediatrics 103:6, 1999
Bhutani Hour-Specific Nomogram & Mollison
and Cutbush 1950
Bhutani Hour-Specific Nomogram & Mollison
and Cutbush 195030-40 mg/dL, 8/11 (73%)
25-29 mg/dL, 4/12 (33%)
19-24 mg/dL, 1/13 (8%)
Bilirubin
Children’s MercyHOSPITALS & CLINICS
Kansas City
Bhutani, Johnson, Sivieri, Pediatrics 103:6, 1999
10-18 mg/dL 0/24 (0%)Mollison and Cutbush, 1954
2006;117;474-485 Pediatrics
The wide spectrum of response to severe hyperbilirubinemia
*
• Newman etal Pediatrics 111:1303, 2003• Ahlfors and Herbsman Pediatrics 111:1110, 2003• Harris etal Pediatrics 107:1075, 2001.
10/29/12
5
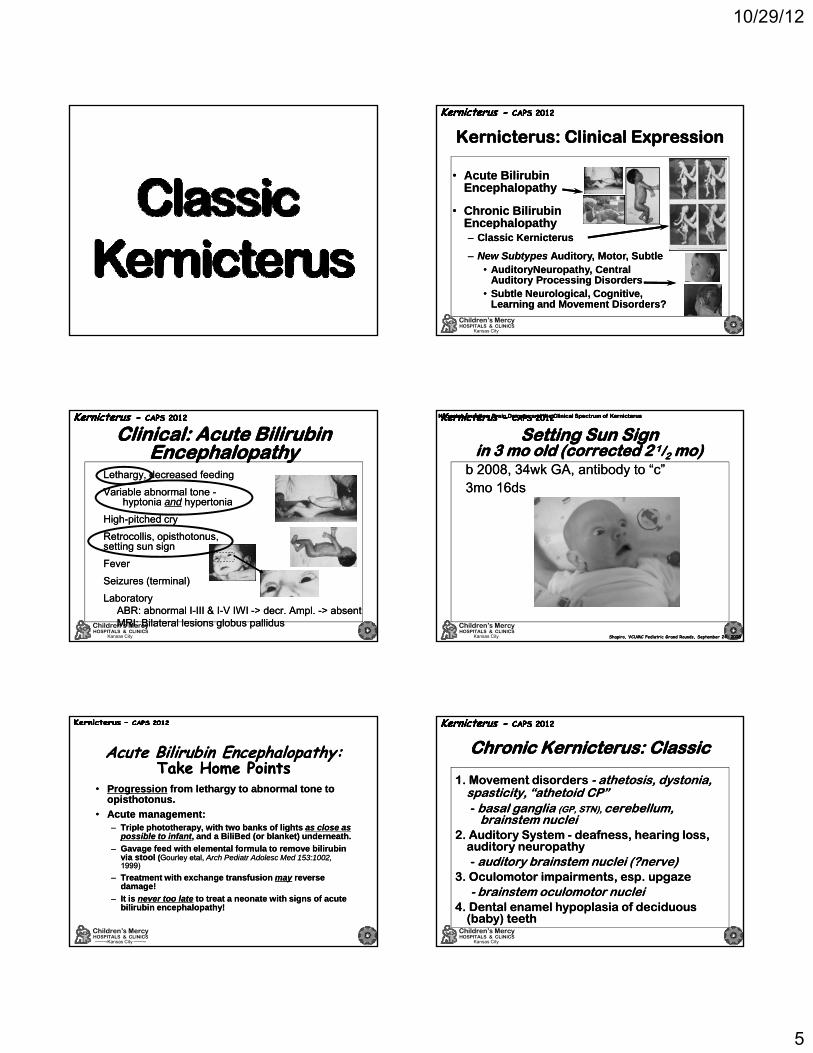
Kernicterus: Clinical ExpressionKernicterus: Clinical Expression
• Acute Bilirubin Encephalopathy
• Acute Bilirubin Encephalopathy
• Chronic Bilirubin Encephalopath
• Chronic Bilirubin Encephalopath
Children’s MercyHOSPITALS & CLINICS
Kansas City
Encephalopathy– Classic Kernicterus
Encephalopathy– Classic Kernicterus
– New Subtypes Auditory, Motor, Subtle• AuditoryNeuropathy, Central
Auditory Processing Disorders• Subtle Neurological, Cognitive,
Learning and Movement Disorders?
– New Subtypes Auditory, Motor, Subtle• AuditoryNeuropathy, Central
Auditory Processing Disorders• Subtle Neurological, Cognitive,
Learning and Movement Disorders?
Clinical: Acute Bilirubin Encephalopathy
Clinical: Acute Bilirubin Encephalopathy
� Lethargy, decreased feeding
� Variable abnormal tone -hyptonia and hypertonia
� High-pitched cry
� Lethargy, decreased feeding
� Variable abnormal tone -hyptonia and hypertonia
� High-pitched cry
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Retrocollis, opisthotonus, setting sun sign
� Fever
� Seizures (terminal)
� Laboratory� ABR: abnormal I-III & I-V IWI -> decr. Ampl. -> absent� MRI: Bilateral lesions globus pallidus
� Retrocollis, opisthotonus, setting sun sign
� Fever
� Seizures (terminal)
� Laboratory� ABR: abnormal I-III & I-V IWI -> decr. Ampl. -> absent� MRI: Bilateral lesions globus pallidus
Neonatal Jaundice, Brain Damage and the Clinical Spectrum of KernicterusNeonatal Jaundice, Brain Damage and the Clinical Spectrum of KernicterusNeonatal Jaundice, Brain Damage and the Clinical Spectrum of KernicterusNeonatal Jaundice, Brain Damage and the Clinical Spectrum of Kernicterus
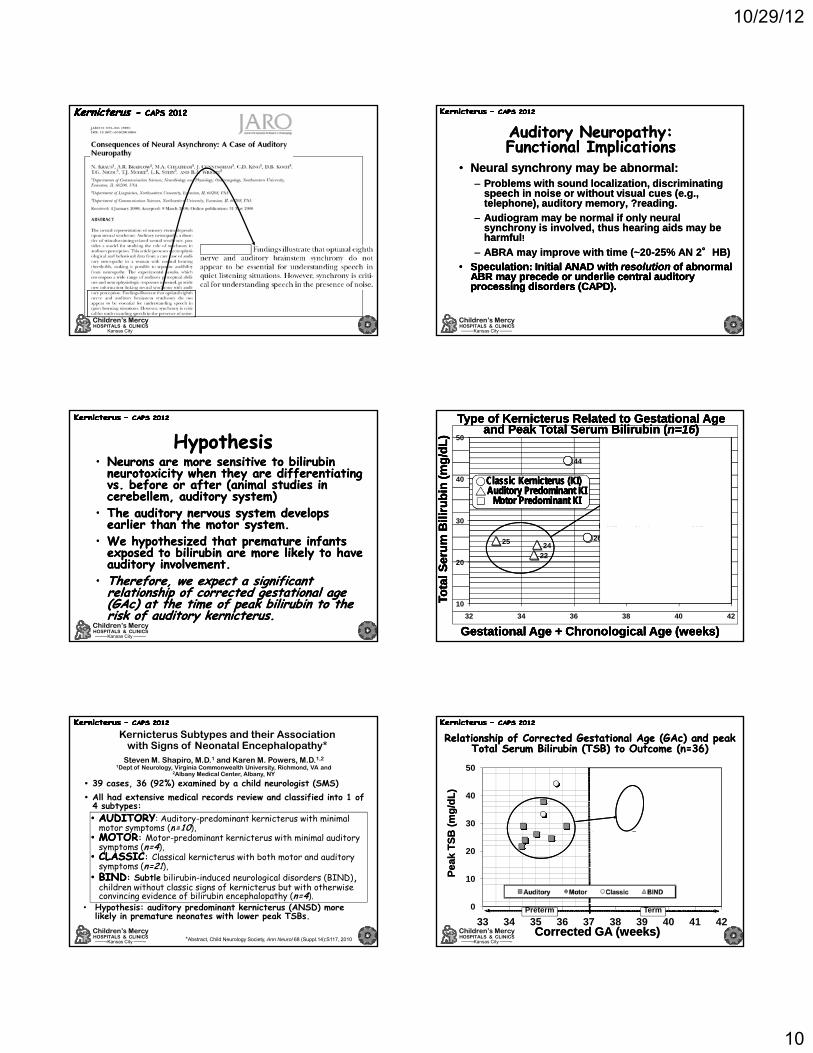
Setting Sun Sign in 3 mo old (corrected 2 1/2 mo)
Setting Sun Sign in 3 mo old (corrected 2 1/2 mo)
� b 2008, 34wk GA, antibody to “c”� 3mo 16ds� b 2008, 34wk GA, antibody to “c”� 3mo 16ds
Children’s MercyHOSPITALS & CLINICS
Kansas City Shapiro, VCUMC Pediatric Grand Rounds, September 24, 2008Shapiro, VCUMC Pediatric Grand Rounds, September 24, 2008
Acute Bilirubin Encephalopathy:Take Home Points
Acute Bilirubin Encephalopathy:Take Home Points
• Progression from lethargy to abnormal tone to opisthotonus.
• Acute management:– Triple phototherapy, with two banks of lights as close as
• Progression from lethargy to abnormal tone to opisthotonus.
• Acute management:– Triple phototherapy, with two banks of lights as close as
Children’s MercyHOSPITALS & CLINICS
Kansas City
p p py, gpossible to infant, and a BiliBed (or blanket) underneath.
– Gavage feed with elemental formula to remove bilirubin via stool (Gourley etal, Arch Pediatr Adolesc Med 153:1002,1999)
– Treatment with exchange transfusion may reverse damage!
– It is never too late to treat a neonate with signs of acute bilirubin encephalopathy!
p p py, gpossible to infant, and a BiliBed (or blanket) underneath.
– Gavage feed with elemental formula to remove bilirubin via stool (Gourley etal, Arch Pediatr Adolesc Med 153:1002,1999)
– Treatment with exchange transfusion may reverse damage!
– It is never too late to treat a neonate with signs of acute bilirubin encephalopathy!
Chronic Kernicterus: ClassicChronic Kernicterus: Classic
1. Movement disorders - athetosis, dystonia, spasticity, “athetoid CP”- basal ganglia (GP, STN), cerebellum,
brainstem nuclei2 A dit S t d f h i l
1. Movement disorders - athetosis, dystonia, spasticity, “athetoid CP”- basal ganglia (GP, STN), cerebellum,
brainstem nuclei2 A dit S t d f h i l
Children’s MercyHOSPITALS & CLINICS
Kansas City
2. Auditory System - deafness, hearing loss, auditory neuropathy- auditory brainstem nuclei (?nerve)
3. Oculomotor impairments, esp. upgaze- brainstem oculomotor nuclei
4. Dental enamel hypoplasia of deciduous (baby) teeth
2. Auditory System - deafness, hearing loss, auditory neuropathy- auditory brainstem nuclei (?nerve)
3. Oculomotor impairments, esp. upgaze- brainstem oculomotor nuclei
4. Dental enamel hypoplasia of deciduous (baby) teeth

10/29/12
6
Kernicterus: SelectivityKernicterus: SelectivitySelective yellow staining of:
� Basal ganglia, esp. globus pallidus� Auditory brainstem nuclei, esp. CN, IC,
SOC� Oculomotor nuclei, esp. nuclei
controlling upgaze� Vestibular nuclei� Cerebellum, esp. purkinje cells� Hippocampus - CA-2 sector, not CA-1 or
Selective yellow staining of:� Basal ganglia, esp. globus pallidus� Auditory brainstem nuclei, esp. CN, IC,
SOC� Oculomotor nuclei, esp. nuclei
controlling upgaze� Vestibular nuclei� Cerebellum, esp. purkinje cells� Hippocampus - CA-2 sector, not CA-1 or
Selective bilirubin staining in the hippocampusSelective bilirubin staining in the hippocampus
CA-2CA-2
- Barmada and Moossy , 1984- Barmada and Moossy , 1984
Selective bilirubin staining in brainstemSelective bilirubin staining in brainstem
� Hippocampus CA 2 sector, not CA 1 or CA-3 (?)
� Hippocampus CA 2 sector, not CA 1 or CA-3 (?)
Classic Kernicterus (cont.)Classic Kernicterus (cont.)
� Cortex = normal => normal intelligence, normal or superior mental function
� May be abnormal sensory integration and sensory motor impairments from involvement of the globus
llid th dit t d th b ll
� Cortex = normal => normal intelligence, normal or superior mental function
� May be abnormal sensory integration and sensory motor impairments from involvement of the globus
llid th dit t d th b ll
Children’s MercyHOSPITALS & CLINICS
Kansas City
pallidus, the auditory system and the cerebellum
� NOT Mentally Retarded!
Some are highly intelligent but trapped in immobile, dysfunctional bodies, deaf, can’t move, can’t sign, can’t type, can’t communicate . . . Locked in!
pallidus, the auditory system and the cerebellum
� NOT Mentally Retarded!
Some are highly intelligent but trapped in immobile, dysfunctional bodies, deaf, can’t move, can’t sign, can’t type, can’t communicate . . . Locked in!
Classic Kernicterus: Classic Kernicterus: Movement Movement disorder disorder Classic Kernicterus: Classic Kernicterus: Movement Movement disorder disorder
Larocche, 1966
Larocche, 1966
�� AthetosisAthetosis, , ““Athetoid Athetoid CPCP””
�� Dystonia Dystonia �� Hypotonia Hypotonia andand
hypertoniahypertonia�� Not spastic (unless Not spastic (unless
concurrent injury)concurrent injury)
�� AthetosisAthetosis, , ““Athetoid Athetoid CPCP””
�� Dystonia Dystonia �� Hypotonia Hypotonia andand
hypertoniahypertonia�� Not spastic (unless Not spastic (unless
concurrent injury)concurrent injury)
1min 18 sec
Children’s MercyHOSPITALS & CLINICS
Kansas City 33yo, Moderate Kernicterus from Rh disease33yo, Moderate Kernicterus from Rh disease
1min 30 sec
20 sec
Dental Dental enamel enamel dysplasiadysplasia of of primary (primary (““babybaby””))teethteeth
Dental Dental enamel enamel dysplasiadysplasia of of primary (primary (““babybaby””))teethteeth
Kernicterus: Kernicterus: Dental Enamel DysplasiaDental Enamel DysplasiaKernicterus: Kernicterus: Dental Enamel DysplasiaDental Enamel Dysplasia
Children’s MercyHOSPITALS & CLINICS
Kansas City
18 mo oldMRI at 5mo; T2
Where Kernicterus Damages Control of Movement and Tone
Where Kernicterus Damages Control of Movement and Tone
Can see on MRI: � damages globus pallidus
(GP) part of basal ganglia)
� different from HIE (thalamus and putamen, cerebral cortex
� leads to excessive mo ements incl ding
Can see on MRI: � damages globus pallidus
(GP) part of basal ganglia)
� different from HIE (thalamus and putamen, cerebral cortex
� leads to excessive mo ements incl ding
T1 early T2 late
Children’s MercyHOSPITALS & CLINICS
Kansas City
STNSTNGPGP
movements, including athetosis and dystoniamovements, including athetosis and dystonia
Cannot see on MRI: � Damages to cerebellar
Purkinje cell layer� Damages to brainstem
nuclei for posture, auditory, vestibular and oculomotor function
Cannot see on MRI: � Damages to cerebellar
Purkinje cell layer� Damages to brainstem
nuclei for posture, auditory, vestibular and oculomotor function
Kernicterus: AuditoryKernicterus: Auditory
Selective bilirubin staining in the brainstem
Selective bilirubin staining in the brainstem
BAEP Changes1. Mild, Reversible
BAEP Changes1. Mild, Reversible
Children’s MercyHOSPITALS & CLINICS
Kansas City
2. BAEPs may be absent.
Absent BAEPs and normal OAEs = Auditory Neuropathy
2. BAEPs may be absent.
Absent BAEPs and normal OAEs = Auditory Neuropathy
Nwaesei, etal, Nwaesei, etal, PediatricsPediatrics 800, 1984.800, 1984.Nwaesei, etal, Nwaesei, etal, PediatricsPediatrics 800, 1984.800, 1984.

10/29/12
7
Auditory Neuropathy -1996
Auditory Neuropathy -1996
Children’s MercyHOSPITALS & CLINICS
Kansas City
Now known as Auditory Neuropathy Spectrum Disorder (ANSD)
Auditory Neuropathy Spectrum Disorder(Auditory Dys-synchrony)
Auditory Neuropathy Spectrum Disorder(Auditory Dys-synchrony)
Functional Definition:Abnormal ABRs, Normal OAEs
� Normal Cochlea (Inner Ear):
N l OAE ( h i l i t it f i )
Functional Definition:Abnormal ABRs, Normal OAEs
� Normal Cochlea (Inner Ear):
N l OAE ( h i l i t it f i )
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Normal OAEs (mechanical integrity of inner ear)
� Normal CMs (outer hair cells of inner ear)
� Abnormal Auditory Pathway Function:
� Absent or Abnormal ABRs
� Described in Infants, ~1/2 reported cases have had very significant neonatal hyperbilirubinemia
� Normal OAEs (mechanical integrity of inner ear)
� Normal CMs (outer hair cells of inner ear)
� Abnormal Auditory Pathway Function:
� Absent or Abnormal ABRs
� Described in Infants, ~1/2 reported cases have had very significant neonatal hyperbilirubinemia
Peripheral vs. Central Auditory Systems
Peripheral vs. Central Auditory Systems
Peripheral Auditory SystemOuter Ear, Middle Ear, Inner Ear (hair cells)
Central Auditory
Peripheral Auditory SystemOuter Ear, Middle Ear, Inner Ear (hair cells)
Central Auditory
OuterOuterEarEar
MiddleMiddleEarEar
AuditoryAuditoryNerveNerve
InnerInnerEarEar
Children’s MercyHOSPITALS & CLINICS
Kansas City
Ce t a ud to ySystemAuditory Nerve, Brainstem, Thalamus (MG), Auditory Cortex (TL)
Ce t a ud to ySystemAuditory Nerve, Brainstem, Thalamus (MG), Auditory Cortex (TL)
Summary: Where Bilirubin Damages the Auditory System
Summary: Where Bilirubin Damages the Auditory System
� Thalamus, cerebral cortex - No!� Brainstem nuclei - YES!
� Cochlear nuclei� Superior olivary complex
Lateral lemnisci
� Thalamus, cerebral cortex - No!� Brainstem nuclei - YES!
� Cochlear nuclei� Superior olivary complex
Lateral lemnisci
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Lateral lemnisci� Trapezoid bodies� Inferior colliculi
� Auditory nerve and spiral ganglia - ?yes, ?at high levels of toxicity
� Inner ear hair cells - No!
� Lateral lemnisci� Trapezoid bodies� Inferior colliculi
� Auditory nerve and spiral ganglia - ?yes, ?at high levels of toxicity
� Inner ear hair cells - No!II
IIIIII
VV
OAEsOAEsCMCM
BDWBDW
Where Bilirubin Damages the Auditory System in Humans
Where Bilirubin Damages the Auditory System in Humans
Abnormal Abnormal
Children’s MercyHOSPITALS & CLINICS
Kansas City
ABRsABRs
Normal CM, (OAEs)Normal CM, (OAEs)
Where does Bilirubin Damage theAuditory System? Nerve? Brainstem-Yes!
Children’s MercyHOSPITALS & CLINICS
Kansas City
ABR
Binaural Interaction ABR

10/29/12
8
•.
Rance, G., et al., Clinical findings for a group of infants and young children with auditory neuropathy.
-Ear Hear 20:238, 1999.
20 infants� 12 of 5199 from an
early hearing loss
Rance, G., et al., Clinical findings for a group of infants and young children with auditory neuropathy.
-Ear Hear 20:238, 1999.
20 infants� 12 of 5199 from an
early hearing loss
59 mg/dl46 mg/dl27 mg/dl 25 mg/dl22 mg/dl
21 mg/dl *
Children’s MercyHOSPITALS & CLINICS
Kansas City
early hearing loss identification program with high rish neonatal or family histories.
Est. 1/433 newborns at risk for hearing loss have AN
� 8 referred
~1/2 (10/20, 10/16 with etiology) had jaundice as risk factor
early hearing loss identification program with high rish neonatal or family histories.
Est. 1/433 newborns at risk for hearing loss have AN
� 8 referred
~1/2 (10/20, 10/16 with etiology) had jaundice as risk factor
32 mg/dl28 mg/dl *25 mg/dl23 mg/dl *
Berlin et.al. 2003, 260 ptswith ANSD
Berlin et.al. 2003, 260 ptswith ANSD
• 49% due to hyperbilirubinemia– 20% had exchange transfusions– 48% premature– Other: otoxic drugs 29%, ventilator 20%, FH+
• 49% due to hyperbilirubinemia– 20% had exchange transfusions– 48% premature– Other: otoxic drugs 29%, ventilator 20%, FH+
Children’s MercyHOSPITALS & CLINICS
Kansas City
g , ,8%; genetic 16%, 6 with mitochondrial disorders
– 13 with CP; 3 with kernicterus• Improvement in speech & language with:
– No treatment: 5%– Hearing Aids: 15% – Cochlear Implants: 85% improvement
g , ,8%; genetic 16%, 6 with mitochondrial disorders
– 13 with CP; 3 with kernicterus• Improvement in speech & language with:
– No treatment: 5%– Hearing Aids: 15% – Cochlear Implants: 85% improvement
. J Audiol 49, 30-43, 2010
ANAD risk incr 10x with BW <1,000g, 5/100 ANAD, 5/100 SNHL
ANAD risk incr 10x with BW <1,000g, 5/100 ANAD, 5/100 SNHL
Children’s MercyHOSPITALS & CLINICS
Kansas City
Children’s MercyHOSPITALS & CLINICS
Kansas City
J Perinatology 25:54, 2005
Kernicterus - SeverityKernicterus - SeverityAcute
Subacute
ChronicSeve
rity
Children’s MercyHOSPITALS & CLINICS
Kansas City
Shapiro, Seminars in Fetal and Neonatal Medicine 15:157, 2010

10/29/12
9
Severe KernicterusSevere Kernicterus
Auditory Predominant KernicterusAuditory Predominant KernicterusAuditory Predominant KernicterusAuditory Predominant Kernicterus
�� B. B. 20012001, 34wk GA, BW , 34wk GA, BW 3174g, 3174g, ApgApg 8/9, A+, 8/9, A+,
Coombs Coombs --�� Absent/Abnormal ABR, Absent/Abnormal ABR,
Acts DeafActs Deaf
�� B. B. 20012001, 34wk GA, BW , 34wk GA, BW 3174g, 3174g, ApgApg 8/9, A+, 8/9, A+,
Coombs Coombs --�� Absent/Abnormal ABR, Absent/Abnormal ABR,
Acts DeafActs Deaf
Children’s MercyHOSPITALS & CLINICS
Kansas City
HypotoniaHypotonia�� Rx: Cochlear ImplantRx: Cochlear Implant
HypotoniaHypotonia�� Rx: Cochlear ImplantRx: Cochlear Implant
15 months15 months15 months15 months
phototherapy
� 1yo male, 34 wk GA, Apg 8/9, AO blood incompat, peak TSB 24.0@4days, photoRx, no X∆
� Failed ABR screen & subsequent ABRs
� 1yo male, 34 wk GA, Apg 8/9, AO blood incompat, peak TSB 24.0@4days, photoRx, no X∆
� Failed ABR screen & subsequent ABRs
Auditory neuropathy + mild motor delay
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Diagnosis: Auditory Neuropathy
� Exam: minimal hypotonia andgross motor delay, hearing impaired, strabismus, upgazeparalysis, dental enamel dysplasia
� Rx: Cochlear implant!
� Diagnosis: Auditory Neuropathy
� Exam: minimal hypotonia andgross motor delay, hearing impaired, strabismus, upgazeparalysis, dental enamel dysplasia
� Rx: Cochlear implant!
Auditory Predominant Auditory Predominant Kernicterus (Kernicterus (Auditory Neuropathy) & occasional muscle cramps
Auditory Predominant Auditory Predominant Kernicterus (Kernicterus (Auditory Neuropathy) & occasional muscle cramps
� b. 1998, 38 wk GA, 2720 g, Apg 7/9
� A-/O+, Rh disease Coombs +
� X∆ transfusion
� b. 1998, 38 wk GA, 2720 g, Apg 7/9
� A-/O+, Rh disease Coombs +
� X∆ transfusion
Children’s MercyHOSPITALS & CLINICS
Kansas City
� Sequelae:� ABR absent -> Abnl� hearing loss and auditory
neuropathy, � dental enamel hypoplasia, � Hyperactive, ?ADHD� muscle cramps
responsive to benzo
� Sequelae:� ABR absent -> Abnl� hearing loss and auditory
neuropathy, � dental enamel hypoplasia, � Hyperactive, ?ADHD� muscle cramps
responsive to benzo
4 years old4 years old
AN/AD SimulationsAN/AD Simulations
Children’s MercyHOSPITALS & CLINICS
Kansas City http://www.ucihs.uci.edu/com/hesp/newversion/procSim/simulations.htm
Simulation 1: From “Original” to “Profound”
Simulation 2: From "Profound" to "Original"
Simulation 1: From “Original” to “Profound”
Simulation 2: From "Profound" to "Original"
10/29/12
10
Children’s MercyHOSPITALS & CLINICS
Kansas City
Auditory Neuropathy:Functional ImplicationsAuditory Neuropathy:Functional Implications
• Neural synchrony may be abnormal:– Problems with sound localization, discriminating
speech in noise or without visual cues (e.g., telephone), auditory memory, ?reading.
– Audiogram may be normal if only neural
• Neural synchrony may be abnormal:– Problems with sound localization, discriminating
speech in noise or without visual cues (e.g., telephone), auditory memory, ?reading.
– Audiogram may be normal if only neural
Children’s MercyHOSPITALS & CLINICS
Kansas City
Audiogram may be normal if only neural synchrony is involved, thus hearing aids may be harmful!
– ABRA may improve with time (~20-25% AN 2°HB)
•• Speculation: Initial ANAD with Speculation: Initial ANAD with resolutionresolution of abnormal of abnormal ABR may precede or underlie central auditory ABR may precede or underlie central auditory processing disorders (CAPD).processing disorders (CAPD).
Audiogram may be normal if only neural synchrony is involved, thus hearing aids may be harmful!
– ABRA may improve with time (~20-25% AN 2°HB)
•• Speculation: Initial ANAD with Speculation: Initial ANAD with resolutionresolution of abnormal of abnormal ABR may precede or underlie central auditory ABR may precede or underlie central auditory processing disorders (CAPD).processing disorders (CAPD).
HypothesisHypothesis• Neurons are more sensitive to bilirubin
neurotoxicity when they are differentiating vs. before or after (animal studies in cerebellem, auditory system)
• The auditory nervous system develops earlier than the motor system
• Neurons are more sensitive to bilirubin neurotoxicity when they are differentiating vs. before or after (animal studies in cerebellem, auditory system)
• The auditory nervous system develops earlier than the motor system
Children’s MercyHOSPITALS & CLINICS
Kansas City
earlier than the motor system.• We hypothesized that premature infants
exposed to bilirubin are more likely to have auditory involvement.
• Therefore, we expect a significant relationship of corrected gestational age (GAc) at the time of peak bilirubin to the risk of auditory kernicterus.
earlier than the motor system.• We hypothesized that premature infants
exposed to bilirubin are more likely to have auditory involvement.
• Therefore, we expect a significant relationship of corrected gestational age (GAc) at the time of peak bilirubin to the risk of auditory kernicterus.
46
29 2931
35
41
44
4039
46
30
40
50B
iliru
bin
(m
g/
Bili
rub
in (
mg
/dL
)d
L)
Bili
rub
in (
mg
/B
iliru
bin
(m
g/d
L)
dL
)
ClassicClassic KernicterusKernicterus (KI)(KI)Auditory Predominant KIAuditory Predominant KI
Motor Predominant KIMotor Predominant KI
ClassicClassic KernicterusKernicterus (KI)(KI)Auditory Predominant KIAuditory Predominant KI
Motor Predominant KIMotor Predominant KI
Type of Kernicterus Related Type of Kernicterus Related to Gestational Age to Gestational Age and Peak Total Serum and Peak Total Serum Bilirubin (Bilirubin (n=16n=16))
Type of Kernicterus Related Type of Kernicterus Related to Gestational Age to Gestational Age and Peak Total Serum and Peak Total Serum Bilirubin (Bilirubin (n=16n=16))
26
29 9
2224
25
21
28
10
20
32 34 36 38 40 42
Gestational Gestational Age + Chronological Age Age + Chronological Age (weeks)(weeks)Gestational Gestational Age + Chronological Age Age + Chronological Age (weeks)(weeks)
Tota
l Ser
um
BTo
tal S
eru
m B
Tota
l Ser
um
BTo
tal S
eru
m B
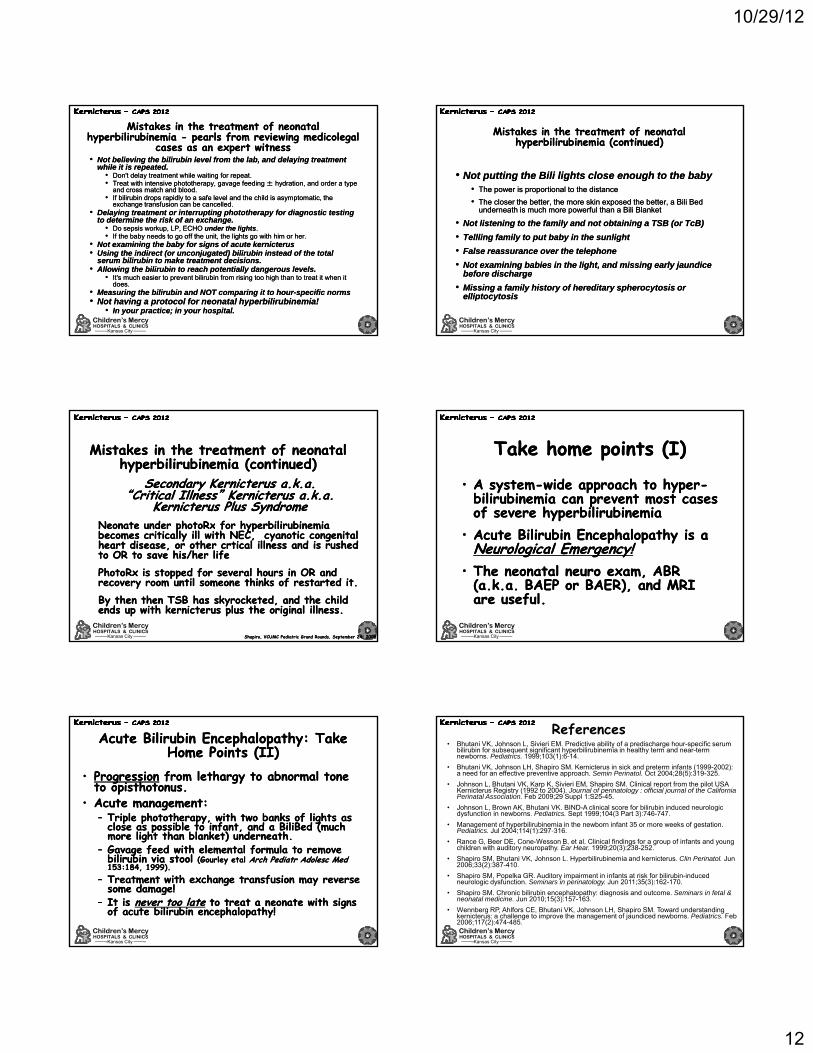
Steven M. Shapiro, M.D.1 and Karen M. Powers, M.D.1,21Dept of Neurology, Virginia Commonwealth University, Richmond, VA and
2Albany Medical Center, Albany, NY
Kernicterus Subtypes and their Association with Signs of Neonatal Encephalopathy*
• 39 cases, 36 (92%) examined by a child neurologist (SMS)• All had extensive medical records review and classified into 1 of
4 subtypes:•• AUDITORYAUDITORY: Auditory-predominant kernicterus with minimal
motor symptoms (n=10),
Children’s MercyHOSPITALS & CLINICS
Kansas City
y p ( ),•• MOTORMOTOR: Motor-predominant kernicterus with minimal auditory
symptoms (n=4),•• CLASSICCLASSIC: Classical kernicterus with both motor and auditory
symptoms (n=21), •• BINDBIND: Subtle bilirubin-induced neurological disorders (BIND),
children without classic signs of kernicterus but with otherwise convincing evidence of bilirubin encephalopathy (n=4).
• Hypothesis: auditory predominant kernicterus (ANSD) more likely in premature neonates with lower peak TSBs.
*Abstract, Child Neurology Society, Ann Neurol 68 (Suppl.14):S117, 2010
Relationship of Corrected Gestational Age (GAc) and peak Total Serum Bilirubin (TSB) to Outcome (n=36)
Relationship of Corrected Gestational Age (GAc) and peak Total Serum Bilirubin (TSB) to Outcome (n=36)
30
40
50
B (
mg
/dL
)B
(m
g/d
L)
Children’s MercyHOSPITALS & CLINICS
Kansas City
0
10
20
33 34 35 36 37 38 39 40 41 42
Auditory Motor Classic BIND
Pea
k T
SB
Pea
k T
SB
Corrected GA (weeks)Corrected GA (weeks)
Preterm Term

10/29/12
11
38
40
week
s)we
eks)
** ***
* = p < 0.05 vs. Auditory** = p < 0.01 vs. Auditory
Corrected Gestational Age (GAc)Mean ± SEM
Corrected Gestational Age (GAc)Mean ± SEM
Children’s MercyHOSPITALS & CLINICS
Kansas City
34
36
Auditory Classical Motor BIND
Kernicterus GroupKernicterus Group
GAGAcc(w(w
Children’s MercyHOSPITALS & CLINICS
Kansas City
Children’s MercyHOSPITALS & CLINICS
Kansas City
Steven M. Shapiro, M.D.1 and Karen M. Powers, M.D.1,21Dept of Neurology, Virginia Commonwealth University, Richmond, VA and 2Albany Medical Center, Albany, NY
Kernicterus Subtypes and their Association with Signs of Neonatal Encephalopathy
Infants with hyperbilirubinemia who develop with Auditory Predominant Kernicterus are more likely to have had no symptoms in the newborn period (50% auditory vs. 19% with classic kernicterus who have no symptoms, Chi square p < 0.005)
60%
% with NO neonatal symptoms
Children’s MercyHOSPITALS & CLINICS
Kansas City
0%
20%
40%
60%
Auditory Classical
**Chi square p < 0.005
5 of 5 4 of 21
50%
19%
Conclusions: Subtype differences in GA of exposure to bilirubin
Conclusions: Subtype differences in GA of exposure to bilirubin
Results support our hypotheses that:• The pattern of bilirubin-induced neurological damage
is neurodevelopmentally dependent. • Earlier GA at time of peak TSB suggests premature
neonates are more likely to develop auditory-predominant kernicterus, i.e., ANSD.
Results support our hypotheses that:• The pattern of bilirubin-induced neurological damage
is neurodevelopmentally dependent. • Earlier GA at time of peak TSB suggests premature
neonates are more likely to develop auditory-predominant kernicterus, i.e., ANSD.
Children’s MercyHOSPITALS & CLINICS
Kansas City
p , ,• Higher TSB in classic kernicterus vs. auditory-
predominant and BIND suggests that higher peak TSB causes more severe or widespread sequelae(Interesting that TSB predictive, but biased sample, all subjects had kernicterus).
• Half of infants who develop auditory (ANSD) kernicterus are likely to have had no neurological symptoms in the newborn period.
p , ,• Higher TSB in classic kernicterus vs. auditory-
predominant and BIND suggests that higher peak TSB causes more severe or widespread sequelae(Interesting that TSB predictive, but biased sample, all subjects had kernicterus).
• Half of infants who develop auditory (ANSD) kernicterus are likely to have had no neurological symptoms in the newborn period.
Is neonatal hyperbilirubinemia the cause of a neurodevelopmental disorder (NDD)?
Is neonatal hyperbilirubinemia the cause of a neurodevelopmental disorder (NDD)?History
� Excessively high bilirubin� Minimum: bilirubin > phototherapy level (15-20 mg/dl)* � Stronger evidence: bilirubin > exchange level (20-25 mg/dl)*� Consider other risk factors, (duration, prematurity, sick, pH, Rh)
� Neurological symptoms at time bilirubin high (tone, cry, posturing, eye movements)
E
History� Excessively high bilirubin
� Minimum: bilirubin > phototherapy level (15-20 mg/dl)* � Stronger evidence: bilirubin > exchange level (20-25 mg/dl)*� Consider other risk factors, (duration, prematurity, sick, pH, Rh)
� Neurological symptoms at time bilirubin high (tone, cry, posturing, eye movements)
E
Children’s MercyHOSPITALS & CLINICS
Kansas City
Exam� Abnormal tone, movements (dysonia, athetosis, incoord)� Hearing impairment, understanding speech in noise, on the
telephone, sound localization, � Abnl eye movemnts, esp. lack of upward gaze (may resolve)� Dental enamel dysplasia (staining/flaking of baby teeth)
Laboratory - specific ABR (BAEP) and MRI findings:� ABR (BAEP) absent or abnormal c/w AN/AD� MRI abnormal globus pallidus ± subthalamic nucleus (T1
hyperintensity early, T2 hyperintensity later)Absent other etiologies (but may be concurrent)
*per AAP Guidelines 2004
Exam� Abnormal tone, movements (dysonia, athetosis, incoord)� Hearing impairment, understanding speech in noise, on the
telephone, sound localization, � Abnl eye movemnts, esp. lack of upward gaze (may resolve)� Dental enamel dysplasia (staining/flaking of baby teeth)
Laboratory - specific ABR (BAEP) and MRI findings:� ABR (BAEP) absent or abnormal c/w AN/AD� MRI abnormal globus pallidus ± subthalamic nucleus (T1
hyperintensity early, T2 hyperintensity later)Absent other etiologies (but may be concurrent)
*per AAP Guidelines 2004
Shapiro, Seminars in Fetal and Neonatal Medicine 15:157, 2010
10/29/12
12
Mistakes in the treatment of neonatal hyperbilirubinemia - pearls from reviewing medicolegal
cases as an expert witness
Mistakes in the treatment of neonatal hyperbilirubinemia - pearls from reviewing medicolegal
cases as an expert witness• Not believing the bilirubin level from the lab, and delaying treatment
while it is repeated.• Don't delay treatment while waiting for repeat.• Treat with intensive phototherapy, gavage feeding ± hydration, and order a type
and cross match and blood. • If bilirubin drops rapidly to a safe level and the child is asymptomatic, the
exchange transfusion can be cancelled.• Delaying treatment or interrupting phototherapy for diagnostic testing
to determine the risk of an exchange
• Not believing the bilirubin level from the lab, and delaying treatment while it is repeated.
• Don't delay treatment while waiting for repeat.• Treat with intensive phototherapy, gavage feeding ± hydration, and order a type
and cross match and blood. • If bilirubin drops rapidly to a safe level and the child is asymptomatic, the
exchange transfusion can be cancelled.• Delaying treatment or interrupting phototherapy for diagnostic testing
to determine the risk of an exchange
Children’s MercyHOSPITALS & CLINICS
Kansas City
to determine the risk of an exchange.• Do sepsis workup, LP, ECHO under the lights. • If the baby needs to go off the unit, the lights go with him or her.
• Not examining the baby for signs of acute kernicterus• Using the indirect (or unconjugated) bilirubin instead of the total
serum bilirubin to make treatment decisions.• Allowing the bilirubin to reach potentially dangerous levels.
• It's much easier to prevent bilirubin from rising too high than to treat it when it does.
• Measuring the bilirubin and NOT comparing it to hour-specific norms• Not having a protocol for neonatal hyperbilirubinemia!
• In your practice; in your hospital.
to determine the risk of an exchange.• Do sepsis workup, LP, ECHO under the lights. • If the baby needs to go off the unit, the lights go with him or her.
• Not examining the baby for signs of acute kernicterus• Using the indirect (or unconjugated) bilirubin instead of the total
serum bilirubin to make treatment decisions.• Allowing the bilirubin to reach potentially dangerous levels.
• It's much easier to prevent bilirubin from rising too high than to treat it when it does.
• Measuring the bilirubin and NOT comparing it to hour-specific norms• Not having a protocol for neonatal hyperbilirubinemia!
• In your practice; in your hospital.
Mistakes in the treatment of neonatal hyperbilirubinemia (continued)
Mistakes in the treatment of neonatal hyperbilirubinemia (continued)
• Not putting the Bili lights close enough to the baby• The power is proportional to the distance
• The closer the better, the more skin exposed the better, a Bili Bed underneath is much more powerful than a Bili Blanket
N t li t i t th f il d t bt i i TSB ( T B)
• Not putting the Bili lights close enough to the baby• The power is proportional to the distance
• The closer the better, the more skin exposed the better, a Bili Bed underneath is much more powerful than a Bili Blanket
N t li t i t th f il d t bt i i TSB ( T B)
Children’s MercyHOSPITALS & CLINICS
Kansas City
• Not listening to the family and not obtaining a TSB (or TcB)
• Tellling family to put baby in the sunlight
• False reassurance over the telephone
• Not examining babies in the light, and missing early jaundice before discharge
• Missing a family history of hereditary spherocytosis or elliptocytosis
• Not listening to the family and not obtaining a TSB (or TcB)
• Tellling family to put baby in the sunlight
• False reassurance over the telephone
• Not examining babies in the light, and missing early jaundice before discharge
• Missing a family history of hereditary spherocytosis or elliptocytosis
Mistakes in the treatment of neonatal hyperbilirubinemia (continued)
Mistakes in the treatment of neonatal hyperbilirubinemia (continued)
Secondary Kernicterus a.k.a.“Critical Illness” Kernicterus a.k.a.
Kernicterus Plus SyndromeNeonate under photoRx for hyperbilirubinemia
Secondary Kernicterus a.k.a.“Critical Illness” Kernicterus a.k.a.
Kernicterus Plus SyndromeNeonate under photoRx for hyperbilirubinemia
Children’s MercyHOSPITALS & CLINICS
Kansas City Shapiro, VCUMC Pediatric Grand Rounds, September 24, 2008Shapiro, VCUMC Pediatric Grand Rounds, September 24, 2008
Neonate under photoRx for hyperbilirubinemia becomes critically ill with NEC, cyanotic congenital heart disease, or other crtical illness and is rushed to OR to save his/her lifePhotoRx is stopped for several hours in OR and recovery room until someone thinks of restarted it. By then then TSB has skyrocketed, and the child ends up with kernicterus plus the original illness.
Neonate under photoRx for hyperbilirubinemia becomes critically ill with NEC, cyanotic congenital heart disease, or other crtical illness and is rushed to OR to save his/her lifePhotoRx is stopped for several hours in OR and recovery room until someone thinks of restarted it. By then then TSB has skyrocketed, and the child ends up with kernicterus plus the original illness.
Take home points (I)Take home points (I)
• A system-wide approach to hyper-bilirubinemia can prevent most cases of severe hyperbilirubinemia
• A system-wide approach to hyper-bilirubinemia can prevent most cases of severe hyperbilirubinemia
Children’s MercyHOSPITALS & CLINICS
Kansas City
• Acute Bilirubin Encephalopathy is a Neurological Emergency!
• The neonatal neuro exam, ABR (a.k.a. BAEP or BAER), and MRI are useful.
• Acute Bilirubin Encephalopathy is a Neurological Emergency!
• The neonatal neuro exam, ABR (a.k.a. BAEP or BAER), and MRI are useful.
Acute Bilirubin Encephalopathy: Take Home Points (II)
Acute Bilirubin Encephalopathy: Take Home Points (II)
• Progression from lethargy to abnormal tone to opisthotonus.
• Acute management:– Triple phototherapy, with two banks of lights as
close as possible to infant, and a BiliBed (much l h h l k ) d h
• Progression from lethargy to abnormal tone to opisthotonus.
• Acute management:– Triple phototherapy, with two banks of lights as
close as possible to infant, and a BiliBed (much l h h l k ) d h
Children’s MercyHOSPITALS & CLINICS
Kansas City
p , (more light than blanket) underneath.
– Gavage feed with elemental formula to remove bilirubin via stool (Gourley etal Arch Pediatr Adolesc Med153:184, 1999).
– Treatment with exchange transfusion may reverse some damage!
– It is never too late to treat a neonate with signs of acute bilirubin encephalopathy!
p , (more light than blanket) underneath.
– Gavage feed with elemental formula to remove bilirubin via stool (Gourley etal Arch Pediatr Adolesc Med153:184, 1999).
– Treatment with exchange transfusion may reverse some damage!
– It is never too late to treat a neonate with signs of acute bilirubin encephalopathy!
• Bhutani VK, Johnson L, Sivieri EM. Predictive ability of a predischarge hour-specific serum bilirubin for subsequent significant hyperbilirubinemia in healthy term and near-term newborns. Pediatrics. 1999;103(1):6-14.
• Bhutani VK, Johnson LH, Shapiro SM. Kernicterus in sick and preterm infants (1999-2002): a need for an effective preventive approach. Semin Perinatol. Oct 2004;28(5):319-325.
• Johnson L, Bhutani VK, Karp K, Sivieri EM, Shapiro SM. Clinical report from the pilot USA Kernicterus Registry (1992 to 2004). Journal of perinatology : official journal of the California Perinatal Association. Feb 2009;29 Suppl 1:S25-45.
• Johnson L, Brown AK, Bhutani VK. BIND-A clinical score for bilirubin induced neurologic dysfunction in newborns. Pediatrics. Sept 1999;104(3 Part 3):746-747.
• Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics Jul 2004;114(1):297-316
References
Children’s MercyHOSPITALS & CLINICS
Kansas City
Pediatrics. Jul 2004;114(1):297 316.
• Rance G, Beer DE, Cone-Wesson B, et al. Clinical findings for a group of infants and young children with auditory neuropathy. Ear Hear. 1999;20(3):238-252.
• Shapiro SM, Bhutani VK, Johnson L. Hyperbilirubinemia and kernicterus. Clin Perinatol. Jun 2006;33(2):387-410.
• Shapiro SM, Popelka GR. Auditory impairment in infants at risk for bilirubin-induced neurologic dysfunction. Seminars in perinatology. Jun 2011;35(3):162-170.
• Shapiro SM. Chronic bilirubin encephalopathy: diagnosis and outcome. Seminars in fetal & neonatal medicine. Jun 2010;15(3):157-163.
• Wennberg RP, Ahlfors CE, Bhutani VK, Johnson LH, Shapiro SM. Toward understanding kernicterus: a challenge to improve the management of jaundiced newborns. Pediatrics. Feb 2006;117(2):474-485.

10/29/12
13
Children’s MercyHOSPITALS & CLINICS
Kansas City
Steven M. Shapiro, MDSteven M. Shapiro, MDsshapirosshapiro@@cmh.educmh.edu
Steven M. Shapiro, MDSteven M. Shapiro, MDsshapirosshapiro@@cmh.educmh.edu
www.kernicterus.orgwww.kernicterus.orgwww.newbornjaundice.orgwww.newbornjaundice.org
www.kernicterus.orgwww.kernicterus.orgwww.newbornjaundice.orgwww.newbornjaundice.org


















