2018 HTRC Irvine Brachial Plexus Barrett - ASHT · Dermatomes vs. Cutaneous Innervation Axillary C5...
17
Hand Therapy Review Course UC Irvine February 9, 2018 Brachial Plexus & Nerve Innervation of the Upper Extremity Nora Barrett, MS, OTR/L, CHT Objectives Brief review of normal and compromised neuroanatomy Brachial plexus anatomy Spinal nerves: pathways, classic lesions, and compression sites Brief review of normal and compromised neuroanatomy Brachial plexus anatomy Spinal nerves: pathways, classic lesions, and compression sites Neuroanatomy Central Nervous System Inside brain and spinal cord Peripheral Nervous System Outside brain and spinal cord CNS & PNS work together as continuum from cortex to motor and sensory end organs PNS injury—> affects cortical level Large cortical representation of hand Neural change in hand—> change in cortex
Transcript of 2018 HTRC Irvine Brachial Plexus Barrett - ASHT · Dermatomes vs. Cutaneous Innervation Axillary C5...

Hand Therapy Review CourseUC Irvine
February 9, 2018
Brachial Plexus & Nerve Innervation of the Upper Extremity
Nora Barrett, MS, OTR/L, CHT
Objectives
Brief review of normal and compromised neuroanatomy
Brachial plexus anatomy
Spinal nerves: pathways, classic lesions, and compression sites
Brief review of normal and compromised neuroanatomy
Brachial plexus anatomy
Spinal nerves: pathways, classic lesions, and compression sites
NeuroanatomyCentral Nervous System Inside brain and spinal cord
Peripheral Nervous SystemOutside brain and spinal cord
CNS & PNS work together as continuum from cortex to motor and sensory end organs
PNS injury—> affects cortical level Large cortical representation of
hand Neural change in hand—> change
in cortex

Peripheral Nerve Anatomy: Connective Tissue
Epineurium-binds fascicles into named nerve
Perineurium-surrounds fascicles
Endoneurium-surrounds the axon
Connective tissue Protection vs.
compression, traction
Allows lengthening
Provides nutrition
Connective Tissue In vulnerable areas of the
body such as anatomic tunnels there are usually more fascicles in the nerves
Fascicle arrangement more complex proximally Jabaley: protection from compression, tensile forces
More fascicles means more epineurium to protect axons from friction or pressure Sunderland: 21-81% CT, >% closer to joint
Connective Tissue
Greater fasiculi: greater connective tissue protection:less deformation with mechanical stress
Connective Tissue Undulations of the nerves allow for more
nerve gliding without tension “Spiral bands of Fontana” Dellon & MacKinnon: absent in area of compression
Normal muscle tone helps prevent excessive traction to the nerve
Nerve TractionUndulation Stretched
Progressive Disruption• Axon• Endoneurium• Perineurium• Epineurium
The elastic limit of a nerve is thought to be about 20%
Nerve Injury
Agents of nerve injury are mechanical, thermal, chemical, or ischemic
Motor loss results in venous/lymphatic stasis; muscle atrophy; muscle/joint fibrosis
Sensory loss results in decreased functional use and increased risk for burn/pressure injury
Sympathetic loss results in vasomotor, sudomotor, pilomotor, and trophic changes
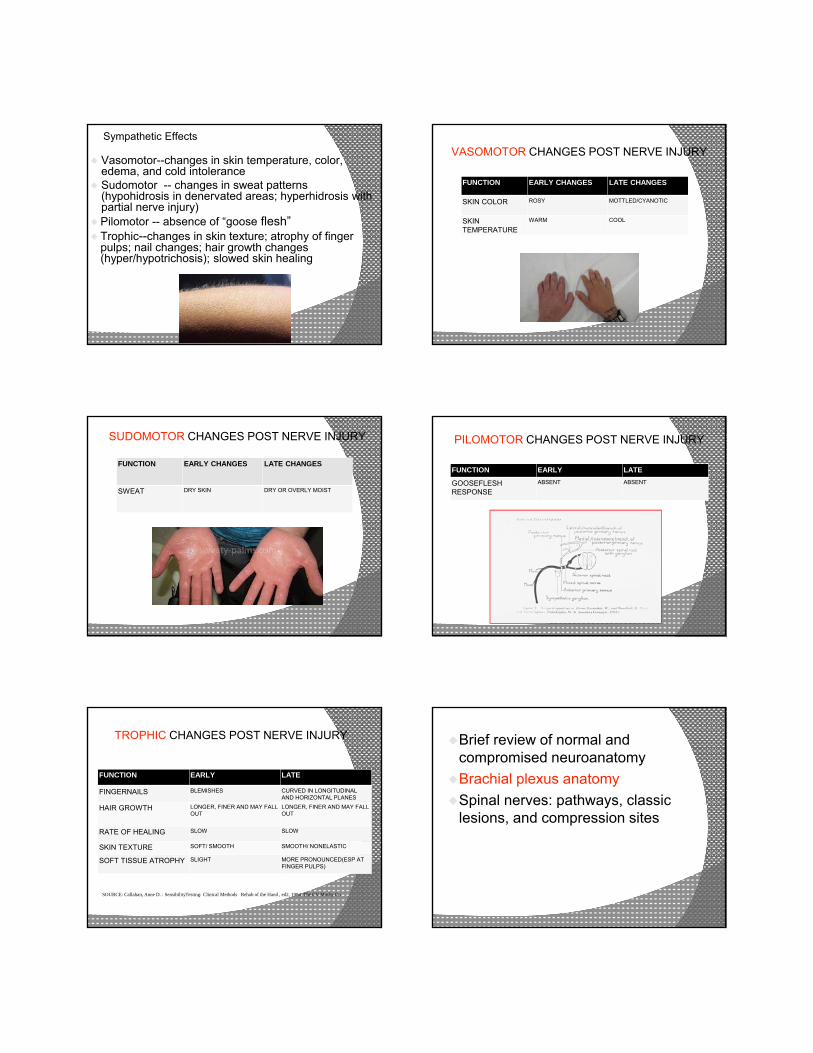
Sympathetic Effects
Vasomotor--changes in skin temperature, color, edema, and cold intolerance
Sudomotor -- changes in sweat patterns (hypohidrosis in denervated areas; hyperhidrosis with partial nerve injury)
Pilomotor -- absence of “goose flesh” Trophic--changes in skin texture; atrophy of finger
pulps; nail changes; hair growth changes (hyper/hypotrichosis); slowed skin healing
VASOMOTOR CHANGES POST NERVE INJURY
FUNCTION EARLY CHANGES LATE CHANGES
SKIN COLOR ROSY MOTTLED/CYANOTIC
SKIN TEMPERATURE
WARM COOL
SUDOMOTOR CHANGES POST NERVE INJURY
FUNCTION EARLY CHANGES LATE CHANGES
SWEAT DRY SKIN DRY OR OVERLY MOIST
PILOMOTOR CHANGES POST NERVE INJURY
FUNCTION EARLY LATE
GOOSEFLESH RESPONSE
ABSENT ABSENT
TROPHIC CHANGES POST NERVE INJURY
FUNCTION EARLY LATE
FINGERNAILS BLEMISHES CURVED IN LONGITUDINAL AND HORIZONTAL PLANES
HAIR GROWTH LONGER, FINER AND MAY FALL OUT
LONGER, FINER AND MAY FALL OUT
RATE OF HEALING SLOW SLOW
SKIN TEXTURE SOFT/ SMOOTH SMOOTH/ NONELASTIC
SOFT TISSUE ATROPHY SLIGHT MORE PRONOUNCED(ESP AT FINGER PULPS)
SOURCE: Callahan, Anne D. : SensibilityTesting: Clinical Methods Rehab of the Hand , ed2, 1984 The CV Mosby Co.
Brief review of normal and compromised neuroanatomy
Brachial plexus anatomy
Spinal nerves: pathways, classic lesions, and compression sites

Anatomy of the Plexus
• Roots C5 through T1
• Begins distal to the scalenes
• Prefixed and Postfixed
Anatomy of the Plexus
• Roots
• Trunks
• Divisions
• Cords
• Nerves
Anatomy
Brachial Plexus: Roots
Location: Behind anterior scalene muscle
Direct BranchesDorsal scapular nerve C5
○ Rhomboid muscles○ Levator scapulae muscle
Long thoracic nerve C5,6,7○ Serratus anterior muscle
Dermatome / Myotome
Specific skin areas supplied by a specific spinal nerve, regardless of the cutaneous nerve that supplies that area (relates to sensation)
Typically crosses 2 or more joints
Represent motor function (weakness)
C5- muscles above elbow except triceps
C6- elbow region C7- muscles in mid
forearm C8, T1- muscles of
hand

Upper Extremity Myotomes
C4 resisted shoulder shrugs (UT)
C5 resisted shoulder abduction (Delt)
C6 resisted elbow flexion (Biceps)
C7 resisted wrist flexion (FCR, Triceps)
C8 resisted thumb extension (EPL, FDS)
T1 finger abduction & adduction (Interossei)
Dermatomes vs. Cutaneous Innervation
Segmental Testing C5Motor: DeltoidReflex: BicepsSensation: Lateral Arm
Segmental Testing C6Motor: Biceps, wrist extensorsReflex: BrachioradialisSensory: Thumb/IF
Segmental Testing C7Motor: Triceps, Wrist Flexors, Finger Ext Reflex: TricepsSensation: Middle finger
Segmental Testing C8
Motor: finger flexors
Reflex: none
Sensation: ring and small fingers

Segmental Testing T1
Motor: Interossei
Reflex: None
Sensation: Medial proximal forearm
Brachial Plexus: Trunks Location: between lateral
border of anterior scalene and clavicle
Upper Trunk C5,6Middle Trunk C7 Lower Trunk C8,T1
Direct branches:Subclavian nerve C5,6
○ Subclavius m.Suprascapular nerve
C5,6○ Supraspinatus muscle○ Infraspinatus muscle
Trunk Lesion Symptoms-segmental Upper trunk lesion: proximal pain,
paresthesias in C5,6 dermatome Lower trunk lesion: distal pain, paresthesias
medial arm, hand
SS
Deltoid
IS
Where is this lesion occurring?
Hint:Wasting of Supraspinatus, InfraspinatusWhich nerve innervates SS, IS?Where does it come off BP?
Also wasting of Deltoid (and TM)Which nerve innervates Delt & TMinor?Where does this nerve come off the BP?
TMinor
Thoracic Outlet Supraclavicular region
containing the brachial plexus and the subclavian artery/vein
Syndrome often correlated with faulty posture, adaptive shortening of anterior cervical and chest muscles, prolonged overhead arm use, and pec minor hypertrophy
Brachial Plexus: Divisions Location: behind clavicle
Cause of lesion: clavicle fracture
Anterior: innervate volar structures
Posterior: innervate dorsal structures
Direct branches: Lateral anterior thoracic
nerve C5,6,7 Pectoralis major (clavicular
head)

Brachial Plexus: Cords
Location Below clavicle, behind
pectoralis minor
Motor and sensory deficits follow the distribution of the affected peripheral nerve
Named relative to axillary artery
LATERAL POSTERIOR MEDIAL
Lateral Cord Medial
Posterior
Brief review of normal and compromised neuroanatomy
Brachial plexus anatomy
Spinal nerves: pathways, classic lesions, and compression sites
Nerves exiting from Lateral Cord
Musculocutaneous nerve C5,6,7Biceps
Brachialis (along with radial nerve)
Corocobrachialis
Lateral root of Median nerve C5,6,7Motor to all median nerve muscles except the
intrinsics
Lateral CordThe Lateral Cord gives rise to two nerves
Lateral portion of Median Nerve:PT, FCR, PL, FDS(weak)
Musculocutaneous Nerve:CoracobrachialisBicepsBrachialis

Musculocutaneous nerveLateral Cord
Musculocutaneous pierces coracobrachialis
Lateral Cord
Musculocutaneous nerve C5,6
Arises from lateral cord
Innervates biceps, brachialis(with radial) and corocobrachialis
Sensory branches to lateral forearm: lateral antebrachial cutaneous nerve
Functional deficit Biceps atrophy Weak elbow flexion in
supination Decreased sensation along
radial and volar aspects of forearm
Lateral CordDermatomes vs. Cutaneous Innervation
Musculocutaneous
C5C6
Posterior CordUpper subscapular nerve C5,6
Subscapularis muscle
Lower subscapular nerve C5,6 Teres major muscle
Axillary nerve C5,6○ Deltoid muscle
Thoracodorsal nerve C6,7,8 Latissimus dorsi muscle
Radial nerve C5,6,7,8,T1Triceps, BR, Anconeus, ECRL/B, Supinator,
ECU, EDC, EDM, APL, EPL, EPB, EIP
Posterior Cord

Posterior Cord The Posterior Cord gives rise to 5 nerves
Axillary Nerve: Deltoid Teres minor
Upper/Lower Subscapular Nerve: SubscapularisTeres Major
Thoracodorsal Nerve: Latissimus Dorsi
Radial Nerve:Triceps, BR, Anconeus, ECRL/B,Supinator, ECU, EDC, EDM, APL, EPL, EPB, EIP
Axillary nerve
Posterior CordAxillary Nerve C5,6
Arises from posterior cord
Originates ventral aspect of subscapularis
Passes laterally toward inferior shoulder joint just inferior to humeral head
Through quadrangular spaceMedial border: humerusLateral border: long head of tricepsSuperior border: teres minor Inferior border: teres major
Wraps horizontally around post surgical neck of humerus
Enters deltoid
Posterior Cord
Axillary Nerve C5,6 Innervates deltoid and teres minor. A
sensory branch supplies the lateral aspect of the upper arm/deltoid tuberosity area
Functional loss-shoulder Abd/ER/elevation, numbness of lateral upper arm
Possible causes of lesions:Shoulder dislocationHumeral neck fractureSerum/vaccine inducedBrachial neuritis
Posterior Cord
Dermatomes vs. Cutaneous Innervation
Axillary
C5C6

Axillary Nerve Injury
Posterior Cord
Deltoid and teres minor wasting
Deltoid
Deltoid
TM
Radial Nerve
Posterior Cord
Radial Nerve C6,7,8,T1
Arises from posterior cord
Emerges between long and medial heads of triceps
Crosses under lateral head of triceps, pierces lateral intermuscular septum, enters anterior compartment of arm
Diverges anterior to radial head in forearm
Posterior Cord
Radial Nerve C6,7,8,T1 Cutaneous branches:Posterior cutaneous of
arm
Lower lateral cutaneous of arm
Posterior cutaneous of forearm
Motor innervation:Triceps
Anconeus
BR
ECRL
Brachialis (musculocutaneous)
Posterior Cord
Radial Nerve in Forearm Bifurcates at anterior radial
head Superficial branch/DRSNDescends forearm just
medial to BRCutaneous supply to
dorsoradial hand Deep branch/PIN SupinatorECRBEDCEDMECUEPL, EPB, APLEIPTerminates in dorsal wrist
capsule: proprioception
Posterior Cord
Dermatomes vs. Cutaneous Innervation
Radial
C6C7C8T1

Superficial RADIAL NERVE Sensory Innervation lesion to the radial sensory nerve
Posterior Cord
Radial Nerve Palsy
RADIAL NERVEPotential Sites of Compression
Radial Groove of Humerus
Lateral Intermuscular Septum
Fibrous Band between BR and Brachialis/ECRB
Leash of Henry
Arcade of Frohse
Supinator
Distal BR
Medial Cord
Medial ant. thoracic nerve C8,T1Pectoralis minor musclePectoralis major muscle
Medial cutaneous nerve of arm C8,T1Medial cutaneous nerve of forearm C8,T1Ulnar nerve C8,T1Medial root of median nerve C8,T1
Median intrinsics and cutaneous in the hand
Medial CordThe Medial Cordgives rise to threemotor nerves
Medial Ant. Thoracic N.: Pectoralis Major/ Minor
Ulnar Nerve:FCU, FDP ¾, AddP, FPB,Lumbrical ¾Interossei, ADM,ODM,FDM
Medial Portion of the Median N.: FDS, FDP 1,2, FPL, PQ, APB, FPB, OP, Lumbricals 1,2

Median Nerve
Lateral root of median nerve from lateral cord
Medial root of median nerve from medial cord
Medial and Lateral Cords Median Nerve C5,6,7,8,T1 Arises from medial and
lateral cords
Descends arm in medial neurovascular bundle with ulnar nerve and brachial artery
Moves laterally to enter cubital fossa and passes deep to bicipital aponeurosis
Exits cubital fossa between 2 heads of PT and fibrous FDS arch in forearm
Medial and Lateral Cords
Median nerve in the forearm Median Nerve C5,6,7,8,T1 AIN branches off median
nerve at approximately level of PT or FDS arch
Median nerve continues in deep position down forearm between FDS and FDP
Medial Palmar Cutaneous (superficial palmar nerve)branches from median at distal 1/3 of FA
Median curves laterally at proximal wrist to be volar to FDS to cross into hand under TCL
Medial and Lateral Cords
AIN
Median Nerve C5,6,7,8,T1 Median motor innervation:PTFCRPLFDSFPB (superficial head)APBOPLumbricals 1 + 2
AIN motor innervation:FPLPQFDP to IF (MF)Terminates in volar wrist
capsule: proprioceptive input
Medial and Lateral Cords Median NerveLevel of the Carpal Tunnel
Medial and Lateral Cords
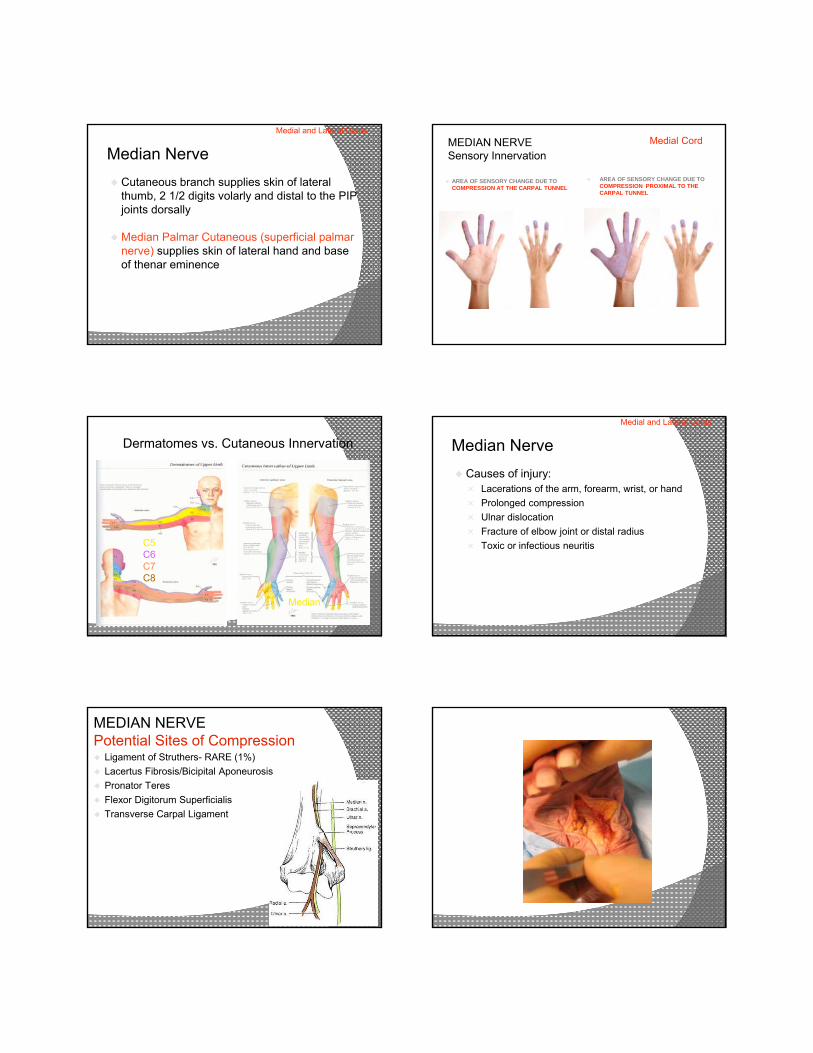
Median Nerve
Cutaneous branch supplies skin of lateral thumb, 2 1/2 digits volarly and distal to the PIP joints dorsally
Median Palmar Cutaneous (superficial palmar nerve) supplies skin of lateral hand and base of thenar eminence
Medial and Lateral Cords
MEDIAN NERVE Sensory Innervation
AREA OF SENSORY CHANGE DUE TO COMPRESSION AT THE CARPAL TUNNEL
Medial Cord
AREA OF SENSORY CHANGE DUE TO COMPRESSION PROXIMAL TO THE CARPAL TUNNEL
Dermatomes vs. Cutaneous Innervation
Median
C5C6C7C8
Median Nerve
Causes of injury: Lacerations of the arm, forearm, wrist, or hand
Prolonged compression
Ulnar dislocation
Fracture of elbow joint or distal radius
Toxic or infectious neuritis
Medial and Lateral Cords
MEDIAN NERVE Potential Sites of Compression Ligament of Struthers- RARE (1%)
Lacertus Fibrosis/Bicipital Aponeurosis
Pronator Teres
Flexor Digitorum Superficialis
Transverse Carpal Ligament

Ulnar Nerve Medial Cord Ulnar Nerve C8,T1 Arises from medial cord
Descends arm in medial neurovascular bundle with median nerve, brachial artery
At distal 1/3 of arm, passes through medial intermuscular septum into posterior compartment
Descends supracondylar area in fascial groove, crosses elbow posteriorly in condylar groove
Enters FA passing between medial epicondyle and olecranon then deep to FCU
Medial Cord
Ulnar Nerve C8,T1 Passes through entire FA deep
to FCU
DUCN, UPC branch off ulnar nerve about distal third of FA
At FCU attachment to pisiform, ulnar nerve passes lateral to pisiform and medial to hook of hamate
Ulnar nerve branches superficial (cutaneous) and deep (motor) within this canal (Guyon’s)
Medial CordUlnar Nerve C8,T1
Motor innervation in FA: FCU FDP to RF/SF
Motor innervation in hand:ADMFDMODMPalmar and Dorsal InterosseiLumbricals 3 & 4Deep head of FPBADd Pollicis
Medial Cord
Ulnar Nerve C8,T1
Cutaneous branch supplies skin of ulnar 1 1/2 digits volarly and distal to the PIP joints dorsally
Ulnar Palmar Cutaneous supplies skin of ulnar volar palm
Dorsal Ulnar Cutaneous supplies the skin of the dorsomedial hand
Medial Cord ULNAR NERVE Sensory Innervation
AREA OF SENSORY CHANGE FROM LESION OF THE ULNAR NERVE DISTAL TO THE DORSAL CUTANEOUS BRANCH
AREA OF SENSORY CHANGE FROM LESION OF THE ULNAR NERVE DISTAL TO PALMAR CUTANEOUS BRANCH
Medial Cord

Dermatomes vs. Cutaneous Innervation
Ulnar
C8T1
Ulnar NervePotential Sites of Compression
Arcade of Struthers
Medial Intermuscular Septum
Subluxing Medial Head of Triceps
Cubital Tunnel
Flexor Carpi Ulnaris
Guyon’s Canal
87
Ulnar Nerve Compression Sites
Cubital Tunnel Guyon’s Canal
Review of Objectives
Brief review of normal and compromised neuroanatomy
Brachial plexus anatomy
Spinal nerves: pathways, classic lesions, and compression sites
THANK YOU!
Acknowledgements:Lorna Canavan Kahn, PT, CHT Milliken Hand Rehabilitation CenterSt. Louis, Missouri
Keith Segalman, MDCurtis National Hand CenterBaltimore, MD

ReferencesBell Krotoski JA. Sensibility Testing: History, Instrumentation, and Clinical
Procedures in Rehabilitation of the Hand and Upper Extremity, 6th Edition. Skirven, Osterman, Fedorczyk, Amadio. Elsevier/Mosby: Philadelphia, PA 2011.
Boyd KU, Nimigan AS & MacKinnon SE. Nerve Reconstruction in the Hand and Upper Extremity. Clin Plast Surg. 2011 Oct; 38(4):643-60.
Callahan A. Sensibility Assessment For Nerve Lesions-In-Continuity and Nerve Lacerations in Rehabilitation of the Hand and Upper Extremity, 5th Edition. Hunter, Mackin, Callahan. Mosby: St. Louis, MO 2002.
Fox IK & MacKinnon SE. Adult Peripheral Nerve Disorders- Nerve Entrapment, Repair, Transfer and Brachial Plexus Disorders. Plast Reconstr Surg 2011 May; 127(5).
Giuffre JL, Kakar S, Bishop AT, Spinner RJ & Shin AY. Current Concepts of the Treatment of Adult Brachial Plexus Injuries. JHS 2010; 35A:678-688.
Henry FP, Farkhad RI, O’Shaughnessy M & O’Sullivan ST. A Comparison Between Complete Immobilisation an Protected Active Mobilization in Sensory Nerve Recovery Following Isolated Digital Nerve Injury. J Hand Surg Eur 2012 Jun; 37(5):422-6.
91
References (cont)Hooper TL, Denton J, McGalliard MK, Brismee JM & Sizer PS. Thoracic
Outlet Syndrome: a controversial clinical condition. Part I: anatomy, and clinical examination/diagnosis. J Manual & Manipulative Therapy 2010 Jun; 18(2):74-83.
Kattan AE & Borschel GH. Anatomy of the Brachial Plexus. J Ped Rehab Med: An Interdisciplinary Approach 2011; 4:107-111.
Limthongthang R, Bachoura A, Songcharoen P & Osterman AL. Adult Brachial Plexus Injury Evaluation and Management. Orthop Clin N Am 2013; 44:591-603.
Novak CB & Mackinnon SE. Outcomes Following Conservative Management of Thoracic Outlet Syndrome. JHS 1995; 20(4):542-548.
Osterman AL & Lincoski C. Thoracic Outlet Syndrome in Rehabilitation of the Hand and Upper Extremity, 6th Edition. Skirven, Osterman, Fedorczyk, Amadio. Elsevier/Mosby: Philadelphia, PA 2011.
Pratt N. Anatomy of Nerve Entrapment Sites in the Upper Quarter. J Hand Ther 2005; 18:216-229.
Sheth RN & Campbell JN. Surgical Treatment of Thoracic Outlet Syndrome: A Randomized Trial Comparing Two Operations. J Neurosurg Spine 2005; 3(5):355-363.
92
Duchenne Sign
Claw deformity of thering and small finger
Low ulnar nerve palsy
*RF/SF MCP hyperextension due to unchecked pull of extrinsic extensors and absence/weakness of intrinsic extension (lumbricals and interossei) *IP joints in flexion due to unopposed extrinsic flexors*FDP weakness with high ulnar nerve palsy diminishes this posture
Andre Thomas Sign
Exaggeration of the claw deformity: In attempt to straighten fingers, wrist falls into flexion during action of the extensors (tenodesis) to the middle finger
Crossed Finger Sign
*Weakness of the interossei limiting ability of the middle finger to fully cross the index finger*Compare with uninvolved side
Egawa Sign
*MF unable to ab/adduct when flexed at IP joints (hook fist position) *IP joint flexion limits ability of extrinsic extensors to give appearance of ab/adduction

Froment Sign
*Patient asked to pull/resist piece of paper held between thumb and radial index finger (lateral type grasp)*With loss/weakness of Adductor Pollicis, Flexor Digitorum Profundus overcompensates with thumb IP joint flexion
Jeanne Sign *Thumb MCP hyperextension in addition to IP joint flexion*Observed during evaluation of Adductor Pollicis (paper pull/resist test or resisted lateral pinch)
Wartenberg Sign
*Small finger posturing in abduction*Inability/weakness limiting SF adduction to RF
Masse Sign*Intrinsic muscle wasting causing flattening of the hypothenar eminence and metacarpal arch